

The Use of an Inspiration-Synchronized Vibrating Mesh Nebulizer for Prolonged Inhalative Iloprost Administration in Mechanically Ventilated Patients—An In Vitro Model


Abstract
1. Introduction
2. Materials and Methods
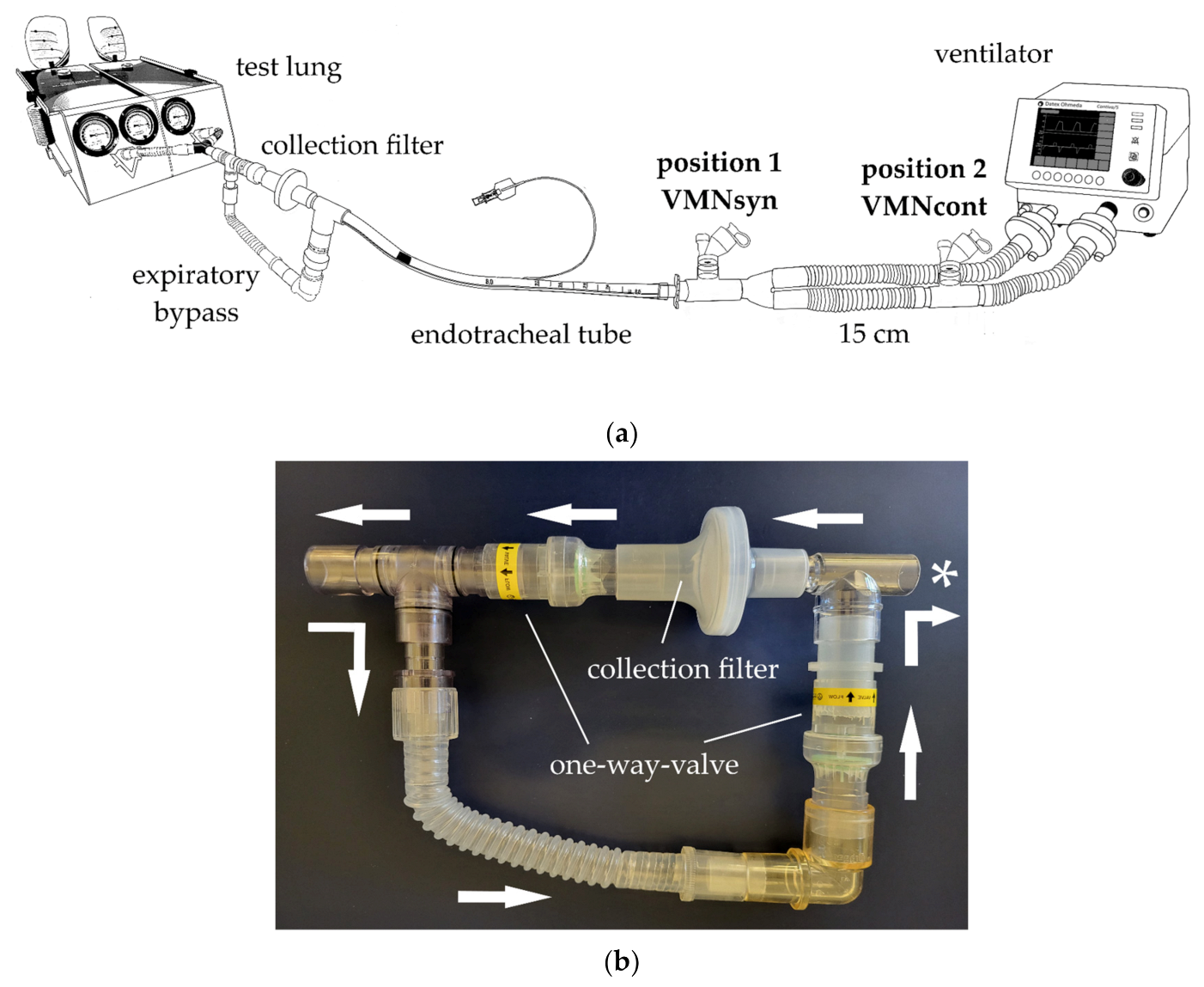
2.1. Ventilator Circuit and Lung Model
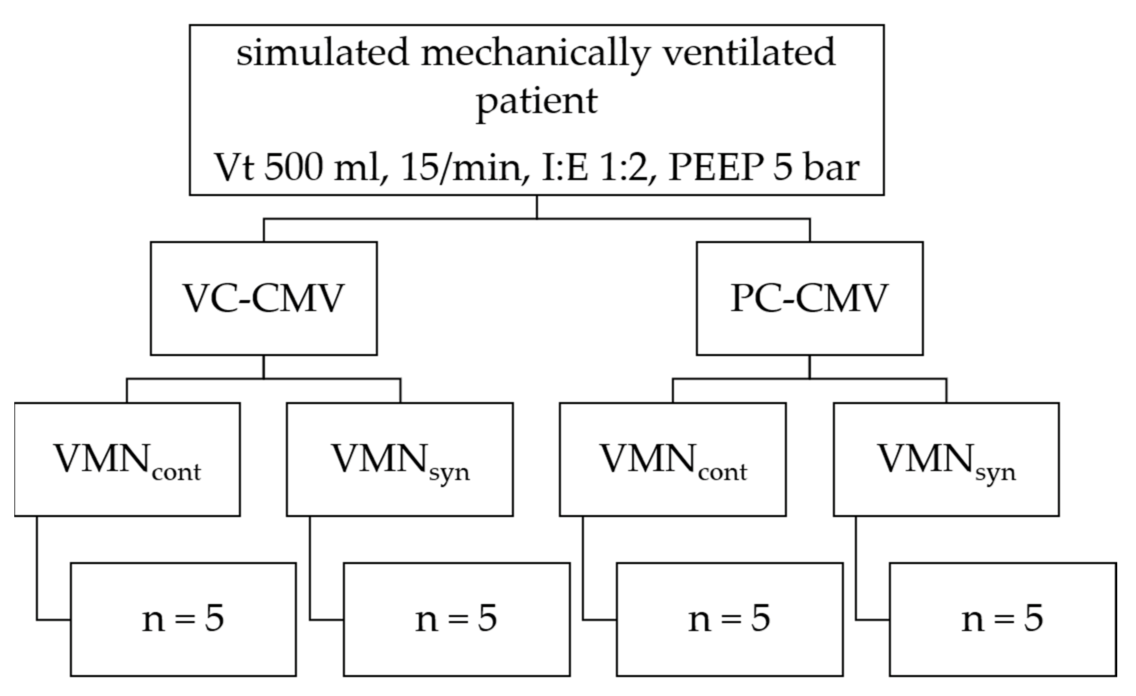
2.2. Ventilator Settings
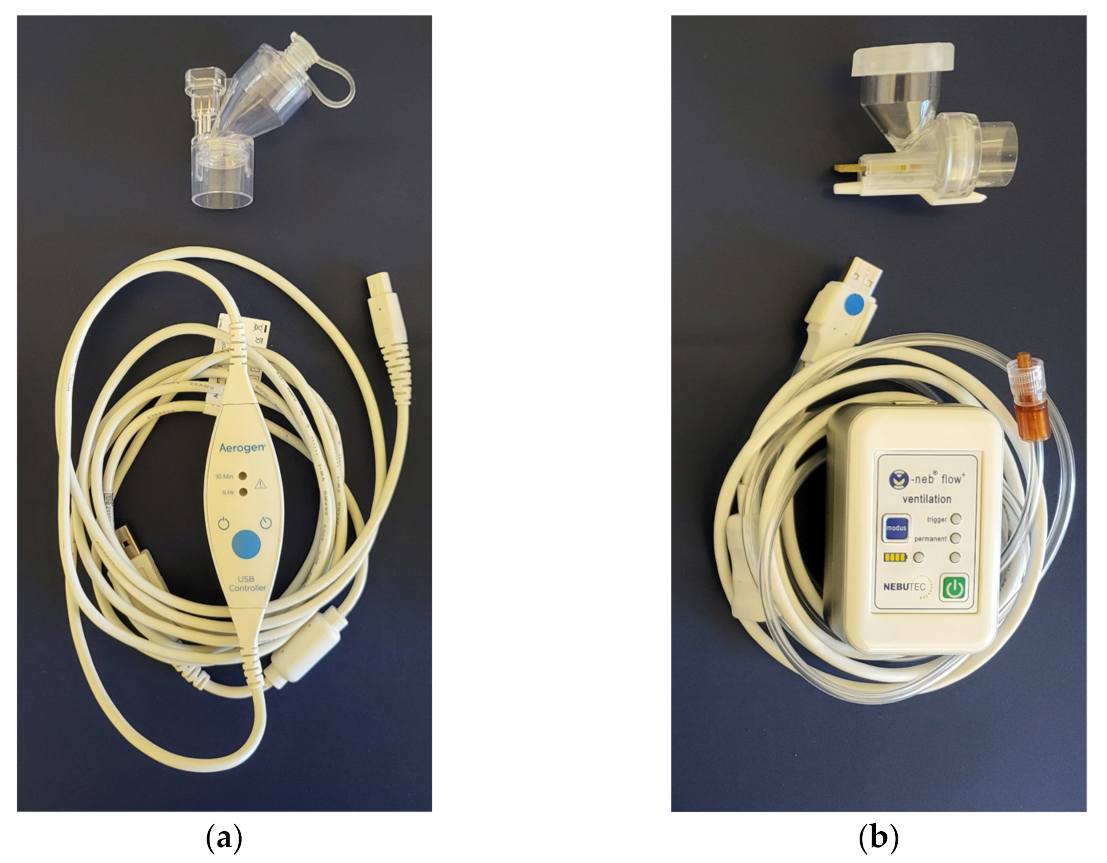
2.3. Nebulizers
2.4. Nebulizer Positions
2.5. Nebulization of Iloprost
2.6. Iloprost Sample Preparation
2.7. Iloprost Analysis and Quantification
2.8. Iloprost Deposition Rate Calculation
2.9. Nebulizer Output Calculation
2.10. Statistical Analysis
3. Results
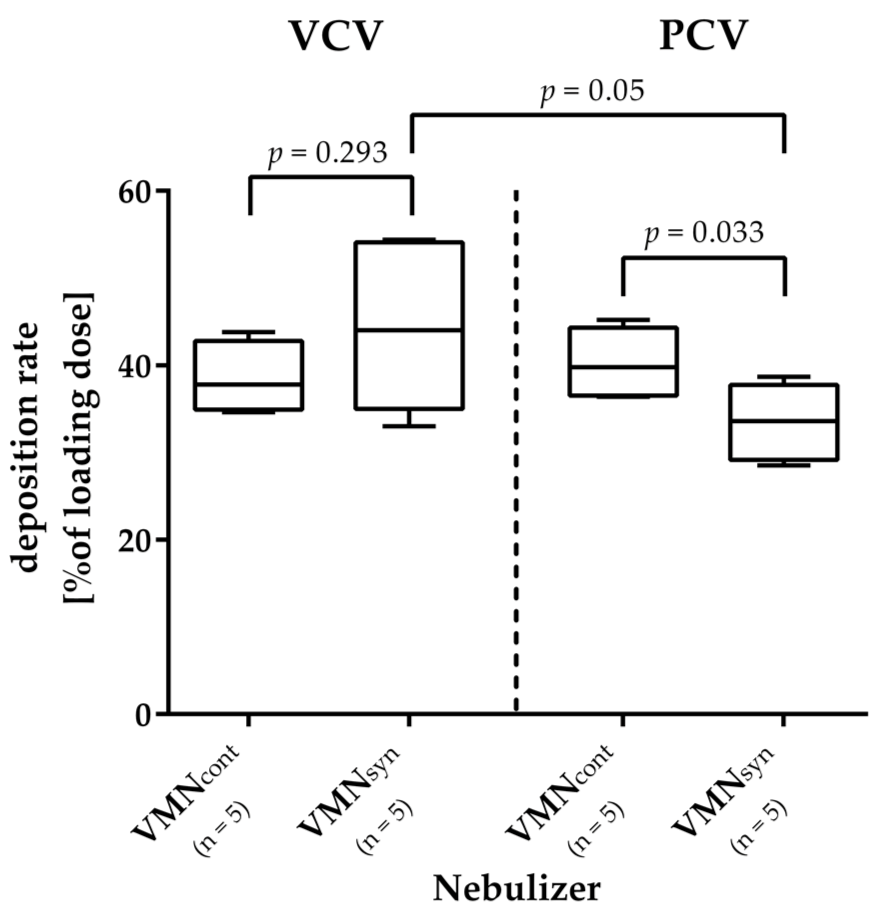
3.1. Iloprost Deposition Rate
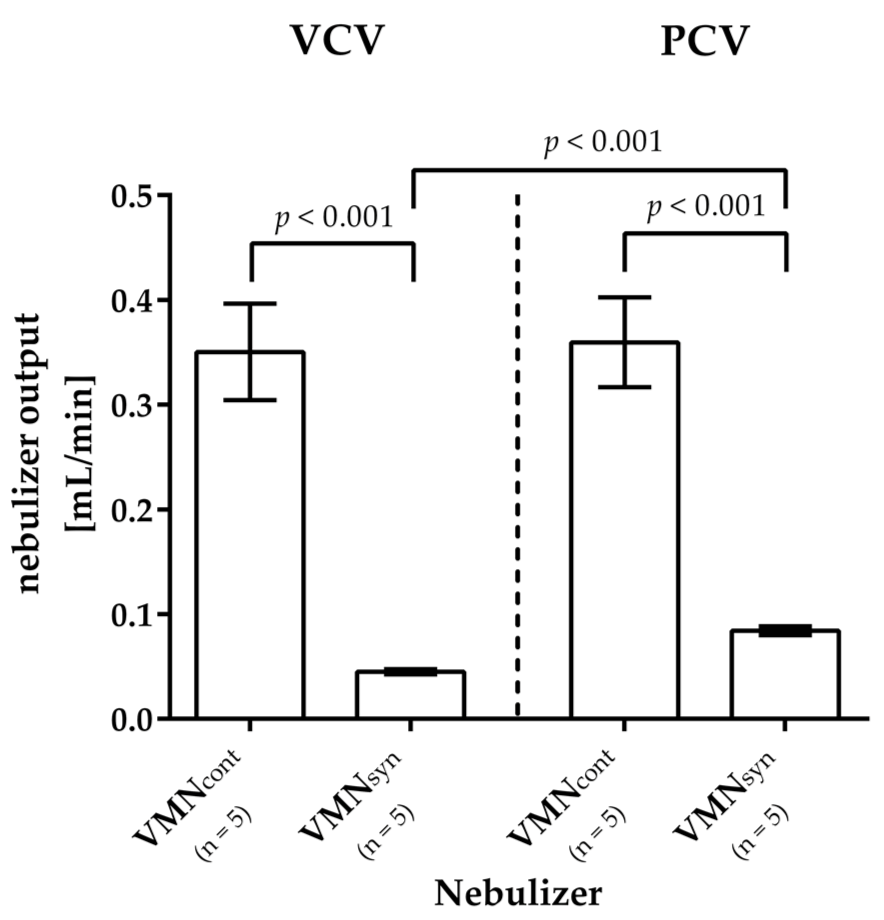
3.2. Aerosol Output and Nebulization Time
4. Discussion
4.1. Iloprost Deposition Rate
4.2. Aerosol Output and Nebulization Time
4.3. Advantages and Disadvantages of Parenteral and Inhaled Iloporost Administration in Mechanically Ventilated Patients
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ARDS | acute respiratory distress syndrome |
| ETT | endotracheal tube |
| HPLC | high-performance liquid chromatography |
| iNO | inhaled nitric oxide |
| LC | liquid chromatography |
| MS | mass spectrometry |
| PC-CMV | pressure-controlled continuous mandatory ventilation |
| PEEP | positive end-expiratory pressure |
| PPH | primary pulmonary hypertension |
| VC-CMV | volume-controlled continuous mandatory ventilation |
| VMN | vibrating mesh nebulizer |
| VMNcont | continuous vibrating mesh nebulizer |
| VMNsyn | inspiration-synchronized vibrating mesh nebulizer |
References
- Price, L.C.; McAuley, D.F.; Marino, P.S.; Finney, S.J.; Griffiths, M.J.; Wort, S.J. Pathophysiology of pulmonary hypertension in acute lung injury. Am. J. Physiol. Lung Cell Mol. Physiol. 2012, 302, L803–L815. [Google Scholar] [CrossRef]
- Bull, T.M.; Clark, B.; McFann, K.; Moss, M. Pulmonary vascular dysfunction is associated with poor outcomes in patients with acute lung injury. Am. J. Respir. Crit. Care Med. 2010, 182, 1123–1128. [Google Scholar] [CrossRef] [PubMed]
- Mekontso Dessap, A.; Boissier, F.; Charron, C.; Bégot, E.; Repessé, X.; Legras, A.; Brun-Buisson, C.; Vignon, P.; Vieillard-Baron, A. Acute cor pulmonale during protective ventilation for acute respiratory distress syndrome: Prevalence, predictors, and clinical impact. Intensive Care Med. 2016, 42, 862–870. [Google Scholar] [CrossRef]
- Ganeriwal, S.; Alves dos Anjos, G.; Schleicher, M.; Hockstein, M.A.; Tonelli, A.R.; Duggal, A.; Siuba, M.T. Right ventricle-specific therapies in acute respiratory distress syndrome: A scoping review. Crit. Care 2023, 27, 104. [Google Scholar] [CrossRef] [PubMed]
- Ymeraj, S.; Attou, R.; Redant, S. Right ventricule-specific therapies in ARDS: Other vasodilating agents to be considered. Crit. Care 2023, 27, 133. [Google Scholar] [CrossRef]
- Moloney, E.D.; Evans, T.W. Pathophysiology and pharmacological treatment of pulmonary hypertension in acute respiratory distress syndrome. Eur. Respir. J. 2003, 21, 720–727. [Google Scholar] [CrossRef]
- Sawheny, E.; Ellis, A.L.; Kinasewitz, G.T. Iloprost improves gas exchange in patients with pulmonary hypertension and ARDS. Chest 2013, 144, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Fuller, B.M.; Mohr, N.M.; Skrupky, L.; Fowler, S.; Kollef, M.H.; Carpenter, C.R. The use of inhaled prostaglandins in patients with ARDS: A systematic review and meta-analysis. Chest 2015, 147, 1510–1522. [Google Scholar] [CrossRef] [PubMed]
- Searcy, R.J.; Morales, J.R.; Ferreira, J.A.; Johnson, D.W. The role of inhaled prostacyclin in treating acute respiratory distress syndrome. Ther. Adv. Respir. Dis. 2015, 9, 302–312. [Google Scholar] [CrossRef] [PubMed]
- Harris, K.W.; O’Riordan, T.G.; Smaldone, G.C. Aerosolized iloprost customized for the critically ill. Respir. Care 2007, 52, 1507–1509. [Google Scholar]
- Rello, J.; Bouglé, A.; Rouby, J.J. Aerosolised antibiotics in critical care. Intensive Care Med. 2023, 49, 848–852. [Google Scholar] [CrossRef]
- Krause, W.; Krais, T. Pharmacokinetics and pharmacodynamics of the prostacyclin analogue iloprost in man. Eur. J. Clin. Pharmacol. 1986, 30, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Higenbottam, T.W.; Butt, A.Y.; Dinh-Xaun, A.T.; Takao, M.; Cremona, G.; Akamine, S. Treatment of pulmonary hypertension with the continuous infusion of a prostacyclin analogue, iloprost. Heart 1998, 79, 175–179. [Google Scholar] [CrossRef] [PubMed]
- Malekmohammad, M.; Sharif-Kashani, B.; Monjazebi, F.; Saliminejad, L. Intermittent intravenous administration of Iloprost in patients with idiopathic pulmonary arterial hypertension. Int. J. Cardiovasc. Acad. 2016, 2, 114–118. [Google Scholar] [CrossRef]
- Anderson, A.C.; Dubosky, M.N.; Fiorino, K.A.; Quintana, V.; Kaplan, C.A.; Vines, D.L. The Effect of Nebulizer Position on Aerosolized Epoprostenol Delivery in an Adult Lung Model. Respir. Care 2017, 62, 1387–1395. [Google Scholar] [CrossRef] [PubMed]
- Rello, J.; Rouby, J.J.; Sole-Lleonart, C.; Chastre, J.; Blot, S.; Luyt, C.E.; Riera, J.; Vos, M.C.; Monsel, A.; Dhanani, J.; et al. Key considerations on nebulization of antimicrobial agents to mechanically ventilated patients. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2017, 23, 640–646. [Google Scholar] [CrossRef]
- Luyt, C.E.; Clavel, M.; Guntupalli, K.; Johannigman, J.; Kennedy, J.I.; Wood, C.; Corkery, K.; Gribben, D.; Chastre, J. Pharmacokinetics and lung delivery of PDDS-aerosolized amikacin (NKTR-061) in intubated and mechanically ventilated patients with nosocomial pneumonia. Crit. Care 2009, 13, R200. [Google Scholar] [CrossRef] [PubMed]
- Dhand, R.; Sohal, H. Pulmonary Drug Delivery System for inhalation therapy in mechanically ventilated patients. Expert Rev. Med. Devices 2008, 5, 9–18. [Google Scholar] [CrossRef]
- Dhand, R. Maximizing aerosol delivery during mechanical ventilation: Go with the flow and go slow. Intensive Care Med. 2003, 29, 1041–1042. [Google Scholar] [CrossRef]
- Ari, A.; Areabi, H.; Fink, J.B. Evaluation of aerosol generator devices at 3 locations in humidified and non-humidified circuits during adult mechanical ventilation. Respir. Care 2010, 55, 837–844. [Google Scholar]
- Demers, R.R.; Burciaga, C.; Sousa, M. The Respirgard II 303 breathing circuit filter is NOT an “absolute filter”. Respir. Care 2016, 61, 1710–1711. [Google Scholar] [CrossRef] [PubMed]
- Hou, H.; Xu, D.; Dai, B.; Zhao, H.; Wang, W.; Kang, J.; Tan, W. Position of different nebulizer types for aerosol delivery in an adult model of mechanical ventilation. Front. Med. 2022, 9, 950569. [Google Scholar] [CrossRef]
- El Taoum, K.K.; Xi, J.; Kim, J.; Berlinski, A. In Vitro Evaluation of Aerosols Delivered via the Nasal Route. Respir. Care 2015, 60, 1015–1025. [Google Scholar] [CrossRef]
- Quinn, W. Effect of a new nebulizer position on aerosol delivery during mechanical ventilation: A bench study. Respir. Care 1992, 37, 423–431. [Google Scholar]
- Hughes, J.M.; Saez, J. Effects of nebulizer mode and deposition in a mechanical ventilator circuit on dose efficiency. Respir. Care 1987, 32, 1131–1135. [Google Scholar]
- Ari, A.; Atalay, O.T.; Harwood, R.; Sheard, M.M.; Aljamhan, E.A.; Fink, J.B. Influence of nebulizer type, position, and bias flow on aerosol drug delivery in simulated pediatric and adult lung models during mechanical ventilation. Respir. Care 2010, 55, 845–851. [Google Scholar] [PubMed]
- Chen, Y.F.; Jowett, S.; Barton, P.; Malottki, K.; Hyde, C.; Gibbs, J.S.; Pepke-Zaba, J.; Fry-Smith, A.; Roberts, J.; Moore, D. Clinical and cost-effectiveness of epoprostenol, iloprost, bosentan, sitaxentan and sildenafil for pulmonary arterial hypertension within their licensed indications: A systematic review and economic evaluation. Health Technol. Assess. 2009, 13, 1–320. [Google Scholar] [CrossRef]
- Barst, R.J.; Rubin, L.J.; Long, W.A.; McGoon, M.D.; Rich, S.; Badesch, D.B.; Groves, B.M.; Tapson, V.F.; Bourge, R.C.; Brundage, B.H.; et al. A comparison of continuous intravenous epoprostenol (prostacyclin) with conventional therapy for primary pulmonary hypertension. New Engl. J. Med. 1996, 334, 296–301. [Google Scholar] [CrossRef] [PubMed]
- Dembinski, R.; Brackhahn, W.; Henzler, D.; Rott, A.; Bensberg, R.; Kuhlen, R.; Rossaint, R. Cardiopulmonary effects of iloprost in experimental acute lung injury. Eur. Respir. J. 2005, 25, 81–87. [Google Scholar] [CrossRef]
- Zwissler, B.; Kemming, G.; Habler, O.; Kleen, M.; Merkel, M.; Haller, M.; Briegel, J.; Welte, M.; Peter, K. Inhaled prostacyclin (PGI2) versus inhaled nitric oxide in adult respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 1996, 154, 1671–1677. [Google Scholar] [CrossRef]
- Walmrath, D.; Schneider, T.; Schermuly, R.; Olschewski, H.; Grimminger, F.; Seeger, W. Direct comparison of inhaled nitric oxide and aerosolized prostacyclin in acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 1996, 153, 991–996. [Google Scholar] [CrossRef] [PubMed]
- Tsareva, N.A.; Avdeev, S.N.; Kosanovic, D.; Schermuly, R.T.; Trushenko, N.V.; Nekludova, G.V. Inhaled iloprost improves gas exchange in patients with COVID-19 and acute respiratory distress syndrome. Crit. Care 2021, 25, 258. [Google Scholar] [CrossRef]
- Byron, P.R.; Hindle, M.; Lange, C.F.; Longest, P.W.; McRobbie, D.; Oldham, M.J.; Olsson, B.; Thiel, C.G.; Wachtel, H.; Finlay, W.H. In Vivo–In Vitro Correlations: Predicting Pulmonary Drug Deposition from Pharmaceutical Aerosols. J. Aerosol. Med. Pulm. Drug Deliv. 2010, 23, S-59–S-69. [Google Scholar] [CrossRef] [PubMed]
- Fink, J.B.; Dhand, R.; Grychowski, J.; Fahey, P.J.; Tobin, M.J. Reconciling in vitro and in vivo measurements of aerosol delivery from a metered-dose inhaler during mechanical ventilation and defining efficiency-enhancing factors. Am. J. Respir. Crit. Care Med. 1999, 159, 63–68. [Google Scholar] [CrossRef]
- Ari, A. Aerosol Therapy in Pulmonary Critical Care. Respir. Care 2015, 60, 858–874. [Google Scholar] [CrossRef] [PubMed]
- Darquenne, C. Aerosol deposition in health and disease. J. Aerosol. Med. Pulm. Drug Deliv. 2012, 25, 140–147. [Google Scholar] [CrossRef]
- Ari, A.; Fink, J.B. Delivered dose with jet and mesh nebulisers during spontaneous breathing, noninvasive ventilation and mechanical ventilation using adult lung models. ERJ Open Res. 2021, 7, 00027–02021. [Google Scholar] [CrossRef]
- Bein, T.; Grasso, S.; Moerer, O.; Quintel, M.; Guerin, C.; Deja, M.; Brondani, A.; Mehta, S. The standard of care of patients with ARDS: Ventilatory settings and rescue therapies for refractory hypoxemia. Intensive Care Med. 2016, 42, 699–711. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Deposition Rate as Percentage of Nominal Dose (Mean ± SD %) | |||
|---|---|---|---|
| Nebulizer | VC-CMV | PC-CMV | |
| VMNcont (n = 5) | 38.5 ± 4.2 | 40.3 ± 4.0 | p = 0.534 |
| VMNsyn (n = 5) | 44.4 ± 9.7 | 33.5 ± 4.4 | p = 0.50 |
| p = 0.293 | p = 0.033 | ||
| Aerosol Output in mL per Minute (Mean ± SD %) | |||
|---|---|---|---|
| Nebulizer | VC-CMV | PC-CMV | |
| VMNcont (n = 5) | 0.36 ± 0.04 | 0.36 ± 0.04 | p = 0.753 |
| VMNsyn (n = 5) | 0.04 ± 0.00 | 0.09 ± 0.00 | p < 0.001 |
| p < 0.001 | p < 0.001 | ||
| Nebulization Time in Min:Sec (Mean ± SD %) | |||
|---|---|---|---|
| Nebulizer | VC-CMV | PC-CMV | |
| VMNcont (n = 5) | 8:26 ± 1:07 | 8:21 ± 1:05 | p = 0.908 |
| VMNsyn (n = 5) | 65:40 ± 3:49 | 35:27 ± 1:38 | p < 0.001 |
| p < 0.001 | p < 0.001 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Otto, M.; Kropp, Y.; Jäger, E.; Neumaier, M.; Thiel, M.; Quintel, M.; Tsagogiorgas, C. The Use of an Inspiration-Synchronized Vibrating Mesh Nebulizer for Prolonged Inhalative Iloprost Administration in Mechanically Ventilated Patients—An In Vitro Model. Pharmaceutics 2023, 15, 2080. https://doi.org/10.3390/pharmaceutics15082080
Otto M, Kropp Y, Jäger E, Neumaier M, Thiel M, Quintel M, Tsagogiorgas C. The Use of an Inspiration-Synchronized Vibrating Mesh Nebulizer for Prolonged Inhalative Iloprost Administration in Mechanically Ventilated Patients—An In Vitro Model. Pharmaceutics. 2023; 15(8):2080. https://doi.org/10.3390/pharmaceutics15082080
Chicago/Turabian StyleOtto, Matthias, Yannik Kropp, Evelyn Jäger, Michael Neumaier, Manfred Thiel, Michael Quintel, and Charalambos Tsagogiorgas. 2023. "The Use of an Inspiration-Synchronized Vibrating Mesh Nebulizer for Prolonged Inhalative Iloprost Administration in Mechanically Ventilated Patients—An In Vitro Model" Pharmaceutics 15, no. 8: 2080. https://doi.org/10.3390/pharmaceutics15082080
APA StyleOtto, M., Kropp, Y., Jäger, E., Neumaier, M., Thiel, M., Quintel, M., & Tsagogiorgas, C. (2023). The Use of an Inspiration-Synchronized Vibrating Mesh Nebulizer for Prolonged Inhalative Iloprost Administration in Mechanically Ventilated Patients—An In Vitro Model. Pharmaceutics, 15(8), 2080. https://doi.org/10.3390/pharmaceutics15082080