
Constant Voltage Iontophoresis Technique to Deliver Terbinafine via Transungual Delivery System: Formulation Optimization Using Box–Behnken Design and In Vitro Evaluation

 , ,
, ,  , , ,
, , ,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Materials
2.2. High-Performance Liquid Chromatography (HPLC)
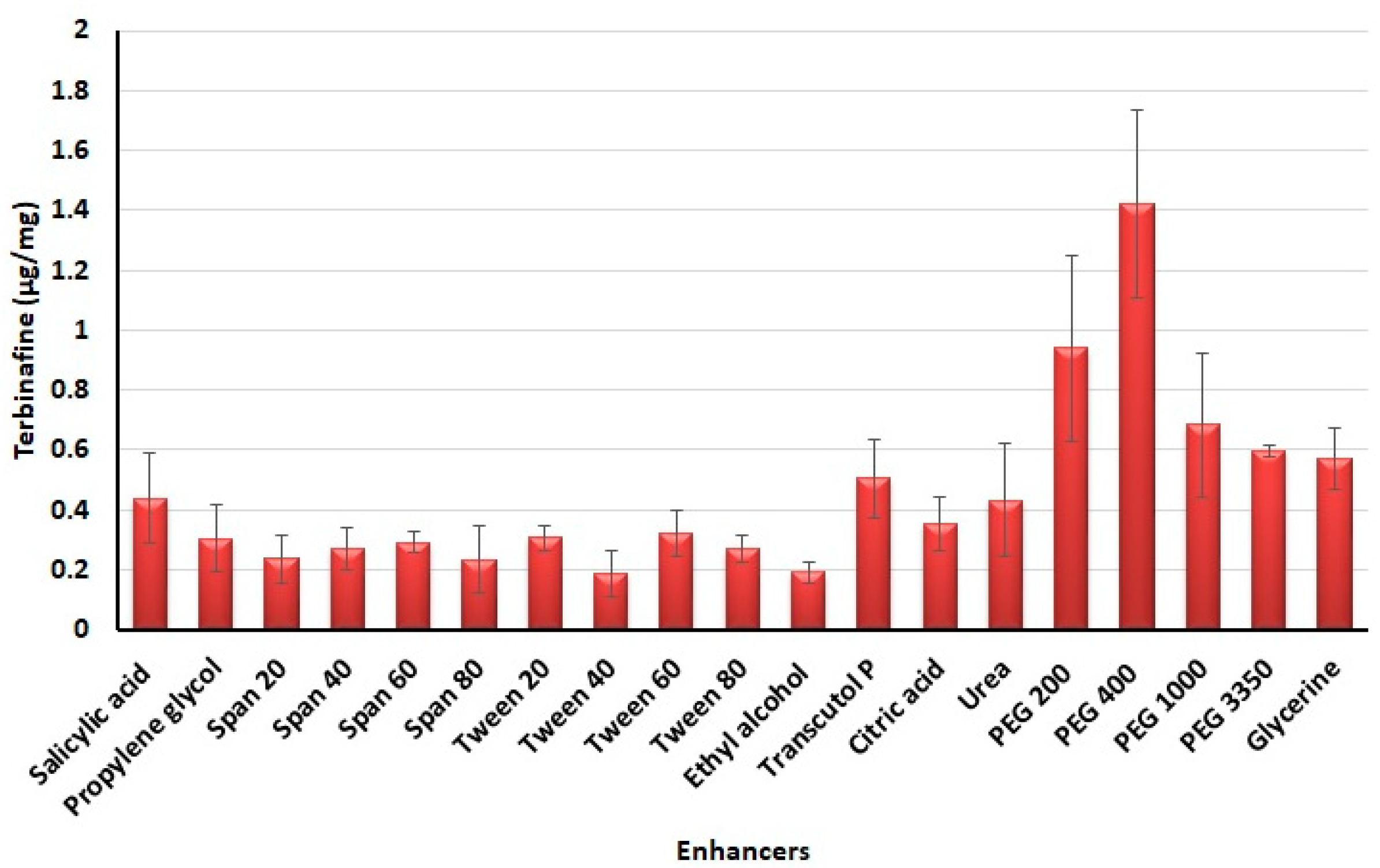
2.3. Screening of Chemical Enhancers
2.4. Preparation of Preliminary Batches
Iontophoresis Study
- Batch T4a: Applied voltage is 6V and duration of 3 h
- Batch T4b: Applied voltage is 6V and duration of 6 h
- Batch T4c: Applied voltage is 12V and duration of 3 h and
- Batch T4d: Applied voltage is 12V and duration of 6 h.
2.5. Experimental Design
2.6. Characterization of Preliminary Formulation
2.6.1. Appearance and pH
2.6.2. Drug Loading Percentage and Loading Efficacy Percentage
2.6.3. Viscosity
2.7. In Vitro Permeation Studies
2.7.1. Passive Permeation
2.7.2. Iontophoresis
2.8. Drug Accumulation into the Nail Tissue
2.9. Characterization of Optimized Formulation
2.9.1. Fourier Transform Infrared (FTIR)
2.9.2. Differential Scanning Calorimetry (DSC)
2.9.3. Field Emission Scanning Electron Microscope
2.10. Drug Release from Nail
2.11. Antifungal Activity
2.12. Stability
2.13. Data Analysis
3. Results and Discussion
3.1. Selection of Chemical Enhancers
3.2. Preliminary Studies
3.3. Optimization Study
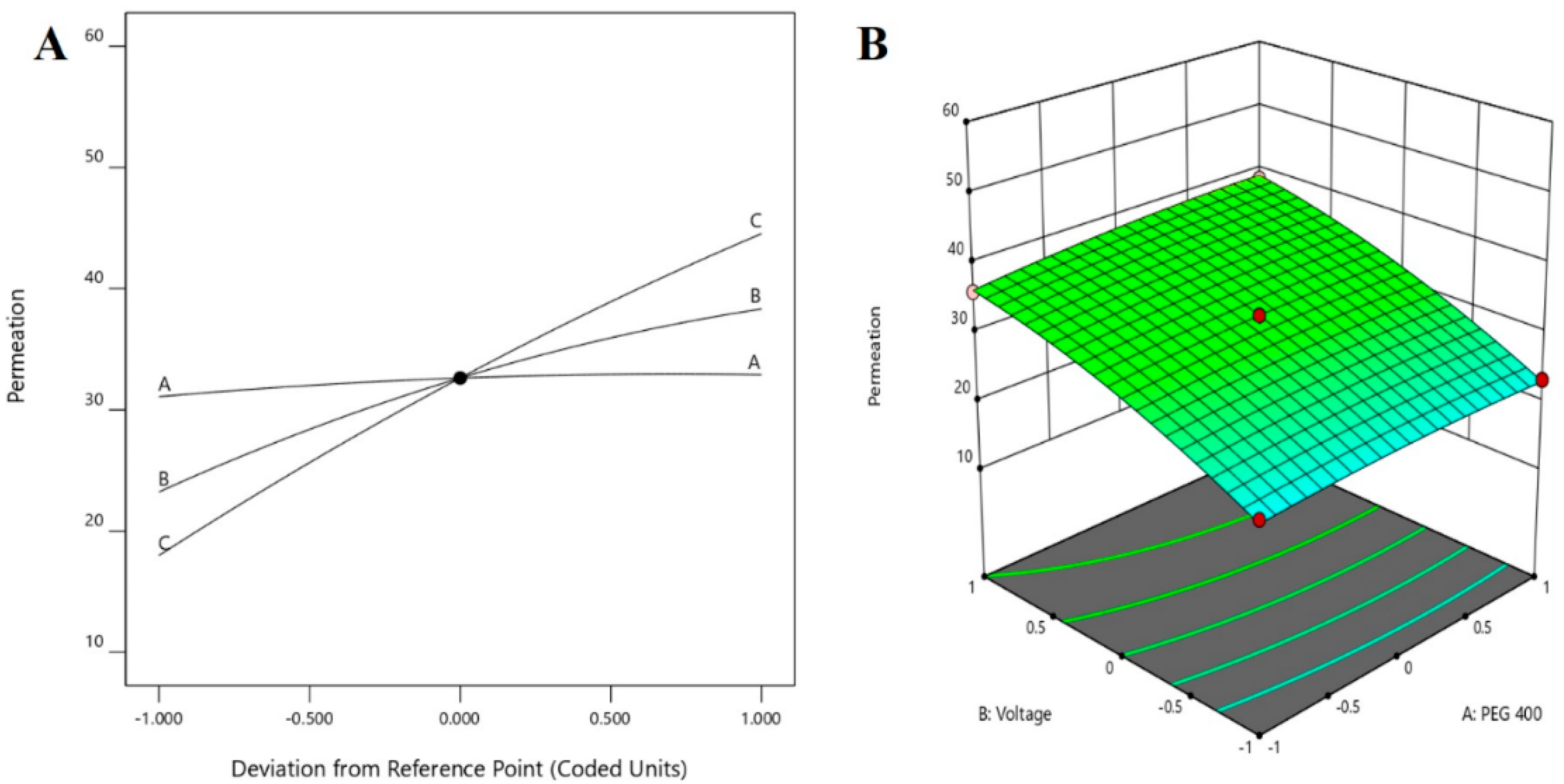
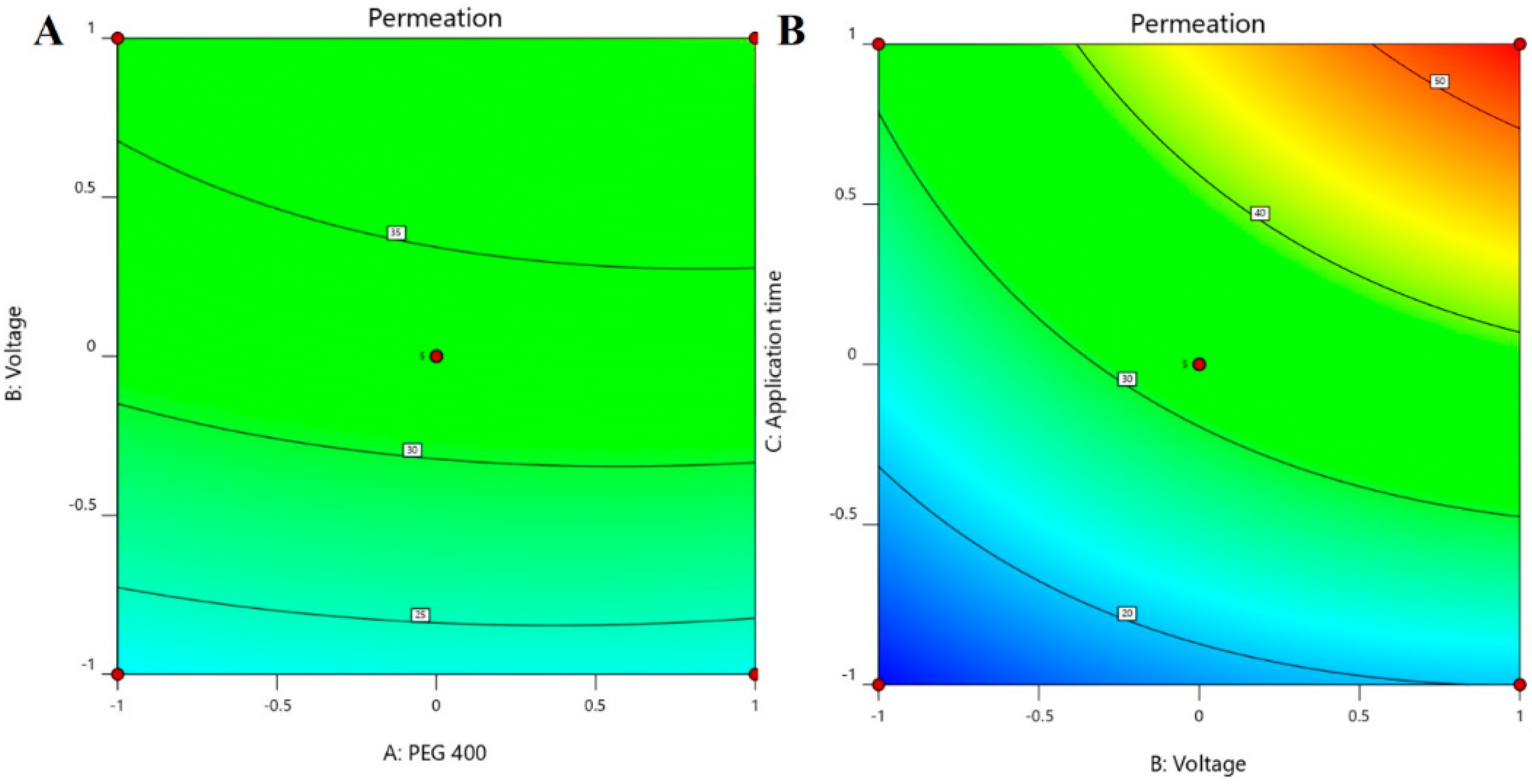
3.3.1. Influence of Independent Variables on Permeation
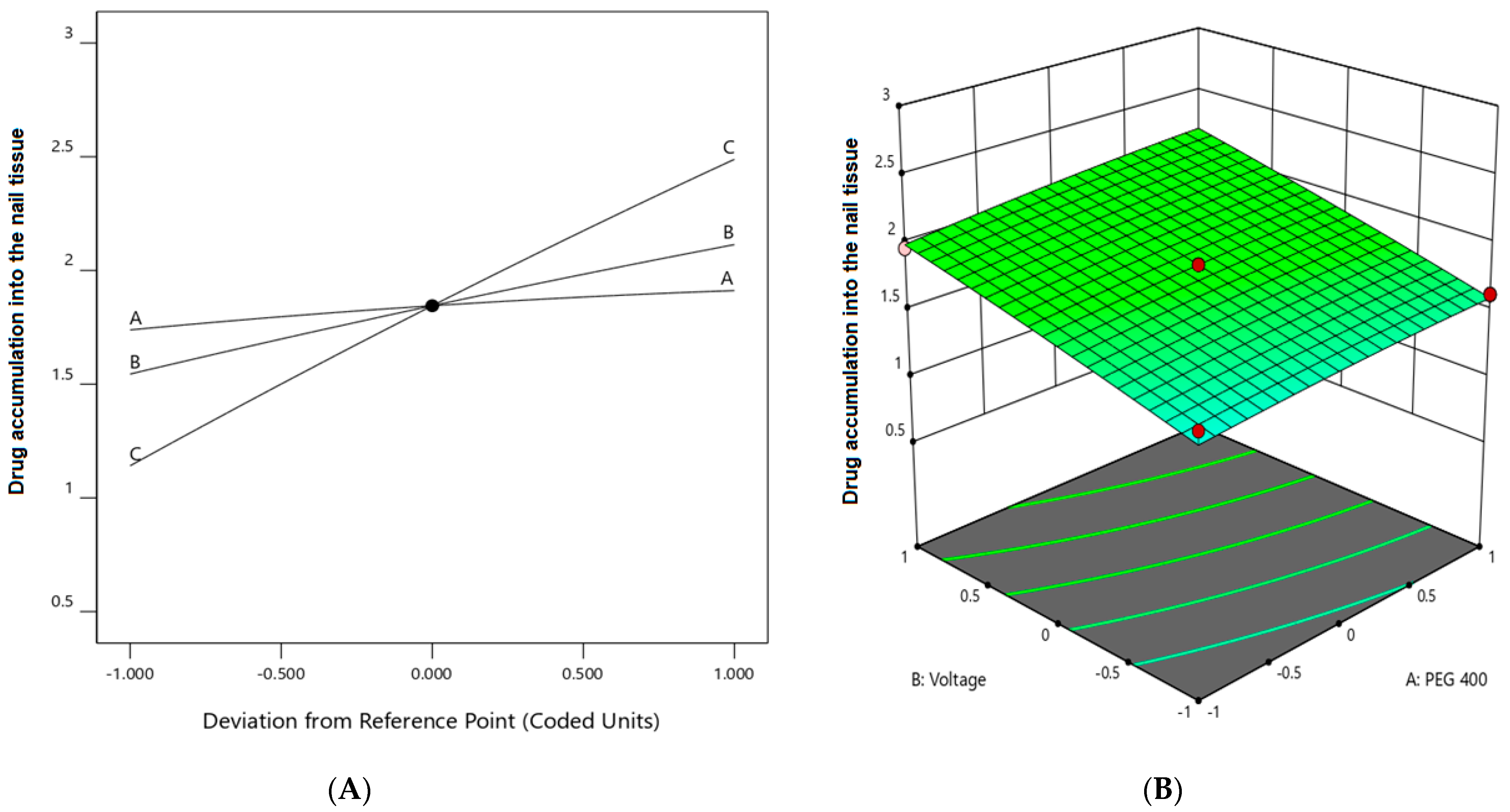
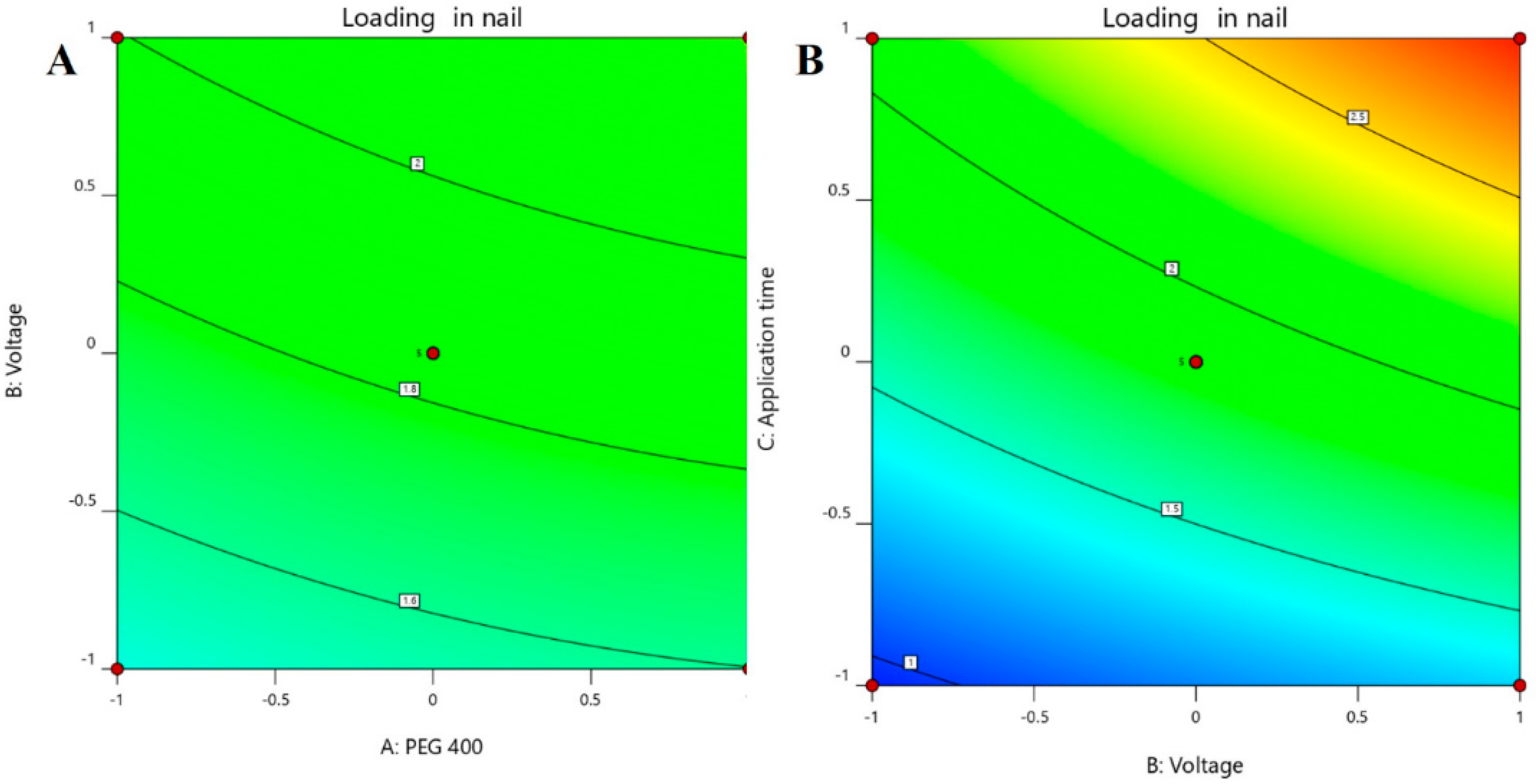
3.3.2. Effect of Independent Variables on Drug Accumulation on the Nails
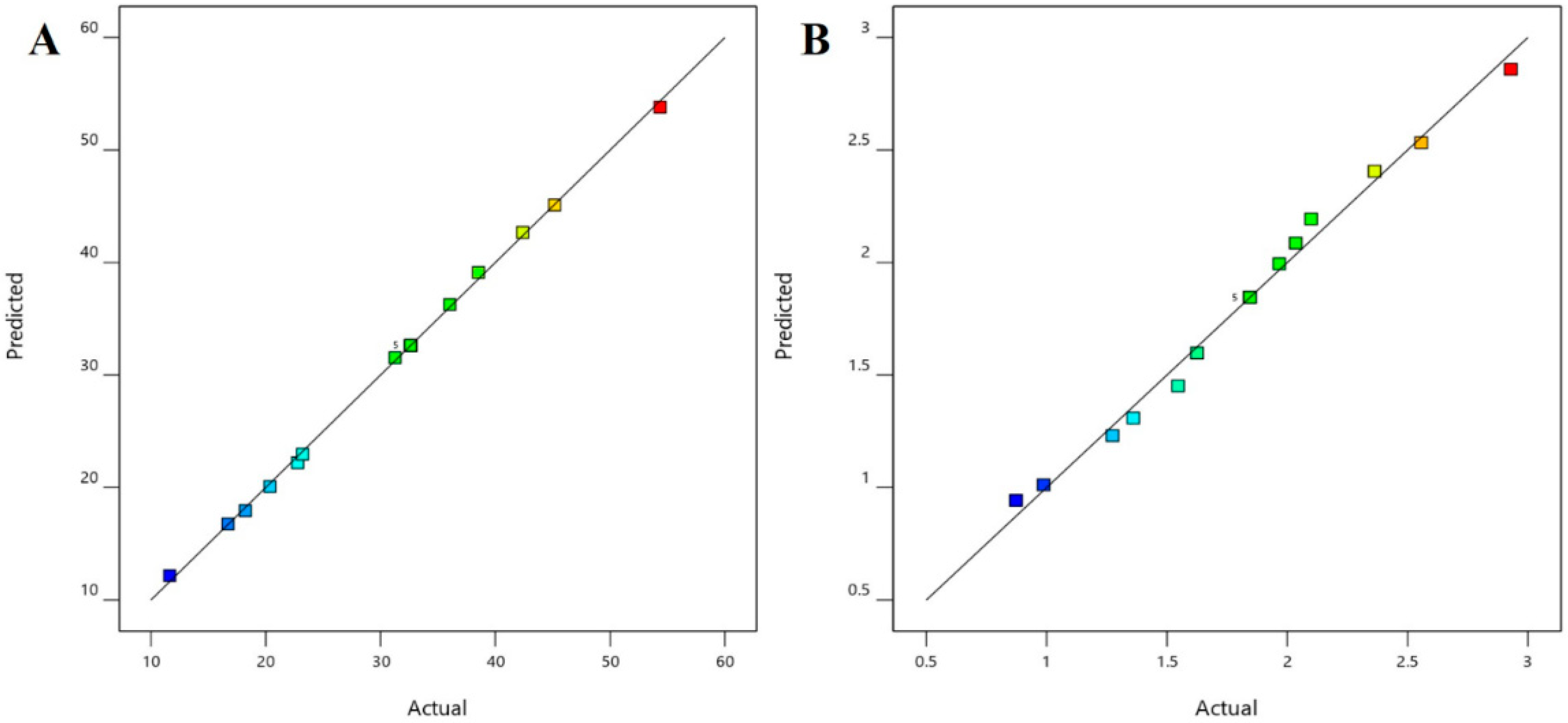
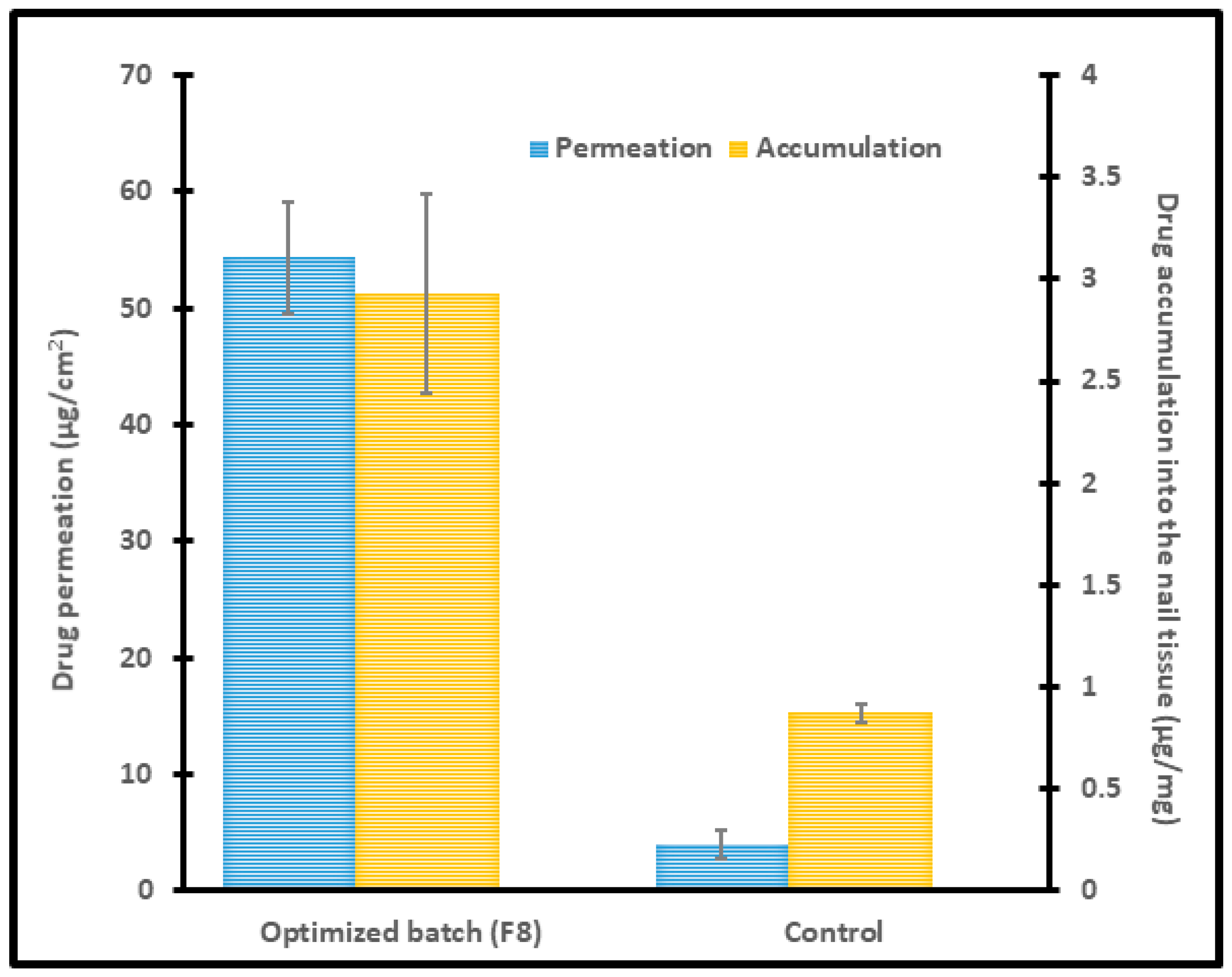
3.3.3. Optimization and Validation
3.4. Characterization of Optimized formulation
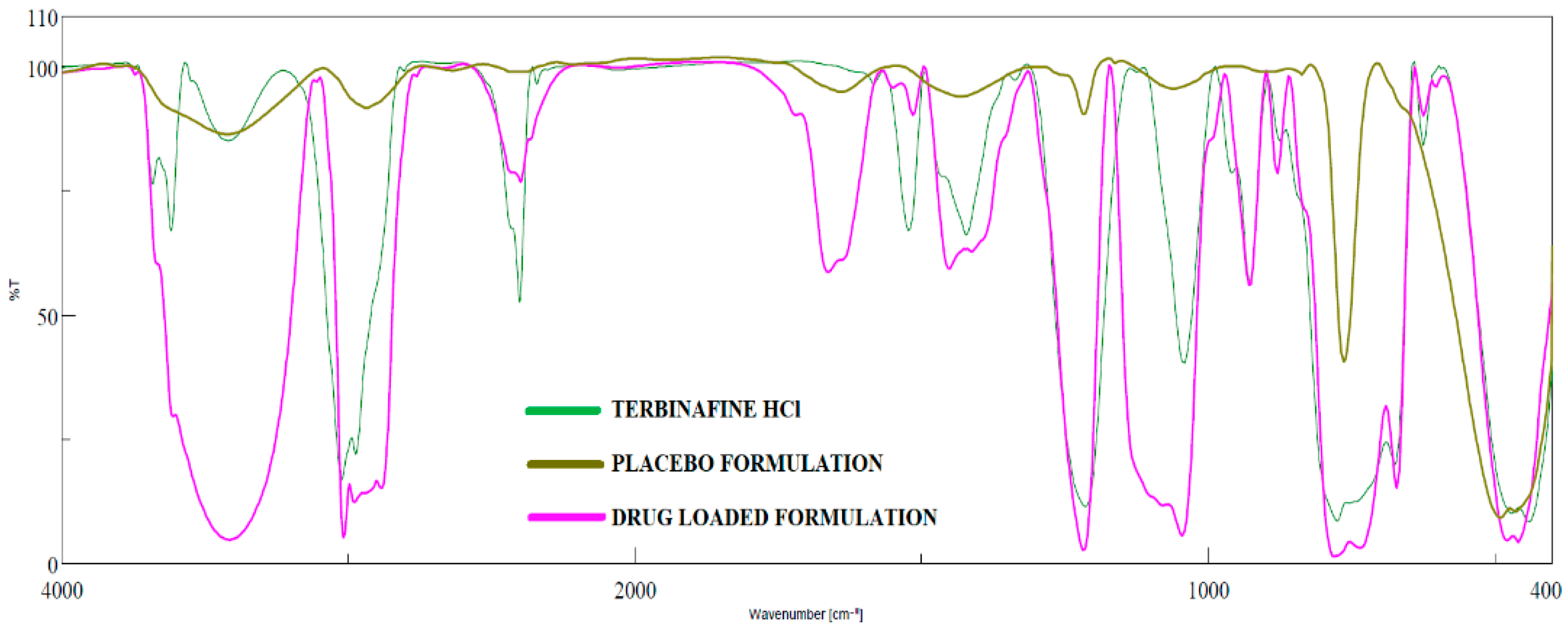
3.4.1. FTIR
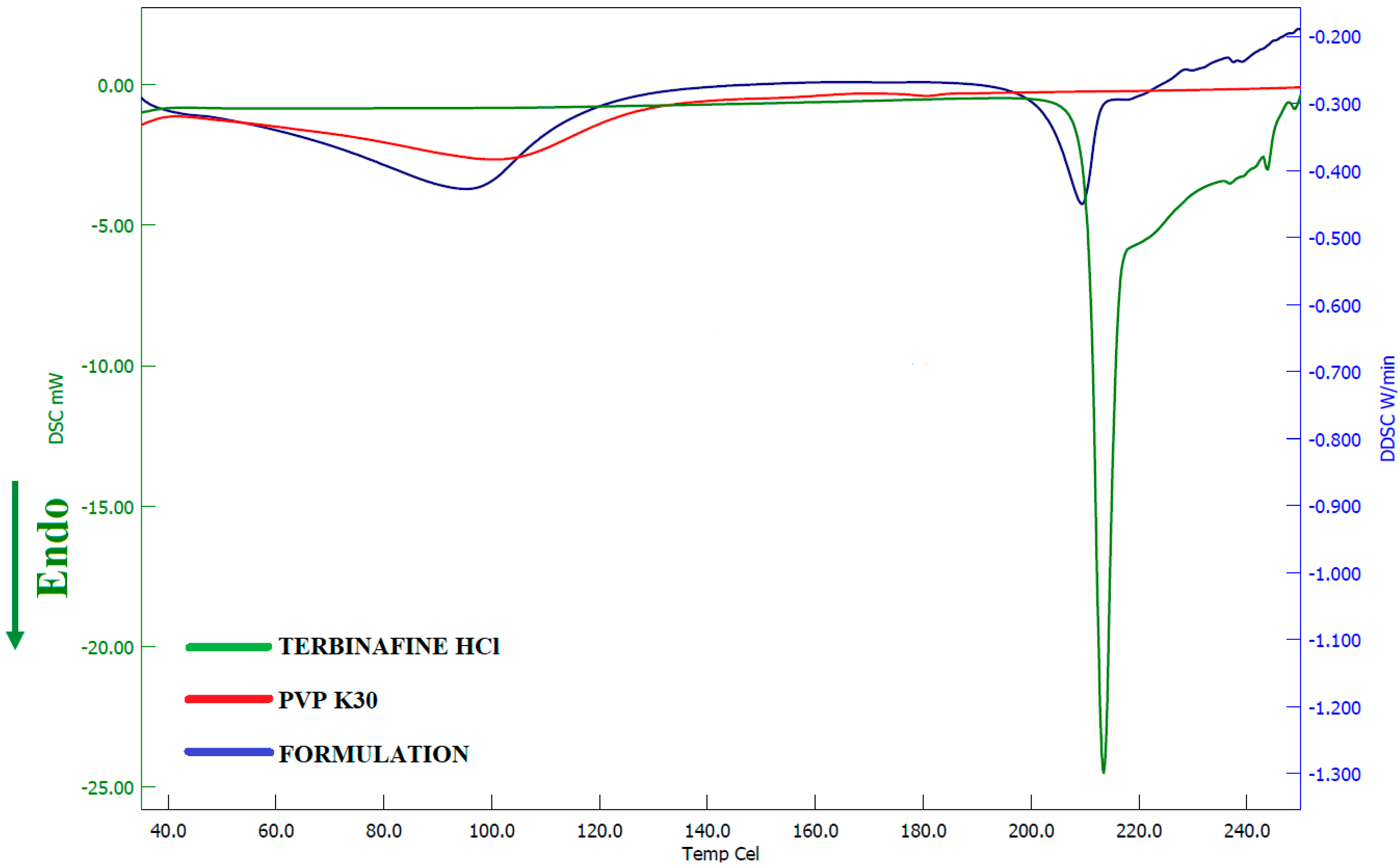
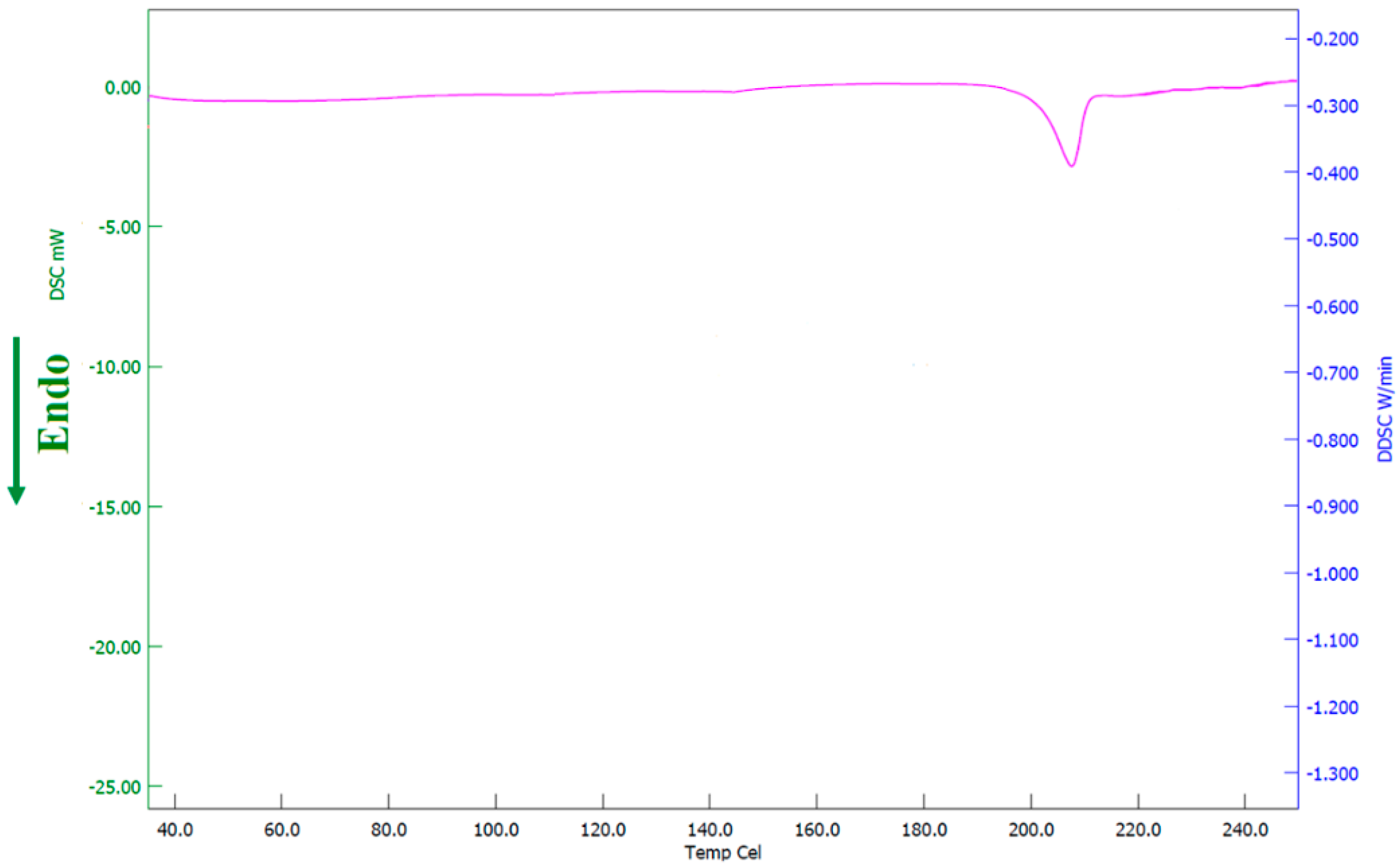
3.4.2. DSC
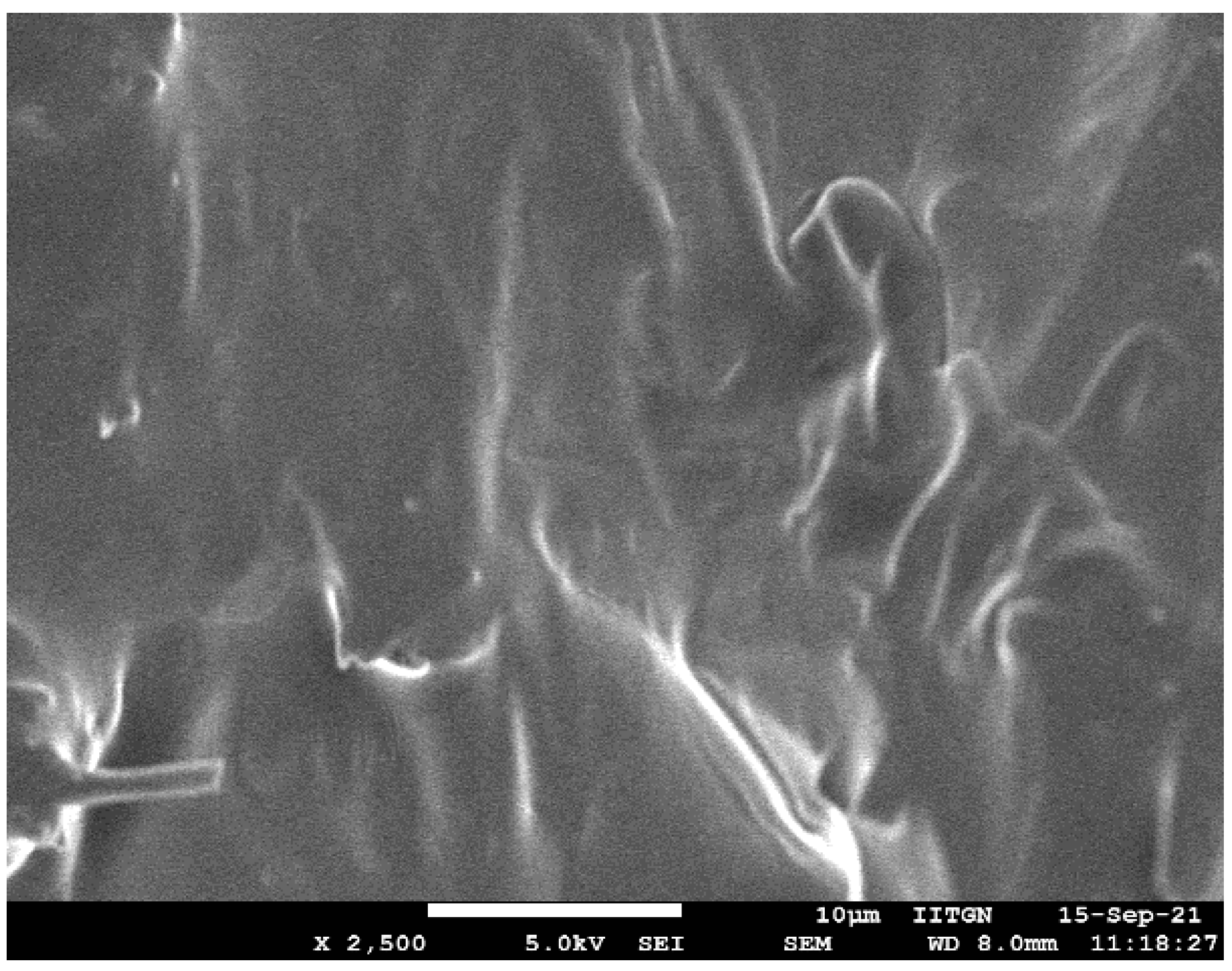
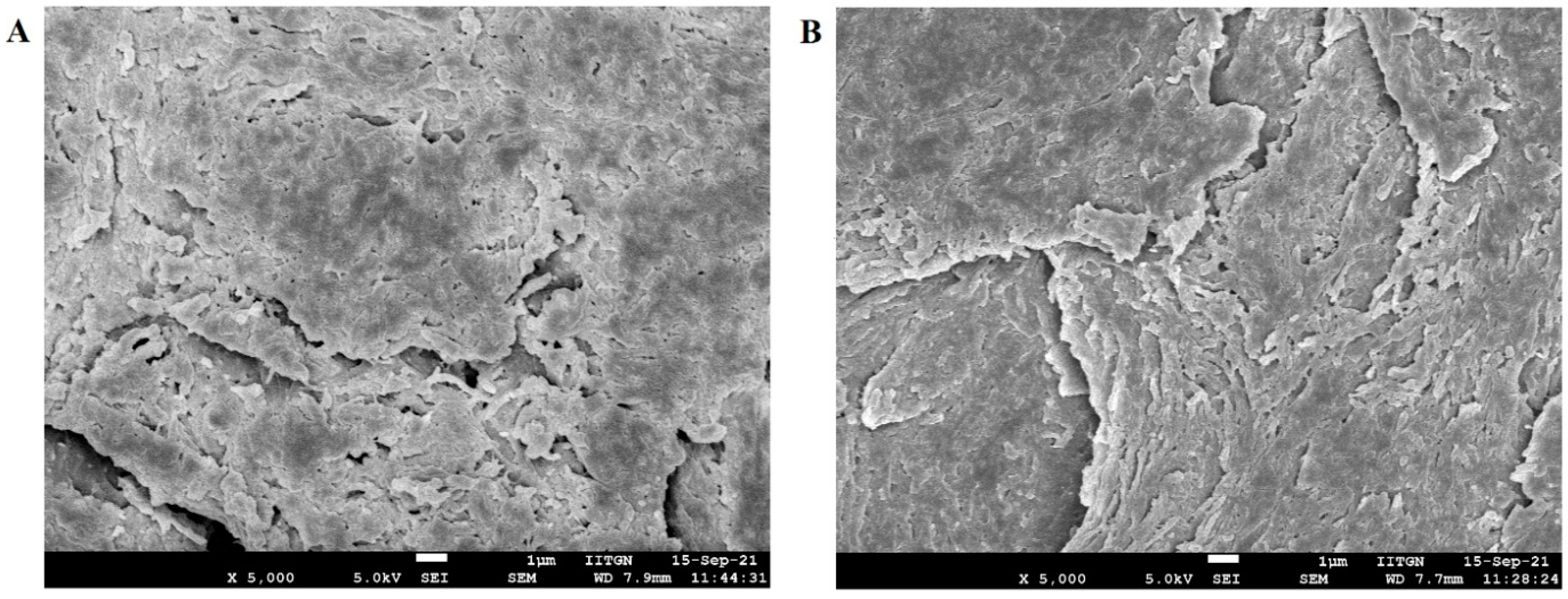
3.4.3. SEM
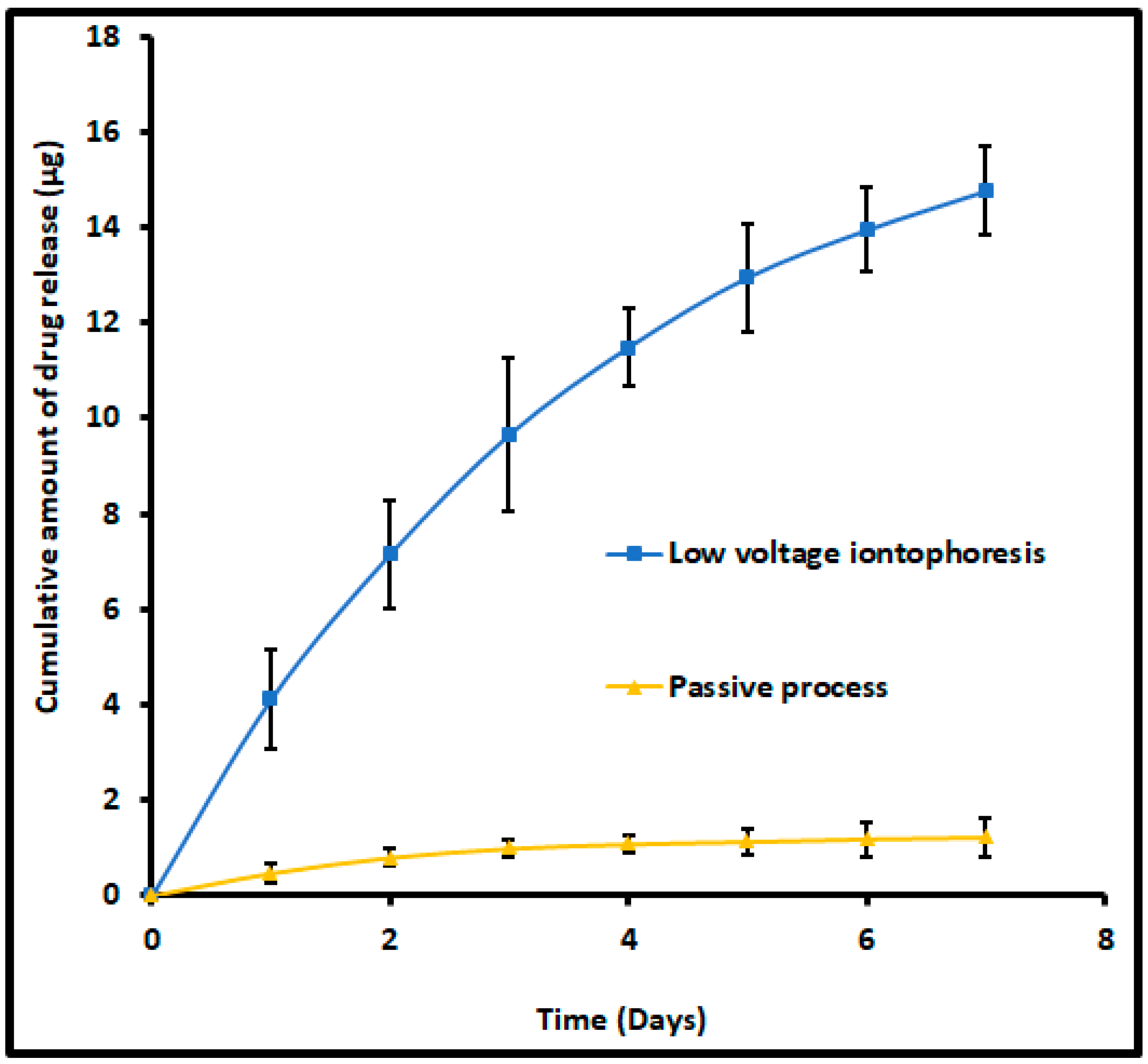
3.5. Drug Release from Nail
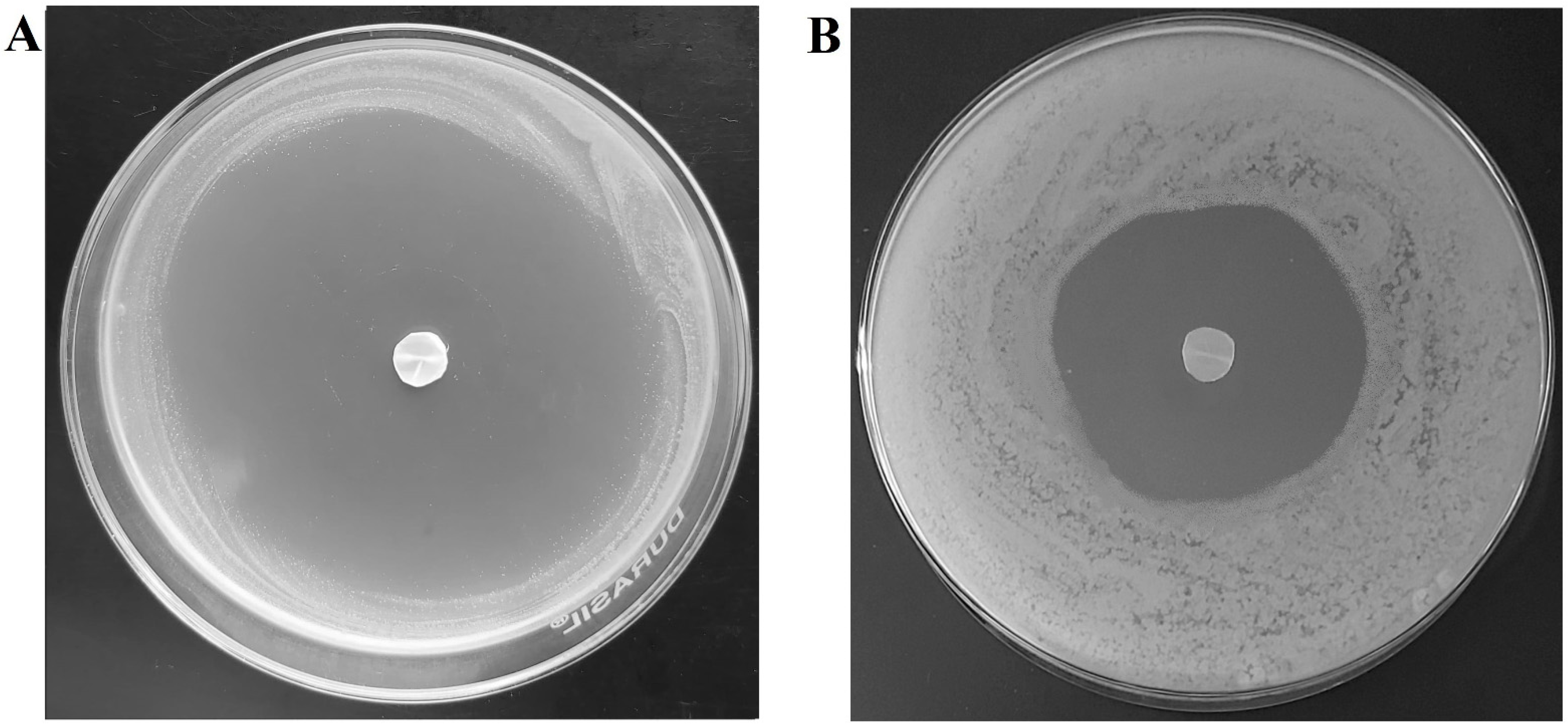
3.6. Antifungal Activity
3.7. Stability
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aggarwal, R.; Targhotra, M.; Kumar, B.; Sahoo, P.K.; Chauhan, M.K. Treatment and management strategies of onychomycosis. J. Mycol. Med. 2020, 30, 100949. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.K.; Stec, N.; Summerbell, R.C.; Shear, N.H.; Piguet, V.; Tosti, A.; Piraccini, B.M. Onychomycosis: A review. J. Eur. Acad. Dermatol. Venereol. JEADV 2020, 34, 1972–1990. [Google Scholar] [CrossRef] [PubMed]
- Aslam, R.; Hussain, T.; Yousaf, A.M.; Ghori, M.U.; Khan, I.U.; Rizvi, S.A.A.; Shahzad, Y. Onychomycosis: Current Understanding and Strategies for Enhancing Drug Delivery into Human Nail Tissue. Curr. Drug Res. Rev. 2021, 13, 25–35. [Google Scholar] [CrossRef]
- Elewski, B.E.; Tosti, A. Risk Factors and Comorbidities for Onychomycosis: Implications for Treatment with Topical Therapy. J. Clin. Aesthetic Dermatol. 2015, 8, 38–42. [Google Scholar]
- Christenson, J.K.; Peterson, G.M.; Naunton, M.; Bushell, M.; Kosari, S.; Baby, K.E.; Thomas, J. Challenges and Opportunities in the Management of Onychomycosis. J. Fungi 2018, 4, 87. [Google Scholar] [CrossRef]
- Lipner, S.R.; Scher, R.K. Onychomycosis: Clinical overview and diagnosis. J. Am. Acad. Dermatol. 2019, 80, 835–851. [Google Scholar] [CrossRef]
- Leung, A.K.C.; Lam, J.M.; Leong, K.F.; Hon, K.L.; Barankin, B.; Leung, A.A.M.; Wong, A.H.C. Onychomycosis: An Updated Review. Recent Pat. Inflamm. Allergy Drug Discov. 2020, 14, 32–45. [Google Scholar] [CrossRef] [PubMed]
- Silva-Neves, V.; Hugo, V.; Alves, P.; Amado, J.C.; Pais-Vieira, C.; Sousa, F.; Cerqueira, F.; Pinto, E.; Pais-Vieira, M. Quality of life and therapeutic regimen management in onychomycosis patients and in vitro study of antiseptic solutions. Sci. Rep. 2021, 11, 12789. [Google Scholar] [CrossRef]
- Gupta, A.K.; Stec, N. Recent advances in therapies for onychomycosis and its management. F1000Research 2019, 8. [Google Scholar] [CrossRef]
- Kreijkamp-Kaspers, S.; Hawke, K.; Guo, L.; Kerin, G.; Bell-Syer, S.E.; Magin, P.; Bell-Syer, S.V.; van Driel, M.L. Oral antifungal medication for toenail onychomycosis. Cochrane Database Syst. Rev. 2017, 7, Cd010031. [Google Scholar] [CrossRef]
- Shanbhag, P.P.; Jani, U. Drug delivery through nails: Present and future. New Horiz. Transl. Med. 2017, 3, 252–263. [Google Scholar] [CrossRef]
- Khoza, S.; Moyo, I.; Ncube, D. Comparative Hepatotoxicity of Fluconazole, Ketoconazole, Itraconazole, Terbinafine, and Griseofulvin in Rats. J. Toxicol. 2017, 2017, 6746989. [Google Scholar] [CrossRef] [PubMed]
- Kreutz, T.; de Matos, S.P.; Koester, L.S. Recent Patents on Permeation Enhancers for Drug Delivery Through Nails. Recent Pat. Drug Deliv. Formul. 2019, 13, 203–218. [Google Scholar] [CrossRef] [PubMed]
- Elsayed, M.M. Development of topical therapeutics for management of onychomycosis and other nail disorders: A pharmaceutical perspective. J. Control. Release Off. J. Control. Release Soc. 2015, 199, 132–144. [Google Scholar] [CrossRef] [PubMed]
- Angelo, T.; Borgheti-Cardoso, L.N.; Gelfuso, G.M.; Taveira, S.F.; Gratieri, T. Chemical and physical strategies in onychomycosis topical treatment: A review. Med. Mycol. 2017, 55, 461–475. [Google Scholar] [CrossRef]
- Kawa, N.; Lee, K.C.; Anderson, R.R.; Garibyan, L. ONYCHOMYCOSIS: A Review of New and Emerging Topical and Device-based Treatments. J. Clin. Aesthetic Dermatol. 2019, 12, 29–34. [Google Scholar]
- Elkeeb, R.; Hui, X.; Murthy, N.; Maibach, H.I. Emerging topical onychomycosis therapies—Quo vadis? Expert Opin. Emerg. Drugs 2014, 19, 489–495. [Google Scholar] [CrossRef]
- Souza, A.M.S.; Ribeiro, R.C.A.; Pinheiro, G.; Pinheiro, F.I.; Oliveira, W.N.; Souza, L.; Silva, A.L.; Amaral-Machado, L.; Alencar, É.N.; Chaves, G.M.; et al. Polishing the Therapy of Onychomycosis Induced by Candida spp.: Amphotericin B-Loaded Nail Lacquer. Pharmaceutics 2021, 13, 784. [Google Scholar] [CrossRef]
- Dhamoon, R.K.; Popli, H.; Gupta, M. Novel Drug Delivery Strategies for the Treatment of Onychomycosis. Pharm. Nanotechnol. 2019, 7, 24–38. [Google Scholar] [CrossRef]
- Vikas, A.; Rashmin, P.; Mrunali, P.; Chavan, R.B.; Kaushik, T. Mechanistic Insights of Formulation Approaches for the Treatment of Nail Infection: Conventional and Novel Drug Delivery Approaches. AAPS PharmSciTech 2020, 21, 67. [Google Scholar] [CrossRef]
- Gupta, A.K.; Foley, K.A.; Versteeg, S.G. New Antifungal Agents and New Formulations Against Dermatophytes. Mycopathologia 2017, 182, 127–141. [Google Scholar] [CrossRef] [PubMed]
- Poulakos, M.; Grace, Y.; Machin, J.D.; Dorval, E. Efinaconazole and Tavaborole. J. Pharm. Pract. 2017, 30, 245–255. [Google Scholar] [CrossRef]
- Sil, B.C.; Patel, A.; Crowther, J.M.; Moore, D.J.; Hadgraft, J.; Hilton, S.T.; Lane, M.E. A Preliminary Investigation of Additive Manufacture to Fabricate Human Nail Plate Surrogates for Pharmaceutical Testing. Pharmaceutics 2019, 11, 250. [Google Scholar] [CrossRef]
- Aggarwal, R.; Targhotra, M.; Sahoo, P.K.; Chauhan, M.K. Onychomycosis: Novel strategies for treatment. J. Drug Deliv. Sci. Technol. 2020, 57, 101774. [Google Scholar] [CrossRef]
- Nair, A.B.; Sammeta, S.M.; Vaka, S.R.; Narasimha Murthy, S. A study on the effect of inorganic salts in transungual drug delivery of terbinafine. J. Pharm. Pharmacol. 2009, 61, 431–437. [Google Scholar] [CrossRef]
- Cutrín-Gómez, E.; Anguiano-Igea, S.; Delgado-Charro, M.B.; Gómez-Amoza, J.L.; Otero-Espinar, F.J. Effect of Penetration Enhancers on Drug Nail Permeability from Cyclodextrin/Poloxamer-Soluble Polypseudorotaxane-Based Nail Lacquers. Pharmaceutics 2018, 10, 273. [Google Scholar] [CrossRef]
- Cutrín-Gómez, E.; Conde-Penedo, A.; Anguiano-Igea, S.; Gómez-Amoza, J.L.; Otero-Espinar, F.J. Optimization of Drug Permeation from 8% Ciclopirox Cyclodextrin/Poloxamer-Soluble Polypseudorotaxane-Based Nail Lacquers. Pharmaceutics 2020, 12, 231. [Google Scholar] [CrossRef]
- Cutrín-Gómez, E.; Anguiano-Igea, S.; Delgado-Charro, M.B.; Gómez-Amoza, J.L.; Otero-Espinar, F.J. Effect on Nail Structure and Transungual Permeability of the Ethanol and Poloxamer Ratio from Cyclodextrin-Soluble Polypseudorotaxanes Based Nail Lacquer. Pharmaceutics 2018, 10, 156. [Google Scholar] [CrossRef] [PubMed]
- Thatai, P.; Sapra, B. Transungual delivery: Deliberations and creeds. Int. J. Cosmet. Sci. 2014, 36, 398–411. [Google Scholar] [CrossRef]
- Shivakumar, H.N.; Juluri, A.; Desai, B.G.; Murthy, S.N. Ungual and transungual drug delivery. Drug Dev. Ind. Pharm. 2012, 38, 901–911. [Google Scholar] [CrossRef]
- Šveikauskaitė, I.; Pockevičius, A.; Briedis, V. Potential of Chemical and Physical Enhancers for Transungual Delivery of Amorolfine Hydrochloride. Materials 2019, 12, 1028. [Google Scholar] [CrossRef]
- Nair, A.B.; Sammeta, S.M.; Kim, H.D.; Chakraborty, B.; Friden, P.M.; Murthy, S.N. Alteration of the diffusional barrier property of the nail leads to greater terbinafine drug loading and permeation. Int. J. Pharm. 2009, 375, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.; Puri, V.; Michniak-Kohn, B. Iontophoresis to Overcome the Challenge of Nail Permeation: Considerations and Optimizations for Successful Ungual Drug Delivery. AAPS J. 2021, 23, 25. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Charro, M.B. Iontophoretic drug delivery across the nail. Expert Opin. Drug Deliv. 2012, 9, 91–103. [Google Scholar] [CrossRef]
- Sprenger, A.B.; Purim, K.S.M.; Sprenger, F.; Queiroz-Telles, F. A Week of Oral Terbinafine Pulse Regimen Every Three Months to Treat all Dermatophyte Onychomycosis. J. Fungi 2019, 5, 82. [Google Scholar] [CrossRef]
- Darkes, M.J.M.; Scott, L.J.; Goa, K.L. Terbinafine. Am. J. Clin. Dermatol. 2003, 4, 39–65. [Google Scholar] [CrossRef]
- Nair, A.B.; Vaka, S.R.; Sammeta, S.M.; Kim, H.D.; Friden, P.M.; Chakraborty, B.; Murthy, S.N. Trans-ungual iontophoretic delivery of terbinafine. J. Pharm. Sci. 2009, 98, 1788–1796. [Google Scholar] [CrossRef]
- Nair, A.B.; Kim, H.D.; Chakraborty, B.; Singh, J.; Zaman, M.; Gupta, A.; Friden, P.M.; Murthy, S.N. Ungual and trans-ungual iontophoretic delivery of terbinafine for the treatment of onychomycosis. J. Pharm. Sci. 2009, 98, 4130–4140. [Google Scholar] [CrossRef]
- Shehata, T.M.; Nair, A.B.; Al-Dhubiab, B.E.; Shah, J.; Jacob, S.; Alhaider, I.A.; Attimarad, M.; Elsewedy, H.S.; Ibrahim, M.M. Vesicular emulgel based system for transdermal delivery of insulin: Factorial design and in vivo evaluation. Appl. Sci. 2020, 10, 5341. [Google Scholar] [CrossRef]
- Nair, A.B.; Shah, J.; Jacob, S.; Al-Dhubiab, B.E.; Sreeharsha, N.; Morsy, M.A.; Gupta, S.; Attimarad, M.; Shinu, P.; Venugopala, K.N. Experimental design, formulation and in vivo evaluation of a novel topical in situ gel system to treat ocular infections. PLoS ONE 2021, 16, e0248857. [Google Scholar] [CrossRef] [PubMed]
- Nair, A.B.; Shah, J.; Aljaeid, B.M.; Al-Dhubiab, B.E.; Jacob, S. Gellan Gum-Based Hydrogel for the Transdermal Delivery of Nebivolol: Optimization and Evaluation. Polymers 2019, 11, 1699. [Google Scholar] [CrossRef] [PubMed]
- Vörös-Horváth, B.; Das, S.; Salem, A.; Nagy, S.; Böszörményi, A.; Kőszegi, T.; Pál, S.; Széchenyi, A. Formulation of Tioconazole and Melaleuca alternifolia Essential Oil Pickering Emulsions for Onychomycosis Topical Treatment. Molecules 2020, 25, 5544. [Google Scholar] [CrossRef] [PubMed]
- Jacob, S.; Nair, A.B.; Al-Dhubiab, B.E. Preparation and evaluation of niosome gel containing acyclovir for enhanced dermal deposition. J. Liposome Res. 2017, 27, 283–292. [Google Scholar] [CrossRef]
- Guideline, I.H.T. Stability testing of new drug substances and products. Q1A (R2) Curr. Step 2003, 4, 1–24. [Google Scholar]
- Murthy, S.N.; Vaka, S.R.; Sammeta, S.M.; Nair, A.B. TranScreen-N: Method for rapid screening of trans-ungual drug delivery enhancers. J. Pharm. Sci. 2009, 98, 4264–4271. [Google Scholar] [CrossRef]
- Nair, A.B.; Chakraborty, B.; Murthy, S.N. Effect of polyethylene glycols on the trans-ungual delivery of terbinafine. Curr. Drug Deliv. 2010, 7, 407–414. [Google Scholar] [CrossRef]
- Calzavara-Pinton, P.; Rossi, M.T.; Sala, R.; Venturini, M. Photodynamic antifungal chemotherapy. Photochem. Photobiol. 2012, 88, 512–522. [Google Scholar] [CrossRef]
- Murdan, S. Drug delivery to the nail following topical application. Int. J. Pharm. 2002, 236, 1–26. [Google Scholar] [CrossRef]
- Akrawi, S.H.; Gorain, B.; Nair, A.B.; Choudhury, H.; Pandey, M.; Shah, J.N.; Venugopala, K.N. Development and Optimization of Naringenin-Loaded Chitosan-Coated Nanoemulsion for Topical Therapy in Wound Healing. Pharmaceutics 2020, 12, 893. [Google Scholar] [CrossRef]
- Kumbhar, S.A.; Kokare, C.R.; Shrivastava, B.; Gorain, B.; Choudhury, H. Preparation, characterization, and optimization of asenapine maleate mucoadhesive nanoemulsion using Box-Behnken design: In vitro and in vivo studies for brain targeting. Int. J. Pharm. 2020, 586, 119499. [Google Scholar] [CrossRef] [PubMed]
- Park, J.S.; Kim, J.S.; Ho, M.J.; Park, D.W.; Kim, E.A.; Choi, Y.S.; Jang, S.W.; Kang, M.J. Effect of Penetration Enhancers on Toenail Delivery of Efinaconazole from Hydroalcoholic Preparations. Molecules 2021, 26, 1650. [Google Scholar] [CrossRef]
- Brown, M.B.; Martin, G.P.; Jones, S.A.; Akomeah, F.K. Dermal and transdermal drug delivery systems: Current and future prospects. Drug Deliv. 2006, 13, 175–187. [Google Scholar] [CrossRef] [PubMed]
- Saner, M.V.; Kulkarni, A.D.; Pardeshi, C.V. Insights into drug delivery across the nail plate barrier. J. Drug Target 2014, 22, 769–789. [Google Scholar] [CrossRef] [PubMed]
- Nair, A.B.; Kim, H.D.; Davis, S.P.; Etheredge, R.; Barsness, M.; Friden, P.M.; Murthy, S.N. An ex vivo toe model used to assess applicators for the iontophoretic ungual delivery of terbinafine. Pharm. Res. 2009, 26, 2194–2201. [Google Scholar] [CrossRef]
- Nair, A.B.; Singh, K.; Shinu, P.; Harsha, S.; Al-Dhubiab, B.E. A comprehensive study to evaluate the effect of constant low voltage iontophoresis on transungual delivery. Drug Dev. Ind. Pharm. 2013, 39, 807–815. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Brazis, P.W. Experiments of DC human body resistance I: Equipment, setup, and contact materials. In Proceedings of the 2018 IEEE Symposium on Product Compliance Engineering (ISPCE), Shenzhen, China, 14–16 May 2018; pp. 1–6. [Google Scholar]
- Nair, A.B.; Vaka, S.R.; Murthy, S.N. Transungual delivery of terbinafine by iontophoresis in onychomycotic nails. Drug Dev. Ind. Pharm. 2011, 37, 1253–1258. [Google Scholar] [CrossRef]
- Bharate, S.S.; Bharate, S.B.; Bajaj, A.N. Interactions and incompatibilities of pharmaceutical excipients with active pharmaceutical ingredients: A comprehensive review. J. Excip. Food Chem. 2016, 1, 1131. [Google Scholar]
- Iizhar, S.A.; Syed, I.A.; Satar, R.; Ansari, S.A. In vitro assessment of pharmaceutical potential of ethosomes entrapped with terbinafine hydrochloride. J. Adv. Res. 2016, 7, 453–461. [Google Scholar] [CrossRef]
- Gaba, B.; Fazil, M.; Khan, S.; Ali, A.; Baboota, S.; Ali, J. Nanostructured lipid carrier system for topical delivery of terbinafine hydrochloride. Bull. Fac. Pharm. Cairo Univ. 2015, 53, 147–159. [Google Scholar] [CrossRef]
- Town, A.R.; Taylor, J.; Dawson, K.; Niezabitowska, E.; Elbaz, N.M.; Corker, A.; Garcia-Tuñón, E.; McDonald, T.O. Tuning HIV drug release from a nanogel-based in situ forming implant by changing nanogel size. J. Mater. Chem. B 2019, 7, 373–383. [Google Scholar] [CrossRef]
- Benzeval, I.; Bowen, C.R.; Guy, R.H.; Delgado-Charro, M.B. Effects of iontophoresis, hydration, and permeation enhancers on human nail plate: Infrared and impedance spectroscopy assessment. Pharm. Res. 2013, 30, 1652–1662. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Lee, B.C.; Pangeni, R.; Na, J.; Koo, K.T.; Park, J.W. Preparation and in vivo evaluation of a highly skin- and nail-permeable efinaconazole topical formulation for enhanced treatment of onychomycosis. Drug Deliv. 2019, 26, 1167–1177. [Google Scholar] [CrossRef] [PubMed]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ingredients | Batch Code | |||||
|---|---|---|---|---|---|---|
| T1 | T2 | T3 | T4 | T5 | T6 | |
| Terbinafine HCl (% w/w) | 4 | 4 | 4 | 4 | 4 | 4 |
| Ethanol (% w/w) | 20 | 20 | 20 | 20 | 20 | 20 |
| Tween 80 (% w/w) | 5 | 5 | 5 | 5 | 5 | 5 |
| Polyethylene glycol 200 (% w/w) | 15 | - | 30 | - | 30 | - |
| Polyethylene glycol 400 (% w/w) | - | 15 | - | 30 | - | 30 |
| Propylene glycol (% w/w) | 10 | 10 | 10 | 10 | 10 | 10 |
| Polyvinylpyrrolidone K 30 (% w/w) | 10 | 10 | 10 | 10 | 20 | 20 |
| Water as required to (% w/w) | 100 | 100 | 100 | 100 | 100 | 100 |
| Parameters | Batch Code | |||||
|---|---|---|---|---|---|---|
| T1 | T2 | T3 | T4 | T5 | T6 | |
| pH | 3.39 ± 0.21 | 3.48 ± 0.37 | 3.26 ± 0.18 | 3.51 ± 0.24 | 3.22 ± 0.15 | 3.44 ± 0.26 |
| Loading efficacy (%) | 97.41 ± 3.67 | 96.57 ± 3.74 | 97.05 ± 3.28 | 98.22 ± 2.62 | 96.88 ± 3.11 | 96.37 ± 3.34 |
| Drug loading (%) | 3.90 ± 0.15 | 3.86 ± 0.14 | 3.88 ± 0.13 | 3.93 ± 0.10 | 3.88 ± 0.12 | 3.85 ± 0.13 |
| Viscosity (cP) at 30 rpm | 62.5 ± 2.65 | 65.1 ± 1.98 | 65.9 ± 2.21 | 68.2 ± 1.50 | 73.3 ± 2.75 | 75.6 ± 2.31 |
| Cumulative amount permeated in 6 h (µg/cm2) | 1.08 ± 0.26 | 2.67 ± 0.74 | 1.83 ± 0.45 | 3.97 ± 1.18 | 1.69 ± 0.42 | 3.80 ± 1.24 |
| Drug accumulation into the nail tissue in 6 h (µg/mg) | 0.22 ± 0.02 | 0.42 ± 0.05 | 0.33 ± 0.04 | 0.87 ± 0.05 | 0.29 ± 0.03 | 0.69 ± 0.07 |
| Batch Code | Values of Independent Variables | Actual Responses | Predicted Responses | ||||
|---|---|---|---|---|---|---|---|
| A | B | C | R1 | R2 | R1 | R2 | |
| (% w/w) | (V) | (h) | (µg/cm2) | (µg/mg) | (µg/cm2) | (µg/mg) | |
| F1 | 0 | 0 | 0 | 32.63 ± 4.76 | 1.85 ± 0.23 | 32.63 | 1.85 |
| F2 | 1 | 1 | 0 | 38.54 ± 4.84 | 2.10 ± 0.30 | 39.11 | 2.19 |
| F3 | 0 | 0 | 0 | 32.63 ± 4.76 | 1.85 ± 0.23 | 32.63 | 1.85 |
| F4 | 0 | 0 | 0 | 32.63 ± 4.76 | 1.85 ± 0.23 | 32.63 | 1.85 |
| F5 | −1 | 0 | 1 | 42.38 ± 4.55 | 2.36 ± 0.39 | 42.68 | 2.41 |
| F6 | 0 | −1 | 1 | 31.26 ± 2.77 | 2.04 ± 0.33 | 31.54 | 2.09 |
| F7 | 0 | −1 | −1 | 11.64 ± 3.00 | 0.87 ±0. 24 | 12.17 | 0.94 |
| F8 | 0 | 1 | 1 | 54.35 ± 4.76 | 2.93 ± 0.49 | 53.82 | 2.86 |
| F9 | −1 | −1 | 0 | 22.78 ± 3.66 | 1.55 ± 0.27 | 22.20 | 1.45 |
| F10 | 1 | 0 | 1 | 45.17 ± 5.93 | 2.56 ± 0.30 | 45.12 | 2.53 |
| F11 | 1 | 0 | −1 | 18.23 ± 3.64 | 1.27 ± 0.25 | 17.94 | 1.23 |
| F12 | −1 | 0 | −1 | 16.71 ± 2.14 | 0.99 ± 0.19 | 16.75 | 1.01 |
| F13 | 0 | 1 | −1 | 20.37 ± 4.23 | 1.36 ± 0.28 | 20.09 | 1.31 |
| F14 | −1 | 1 | 0 | 36.03 ± 5.93 | 1.97 ± 0.24 | 36.27 | 1.99 |
| F15 | 0 | 0 | 0 | 32.63 ± 4.76 | 1.85 ± 0.23 | 32.63 | 1.85 |
| F16 | 0 | 0 | 0 | 32.63 ± 4.76 | 1.85 ± 0.23 | 32.63 | 1.85 |
| F17 | 1 | −1 | 0 | 23.21 ± 4.25 | 1.63 ± 0.22 | 22.98 | 1.60 |
| Independent variable | Low (−1) | Medium (0) | Upper (+1) | ||||
| A = PEG 400 (% w/w) | 20 | 30 | 40 | ||||
| B = Voltage (V) | 6 | 9 | 12 | ||||
| C = Application time (h) | 2 | 4 | 6 | ||||
| Dependent variables: R1 = Permeation (µg/cm2) R2 = Accumulation into the nail tissue (µg/mg) | |||||||
| Source | Permeation | ||
|---|---|---|---|
| Sum of Squares | F-Value | p-Value | |
| Model | 1952.29 | 911.96 | <0.0001 |
| A-PEG 400 | 6.57 | 27.63 | 0.0012 |
| B-Voltage | 456.15 | 1917.71 | <0.0001 |
| C-Application time | 1410.16 | 5928.47 | <0.0001 |
| AB | 1.08 | 4.54 | 0.0705 |
| AC | 0.3964 | 1.67 | 0.2377 |
| BC | 51.57 | 216.82 | <0.0001 |
| A2 | 1.69 | 7.12 | 0.0320 |
| B2 | 14.45 | 60.77 | 0.0001 |
| C2 | 7.91 | 33.26 | 0.0007 |
| Residual | 1.67 | ||
| Lack of Fit | 1.67 | ||
| Pure Error | 0.0000 | ||
| Cor Total | 1953.96 | ||
| Source | Accumulation into the Nail Tissue | ||
|---|---|---|---|
| Sum of Squares | F-Value | p-Value | |
| Model | 4.39 | 87.16 | <0.0001 |
| A-PEG 400 | 0.0599 | 10.70 | 0.0137 |
| B-Voltage | 0.6479 | 115.76 | <0.0001 |
| C-Application time | 3.63 | 648.86 | <0.0001 |
| AB | 0.0007 | 0.1275 | 0.7316 |
| AC | 0.0021 | 0.3792 | 0.5575 |
| BC | 0.0413 | 7.39 | 0.0299 |
| A2 | 0.0017 | 0.2958 | 0.6034 |
| B2 | 0.0010 | 0.1874 | 0.6781 |
| C2 | 0.0038 | 0.6739 | 0.4388 |
| Residual | 0.0392 | ||
| Lack of Fit | 0.0392 | ||
| Pure Error | 0.0000 | ||
| Cor Total | 4.43 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nair, A.B.; Al-Dhubiab, B.E.; Shah, J.; Gorain, B.; Jacob, S.; Attimarad, M.; Sreeharsha, N.; Venugopala, K.N.; Morsy, M.A. Constant Voltage Iontophoresis Technique to Deliver Terbinafine via Transungual Delivery System: Formulation Optimization Using Box–Behnken Design and In Vitro Evaluation. Pharmaceutics 2021, 13, 1692. https://doi.org/10.3390/pharmaceutics13101692
Nair AB, Al-Dhubiab BE, Shah J, Gorain B, Jacob S, Attimarad M, Sreeharsha N, Venugopala KN, Morsy MA. Constant Voltage Iontophoresis Technique to Deliver Terbinafine via Transungual Delivery System: Formulation Optimization Using Box–Behnken Design and In Vitro Evaluation. Pharmaceutics. 2021; 13(10):1692. https://doi.org/10.3390/pharmaceutics13101692
Chicago/Turabian StyleNair, Anroop B., Bandar E. Al-Dhubiab, Jigar Shah, Bapi Gorain, Shery Jacob, Mahesh Attimarad, Nagaraja Sreeharsha, Katharigatta N. Venugopala, and Mohamed A. Morsy. 2021. "Constant Voltage Iontophoresis Technique to Deliver Terbinafine via Transungual Delivery System: Formulation Optimization Using Box–Behnken Design and In Vitro Evaluation" Pharmaceutics 13, no. 10: 1692. https://doi.org/10.3390/pharmaceutics13101692
APA StyleNair, A. B., Al-Dhubiab, B. E., Shah, J., Gorain, B., Jacob, S., Attimarad, M., Sreeharsha, N., Venugopala, K. N., & Morsy, M. A. (2021). Constant Voltage Iontophoresis Technique to Deliver Terbinafine via Transungual Delivery System: Formulation Optimization Using Box–Behnken Design and In Vitro Evaluation. Pharmaceutics, 13(10), 1692. https://doi.org/10.3390/pharmaceutics13101692