
High Hepatitis E Virus (HEV) Seroprevalence and No Evidence of HEV Viraemia in Vietnamese Blood Donors

 ,
,  ,
,  , , ,
, , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Study Cohort
2.3. Serological Assays
2.4. Nucleic Acid Isolation
2.5. HEV-Specific RT-PCR
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics
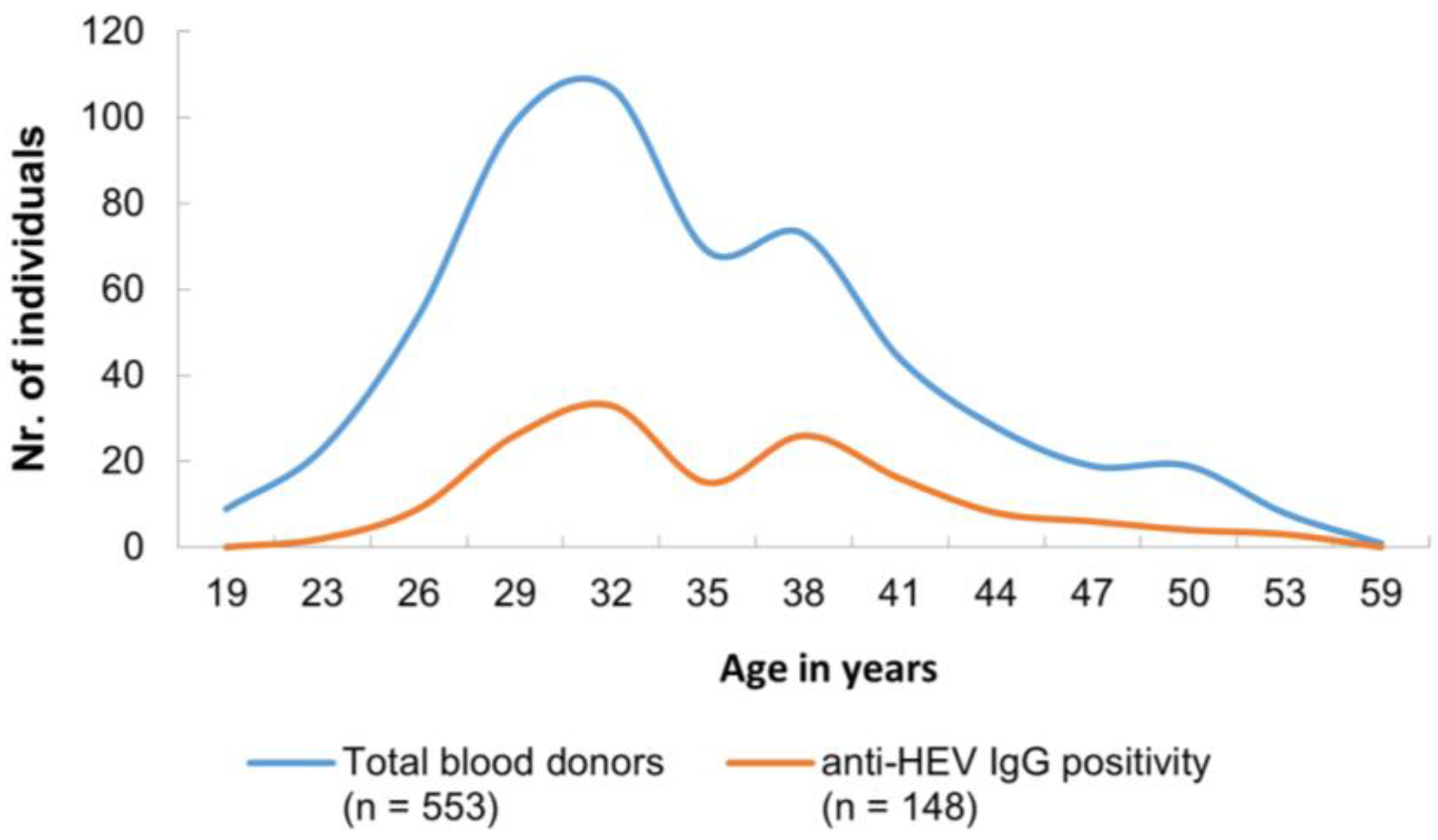
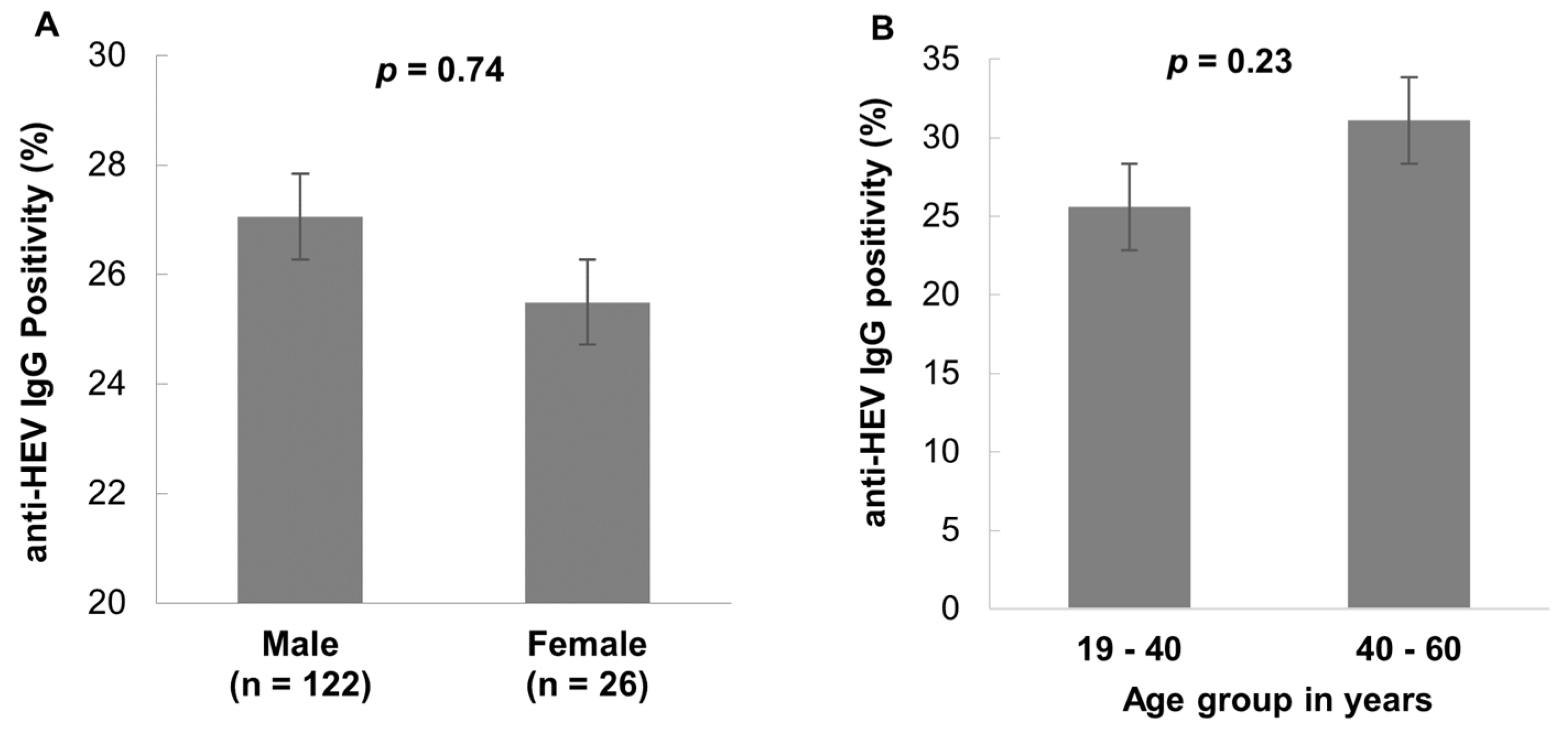
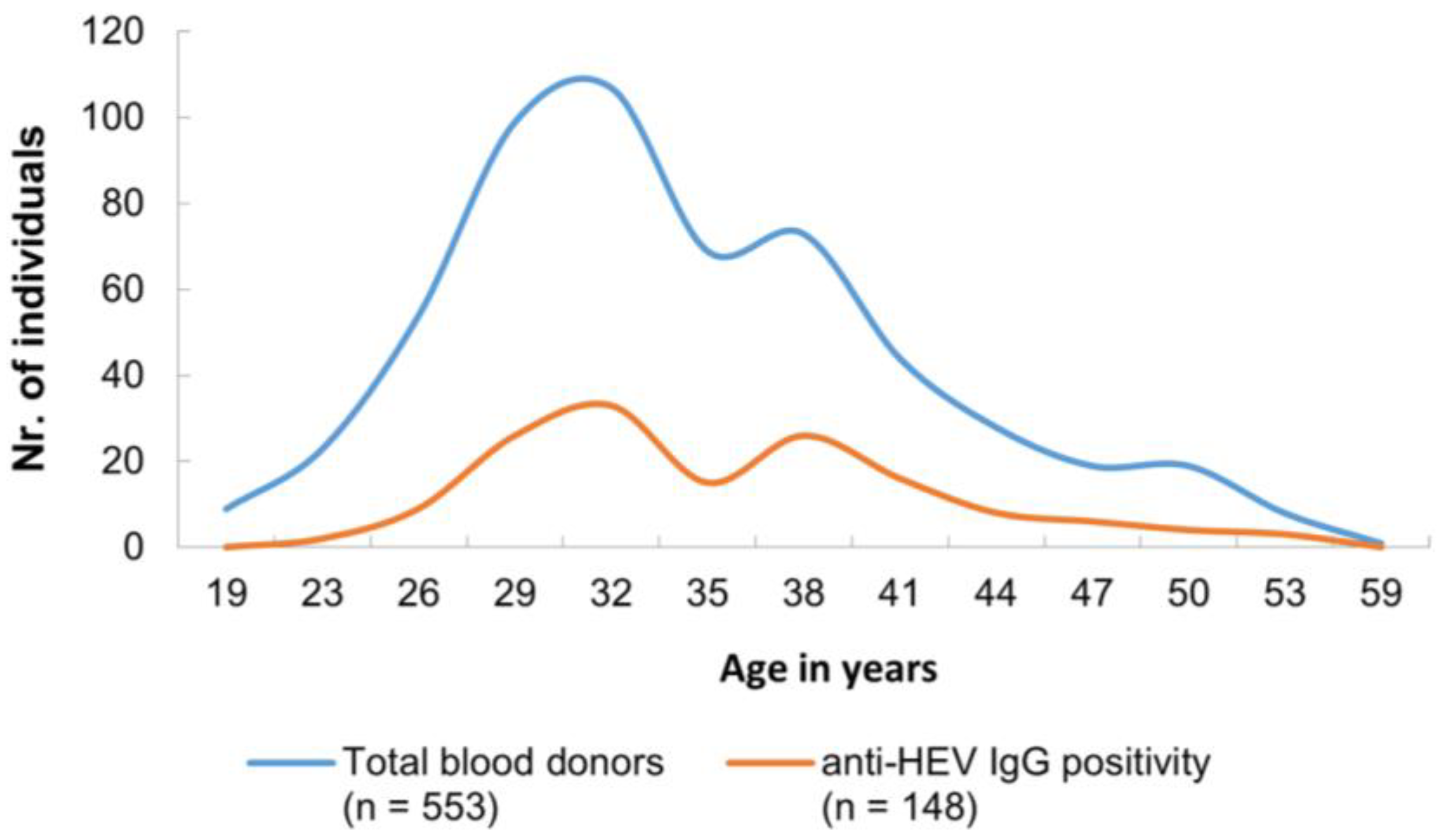
3.2. HEV Seroprevalence
3.3. HEV Nucleic Acid Testing
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Hepatitis E: Fact Sheet 20 July 2023. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-e (accessed on 21 July 2023).
- Velavan, T.P.; Pallerla, S.R.; Johne, R.; Todt, D.; Steinmann, E.; Schemmerer, M.; Wenzel, J.J.; Hofmann, J.; Shih, J.W.K.; Wedemeyer, H.; et al. Hepatitis E: An update on One Health and clinical medicine. Liver Int. 2021, 41, 1462–1473. [Google Scholar] [CrossRef] [PubMed]
- Purdy, M.A.; Drexler, J.F.; Meng, X.-J.; Norder, H.; Okamoto, H.; Van der Poel, W.H.M.; Reuter, G.; de Souza, W.M.; Ulrich, R.G.; Smith, D.B. ICTV Virus Taxonomy Profile: Hepeviridae 2022. J. Gen. Virol. 2022, 103, 001778. [Google Scholar] [CrossRef] [PubMed]
- Huy, P.X.; Chung, D.T.; Linh, D.T.; Hang, N.T.; Rachakonda, S.; Pallerla, S.R.; Linh, L.T.K.; Tong, H.V.; Dung, L.M.; Mao, C.V.; et al. Low Prevalence of HEV Infection and No Associated Risk of HEV Transmission from Mother to Child among Pregnant Women in Vietnam. Pathogens 2021, 10, 1340. [Google Scholar] [CrossRef] [PubMed]
- Perez-Gracia, M.T.; Suay-Garcia, B.; Mateos-Lindemann, M.L. Hepatitis E and pregnancy: Current state. Rev. Med. Virol. 2017, 27, e1929. [Google Scholar] [CrossRef] [PubMed]
- Berto, A.; Pham, H.A.; Thao, T.T.N.; Vy, N.H.T.; Caddy, S.L.; Hiraide, R.; Tue, N.T.; Goodfellow, I.; Carrique-Mas, J.J.; Thwaites, G.E.; et al. Hepatitis E in southern Vietnam: Seroepidemiology in humans and molecular epidemiology in pigs. Zoonoses Public Health 2018, 65, 43–50. [Google Scholar] [CrossRef]
- Hoan, N.X.; Huy, P.X.; Sy, B.T.; Meyer, C.G.; Son, T.V.; Binh, M.T.; Giang, D.P.; Tu Anh, D.; Bock, C.T.; Wang, B.; et al. High Hepatitis E virus (HEV) Positivity Among Domestic Pigs and Risk of HEV Infection of Individuals Occupationally Exposed to Pigs and Pork Meat in Hanoi, Vietnam. Open Forum Infect. Dis. 2019, 6, ofz306. [Google Scholar] [CrossRef]
- Pallerla, S.R.; Harms, D.; Johne, R.; Todt, D.; Steinmann, E.; Schemmerer, M.; Wenzel, J.J.; Hofmann, J.; Shih, J.W.K.; Wedemeyer, H.; et al. Hepatitis E Virus Infection: Circulation, Molecular Epidemiology, and Impact on Global Health. Pathogens 2020, 9, 856. [Google Scholar] [CrossRef]
- Westholter, D.; Hiller, J.; Denzer, U.; Polywka, S.; Ayuk, F.; Rybczynski, M.; Horvatits, T.; Gundlach, S.; Blocker, J.; Schulze Zur Wiesch, J.; et al. HEV-positive blood donations represent a relevant infection risk for immunosuppressed recipients. J. Hepatol. 2018, 69, 36–42. [Google Scholar] [CrossRef]
- Matsubayashi, K.; Nagaoka, Y.; Sakata, H.; Sato, S.; Fukai, K.; Kato, T.; Takahashi, K.; Mishiro, S.; Imai, M.; Takeda, N.; et al. Transfusion-transmitted hepatitis E caused by apparently indigenous hepatitis E virus strain in Hokkaido, Japan. Transfusion 2004, 44, 934–940. [Google Scholar] [CrossRef]
- Cheung, C.K.M.; Wong, S.H.; Law, A.W.H.; Law, M.F. Transfusion-transmitted hepatitis E: What we know so far? World J. Gastroenterol. 2022, 28, 47–75. [Google Scholar] [CrossRef]
- Boland, F.; Martinez, A.; Pomeroy, L.; O’Flaherty, N. Blood Donor Screening for Hepatitis E Virus in the European Union. Transfus. Med. Hemother. 2019, 46, 95–103. [Google Scholar] [CrossRef] [PubMed]
- Tripathy, A.S.; Puranik, S.; Sharma, M.; Chakraborty, S.; Devakate, U.R. Hepatitis E virus seroprevalence among blood donors in Pune, India. J. Med. Virol. 2019, 91, 813–819. [Google Scholar] [CrossRef] [PubMed]
- Fu, P.; Lin, B.; Wu, B.; Ke, L.; Yang, T.; Du, Y.; Cheng, L.; Li, Z.; Li, T.; Liu, Y. Hepatitis E virus prevalence among blood donors in Dali, China. Virol. J. 2021, 18, 141. [Google Scholar] [CrossRef]
- Nouhin, J.; Prak, S.; Madec, Y.; Barennes, H.; Weissel, R.; Hok, K.; Pavio, N.; Rouet, F. Hepatitis E virus antibody prevalence, RNA frequency, and genotype among blood donors in Cambodia (Southeast Asia). Transfusion 2016, 56, 2597–2601. [Google Scholar] [CrossRef] [PubMed]
- Hoan, N.X.; Tong, H.V.; Hecht, N.; Sy, B.T.; Marcinek, P.; Meyer, C.G.; Song, L.H.; Toan, N.L.; Kurreck, J.; Kremsner, P.G.; et al. Hepatitis E Virus Superinfection and Clinical Progression in Hepatitis B Patients. EbioMedicine 2015, 2, 2080–2086. [Google Scholar] [CrossRef]
- Mansuy, J.M.; Bendall, R.; Legrand-Abravanel, F.; Saune, K.; Miedouge, M.; Ellis, V.; Rech, H.; Destruel, F.; Kamar, N.; Dalton, H.R.; et al. Hepatitis E virus antibodies in blood donors, France. Emerg. Infect. Dis. 2011, 17, 2309–2312. [Google Scholar] [CrossRef]
- Faber, M.; Willrich, N.; Schemmerer, M.; Rauh, C.; Kuhnert, R.; Stark, K.; Wenzel, J.J. Hepatitis E virus seroprevalence, seroincidence and seroreversion in the German adult population. J. Viral Hepat. 2018, 25, 752–758. [Google Scholar] [CrossRef]
- Spada, E.; Pupella, S.; Pisani, G.; Bruni, R.; Chionne, P.; Madonna, E.; Villano, U.; Simeoni, M.; Fabi, S.; Marano, G.; et al. A nationwide retrospective study on prevalence of hepatitis E virus infection in Italian blood donors. Blood Transfus. 2018, 16, 413–421. [Google Scholar] [CrossRef]
- Mah, J.K.; Keck, M.; Chu, D.Y.; Sooryanarain, H.; Sahoo, M.K.; Lau, P.; Huang, C.; Weber, J.; Belanger, G.A.; Keck, Z.; et al. Hepatitis E virus seropositivity in an ethnically diverse community blood donor population. Vox Sang. 2023, 118, 674–680. [Google Scholar] [CrossRef]
- Feng, Y.; Feng, Y.M.; Wang, S.; Xu, F.; Zhang, X.; Zhang, C.; Jia, Y.; Yang, W.; Xia, X.; Yin, J. High seroprevalence of hepatitis E virus in the ethnic minority populations in Yunnan, China. PLoS ONE 2018, 13, e0197577. [Google Scholar] [CrossRef]
- Kamar, N.; Bendall, R.; Legrand-Abravanel, F.; Xia, N.S.; Ijaz, S.; Izopet, J.; Dalton, H.R. Hepatitis E. Lancet 2012, 379, 2477–2488. [Google Scholar] [CrossRef]
- Pallerla, S.R.; Schembecker, S.; Meyer, C.G.; Linh, L.T.K.; Johne, R.; Wedemeyer, H.; Bock, C.T.; Kremsner, P.G.; Velavan, T.P. Hepatitis E virus genome detection in commercial pork livers and pork meat products in Germany. J. Viral Hepat. 2021, 28, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Ferri, G.; Lauteri, C.; Festino, A.R.; Piccinini, A.; Olivastri, A.; Vergara, A. Hepatitis E Virus Detection in Hunted Wild Boar Liver and Muscle Tissues in Central Italy. Microorganisms 2022, 10, 1628. [Google Scholar] [CrossRef] [PubMed]
- Caruso, C.; Modesto, P.; Bertolini, S.; Peletto, S.; Acutis, P.L.; Dondo, A.; Robetto, S.; Mignone, W.; Orusa, R.; Ru, G.; et al. Serological and virological survey of hepatitis E virus in wild boar populations in northwestern Italy: Detection of HEV subtypes 3e and 3f. Arch. Virol. 2015, 160, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Lhomme, S.; Gallian, P.; Dimeglio, C.; Assal, A.; Abravanel, F.; Tiberghien, P.; Izopet, J. Viral load and clinical manifestations of hepatitis E virus genotype 3 infections. J. Viral Hepat. 2019, 26, 1139–1142. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Biomarkers | n (%) | 95% CI |
|---|---|---|
| anti HEV-IgG | 148/553 (26.8) | 23.1–30.6 |
| anti HEV-IgM | 3/553 (0.5) | 0.1–1.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cao, L.C.; Martin, V.; Linh, L.T.K.; Giang, T.T.; Chau, N.T.M.; Anh, T.N.P.; Nghia, V.X.; The, N.T.; My, T.N.; Sy, B.T.; et al. High Hepatitis E Virus (HEV) Seroprevalence and No Evidence of HEV Viraemia in Vietnamese Blood Donors. Viruses 2023, 15, 2075. https://doi.org/10.3390/v15102075
Cao LC, Martin V, Linh LTK, Giang TT, Chau NTM, Anh TNP, Nghia VX, The NT, My TN, Sy BT, et al. High Hepatitis E Virus (HEV) Seroprevalence and No Evidence of HEV Viraemia in Vietnamese Blood Donors. Viruses. 2023; 15(10):2075. https://doi.org/10.3390/v15102075
Chicago/Turabian StyleCao, Le Chi, Vanessa Martin, Le Thi Kieu Linh, Tran Thi Giang, Ngo Thi Minh Chau, Ton Nu Phuong Anh, Vu Xuan Nghia, Nguyen Trong The, Truong Nhat My, Bui Tien Sy, and et al. 2023. "High Hepatitis E Virus (HEV) Seroprevalence and No Evidence of HEV Viraemia in Vietnamese Blood Donors" Viruses 15, no. 10: 2075. https://doi.org/10.3390/v15102075
APA StyleCao, L. C., Martin, V., Linh, L. T. K., Giang, T. T., Chau, N. T. M., Anh, T. N. P., Nghia, V. X., The, N. T., My, T. N., Sy, B. T., Toan, N. L., Song, L. H., Bock, C.-T., & Velavan, T. P. (2023). High Hepatitis E Virus (HEV) Seroprevalence and No Evidence of HEV Viraemia in Vietnamese Blood Donors. Viruses, 15(10), 2075. https://doi.org/10.3390/v15102075