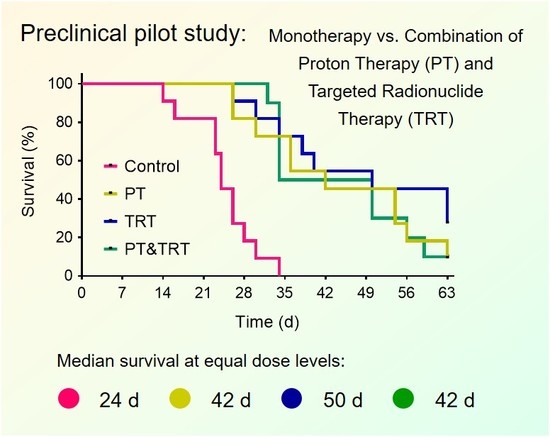
Combination of Proton Therapy and Radionuclide Therapy in Mice: Preclinical Pilot Study at the Paul Scherrer Institute


 ,
,  and
and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. In Vivo Experiments
2.2. Preparation of Mice
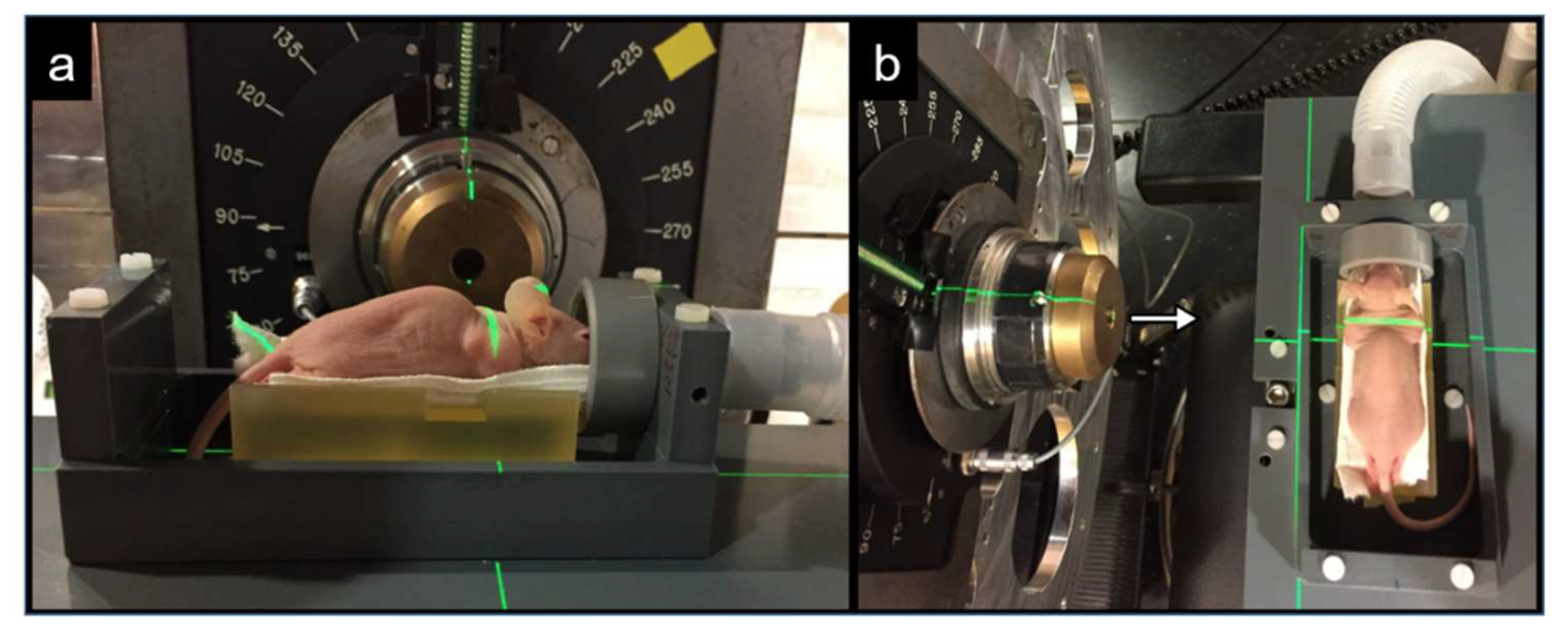
2.3. Irradiation Station for Mice
2.4. Irradiation of Tumor-Bearing Mice with Protons
2.5. Preparation and Application of 177Lu-Labeled Radioligands
2.6. Dosimetric Calculations for TRT
2.7. Therapy Studies
2.8. Assessment of the Therapy Studies
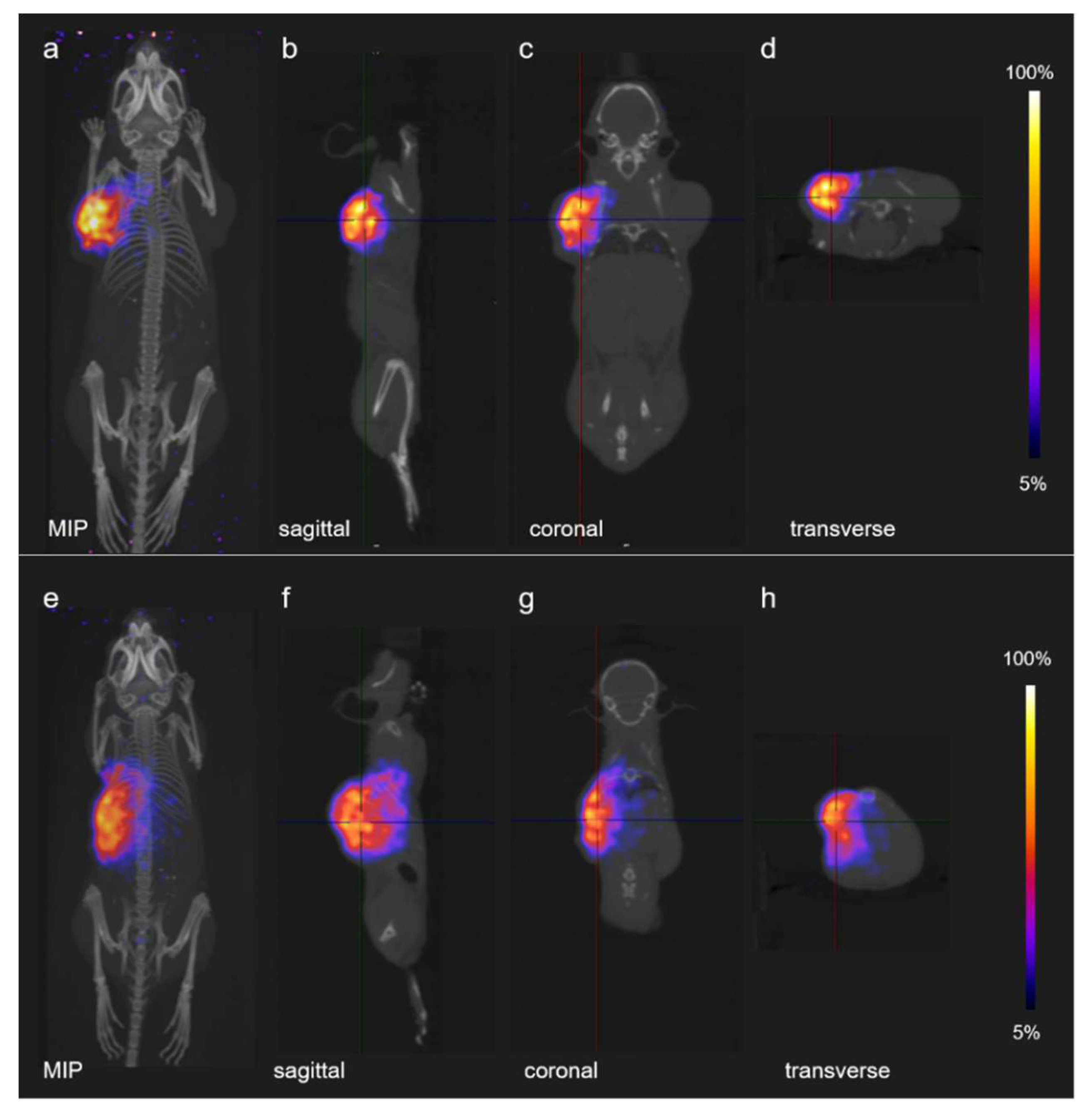
2.9. PET Imaging
3. Results
3.1. Dosimetry Estimation for TRT Using 177Lu-Folate and 177Lu-PSMA-617
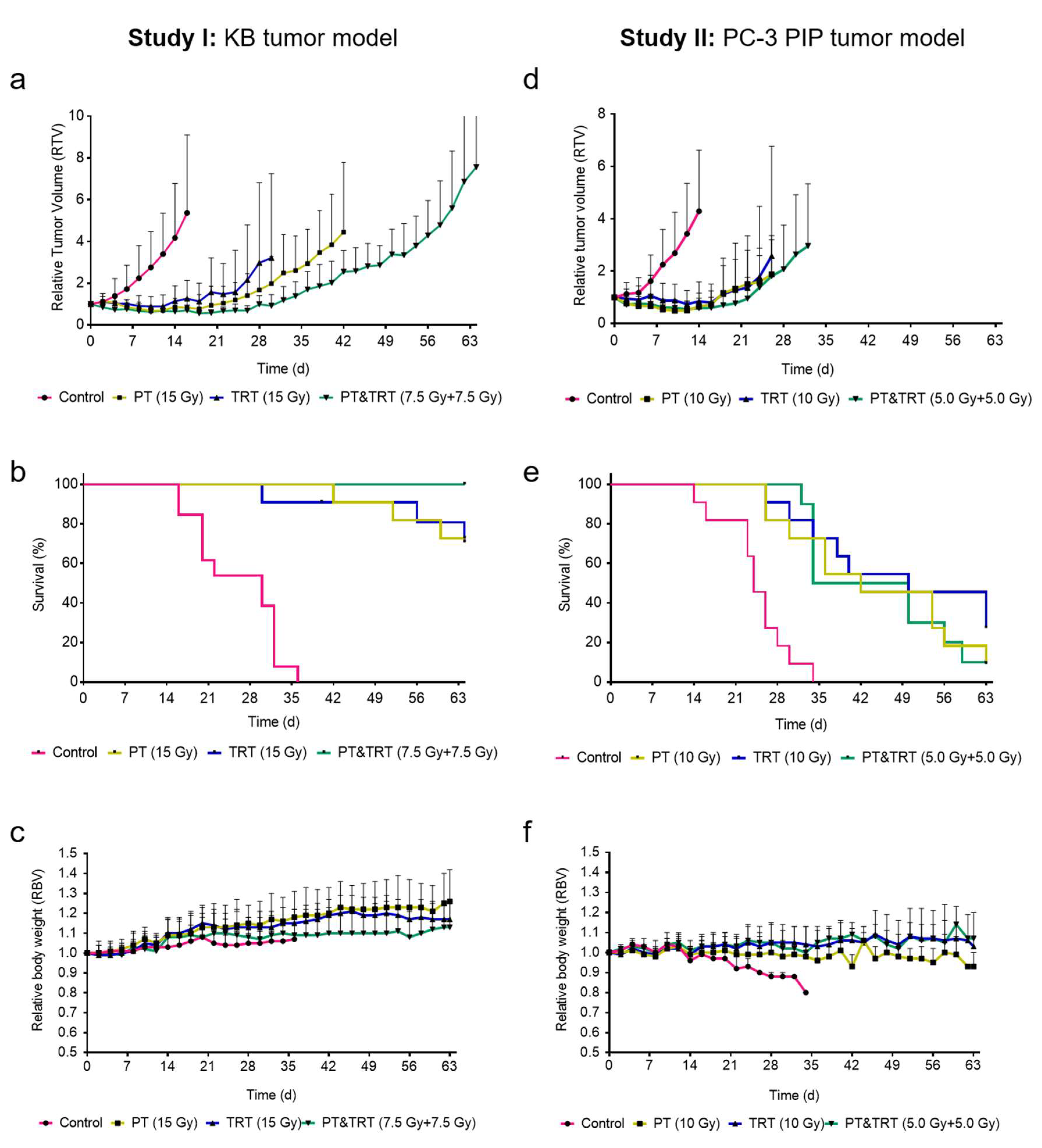
3.2. Therapy Studies
3.2.1. Therapy Study I: Combination Proton Therapy and 177Lu-Folate Therapy
3.2.2. Therapy Study II: Combination of Proton Therapy and 177Lu-PSMA-617 Therapy
3.3. PET-Based Imaging of Tissue Activation after Proton Irradiation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Tian, X.; Liu, K.; Hou, Y.; Cheng, J.; Zhang, J. The evolution of proton beam therapy: Current and future status. Mol. Clin. Oncol. 2018, 8, 15–21. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food and Drug Administration. FDA approves Lutathera for GEP NET therapy. J. Nucl. Med. 2018, 59, 9N. [Google Scholar]
- Alcindor, T.; Witzig, T.E. Radioimmunotherapy with yttrium-90 ibritumomab tiuxetan for patients with relapsed CD20+ B-cell non-hodgkin’s lymphoma. Curr. Treat. Options Oncol. 2002, 3, 275–282. [Google Scholar] [CrossRef] [PubMed]
- Rahbar, K.; Ahmadzadehfar, H.; Kratochwil, C.; Haberkorn, U.; Schafers, M.; Essler, M.; Baum, R.P.; Kulkarni, H.R.; Schmidt, M.; Drzezga, A.; et al. German multicenter study investigating 177Lu-PSMA-617 radioligand therapy in advanced prostate cancer patients. J. Nucl. Med. 2017, 58, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Lambert, B.; Cybulla, M.; Weiner, S.M.; Van De Wiele, C.; Ham, H.; Dierckx, R.A.; Otte, A. Renal toxicity after radionuclide therapy. Radiat. Res. 2004, 161, 607–611. [Google Scholar] [CrossRef] [PubMed]
- Sabet, A.; Ezziddin, K.; Pape, U.F.; Ahmadzadehfar, H.; Mayer, K.; Poppel, T.; Guhlke, S.; Biersack, H.J.; Ezziddin, S. Long-term hematotoxicity after peptide receptor radionuclide therapy with 177Lu-octreotate. J. Nucl. Med. 2013, 54, 1857–1861. [Google Scholar] [CrossRef] [PubMed]
- Buchegger, F.; Rojas, A.; Delaloye, A.B.; Vogel, C.A.; Mirimanoff, R.O.; Coucke, P.; Sun, L.Q.; Raimondi, S.; Denekamp, J.; Pelgrin, A.; et al. Combined radioimmunotherapy and radiotherapy of human colon carcinoma grafted in nude mice. Cancer Res. 1995, 55, 83–89. [Google Scholar] [PubMed]
- Kreissl, M.C.; Hanscheid, H.; Lohr, M.; Verburg, F.A.; Schiller, M.; Lassmann, M.; Reiners, C.; Samnick, S.S.; Buck, A.K.; Flentje, M.; et al. Combination of peptide receptor radionuclide therapy with fractionated external beam radiotherapy for treatment of advanced symptomatic meningioma. Radiat. Oncol. 2012, 7, 99. [Google Scholar] [CrossRef]
- Müller, C. Folate based radiopharmaceuticals for imaging and therapy of cancer and inflammation. Curr. Pharm. Des. 2012, 18, 1058–1083. [Google Scholar] [CrossRef]
- Siwowska, K.; Muller, C. Preclinical development of small-molecular-weight folate-based radioconjugates: A pharmacological perspective. Q. J. Nucl. Med. Mol. Imaging 2015, 59, 269–286. [Google Scholar]
- Benešová, M.; Umbricht, C.A.; Schibli, R.; Müller, C. Albumin-binding PSMA ligands: Optimization of the tissue distribution profile. Mol. Pharm. 2018, 15, 934–946. [Google Scholar] [CrossRef] [PubMed]
- Umbricht, C.A.; Benešová, M.; Schibli, R.; Müller, C. Preclinical development of novel PSMA-targeting radioligands: Modulation of albumin-binding properties to improve prostate cancer therapy. Mol. Pharm. 2018, 15, 2297–2306. [Google Scholar] [CrossRef] [PubMed]
- Müller, C.; Struthers, H.; Winiger, C.; Zhernosekov, K.; Schibli, R. DOTA conjugate with an albumin-binding entity enables the first folic acid-targeted 177Lu-radionuclide tumor therapy in mice. J. Nucl. Med. 2013, 54, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Haller, S.; Reber, J.; Brandt, S.; Bernhardt, P.; Groehn, V.; Schibli, R.; Müller, C. Folate receptor-targeted radionuclide therapy: Preclinical investigation of anti-tumor effects and potential radionephropathy. Nucl. Med. Biol. 2015, 42, 770–779. [Google Scholar] [CrossRef] [PubMed]
- Pedroni, E.; Bacher, R.; Blattmann, H.; Bohringer, T.; Coray, A.; Lomax, A.; Lin, S.; Munkel, G.; Scheib, S.; Schneider, U.; et al. The 200-MeV proton therapy project at the Paul Scherrer Institute: Conceptual design and practical realization. Med. Phys. 1995, 22, 37–53. [Google Scholar] [CrossRef] [PubMed]
- Lomax, A. Intensity modulation methods for proton radiotherapy. Phys. Med. Biol. 1999, 44, 185–205. [Google Scholar] [CrossRef] [PubMed]
- Weber, D.C.; Malyapa, R.; Albertini, F.; Bolsi, A.; Kliebsch, U.; Walser, M.; Pica, A.; Combescure, C.; Lomax, A.J.; Schneider, R. Long term outcomes of patients with skull-base low-grade chondrosarcoma and chordoma patients treated with pencil beam scanning proton therapy. Radiother. Oncol. 2016, 120, 169–174. [Google Scholar] [CrossRef]
- Murray, F.R.; Snider, J.W.; Bolsi, A.; Lomax, A.J.; Walser, M.; Kliebsch, U.; Schneider, R.A.; Weber, D.C. Long-term clinical outcomes of pencil beam scanning proton therapy for benign and non-benign intracranial meningiomas. Int. J. Radiat. Oncol. Biol. Phys. 2017, 99, 1190–1198. [Google Scholar] [CrossRef]
- Snider, J.W.; Schneider, R.A.; Poelma-Tap, D.; Stieb, S.; Murray, F.R.; Placidi, L.; Albertini, F.; Lomax, A.; Bolsi, A.; Kliebsch, U.; et al. Long-term outcomes and prognostic factors after pencil-beam scanning proton radiation therapy for spinal chordomas: A large, single-institution cohort. Int. J. Radiat. Oncol. Biol. Phys. 2018, 101, 226–233. [Google Scholar] [CrossRef]
- Egger, E.; Schalenbourg, A.; Zografos, L.; Bercher, L.; Boehringer, T.; Chamot, L.; Goitein, G. Maximizing local tumor control and survival after proton beam radiotherapy of uveal melanoma. Int. J. Radiat. Oncol. Biol. Phys. 2001, 51, 138–147. [Google Scholar] [CrossRef]
- Egger, E.; Zografos, L.; Schalenbourg, A.; Beati, D.; Bohringer, T.; Chamot, L.; Goitein, G. Eye retention after proton beam radiotherapy for uveal melanoma. Int. J. Radiat. Oncol. Biol. Phys. 2003, 55, 867–880. [Google Scholar] [CrossRef]
- Siwowska, K.; Haller, S.; Bortoli, F.; Benešová, M.; Groehn, V.; Bernhardt, P.; Schibli, R.; Müller, C. Preclinical comparison of albumin-binding radiofolates: Impact of linker entities on the in vitro and in vivo properties. Mol. Pharm. 2017, 14, 523–532. [Google Scholar] [CrossRef] [PubMed]
- Uusijärvi, H.; Bernhardt, P.; Ericsson, T.; Forssell-Aronsson, E. Dosimetric characterization of radionuclides for systemic tumor therapy: Influence of particle range, photon emission, and subcellular distribution. Med. Phys. 2006, 33, 3260–3269. [Google Scholar] [CrossRef] [PubMed]
- Gu, Z.; Taschereau, R.; Vu, N.T.; Prout, D.L.; Silverman, R.W.; Lee, J.T.; Chatziioannou, A.F. Performance evaluation of G8, a high-sensitivity benchtop preclinical PET/CT tomograph. J. Nucl. Med. 2019, 60, 142–149. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; El Fakhri, G. Proton therapy verification with pet imaging. Theranostics 2013, 3, 731–740. [Google Scholar] [CrossRef] [PubMed]
- Schild, S.E.; Rule, W.G.; Ashman, J.B.; Vora, S.A.; Keole, S.; Anand, A.; Liu, W.; Bues, M. Proton beam therapy for locally advanced lung cancer: A review. World J. Clin. Oncol. 2014, 5, 568–575. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.J., Jr.; Zeng, J.; Rengan, R. Proton beam therapy and immunotherapy: An emerging partnership for immune activation in non-small cell lung cancer. Transl. Lung Cancer Res. 2018, 7, 180–188. [Google Scholar]
- Pouget, J.P.; Navarro-Teulon, I.; Bardies, M.; Chouin, N.; Cartron, G.; Pelegrin, A.; Azria, D. Clinical radioimmunotherapy - the role of radiobiology. Nat. Rev. Clin. Oncol. 2011, 8, 720–734. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study I: KB Tumor Mouse Model | ||||
| Groups | A: Control | B: PT | C: TRT | D: PT and TRT |
| Proton Irradiation | Sham irradiation | Irradiation: 15 Gy | Sham irradiation | Irradiation: 7.5 Gy |
| 177Lu-Folate Treatment | Saline injection | Saline injection | 177Lu-folate 15 Gy (17 MBq) 1 nmol/mouse | 177Lu-folate 7.5 Gy (8.5 MBq) 1 nmol/mouse |
| Number of Mice | n = 13 | n = 11 | n = 11 | n = 11 |
| Study II: PC-3 PIP Tumor Mouse Model | ||||
| Groups | A: Control | B: PT | C: TRT | D: PT and TRT |
| Proton Irradiation | Sham irradiation | Irradiation: 10 Gy | Sham irradiation | Irradiation: 5.0 Gy |
| 177Lu-PSMA-617 Treatment | Saline injection | Saline injection | 177Lu-folate: 10 Gy (2.5 MBq) 1 nmol/mouse | 177Lu-folate: 5.0 Gy (1.25 MBq) 1 nmol/mouse |
| Number of Mice | n = 11 | n = 11 | n = 11 | n = 11 |
| Study I: KB Tumor Mouse Model | |||||||
| Group | Tumor Dose (Gy) | First Mouse Euthanized (Day) | Last Mouse Euthanized (Day) | Median Survival (days) | Average Survival (days) | TGDI2 | TGDI5 |
| A: Saline | - | 16 | 36 | 30 | 27 ± 9 (n = 13) | 1.0 ± 0.4 (n = 13) | 1.0 ± 0.3 (n = 13) |
| B: PT | 15 | 42 | 64 (study end) | not reached | n = 3 (endpoint) 1 n = 8 (alive) 2 | 3.5 ± 1.1 (n = 11) | 2.7 ± 0.7 (n = 9) |
| C: TRT | ~15 | 30 | 64 (study end) | not reached | n = 3 (endpoint) 1 n = 8 (alive) 2 | 3.2 ± 1.1 (n = 10) | 2.4 ± 0.9 (n = 10) |
| D: PT & TRT | 7.5 + ~7.5 | none | 64 (study end) | not reached | n = 0 (endpoint) 1 n = 11 (alive) 2 | 4.2 ± 0.6 (n = 11) | 3.2 ± 0.2 (n = 11) |
| Study II: PC-3 PIP Tumor Mouse Model | |||||||
| Group | Tumor Dose (Gy) | First Mouse Euthanized (Day) | Last Mouse Euthanized (Day) | Median Survival (days) | Average Survival (days) | TGDI2 | TGDI5 |
| A: Saline | - | 14 | 34 | 24 | 26 ± 6 (n = 11) | 1.0 ± 0.5 (n = 11) | 1.0 ± 0.4 (n = 10) |
| B: PT | 10 | 26 | 64 (study end) | 42 | n = 10 (endpoint) 1 n = 1 (alive) 2 | 3.3 ± 1.5 (n = 11) | 2.3 ± 0.4 (n = 8) |
| C: TRT | ~10 | 26 | 64 (study end) | 50 | n = 8 (endpoint) 1 n = 3 (alive) 2 | 3.8 ± 2.1 (n = 9) | 1.7 ± 0.6 (n = 6) |
| D: PT & TRT | 5.0 + ~5.0 | 32 | 64 (study end) | 42 | n = 10 (endpoint) 1 n = 1 (alive) | 3.6 ± 1.3 (n = 11) | 2.1 ± 0.6 (n = 11) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Müller, C.; De Prado Leal, M.; Dominietto, M.D.; Umbricht, C.A.; Safai, S.; Perrin, R.L.; Egloff, M.; Bernhardt, P.; van der Meulen, N.P.; Weber, D.C.; et al. Combination of Proton Therapy and Radionuclide Therapy in Mice: Preclinical Pilot Study at the Paul Scherrer Institute. Pharmaceutics 2019, 11, 450. https://doi.org/10.3390/pharmaceutics11090450
Müller C, De Prado Leal M, Dominietto MD, Umbricht CA, Safai S, Perrin RL, Egloff M, Bernhardt P, van der Meulen NP, Weber DC, et al. Combination of Proton Therapy and Radionuclide Therapy in Mice: Preclinical Pilot Study at the Paul Scherrer Institute. Pharmaceutics. 2019; 11(9):450. https://doi.org/10.3390/pharmaceutics11090450
Chicago/Turabian StyleMüller, Cristina, Maria De Prado Leal, Marco D. Dominietto, Christoph A. Umbricht, Sairos Safai, Rosalind L. Perrin, Martina Egloff, Peter Bernhardt, Nicholas P. van der Meulen, Damien C. Weber, and et al. 2019. "Combination of Proton Therapy and Radionuclide Therapy in Mice: Preclinical Pilot Study at the Paul Scherrer Institute" Pharmaceutics 11, no. 9: 450. https://doi.org/10.3390/pharmaceutics11090450
APA StyleMüller, C., De Prado Leal, M., Dominietto, M. D., Umbricht, C. A., Safai, S., Perrin, R. L., Egloff, M., Bernhardt, P., van der Meulen, N. P., Weber, D. C., Schibli, R., & Lomax, A. J. (2019). Combination of Proton Therapy and Radionuclide Therapy in Mice: Preclinical Pilot Study at the Paul Scherrer Institute. Pharmaceutics, 11(9), 450. https://doi.org/10.3390/pharmaceutics11090450