
A Review of Repurposed Cancer Drugs in Clinical Trials for Potential Treatment of COVID-19



Abstract
1. Introduction
2. Materials and Methods
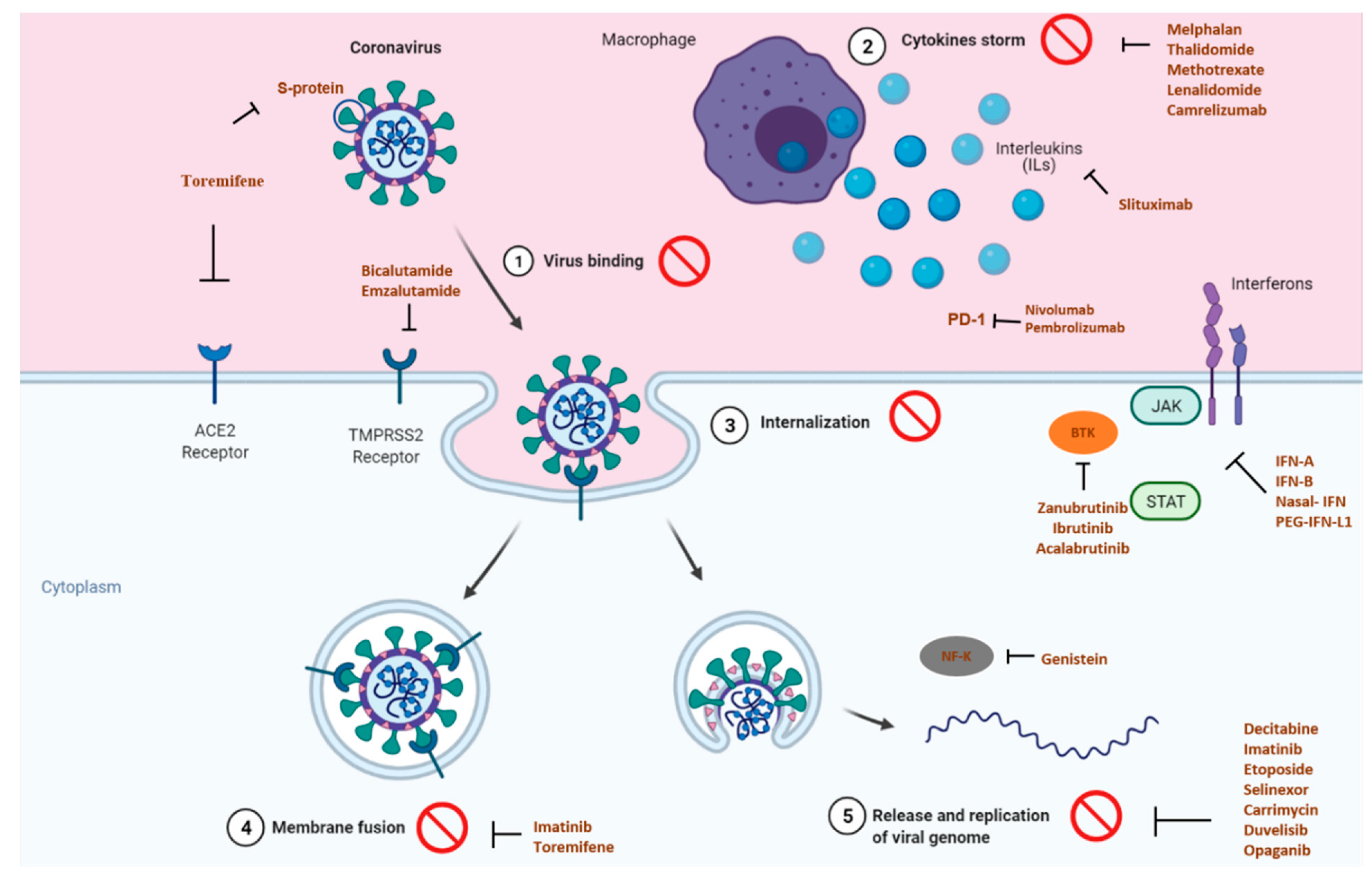
3. Viral, Host and Immune Targets in COVID-19
4. Similarities of Cancer Immune Response and COVID-19
5. Repurposing Anticancer Drugs against COVID-19
5.1. Interferon-Based Therapies
5.2. Anticytokine Agents
5.3. Immune-Checkpoint Inhibitors
5.4. Hormone Therapy
5.5. Inhibitor of Elongation Factor 1A and the Eukaryotic Initiation Factor 4A
5.6. Blockade of Kinase Cascades
5.7. Radiation and Prophylactic Vitamin D
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
Appendix A

{kind=link}
| Anticancer Drug | Viral—Host Targets | Mechanism of Action | Tested in Clinical Trials | NCT Identifier | Combination | Status | Phase | Eligible Population | Primary End-Point | Source (20 May 2021) |
|---|---|---|---|---|---|---|---|---|---|---|
| Acalabrutinib | BTK | Inhibits the activity of BTK and prevents the activation of the B-cell antigen receptor | United states | NCT04380688 | - | Completed | Phase 2 | COVIDCOVID-19 infection | Occurrence of Adverse Events and Serious Adverse Events | [10] |
| Several locations | NCT04346199 | - | Completed | Phase 2 | COVID-19 infection | Subject alive and free of respiratory failure | ||||
| Bevacizumab | VEGF | Vascular permeability inhibition | Yes (France and China) | NCT04275414 | - | Completed | Phase 2 | Severe lung disease or critical disease | Change of PaO2 to FiO2 ratio | [10] |
| NCT04344782 | - | Not yet recruiting | Phase 2 | Severe lung disease | Number of patients who avoid mechanical-assisted ventilation | |||||
| NCT04305106 | - | Recruiting | Not applicable | Disease requiring O2-support | Time to clinical improvement | |||||
| Bicalutamide | Downregulates TMPRSS2 | Binding of androgen receptor | Yes | NCT04509999 | - | Recruiting | Phase 3 | COVID-19 infection, confirmed | COVID-19 symptom relief | [9] |
| NCT04652765 | camostat | Recruting | Phase 1 | COVID-19 infection, confirmed | Reduce number of participants requiring hospitalization | |||||
| Camrelizumab | Immune homeostasis | PD-1/PD-L1 pathway | Yes (China) | ChiCTR2000029806 | - | Recruiting | Not applicable | COVID-19 infection | Proportion of patients with | [10] |
| Blockade | a lung injury score | |||||||||
| - | reduction | |||||||||
| Carrimycin | Inhibit the replication of SARS-CoV-2 in the<break/>cells | Inhibits mTOR pathway | Not provided | NCT04286503 | - | Not yet recruting | Phase 4 | COVID-19 infection | Fever to normal time | [11] |
| NCT04672564 | - | Recruting | Phase 3 | Patient with SARS-CoV-2 infection | Percentage of patients alive without need for supplemental oxygen and ongoing in patient-medical care | |||||
| Decitabine | Nucleic Acid Synthesis Inhibitor | Nucleic acid synthesis inhibitor | Yes (USA) | NCT04482621 | - | Recruting | Phase 2 | COVID infection | Clinical improvement | [9] |
| Duvelisib | PI3K inhibition | Immune homeostasis restoration and viral replication inhibition | Yes (USA) | NCT04372602 | - | Recruting | Phase 2 | Critical disease | Overall survival | [10] |
| NCT04487886 | - | Recruting | Phase 2 | severe COVID-19 who do not require mechanical ventilation | Reduce overall necessity of ventilation | |||||
| Ensifentrine | High selectivity for PDE3 and PDE4 over other enzymes and receptors to minimize off-target effects | Dual inhibitor of phosphodiesterase 3 (PDE3) and 4 (PDE4) | United states | NCT04527471 | None | Active, not recruting | Phase 2 | SARS-CoV-2 infection | Proportion of patients with recovery | [11] |
| Enzalutamide | reduce androgen driven morbidity in COVID-19 | Competitive binder of androgens | Sweden | NCT04475601 | - | Recruting | Phase 2 | SARS-CoV-2 infection | Time to worsening of disease | [9] |
| Etoposide | Topoisomerase II | Inhibits DNA synthesis by forming a complex with topoisomerase II and DNA | United states | NCT04356690 | - | Active, not yet Recruting | Phase 2 | Confirmed COVID-19 infection | Change in pulmonary status | [9] |
| FN-B1A | Jak1 and Tyk2 | Jak1 and Tyk2 | UK | NCT04385095 | - | Recruiting | Phase 2 | COVID-19 infection | Clinical Improvement | [10] |
| Jak1 and Tyk2 | Several locations | NCT04315948 | Lopinavir, ritonavir | Active, not yet Recruiting | Phase 3 | COVID-19 infection | Percentage of subjects reporting severity | |||
| - | Iran | NCT04350671 | Hydroxychloroquine, lopinavir, ritonavir | Enrolling by invitation | Phase 4 | COVID-19 infection | Reduce Mortality | |||
| - | Irna | NCT04350684 | Hydroxychloroquine, lopinavir, ritonavir, umifenovir | Enrolling by invitation | Phase 4 | COVID-19 infection | Time to clinical improvement | |||
| - | Several locations | NCT02735707 | Multifactorial | Recruiting | Phase 4 | COVID-19 infection | All-cause mortality | |||
| Genistein | Inhibition of<break/>both transcription nuclear factor-κB (NF-κB) activation and chemokine-8 secretion | Triggers the ER stress through upregulation of glucose-regulated protein 78 (GRP78) expression | United statwa | NCT04482595 | - | Recruting | Phase 2 | Patients hospitalized for COVID-19 | Change in Diffusing capacity of the lungs for carbon monoxide | [9] |
| Ibrutinib | Inhibition of the Bruton tyrosine kinase | Protection against immune-induced lung injury | Yes (USA) | NCT04375397 | - | Active, not yet Recruiting | Phase 2 | Hospitalised patients with severe pneumonia | Respiratory failure-free survival rate, overall survival | [10] |
| NCT04439006 | - | Recruting | Phase 2 | Patients Requiring Hospitalization | Patients with diminished respiratory failure and death | |||||
| IFN | Jak1 and Tyk2 | Jak1 and Tyk2 | Canada | NCT04354259 | - | Recruiting | Phase 2 | COVID-19 infection | Negative SARS-CoV-2 RNA on nasopharyngeal swab | [10] |
| Jak1 and Tyk2 | Jak1 and Tyk2 | China | NCT04331899 | - | Active, Not yet recruiting | Phase 2 | COVID-19 infection | |||
| IFN beta 1b | Jak1 and Tyk2 | Jak1 and Tyk2 | Hong kong | NCT04647695 | Remdesivir | Recruiting | Phase 2 | high risk of clinical deterioration | Clinical improvement | [10] |
| NCT04494399 | ribavirin | Recruiting | Phase 2 | COVID-19 infection | Reduce hospitalisation | |||||
| IFN-A2B | activate two Jak (Janus kinase) tyrosine kinases (Jak1 and Tyk2) | activate two Jak (Janus kinase) tyrosine kinases (Jak1 and Tyk2) | United States | NCT04349410 | - | Completed | Phase 2/3 | CoVid-19 infection | Improvement in FMTVDM Measurement with nuclear imaging | [10] |
| NCT04379518 | - | Recruiting | Phase 1/2 | Patients with cancer and mild or moderate symptomatic infection | Incidence of adverse events | |||||
| IFN-B1A/B | Jak1 and Tyk2 | Jak1 and Tyk2 | Irnan | NCT04343768 | Hydroxychloroquine, lopinavir, ritonavir | Completed | Phase 2 | COVID-19 infection | Time to clinical improvement | [10] |
| IFN-B1B | Jak1 and Tyk2 | Jak1 and Tyk2 | Hong kong | NCT04350281 | Hydroxychloroquine, lopinavir, ritonavir | Completed | Phase 2 | COVID-19 infection | Time to negative NPS viral load | [10] |
| Jak1 and Tyk2 | Jak1 and Tyk2 | Hong kong | NCT04276688 | Ribavirin, lopinavir, ritonavir | Completed | Phase 2 | COVID-19 infection | Time to negative NPS | ||
| Imatinib | BCR/ABL kinase inhibition | Blockade of cell entry and endosomal trafficking | Yes (France, Spain and USA) | NCT04357613 | - | Not yet Recruitng | Phase 2 | Hospitalised patients | Rate of prevented severe disease worsening | [10] |
| Interferon | Jak1 and Tyk2 | Jak1 and Tyk2 | China | NCT04291729 | Danoprevir, ritonavir | Completed | Phase 4 | COVID-19 infectio | Rate of composite adverse outcome | [10] |
| Lenalidomide | Immunomodulatory agent | substrate specificity of the CRL4CRBN E3 ubiquitin ligase | Spain | NCT04361643 | - | Not yet recruting | Phase 4 | COVID-19 infection | Clinical improvement | [10] |
| Leronlimab | Disruption of the CCL5/RANTES-CCR5 pathway | Immune homeostasis restoration | Yes (USA) | NCT04343651 | - | Active, not recruitng | Phase 2 | Mild/moderate disease | Clinical improvement | [10] |
| NCT04347239 | - | Recruting | Phase 2 | Severe lung disease or critical disease | Overall survival | [10] | ||||
| Masitinib | directly binds to the active site of 3CLpro | Tyrosine kinase inhibitor | Yes (France) | NCT04622865 | Isoquercetin | Recrutiting | Phase 2 | COVID 19 diagnosis | Clinical status of patients at day-15 | [9] |
| Melphalan | anti-inflammatory response | Inhibition of DNA and RNA synthesis by realizing an alkylating peptide | Yes (Russian Federation) | NCT04380376 | - | Recrutiting | Phase 2 | COVID 19 diagnosis | The changes of COVID Ordinal Outcomes Scale | [9] |
| Methotrexate | Immunomodulatory agent | inhibition of folate dependent pathways leading to inhibition of DNA synthesis | France | NCT04481633 | Hydroxychloroquine | Recruiting | Not applicable | COVID-19 infection | Rate of patients with positive anti-COVID19 serology | [10] |
| Nasal IFN-A1B | Jak1 and Tyk2 | Jak1 and Tyk2 | China | NCT04320238 | Anti-thymosin | Recruiting | Phase 3 | Formally serving medical staff in Taihe Hospital | new-onset COVID-19 | [10] |
| Nivolumab | PD-1/PD-L1 pathway blockade | Immune homeostasis restoration | Yes (France and China) | NCT04343144 | - | Not yet recruiting | Phase 2 | Disease requiring O2-support | Time to clinical improvement | [10] |
| NCT04413838 | - | Not yet recruiting | Phase 2 | Obese individuals | Efficacy and safety | [10] | ||||
| NCT04356508 | - | Not yet recruiting | Phase 2 | Clinically stable patients with mild or moderate disease and asymptomatic patients | Viral clearance kinetics | [10] | ||||
| Opaganib | Inhibition of sphingosine kinase-2 | Anti-inflammatory and antiviral properties | Yes (Israel) | NCT04414618 | - | Completed | Phase 2 | Disease requiring O2-support | Measurement of the daily O2 requirements | [10] |
| NCT04467840 | - | Recruting | Phase 2 and 3 | Disease requiring O2-support | Reduce Intubation and mechanical ventilation | |||||
| NCT04435106 | - | Completed | - | severe COVID-19 who required oxygen support via high-flow nasal cannula | Measure the time to weaning from high-flow nasal cannula and | |||||
| Measure the time to breathing ambient | ||||||||||
| NCT04502069 | - | Withdrawn (To be replaced with a randomized placebo-controlled study.) | Phase 1 and 2 | Pneumonia Requiring Oxygen | Time to breathing room air | |||||
| PD-1 blocking antibody | PD-1 | Can prevent the tumor cell from binding PD-1 | Not provided | NCT04268537 | - | Not yet recruiting | Phase 2 | COVID-19 infection | lung injury score | [10] |
| Peg-IFN-L1 | Jak1 and Tyk2 | Jak1 and Tyk2 | United states | NCT04343976 | - | Enrolling by invitation | Phase 2 | COVID-19 infectio | Negative SARS-CoV-2 RNA on nasopharyngeal swab | [10] |
| Peg-IFN-L1A | Jak1 and Tyk2 | Jak1 and Tyk2 | United states | NCT04388709 | - | Withdrawn (Due to the number of competing trials at their site, the study team has closed enrollment and withdrawn this trial.) | Phase 2 | COVID-19 infection | Number of participants with resolution of hypoxia | [10] |
| United states | NCT04344600 | - | Not yet recruiting | Phase 2 | COVID-19 infection | Proportion of participants with no evidence of SARS-CoV-2 infection | ||||
| Pembrolizumab | PD-1/PD-L1 pathway blockade | Immune homeostasis restoration | Yes (Spain) | NCT04335305 | Tocilizumab | Recruiting | Phase 2 | Severe lung disease or critical disease | Percentage of patients with normalisation of SpO2 ≥96% on room air | [10] |
| Plitidepsin | Blockade of eEF1A | Interference with the viral cycle | Yes (Spain) | NCT04382066 | - | Completed | Phase 1 | Hospitalised patients | Frequency of occurrence of Grade 3 or higher AEs | [10] |
| Selinexor | Blockade of nucleocytoplasmic transport | Antiviral and anti-inflammatory properties | Yes (USA, France, Austria, Spain and United Kingdom) | NCT04355676 | - | Withdrawn (No participants enrolled) | Phase 2 | Hospitalised patients with moderate or severe disease | Percentage of participants with at least a two-point improvement in the ordinal scale | [10] |
| NCT04349098 | - | Completed | Phase 2 | Hospitalised patients with severe disease | Improvement | |||||
| NCT04534725 | - | Recruiting | Phase 3 | received cancer related treatment | COVID-19 Prevention and Treatment in Cancer | |||||
| SFX-01 | up-regulates the Nrf2 pathway | Up-regulates the Nrf2 pathway | UK + Evgen Pharma | - | - | Enrolment begins in July (results are expected in 2021) | Phase 2/3 | - | Efficacy at treating ARDS | [11] |
| Siltuximab | Interleukin-6 | Interleukin-6 | Spain | NCT04329650 | - | Recruiting | Phase 2 | Hospitalized patient | Proportion of patients requiring ICU admission at any time | [11] |
| Italy | NCT04322188 | - | Completed | - | COVID-19 infection | mortality in siltuximab treated patients | ||||
| Belgium | NCT04330638 | Anakinra | Active, not recruting | Phase 3 | COVID-19 infection | Time to Clinical Improvement | ||||
| Saudi Arabia | NCT04486521 | tocilizumab | Recruiting | - | COVID-19 infection | Ventilator-Free Days | ||||
| Tamoxifen | Decreased the PGE2 production | Compete with 17β-estradiol (E2) at the receptor site | Egypt | NCT04568096 | - | Not yet recruting | Phase 2 | Adult SARI patients with COVID-19 infection | Lung injury score | [9] |
| Tetrandrine | Ability to block the two-pore channel 2 (TPC2) | Checkpoint inhibitor of the cell cycle | China | NCT04308317 | - | Enrolling by invitation | Phase 4 | COVID-19 infection | Survival rate | [10] |
| Thalidomide | inhibition of inflammatory cytokine production | Inhibit the production of interleukin (IL)-6, | China | NCT04273529 | - | Not yet recruiting | Phase 2 | COVID-19 infection | Time to Clinical recovery | [10] |
| Toremifene | Interaction with coronavirus proteins | Inhibition of viral membranes fusion with host cell endosomes | ? (Not provided) | NCT04531748 | Melatonin | Withdrawn (Funding) | Phase 2 | - | Clinical improvement | [10] |
| Zanubrutinib | Inhibition of the Bruton tyrosine kinase | Protection against immune, lethal and sepsis-induced pulmonary injuries | Yes (USA) | NCT04382586 | - | Completed | Phase 2 | Disease requiring O2-support | Respiratory failure-free survival rate | [10] |
| Zotatifin | Blockade of eIF4A | Inhibition of protein biogenesis | No | NCT04632381 | - | Not yet recruiting | Phase 1 | - | - | [10] |
References
- Zheng, J. SARS-CoV-2: An Emerging Coronavirus that Causes a Global Threat. Int J Biol Sci. 2020, 16, 1678–1685, Published 15 March 2020. [Google Scholar] [CrossRef] [PubMed]
- Drinka, P.J. Influenza vaccination and antiviral therapy: Is there a role for concurrent administration in the institutionalised elderly? Drugs Aging 2003, 20, 165–174. [Google Scholar] [CrossRef] [PubMed]
- Deb, P.; Molla, M.A.; Saif-Ur-Rahman, K. An update to monoclonal antibody as therapeutic option against COVID-19. Biosaf. Health 2021. [Google Scholar] [CrossRef] [PubMed]
- Pushpakom, S.; Iorio, F.; Eyers, P.A.; Escott, K.J.; Hopper, S.; Wells, A.; Doig, A.; Guilliams, T.; Latimer, J.; McNamee, C.; et al. Drug repurposing: Progress, challenges and recommendations. Nat. Rev. Drug Discov. 2019, 18, 41–58. [Google Scholar] [CrossRef]
- Hernandez, J.J.; Pryszlak, M.; Smith, L.; Yanchus, C.; Kurji, N.; Shahani, V.M.; Molinski, S.V. Giving Drugs a Second Chance: Overcoming Regulatory and Financial Hurdles in Repurposing Approved Drugs As Cancer Therapeutics. Front Oncol. 2017, 7, 273. [Google Scholar] [CrossRef]
- Sultana, J.; Crisafulli, S.; Gabbay, F.; Lynn, E.; Shakir, S.; Trifirò, G. Challenges for drug repurposing in the COVID-19 pandemic era. Front. Pharmacol. 2020, 11, 1657. [Google Scholar] [CrossRef]
- Parvathaneni, V.; Gupta, V. Utilizing drug repurposing against COVID-19—Efficacy, limitations, and challenges. Life Sci. 2020, 259, 118275. [Google Scholar] [CrossRef] [PubMed]
- Saini, K.S.; Lanza, C.; Romano, M.; De Azambuja, E.; Cortes, J.; Heras, B.D.L.; De Castro, J.; Saini, M.L.; Loibl, S.; Curigliano, G.; et al. Repurposing anticancer drugs for COVID-19-induced inflammation, immune dysfunction, and coagulopathy. Br. J. Cancer 2020, 123, 694–697. [Google Scholar] [CrossRef]
- National Center for Advancing Translational Sciences|OpenData Portal. Available online: https://opendata.ncats.nih.gov/covid19/databrowser (accessed on 6 February 2021).
- ClinicalTrials.gov. Available online: https://www.clinicaltrials.gov/ct2/home (accessed on 6 February 2021).
- European Pharmaceutical Review|News. Available online: https://www.europeanpharmaceuticalreview.com/ (accessed on 6 February 2021).
- Richman, D.D.; Nathanson, N. Antiviral Therapy. Viral Pathog. 2016, 271–287. [Google Scholar] [CrossRef]
- Fehr, A.R.; Perlman, S. Coronaviruses: An overview of their replication and pathogenesis. Methods Mol. Biol. 2015, 1282, 1–23. [Google Scholar] [CrossRef]
- Astuti, I.; Ysrafil. Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2): An overview of viral structure and host response. Diabetes Metab. Syndr. 2020, 14, 407–412. [Google Scholar] [CrossRef]
- Romano, M.; Ruggiero, A.; Squeglia, F.; Maga, G.; Berisio, R.A. Structural View of SARS-CoV-2 RNA Replication Machinery: RNA Synthesis, Proofreading and Final Capping. Cells 2020, 9, 1267. [Google Scholar] [CrossRef]
- Zingaropoli, M.A.; Perri, V.; Pasculli, P.; Dezza, F.C.; Nijhawan, P.; Savelloni, G.; La Torre, G.; D’Agostino, C.; Mengoni, F.; Lichtner, M.; et al. Major reduction of NKT cells in patients with severe COVID-19 pneumonia. Clin. Immunol. 2021, 222, 108630. [Google Scholar] [CrossRef]
- Jin, Y.; Ji, W.; Yang, H.; Chen, S.; Zhang, W.; Duan, G. Endothelial activation and dysfunction in COVID-19: From basic mechanisms to potential therapeutic approaches. Signal. Transduct. Target. Ther. 2020, 5, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Boechat, J.L.; Chora, I.; Morais, A.; Delgado, L. The immune response to SARS-CoV-2 and COVID-19 immunopathology–current perspectives. Pulmonology 2021. [Google Scholar] [CrossRef] [PubMed]
- Minn, A.J. Interferons and the immunogenic effects of cancer therapy. Trends Immunol. 2015, 36, 725–737. [Google Scholar] [CrossRef] [PubMed]
- Lin, F.C.; Young, H.A. Interferons: Success in anti-viral immunotherapy. Cytokine Growth Factor Rev. 2014, 25, 369–376. [Google Scholar] [CrossRef]
- Hung, I.F.-N.; Lung, K.-C.; Tso, E.Y.-K.; Liu, R.; Chung, T.W.-H.; Chu, M.-Y.; Ng, Y.-Y.; Lo, J.; Chan, J.; Tam, A.R.; et al. Triple combination of interferon beta-1b, lopinavir–ritonavir, and ribavirin in the treatment of patients admitted to hospital with COVID-19: An open-label, randomised, phase 2 trial. Lancet 2020, 395, 1695–1704. [Google Scholar] [CrossRef]
- Abdolvahab, M.H.; Moradi-Kalbolandi, S.; Zarei, M.; Bose, D.; Majidzadeh, -A.K.; Farahmand, L. Potential role of interferons in treating COVID-19 patients. Int. Immunopharmacol. 2021, 90, 107171. [Google Scholar] [CrossRef]
- Costela-Ruiz, V.J.; Illescas-Montes, R.; Puerta-Puerta, J.M.; Ruiz, C.; Melguizo-Rodríguez, L. SARS-CoV-2 infection: The role of cytokines in COVID-19 disease. Cytokine Growth Factor Rev. 2020, 54, 62–75. [Google Scholar] [CrossRef]
- Lacroix, M.; Rousseau, F.; Guilhot, F.; Malinge, P.; Magistrelli, G.; Herren, S.; Jones, S.A.; Jones, G.W.; Scheller, J.; Lissilaa, R.; et al. Novel Insights into Interleukin 6 (IL-6) Cis- and Trans-signaling Pathways by Differentially Manipulating the Assembly of the IL-6 Signaling Complex. J. Biol. Chem. 2020, 290, 26943–26953. [Google Scholar] [CrossRef] [PubMed]
- Khan, F.A.; Stewart, I.; Fabbri, L.; Moss, S.; Robinson, K.; Smyth, A.R.; Jenkins, G. Systematic review and meta-analysis of anakinra, sarilumab, siltuximab and tocilizumab for COVID-19. Thorax 2021. [Google Scholar] [CrossRef]
- Sullivan, R.J.; Johnson, D.B.; Rini, B.; Neilan, T.G.; Lovly, C.M.; Moslehi, J.J.; Reynolds, K.L. COVID-19 and immune checkpoint inhibitors: Initial considerations. J. Immunother. Cancer 2020, 8. [Google Scholar] [CrossRef]
- Chen, Z.; Wherry, E.J. T cell responses in patients with COVID-19. Nat. Rev. Immunol. 2020, 20, 529–536. [Google Scholar] [CrossRef]
- Saito, N.; Yoshida, K.; Okamoto, M.; Sasaki, J.; Kuroda, C.; Ishida, H.; Ueda, K.; Ideta, H.; Kamanaka, T.; Sobajima, A.; et al. Anti-PD-1 antibody decreases tumour-infiltrating regulatory T cells. BMC Cancer 2019, 20. [Google Scholar] [CrossRef]
- Mollica, V.; Rizzo, A.; Massari, F. The pivotal role of TMPRSS2 in coronavirus disease 2019 and prostate cancer. Future Oncol. 2020, 16, 2029–2033. [Google Scholar] [CrossRef]
- Chakravarty, D.; Nair, S.S.; Hammouda, N.; Ratnani, P.; Gharib, Y.; Wagaskar, V.; Mohamed, N.; Lundon, D.; Dovey, Z.; Kyprianou, N.; et al. Sex differences in SARS-CoV-2 infection rates and the potential link to prostate cancer. Commun. Biol. 2020, 3, 1–12. [Google Scholar] [CrossRef]
- Martin, W.R.; Cheng, F. Repurposing of FDA-Approved Toremifene to Treat COVID-19 by Blocking the Spike Glycoprotein and NSP14 of SARS-CoV-2. J. Proteome Res. 2020, 19, 4670–4677. [Google Scholar] [CrossRef]
- Cheng, F.; Rao, S.; Mehra, R. COVID-19 treatment: Combining anti-inflammatory and antiviral therapeutics using a network-based approach. Cleve Clin. J. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- White, K.M.; Rosales, R.; Yildiz, S.; Kehrer, T.; Miorin, L.; Moreno, E.; Jangra, S.; Uccellini, M.B.; Rathnasinghe, R.; Coughlan, L.; et al. Plitidepsin has potent preclinical efficacy against SARS-CoV-2 by targeting the host protein eEF1A. Science 2021, 926–931. [Google Scholar] [CrossRef] [PubMed]
- Nebigil, C.G.; Moog, C.; Vagner, S.; Benkirane-Jessel, N.; Smith, D.R.; Désaubry, L. Flavaglines as natural products targeting eIF4A and prohibitins: From traditional Chinese medicine to antiviral activity against coronaviruses. Eur. J. Med. Chem. 2020, 203, 112653. [Google Scholar] [CrossRef] [PubMed]
- Sriskantharajah, S.; Hamblin, N.; Worsley, S.; Calver, A.R.; Hessel, E.M.; Amour, A. Targeting phosphoinositide 3-kinase δ for the treatment of respiratory diseases. Ann. N. Y. Acad. Sci. 2013, 1280, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Murdaca, G.; Pioggia, G.; Negrini, S. Vitamin D and Covid-19: An update on evidence and potential therapeutic implications. Clin. Mol. Allergy 2020, 18, 1–8. [Google Scholar] [CrossRef]
- Gordon, D.E.; Jang, G.M.; Bouhaddou, M.; Xu, J.; Obernier, K.; White, K.M.; O’Meara, M.J.; Rezelj, V.V.; Guo, J.Z.; Swaney, D.L.; et al. A SARS-CoV-2 protein interaction map reveals targets for drug repurposing. Nature 2020, 583, 459–468. [Google Scholar] [CrossRef] [PubMed]
- Repurposed Drugs with Broad-Spectrum Antiviral Activity, by BioRender.com. Available online: https://app.biorender.com/biorender-templates (accessed on 3 January 2020).

| Anticancer Drug | Viral—Host Targets | Mechanism of Action | Combination | Primary End-Point | Source (20 May 2021) |
|---|---|---|---|---|---|
| IFN | Jak1 and Tyk2 | Jak1 and Tyk2 | - | Negative SARS-CoV-2 RNA on a nasopharyngeal swab | [10] |
| Jak1 and Tyk2 | Jak1 and Tyk2 | - | |||
| IFN-B1A | Jak1 and Tyk2 | Jak1 and Tyk2 | - | Clinical Improvement | [10] |
| Jak1 and Tyk2 | Lopinavir, ritonavir | Percentage of subjects reporting severity | |||
| Hydroxychloroquine, lopinavir, ritonavir | Reduce Mortality | ||||
| Hydroxychloroquine, lopinavir, ritonavir, umifenovir | Time to clinical improvement | ||||
| Multifactorial | All-cause mortality | ||||
| IFN beta 1b | Jak1 and Tyk2 | Jak1 and Tyk2 | Remdesivir | Clinical improvement | [10] |
| ribavirin | Reduce hospitalisation | ||||
| IFN-A2B | activate two Jak (Janus kinase) tyrosine kinases (Jak1 and Tyk2) | activate two Jak (Janus kinase) tyrosine kinases (Jak1 and Tyk2) | - | Improvement in FMTVDM Measurement with nuclear imaging | [10] |
| - | Incidence of adverse events | ||||
| IFN-B1A/B | Jak1 and Tyk2 | Jak1 and Tyk2 | Hydroxychloroquine, lopinavir, ritonavir | Time to clinical improvement | [10] |
| IFN-B1B | Jak1 and Tyk2 | Jak1 and Tyk2 | Hydroxychloroquine, lopinavir, ritonavir | Time to negative NPS viral load | [10] |
| Jak1 and Tyk2 | Jak1 and Tyk2 | Ribavirin, lopinavir, ritonavir | Time to negative NPS |
| Anticancer Drug | Viral—Host Targets | Mechanism of Action | Combination | Primary End-Point | Source (20 May 2021) |
|---|---|---|---|---|---|
| Thalido-mide | Inhibition of inflammatory cytokine production | Inhibit the producti-on of interleukin (IL)-6 | - | Time to clinical recovery | [10] |
| Siltuximab | Interleukin-6 | Interleukin-6 | - | The proportion of patients Requiring ICU admission at any time | |
| - | Mortality in siltuximab treated patients | [11] | |||
| Anakinra | Time to clinical improvement | ||||
| tocilizumab | Ventilator-free days |
| Anticancer Drug | Viral—Host Targets | Mechanism of Action | Combination | Primary End-Point | Source (20 May 2021) |
|---|---|---|---|---|---|
| PD-1 blocking antibody | PD-1 | Can prevent the tumor cell from binding PD-1 | - | Lung injury score | [10] |
| Nivolumab | PD-1/PD-L1 pathway blockade | Immune homeostasis restoration | - | Time to clinical improvement | [10] |
| - | Efficacy and safety | [10] | |||
| - | Viral clearance kinetics | [10] | |||
| Pembrolizumab | PD-1/PD-L1 pathway blockade | Immune homeostasis restoration | Tocilizumab | Percentage of patients with the normalisation of SpO2 ≥96% in room air | [10] |
| Anticancer Drug | Viral—Host Targets | Mechanism of Action | Combination | Primary End-Point | Source (6 February 2021) |
|---|---|---|---|---|---|
| Bicalutami-de | Downregulates TMPRSS2 | Binding of androgen receptor | - | COVID-19 symptom relief | [9] |
| Camostat | Reduce number of participants requiring hospitalization | ||||
| Enzalutami-de | Reduce androgen driven morbidity in COVID-19 | Competitive binder of androgens | - | Time to worsening of disease | [9] |
| Toremifene | Interaction with coronavirus proteins | Inhibition of viral membranes fusion with Host cell endosomes | Melatonin | Clinical improvement | [10] |
| Tamoxifen | Decreased the PGE2 production | Compete with 17β-estradiol (E2) at the receptor site | - | Lung injury score | [9] |
| Anticancer Drug | Viral—Host Targets | Mechanism of Action | Combination | Primary End-Point | Source (20 May 2021) |
|---|---|---|---|---|---|
| Plitidepsin | Blockade of eEF1A | Interference with the viral cycle | - | Frequency of occurrence of Grade 3 or higher AEs | [10] |
| Zotatifin | Blockade of eIF4A | Inhibition of protein biogenesis | - | – | [10] |
| Anticancer Drug | Viral—Host Targets | Mechanism of Action | Combination | Primary End-Point | Source (20 May 2021) |
|---|---|---|---|---|---|
| Duvelisib | PI3K inhibition | Immune homeostasis restoration and viral replication inhibition | - | Overall survival | [10] |
| - | Reduce overall necessity of ventilation | ||||
| Zanubrutinib | Inhibition of the Bruton tyrosine kinase | Protection against immune, lethal and sepsis-induced pulmonary injuries | - | The respiratory failure-free survival rate | [10] |
| Carrimycin | Inhibit the replication of SARS-CoV-2 in the cells | Inhibits mTOR pathway | - | Fever to normal time | [11] |
| - | Percentage of patients alive without the need for supplemental oxygen and ongoing in patient-medical care | ||||
| Ibrutinib | Inhibition of the Bruton tyrosine kinase | Protection against immune-induced lung injury | - | The respiratory failure-free survival rate, overall survival | [10] |
| - | Patients with diminished respiratory failure and death |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costa, B.; Vale, N. A Review of Repurposed Cancer Drugs in Clinical Trials for Potential Treatment of COVID-19. Pharmaceutics 2021, 13, 815. https://doi.org/10.3390/pharmaceutics13060815
Costa B, Vale N. A Review of Repurposed Cancer Drugs in Clinical Trials for Potential Treatment of COVID-19. Pharmaceutics. 2021; 13(6):815. https://doi.org/10.3390/pharmaceutics13060815
Chicago/Turabian StyleCosta, Bárbara, and Nuno Vale. 2021. "A Review of Repurposed Cancer Drugs in Clinical Trials for Potential Treatment of COVID-19" Pharmaceutics 13, no. 6: 815. https://doi.org/10.3390/pharmaceutics13060815
APA StyleCosta, B., & Vale, N. (2021). A Review of Repurposed Cancer Drugs in Clinical Trials for Potential Treatment of COVID-19. Pharmaceutics, 13(6), 815. https://doi.org/10.3390/pharmaceutics13060815