A Pediatrics Utilization Study in The Netherlands to Identify Active Pharmaceutical Ingredients Suitable for Inkjet Printing on Orodispersible Films

 ,
, 
 ,
,  and
and
Abstract
1. Introduction
2. Methods
2.1. Data Source
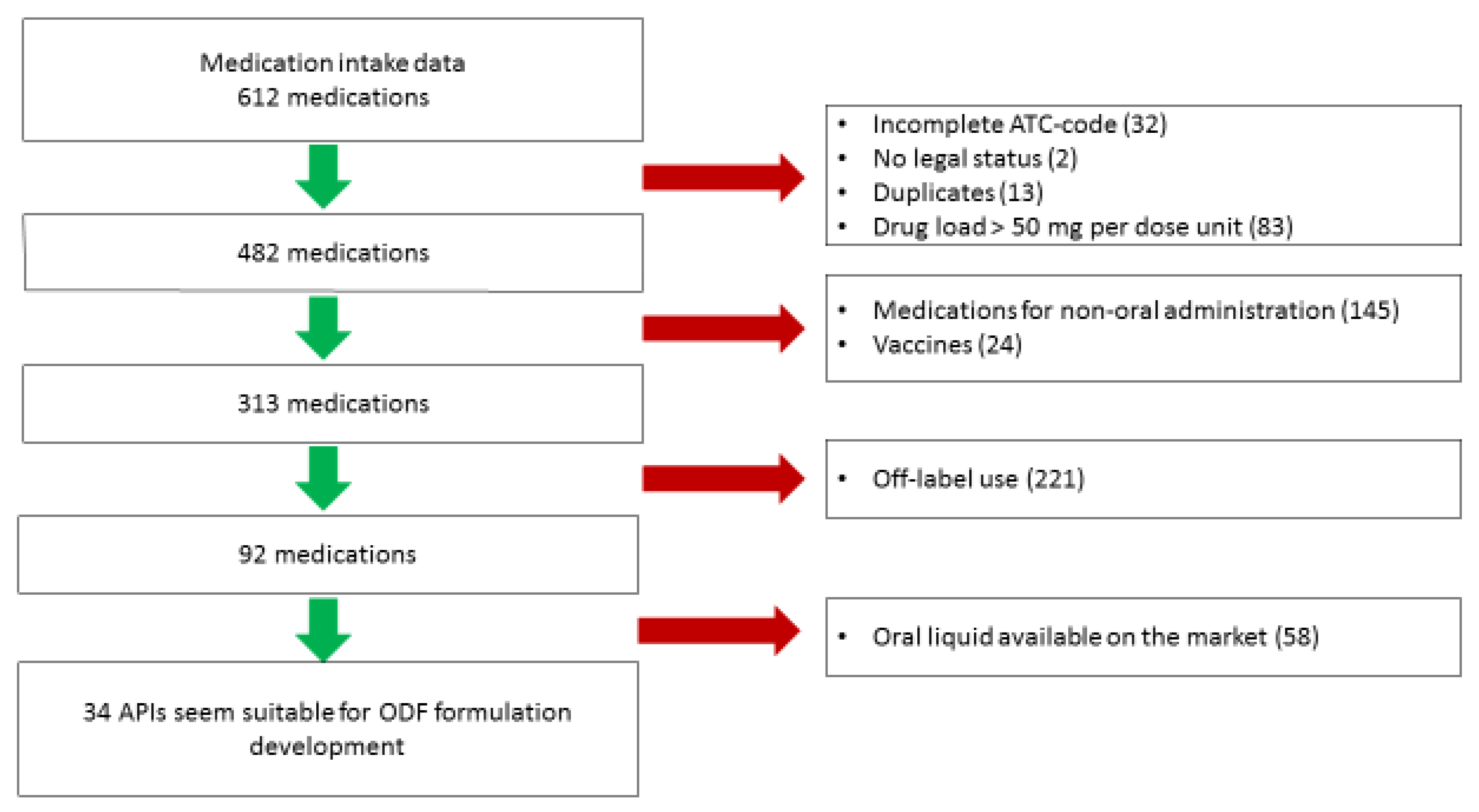
2.2. Selection of the Candidates for Development of ODFs
2.3. Ethical Statement
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Visser, J.C.; Wibier, L.; Mekhaeil, M.; Woerdenbag, H.J.; Taxis, K. Orodispersible films as a personalized dosage form for nursing home residents, an exploratory study. Int. J. Clin. Pharm. 2020, 1–9, (submitted, minor revisions). [Google Scholar] [CrossRef]
- Neubert, A.; Taxis, K.; Wong, A.C.K. Drug utilization in the paediatric population. In Drug Utilization Research Methods and Applications; Elseviers, M., Ed.; Wiley Blackwell: Chichester, UK, 2016; pp. 248–258. [Google Scholar]
- European Medicines Agency (EMA). Reflection Paper: Formulations of Choice for the Paediatric Population. 2006. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/reflection-paper-formulations-choice-paediatric-population_en.pdf (accessed on 27 November 2019).
- Chedoe, I.; Molendijk, H.; Hospes, W.; Van den Heuvel, E.R.; Taxis, K. The effect of a multifaceted educational intervention on medication preparation and administration errors in neonatal intensive care. Arch. Dis. Child Fetal Neonatal Ed. 2012, 97, F449–F455. [Google Scholar] [CrossRef] [PubMed]
- Visser, J.C.; Woerdenbag, H.J.; Hanff, L.M.; Frijlink, H.W. Personalized medicine in pediatrics: The clinical potential of orodispersible films. AAPS PharmSciTech 2017, 18, 267–272. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency (EMA): Guideline on Pharmaceutical Development of Medicines for Paediatric Use 2013. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-pharmaceutical-development-medicines-paediatric-use_en.pdf (accessed on 27 November 2019).
- Visser, J.C.; Woerdenbag, H.J.; Crediet, S.; Gerrits, E.; Lesschen, M.A.; Hinrichs, W.L.J.; Breitkreitz, J.; Frijlink, H.W. Orodispersible films in individualized pharmacotherapy: The development of a formulation for pharmacy preparations. Int. J. Pharm. 2015, 478, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Ranmal, S.R.; Batchelor, H.K.; Orlu-Gul, M.; Ernest, T.B.; Thomas, I.W.; Flanagan, T.; Tuleu, C. Patient-centred pharmaceutical design to improve acceptability of medicines: Similarities and differences in paediatric and geriatric populations. Drugs 2014, 74, 1871–1889. [Google Scholar] [CrossRef] [PubMed]
- Orlu, M.; Ranmal, S.R.; Sheng, Y.; Tuleu, C.; Seddon, P. Acceptability of orodispersible films for delivery of medicines to infants and preschool children. Drug Deliv. 2017, 24, 1243–1248. [Google Scholar] [CrossRef] [PubMed]
- Krampe, R.; Visser, J.C.; Frijlink, H.W.; Breitkreutz, J.; Woerdenbag, H.J.; Preis, M. Oromucosal film preparations: Points to consider for patient centricity and manufacturing processes. Expert Opin. Drug Deliv. 2016, 13, 493–506. [Google Scholar] [CrossRef]
- Sandler, N.; Määttänen, A.; Ihalainen, P.; Kronberg, L.; Meierjohann, A.; Viitala, T.; Peltonen, J. Inkjet printing of drug substrates and use of porous substrates-towards individualized dosing. J. Pharm. Sci. 2011, 8, 3386–3395. [Google Scholar] [CrossRef]
- Öblom, H.; Sjöholm, E.; Rautamo, M.; Sandler, N. Towards Printed Pediatric Medicines in Hospital Pharmacies: Comparison of 2D and 3D-Printed Orodispersible Warfarin Films with Conventional Oral Powders in Unit Dose Sachets. Pharmaceutics 2019, 11, 334. [Google Scholar] [CrossRef]
- Tian, Y.; Orlu, M.; Woerdenbag, H.J.; Scarpa, M.; Kiefer, O.; Kottke, D.; Sjöblom, E.; Öblom, H.; Sandler, N.; Hinrichs, W.L.J.; et al. Oromucosal films: From patient centricity to production by printing techniques. Expert Opin. Drug Deliv. 2019, 16, 981–993. [Google Scholar] [CrossRef]
- Thabet, Y.; Lunter, D.; Breitkreutz, J. Continuous Inkjet Printing of Enalapril Maleate onto Orodispersible Film Formulations. Int. J. Pharm. 2018, 546, 180–187. [Google Scholar] [CrossRef] [PubMed]
- IADB Pharmacy Dispensing Database. Available online: http://iadb.nl/ (accessed on 27 November 2019).
- Dutch Paediatric Formulary (Kinderformularium). Available online: https://www.kinderformularium.nl/ (accessed on 27 November 2019).
- Informatorium Medicamentorium. Available online: www.kennisbank.knmp.nl (accessed on 27 November 2019).
- Farmacotherapeutisch Kompas. Available online: https://www.farmacotherapeutischkompas.nl/ (accessed on 27 November 2019).
- European Pharmacopoeia. Available online: https://pheur.edqm.eu/home (accessed on 27 November 2019).
- Pubchem. Available online: https://pubchem.ncbi.nlm.nih.gov/ (accessed on 27 November 2019).
- Federa. Available online: www.federa.org/federa-english (accessed on 9 February 2020).
- European Commission. Study on Off-Label Use of Medicinal Products in the European Union. Available online: https://ec.europa.eu/health/sites/health/files/files/documents/2017_02_28_final_study_report_on_off-label_use_.pdf (accessed on 27 November 2019).
- Schrier, L.; Hadjipanayis, A.; Stiris, T.; Ross-Russell, R.I.; Valiulis, A.; Turner, M.A.; Zhao, W.; De Cock, P.; de Wildt, S.N.; Allegaert, K.; et al. Off-label use of medicines in neonates, infants, children, and adolescents: A joint policy statement by the European Academy of Paediatrics and the European society for Developmental Perinatal and Pediatric Pharmacology. Eur. J. Pediatr. 2020. [Google Scholar] [CrossRef] [PubMed]
- Summary of Products Characteristics Gemfibrozil. Available online: https://www.medicines.org.uk/emc/product/132/smpc (accessed on 27 November 2019).
- Kim, K.; Kleinman, H.K.; Lee, H.J.; Pahan, K. Safety and potential efficacy of gemfibrozil as a supportive treatment for children with late infantile neuronal ceroid lipofuscinosis and other lipid storage disorders. Orphanet J. Rare Dis. 2017, 12, 113. [Google Scholar] [CrossRef] [PubMed]
- Kohlschütter, A.; Schulz, A.; Bartsch, U.; Storch, S. Current and Emerging Treatment Strategies for Neuronal Ceroid Lipofuscinoses. CNS Drugs 2019, 33, 315–325. [Google Scholar] [CrossRef] [PubMed]
- Meyers, R. A wish list for drug development in pediatrics. J. Pharm. Sci. 2019, 109, 939–943. [Google Scholar] [CrossRef] [PubMed]
- Van Riet-Nales, D.A.; de Neef, B.J.; Schobben, A.F.; Ferreira, J.A.; Egberts, T.C.; Rademaker, C.M. Acceptability of different oral formulations in infants and preschool children. Arch. Dis. Child. 2013, 98, 725–731. [Google Scholar] [CrossRef]
- Thabet, Y.; Klingmann, V.; Breitkreutz, J. Drug formulations: Standards and novel strategies for drug administration in pediatrics. J. Clin. Pharmacol. 2018, 58, S26–S35. [Google Scholar] [CrossRef]
- Mistry, P.; Batchelor, H. SPaeDD-UK project (Smart Paediatric Drug Development-UK), Evidence of acceptability of oral paediatric medicines: A review. J. Pharm. Pharmacol. 2017, 69, 361–376. [Google Scholar] [CrossRef]
- Pardeike, J.; Strohmeier, D.M.; Schrödl, N.; Voura, C.; Gruber, M.; Khinast, J.G.; Zimmer, A. Nanosuspensions as advanced printing ink for accurate dosing of poorly soluble drugs in personalized medicines. Int. J. Pharm. 2011, 420, 93–100. [Google Scholar] [CrossRef]
- Kollamaram, G.; Hopkins, S.C.; Glowacki, B.A.; Croker, D.M.; Walker, G.M. Inkjet printing of paracetamol and indomethacin using electromagnetic technology: Rheological compatibility and polymorphic selectivity. Eur. J. Pharm. Sci. 2018, 115, 248–257. [Google Scholar] [CrossRef]
- Genina, N.; Fors, D.; Palo, M.; Peltonen, J.; Sandler, N. Behavior of printable formulations of loperamide and caffeine on different substrates--effect of print density in inkjet printing. Int. J. Pharm. 2013, 453, 488–497. [Google Scholar] [CrossRef]
- Iftimi, L.D.; Edinger, M.; Bar-Shalom, D.; Rantanen, J.; Genina, N. Edible solid foams as porous substrates for inkjet-printable pharmaceuticals. Eur. J. Pharm. Biopharm. 2019, 136, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Edinger, M.; Bar-Shalom, D.; Sandler, N.; Rantanen, J.; Genina, N. QR encoded smart oral dosage forms by inkjet printing. Int. J. Pharm. 2018, 536, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Eleftheriadis, G.K.; Monou, P.K.; Bourppoulos, N.; Fatouris, D.G. In Vitro Evaluation of 2D-Printed Edible Films for the Buccal Delivery of Diclofenac Sodium. Materials 2018, 11, 864. [Google Scholar] [CrossRef]
- Wickstrom, H.; Palo, M.; Rijckaert, K.; Kolakovoc, R.; Nyman, J.O.; Määttänen, A.; Ihalainen, O.; Peltonen, J.; Genina, N.; de Beer, T.; et al. Improvement of dissolution rate of indomethacin by inkjet printing. Eur. J. Pharm. Sci. 2015, 75, 91–100. [Google Scholar] [CrossRef]
- Edinger, M.; Iftimi, L.D.; Markl, D.; Al-Sharabi, M.; Bar-Shalom, D.; Rantanen, J.; Genina, N. Quantification of Inkjet-Printed Pharmaceuticals on Porous Substrates Using Raman Spectroscopy and Near-Infrared Spectroscopy. AAPS PharmSciTech 2019, 20, 207. [Google Scholar] [CrossRef]
- Vakili, H.; Wickström, H.; Desei, D.; Preis, M.; Sandler, N. Application of a handheld NIR spectrometer in prediction of drug content in inkjet printed orodispersible formulations containing prednisolone and levothyroxine. Int. J. Pharm. 2017, 524, 414–423. [Google Scholar] [CrossRef]


{kind=link}
| ATC Level | Number of Dispensed Medications (% of Total Dispensed Medications) |
|---|---|
| J (anti-infectives for systemic use) | 67,292 (29.5%) |
| R (respiratory system) | 59,984 (26.3%) |
| A (alimentary tract and metabolism) | 58,327 (25.9%) |
| S (sensory organs) | 13,338 (5.9%) |
| N (nervous system) | 11,619 (5.1%) |
| H (systemic hormonal preparations, excluding sex hormones and insulins) | 4202 (1.8%) |
| C (cardiovascular system) | 4109 (1.8%) |
| B (blood and blood forming organs) | 3184 (1.4%) |
| M (musculoskeletal system) | 1967 (0.9%) |
| P (antiparasitic products, insecticides and repellents) | 1288 (0.6%) |
| L (antineoplastic and immunomodulating agents) | 1286 (0.6%) |
| G (genitourinary system and sex hormones) | 1180 (0.5%) |
| V (various) | 122 (0.05%) |
| ATC Code | Medications | Number of Users (n) | Percentage of Users (%) | |
|---|---|---|---|---|
| 1 | J01CA04 | Amoxicillin | 25265 | 49.2 |
| 2 | R03AC02 | Salbutamol | 11150 | 20.8 |
| 3 | A07AA02 | Nystatin | 6767 | 12.6 |
| 4 | A06AD15 | Macrogol | 5338 | 10 |
| 5 | J01CR02 | Amoxicilline plus β-lactamase inhibitor | 4514 | 8.4 |
| 6 | S01AA01 | Chloramphenicol | 3895 | 7.3 |
| 7 | R06AX27 | Desloratidine | 3685 | 6.9 |
| 8 | J01FA10 | Azithromycine | 3376 | 6.3 |
| 9 | A06AD11 | Lactulose | 3272 | 6.1 |
| 10 | S01AA13 | Fusidic acid | 3244 | 6.1 |
| 11 | R01AA07 | Xylometazoline | 2949 | 5.5 |
| 12 | R03BA05 | Fluticasone | 2739 | 5.1 |
| 13 | A06AD65 | Macrogol, combinations | 1687 | 3.2 |
| 14 | J01CF05 | Flucloxacillin | 1679 | 3.1 |
| 15 | J01FA09 | Clarithromycin | 1576 | 2.9 |
| ATC Code | Name | Water Solubility (g/L) | Taste | Number of Users (n) | Daily Dose ** | |
|---|---|---|---|---|---|---|
| 1 * | N06AA04 | Clomipramine | 0.000294 | n/a | 1 | 0.25–0.5 mg/kg/day in two doses |
| 2 | M01AB01 | Indomethacin | 0.000937 | Slightly bitter | 4 | 2 mg/kg/day in two to four doses |
| 3 | A06AB02 | Bisacodyl | 0.00127 | Tasteless | 340 | 5 mg/day |
| 4 | L04AA18 | Everolimus | 0.00163 | n/a | 2 | 1.6–9 mg/m2/day |
| 5 | M01AB05 | Diclofenac | 0.00237 | n/a | 754 | 1–3 mg/kg/day, in two to four doses |
| 6 | C08DA01 | Verapamil | 0.00447 | n/a | 3 | 3–8 mg/kg/day, in three doses |
| 7 | A11CC04 | Calcitriol | 0.00667 | n/a | 1 | 0.01–0.1 mics/kg/day, in two doses |
| 8 | N02CX01 | Pizotifen | 0.00706 | n/a | 1 | 0.5–1.5 mg/day, in one to three doses |
| 9 | N05CD08 | Midazolam | 0.00987 | Bitter | 157 | 0.2–0.5 mg/kg |
| 10 | N05AG02 | Pimozide | 0.01 | n/a | 1 | 0.5–1 mg/day |
| 12 | N06AA02 | Imipramine | 0.0182 | n/a | 3 | 20–30 mg/day |
| 13 | N04AA02 | Biperiden | 0.0251 | n/a | 9 | 1–2 mg, one to three times daily |
| 14 | N05CD02 | Nitrazepam | 0.0299 | n/a | 9 | 2.5–5 mg/day |
| 15 | N05BA01 | Diazepam | 0.050 | Bitter aftertaste | 501 | 0.1–0.8 mg/kg/day, in four doses |
| y16 | H02AB07 | Prednisone | 0.07754 | Bitter aftertaste | 8 | 1–2 mg/kg, in two doses |
| 17 | C05AA12 | Triamcinolone | 0.080 | Bitter | 2 | <35 kg: 4–12 mg/day |
| 18 | H01BA02 | Desmopressin | 0.11 | n/a | 43 | 0.2 mg/day |
| 19 | C03BA04 | Chlorthalidone | 0.12 | n/a | 3 | 0.5–1 mg/kg, max 1.7 mg/kg per 48 h |
| 20 | H02AA02 | Fludrocortisone | 0.14 | n/a | 11 | 50–150 mics/day, in two doses |
| 21 | N03AX09 | Lamotrigine | 0.17 | n/a | 35 | 0.3–1.2 mg/kg |
| 22 | N05BA04 | Oxazepam | 0.179 | Bitter | 27 | 10–30 mg per day, in three to four doses |
| 23 | A02BC01 | Omeprazole | 0.359 | n/a | 453 | 1 mg/kg/day in one to two doses, max 40 mg/day |
| 24 | J04BA02 | Dapsone | 0.38 | Slightly bitter | 2 | 1–1.5 mg/kg/day |
| 25 | N05BB01 | Hydroxyzine | 0.428 | Bitter | 7 | 1–2 mg/kg/day, max 100 mg/day |
| 26 | N07CA02 | Cinnarizine | 0.75 | Bitter | 3 | 12.5 mg, if necessary, three to four times per day |
| 27 | R06AE05 | Meclozine | 1 | tasteless | 1 | 6.25 mg, if necessary, three to four times per day |
| 28 | N07AA02 | Pyridostigmine | 1.04 | tasteless | 18 | 10 mg/day, max 100–500 mg in three doses |
| 29 | N02AE01 | Buprenorphine | 1.680 | Bitter | 3 | 15 mics/kg/day in three doses |
| 30 | L04AX03 | Methotrexate | 2.6 | n/a | 28 | 10–15 mg/m2/dose, once per week |
| 31 | V03AH01 | Diazoxide | 2.85 | n/a | 1 | 5 mg/kg/day, in two doses |
| 32 | N03AX11 | Topiramate | 9.8 | Bitter | 11 | 1–3 mg/kg/day |
| 33 | M04AC01 | Colchicine | 10 | n/a | 7 | 0.5–1 mg/day, in one to two doses |
| 34 | R03DC03 | Montelukast | >100 | n/a | 178 | 4 mg per day |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Visser, J.C.; Wibier, L.; Kiefer, O.; Orlu, M.; Breitkreutz, J.; Woerdenbag, H.J.; Taxis, K. A Pediatrics Utilization Study in The Netherlands to Identify Active Pharmaceutical Ingredients Suitable for Inkjet Printing on Orodispersible Films. Pharmaceutics 2020, 12, 164. https://doi.org/10.3390/pharmaceutics12020164
Visser JC, Wibier L, Kiefer O, Orlu M, Breitkreutz J, Woerdenbag HJ, Taxis K. A Pediatrics Utilization Study in The Netherlands to Identify Active Pharmaceutical Ingredients Suitable for Inkjet Printing on Orodispersible Films. Pharmaceutics. 2020; 12(2):164. https://doi.org/10.3390/pharmaceutics12020164
Chicago/Turabian StyleVisser, J. Carolina, Lisa Wibier, Olga Kiefer, Mine Orlu, Jörg Breitkreutz, Herman J. Woerdenbag, and Katja Taxis. 2020. "A Pediatrics Utilization Study in The Netherlands to Identify Active Pharmaceutical Ingredients Suitable for Inkjet Printing on Orodispersible Films" Pharmaceutics 12, no. 2: 164. https://doi.org/10.3390/pharmaceutics12020164
APA StyleVisser, J. C., Wibier, L., Kiefer, O., Orlu, M., Breitkreutz, J., Woerdenbag, H. J., & Taxis, K. (2020). A Pediatrics Utilization Study in The Netherlands to Identify Active Pharmaceutical Ingredients Suitable for Inkjet Printing on Orodispersible Films. Pharmaceutics, 12(2), 164. https://doi.org/10.3390/pharmaceutics12020164