1. Introduction
Three-dimensional (3D) printing, also known by the term additive manufacturing (AM), rapid prototyping [
1], layered manufacturing [
2], or slicing [
3], is a rapidly developing technology that has gained wide acceptance and application in the medical field [
4], particularly in dentistry [
5], as it allows objects and models to be created in a short time, simultaneously and without the need for dental labor, starting from three-dimensional digital images. In the past, the main limitation to the use of 3D printers by a private dentist was the cost, but now, these devices are no longer limited to industrial use; it is an equipment that can be used directly at the dental office [
6] since it is a simple machine and compact in size, with an acceptable cost for professional dentists [
7,
8]. Three-dimensional printers are integrated into dental training to make models for teaching dental anatomy and for practicing procedures such as fillings and root canal treatments, replacing the use of extracted teeth that are prone to contamination [
9,
10]. In endodontics, 3D-printed guides based on CBCT data are used to find highly calcified canals in non-surgical root canal treatment and for an apicoectomy of posterior teeth in surgical endodontics [
11]. Metal structures that can be 3D-printed include removable partial dentures, overdentures, fixed prosthetic structures, and metal implants [
12]. Three-dimensional printing of dental crowns and bridges is one of the most appealing applications of 3D printing technology in dentistry [
13]. In oral surgery, CBCT, in combination with 3D printing, can also be used to create drilling or cutting guides that make surgery more predictable and quicker, as well as reducing its invasiveness [
14]. CAD/CAM osteotomy and repositioning guides are used to achieve virtual 3D planning of the patient’s case for operational simplification and reduction in surgical errors. Biomedical printing and direct metal laser sintering technologies can lead to prefabricated titanium miniplates to be used for screw fixation after bone repositioning [
15]. In orthodontics, the printer is often used for the production of surgical guides for the safe, studied, and controlled insertion of miniscrews, even in difficult locations, to save noble, nervous, and vascular structures [
16]. Another use is for orthodontic templates to carry out indirect orthodontic bonding, increasingly adopted to shorten the time spent in the chair [
17]. Patients’ growing desire for “invisible” alternative treatments has contributed to the spread of mass-produced clear aligners that are manufactured based on traditional impressions or digital scans of the patient’s teeth. With the advent of ever faster and better-performing 3D printers, it will be possible to switch from an STL file to a 3D-printed aligner directly in a few hours under the clinician’s guidance, shortening production times and costs [
18]; gnathological bites [
19,
20] and vacuum formed retainers [
21] can be printed using this technique, along with simple data processing software, resulting in very low production times and costs for both the patient and the operator.
The most common 3D printing techniques can be summarized into three types: stereolithography (SLA), Digital Light Processing (DLP), Polyjet, which includes the powder binder printer (PBP), PhotoPolymer Jetting (PPJ), Fused Deposition Modeling (FDM), Selective Laser Melting (SLM), and Selective Laser Sintering (SLS) [
22]. This study focused exclusively on DLP 3D printing technology due to its widespread use in dental applications, particularly for producing high-resolution and biocompatible resin components. DLP systems offer faster build times and improved detail reproduction compared to other photopolymerization techniques, making them clinically relevant. SLA and FDM differ significantly in their printing mechanisms, resolutions, and material properties: SLA achieves smoother surfaces but slower print times, while FDM uses thermoplastic filaments, which are less suitable for fine dental structures. These differences in material composition, layer bonding, and polymerization processes could affect mechanical properties such as flexural strength [
23].
There are many studies in the literature that have evaluated the deflection, maximum load, flexural strength, and elastic modulus of dental materials; however, these studies have always investigated the behavior of restorative materials traditionally used in dentistry, such as different generations and components of composites. Other studies have compared the flexural strength and Weibull characteristics of milled zirconia produced by additive stereolithography techniques [
24]. In a study, Keerthana B et al. evaluated the flexural strength of two different glass ionomer cements after immersion in juice [
25]. To date, few studies have investigated the topic regarding the different mechanical properties of 3D-printed specimens in dentistry. In 2020, a research was conducted to evaluate and compare the mechanical properties (flexural strength and surface hardness) of different materials and technologies for the fabrication of prostheses obtained by three different methods: polymerization, Computer-Aided Designing/Computer-Aided Manufacturing (CAD/CAM) technology, and 3D printing; it was seen that CAD/CAM materials had better mechanical properties than heat-cured and 3D-printed materials [
26]. In 2022, a systematic literature review and meta-analysis compared the physical and mechanical properties of 3D-printed temporary crowns and FDP resin materials with CAD/CAM-milled materials and conventional temporary resins and found that 3D-printed temporary crown and FDP resin materials have superior mechanical properties but inferior physical properties compared to CAD/CAM milling and other conventionally fabricated materials; 3D-printed temporary crowns and FDP materials can be used as an alternative to conventional and CAD/CAM-milled temporary materials in the long term [
27]. In January 2023, a study was conducted with the purpose of comparing the flexural strength of CAD-CAM-milled, 3D-printed, and conventional compression-molded base resin (DBR). CAD-CAM-milled DBRs showed the highest flexural strength compared to conventional compression-molded or 3D-printed DBRs [
28].
There are various factors that influence molded artifacts, thus affecting accuracy, processing time, and material properties such as the ultimate tensile stress, modulus elasticity, yield strength, impact strength, and fatigue-induced residual [
29]. For SLA or DLP manufacturing processes, the build angle indicates the direction in which the object is cut during the build-up process [
30]. The optimal build angle should provide a self-supporting geometry and thus require minimal support structure during the printing process [
29].
Previous studies have demonstrated that build orientation in DLP 3D printing can significantly influence the flexural strength of dental resins, with variations observed across different materials and orientations. These findings underscore the importance of systematically evaluating the mechanical performance of 3D-printed dental resins concerning build orientation to inform clinical applications and material selection. On the other hand, previous studies evaluating the effect of build angle on dimensional accuracy in DLP printing have reported minimal or inconsistent impacts, especially when proper calibration protocols are followed. It was hypothesized that orientation might also have a limited effect on flexural strength. However, mechanical behavior involves interlayer bonding and polymerization dynamics, which are not fully captured by dimensional accuracy alone. Therefore, this study aimed to test whether variations in build angle significantly affect flexural performance [
31,
32,
33]. In the literature, there are still no conclusive results for the optimal build angles in different dental applications. A study by Quintana et al. showed that tensile stress and modulus of elasticity are not significantly influenced by axis and position, but layout settings have a significant effect on both properties. Samples built on a corner showed better performance than the other layout [
34]. Another study showed that the direction of the molded layer perpendicular to the direction of loading is better than a parallel direction in terms of the compressive strength of the material [
35]. A study by Alharbi evaluated the influence of build angle and substrate configuration on the dimensional accuracy of full-coverage dental restorations molded using SLA technology, and the results of the study revealed that both factors influence the size and accuracy of molded parts [
36]. In their study, Unkovskiy et al. evaluated the influence of printing parameters on the flexural properties and precision of material samples, prismatic in shape and of the same size as those in the present study, which were printed with an SLA 3D printer. The print orientation influences the printing accuracy [
37].
Once the printing phase is completed, the post-processing steps can improve the performance of printed samples at an increased cost and greater time consumption. UV and/or microwave post-curing can improve the modulus of elasticity and ultimate strength of the samples, while increased laser power can also increase the strength of the sample.
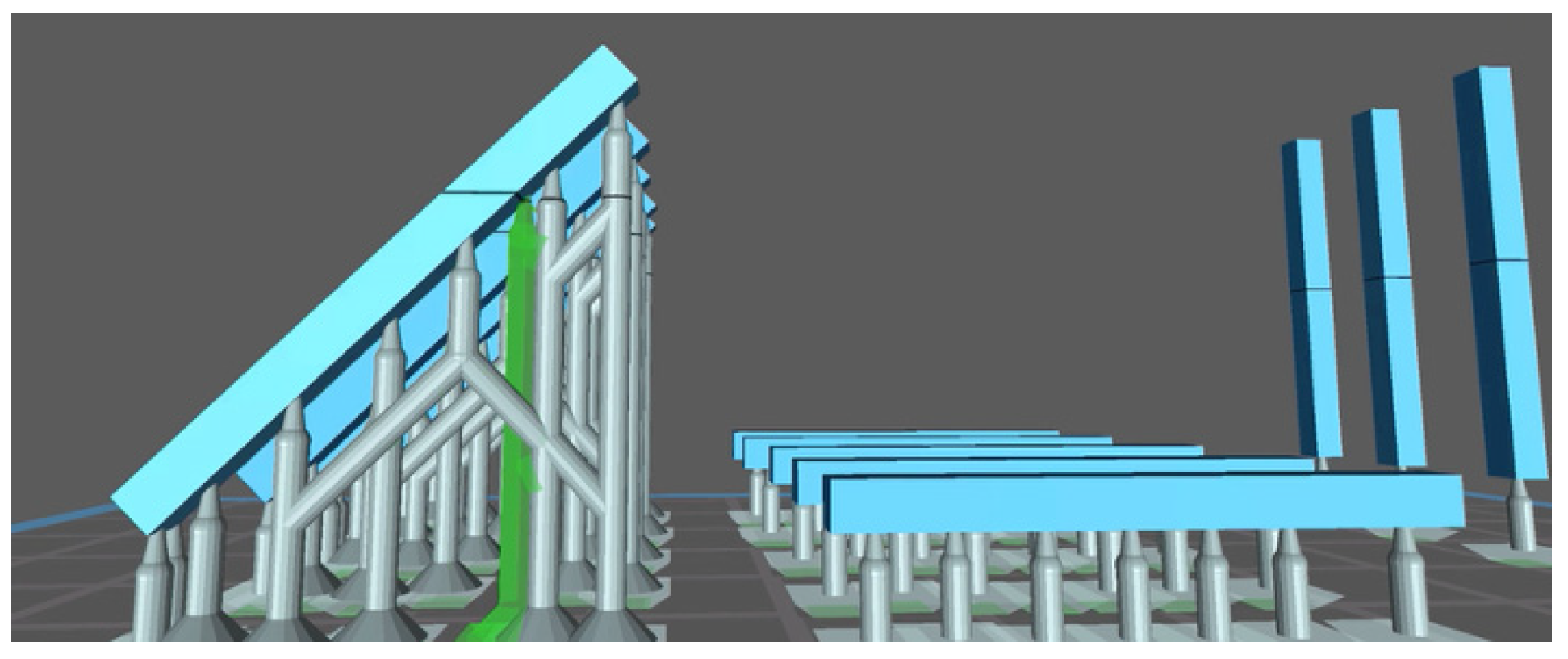
However, while several studies have investigated the dimensional accuracy or biocompatibility of dental resins, few have focused on their mechanical behavior—especially flexural strength—under different printing orientations. This is particularly relevant in DLP 3D printing, where the build angle can influence polymerization and interlayer bonding. Therefore, this study aims to address this gap by analyzing how the print orientation affects the flexural performance of two commonly used dental resins. The purpose of this study is to analyze the flexural strength of a series of 2 mm × 2 mm × 25 mm light-cured resin samples based on two different materials obtained from two different DLP 3D printers and to evaluate whether the flexural strength of the products can be affected by the different printing orientations (0°, 45°, and 90°) and the use of a different printer. The null hypothesis of this study is that there are no significant differences among the flexural strengths of the various groups tested.
4. Discussion
Three-dimensional (3D) printing technology produces three-dimensional objects based on patterns previously designed on a computer. This new production model is consistent with the assumptions of Industry 5.0, based on automation and digitization, which perfectly correlates with the assumptions of 3D printing technology [
44]. An important element of Industry 5.0 is 3D printing technology because of its favorable environmental orientation and production flexibility. Three-dimensional printing technology uses recycled materials such as powders. Therefore, it can be part of a circular economy, contributing to environmental protection.
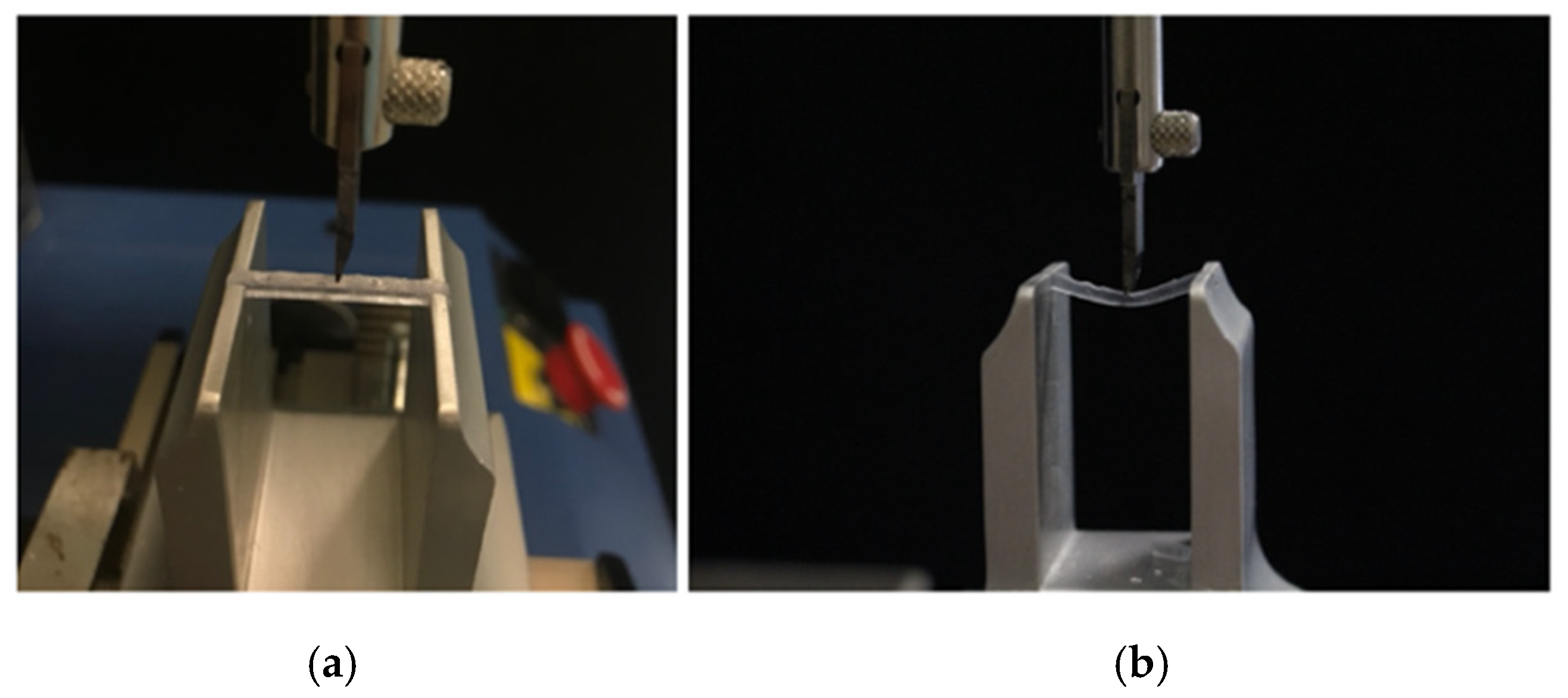
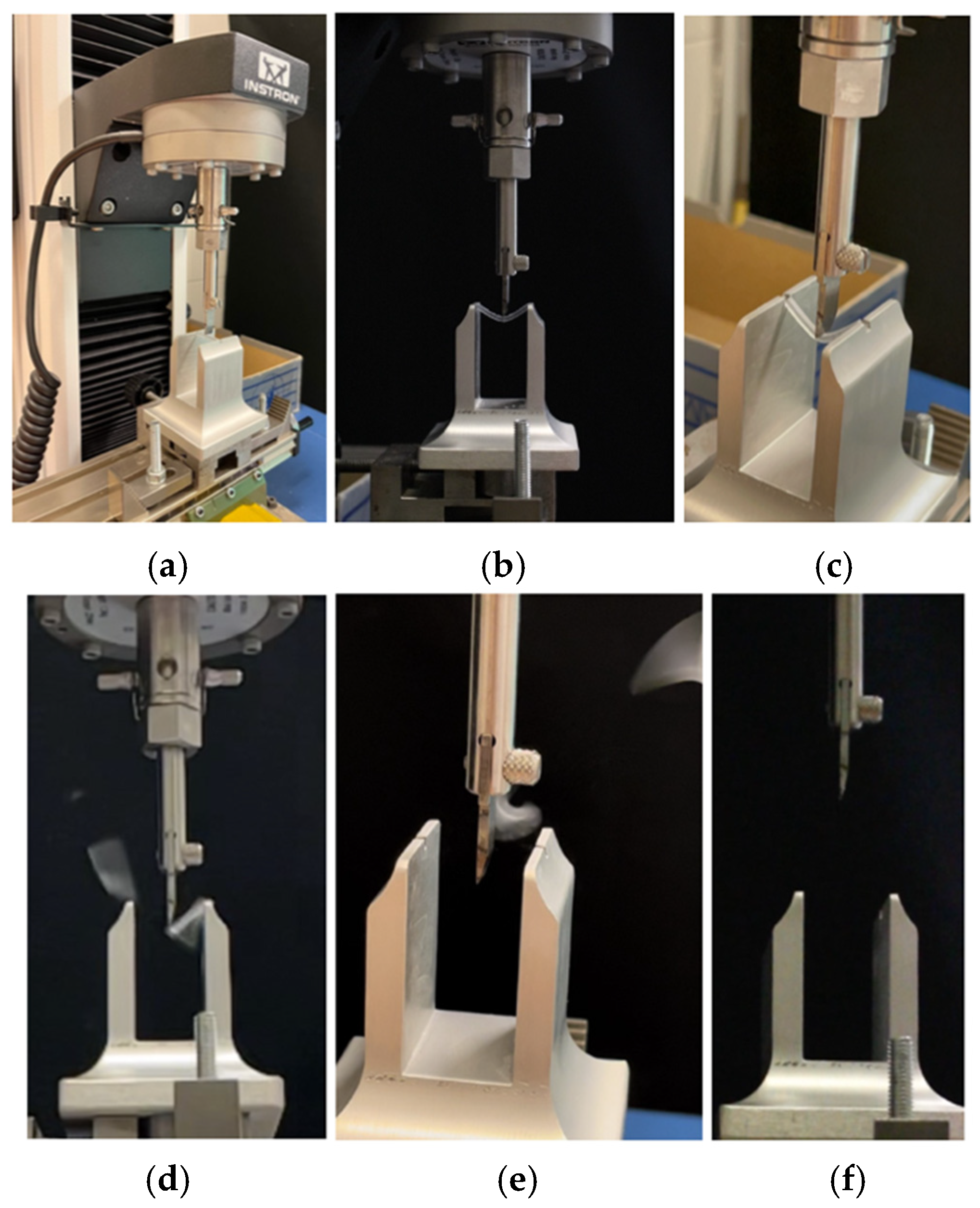
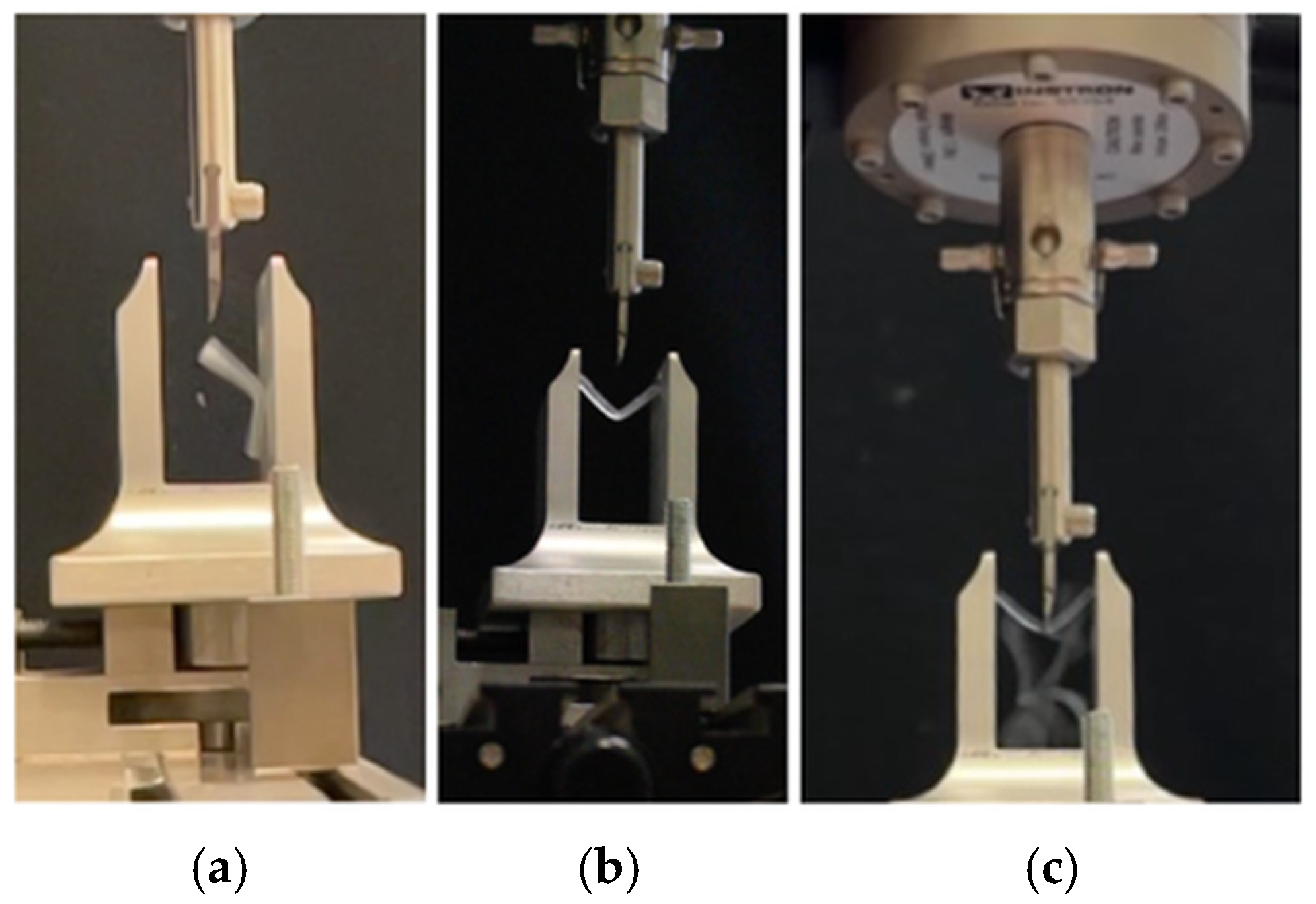
This in vitro study focused on the innovative topic of analyzing the different mechanical properties of resin materials printed with DLP 3D printing technology, with a special focus on the parameter of flexural strength. Flexural testing was chosen because it simulates the combined tensile and compressive stresses experienced by dental restorations during clinical function. This type of loading is particularly relevant for temporary crowns, bridges, and surgical guides, which are subject to masticatory forces and off-axis loading in the oral environment. Compared to isolated tensile or shear tests, flexural tests provide a more realistic assessment of a material’s ability to withstand functional intraoral stresses [
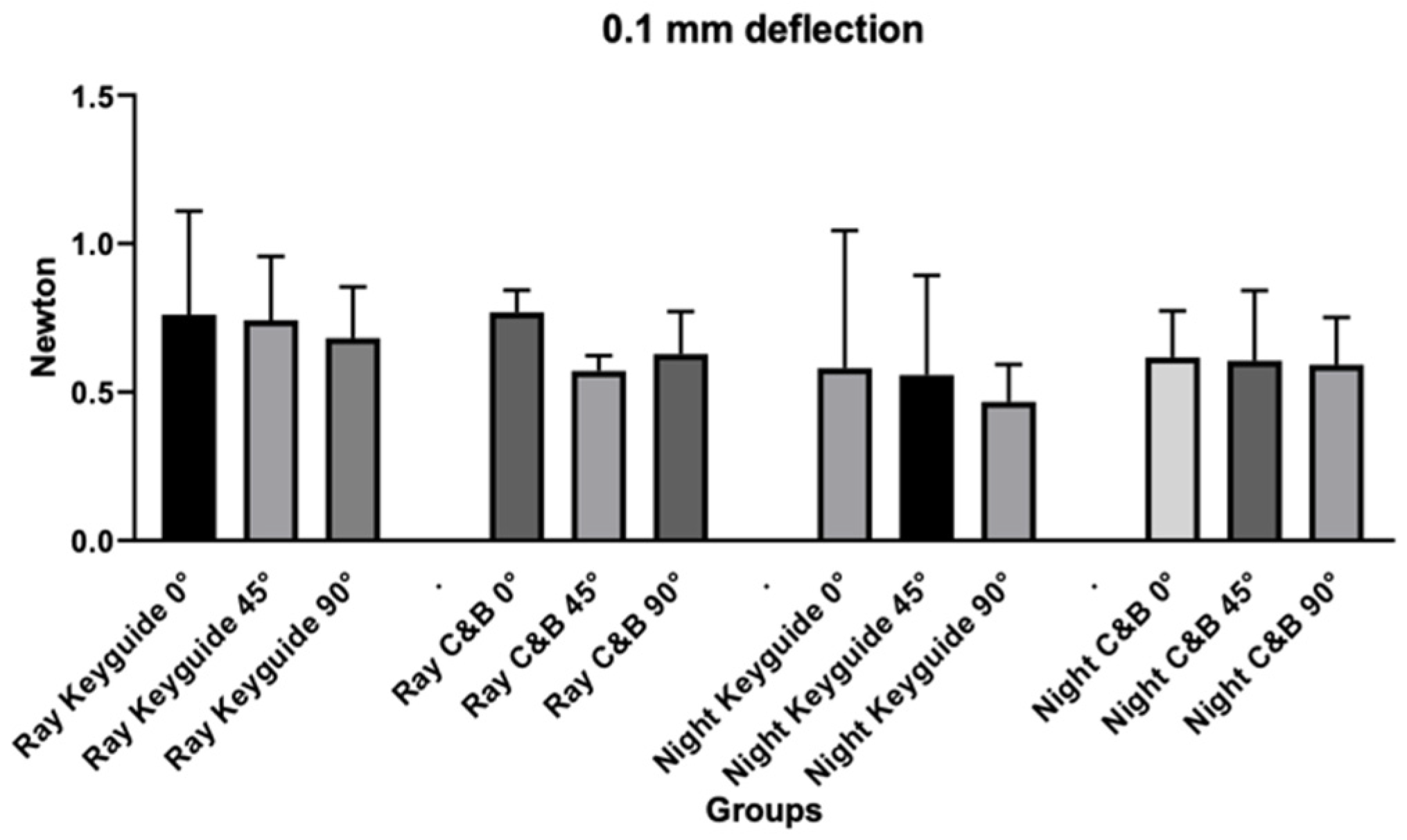
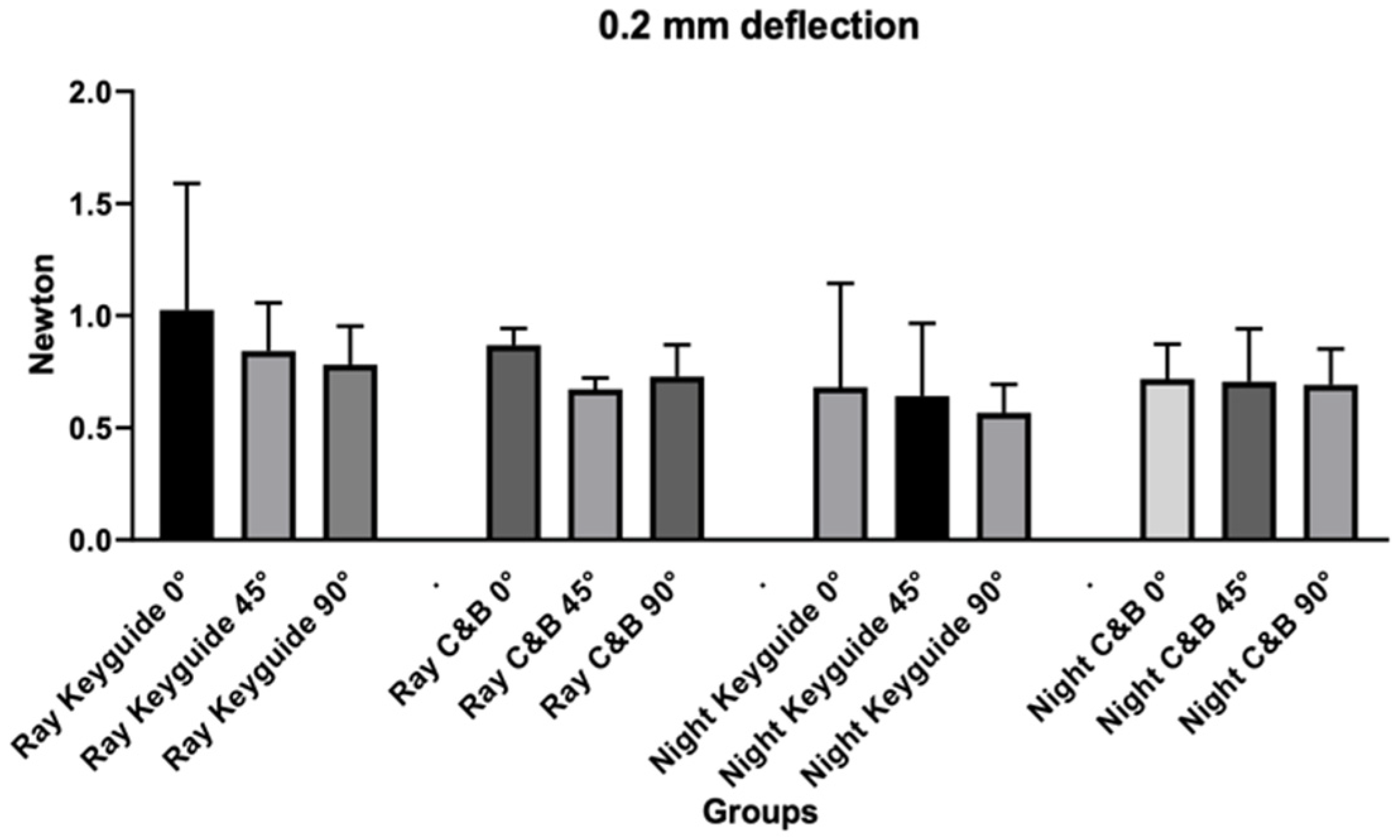
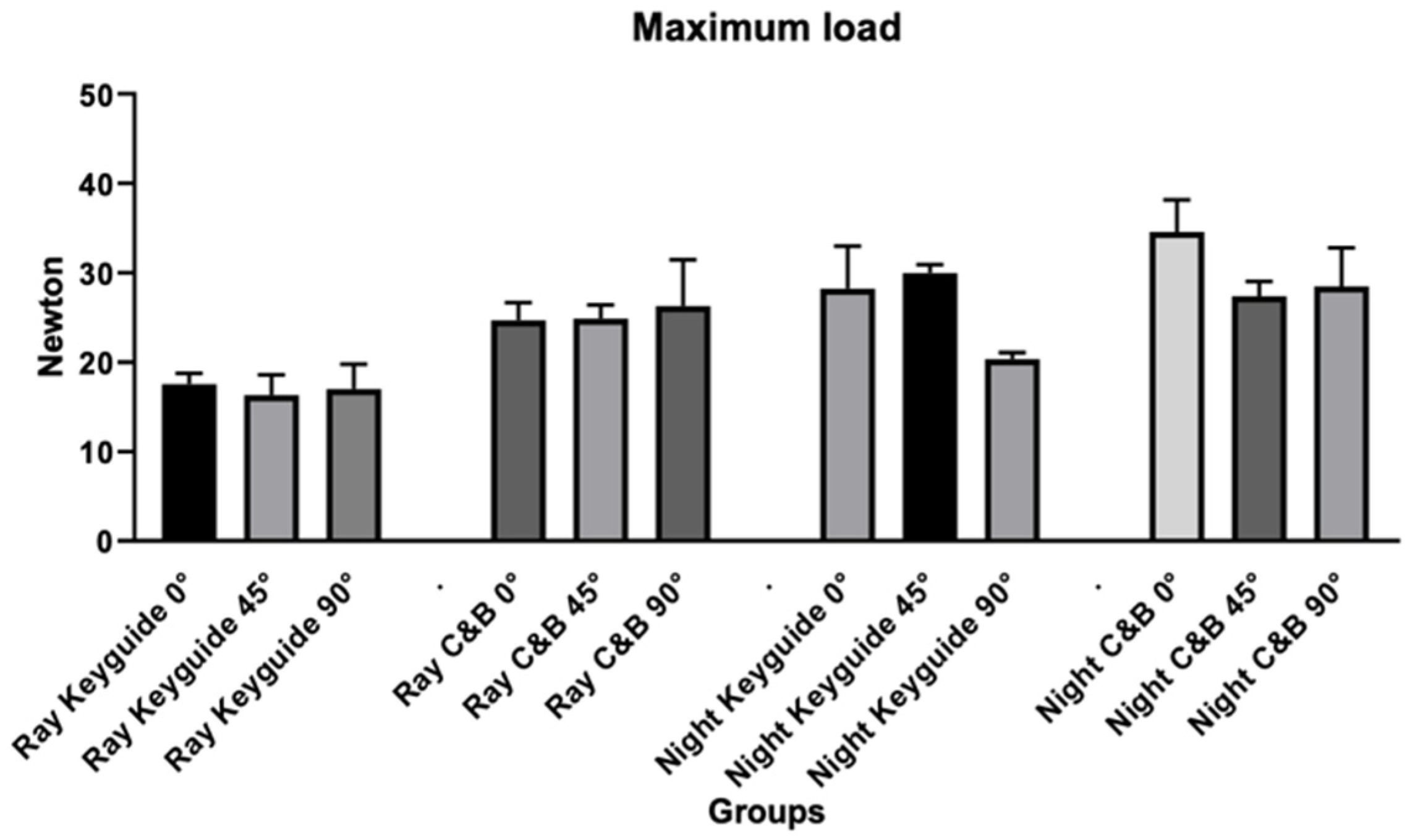
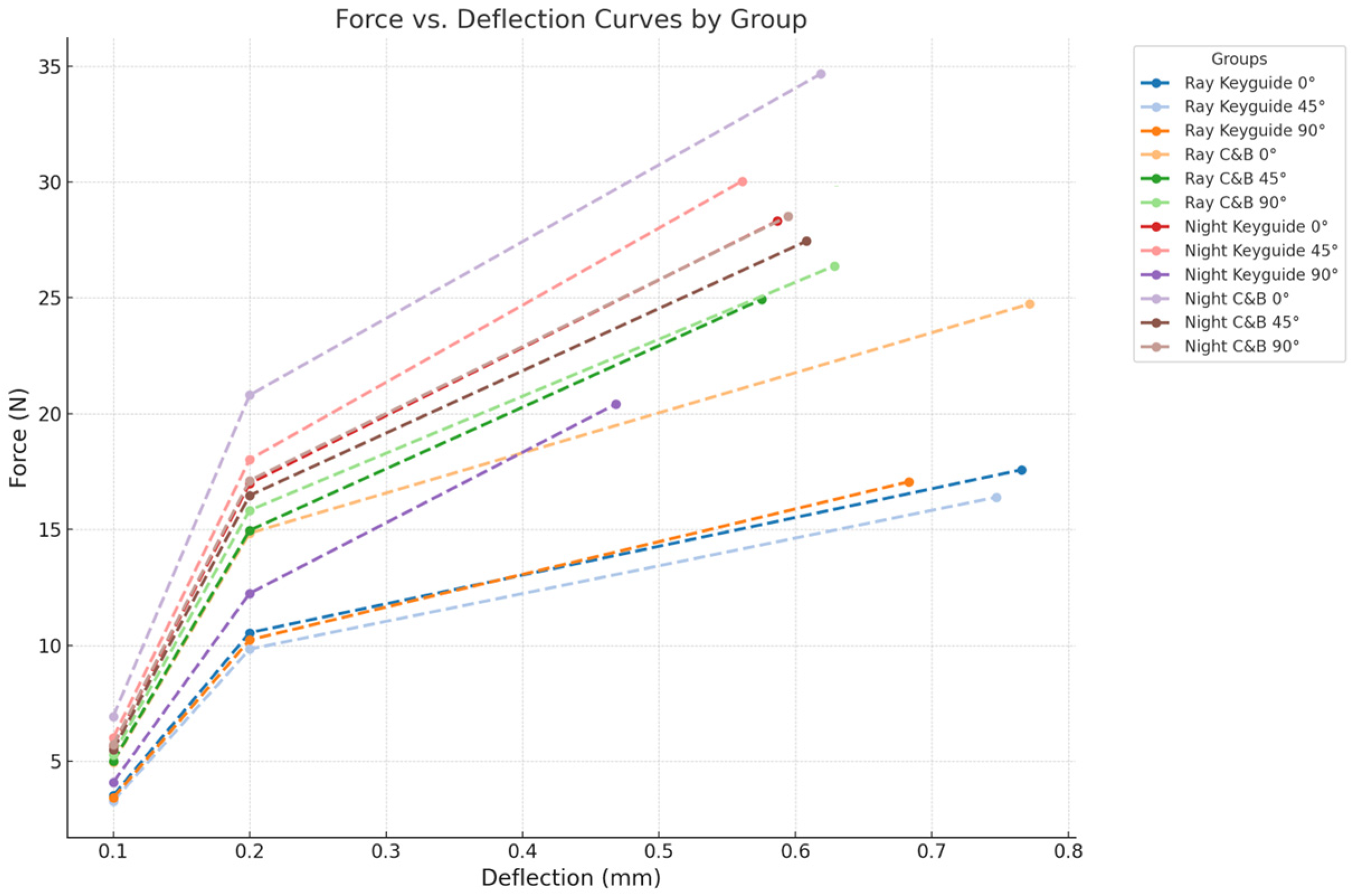
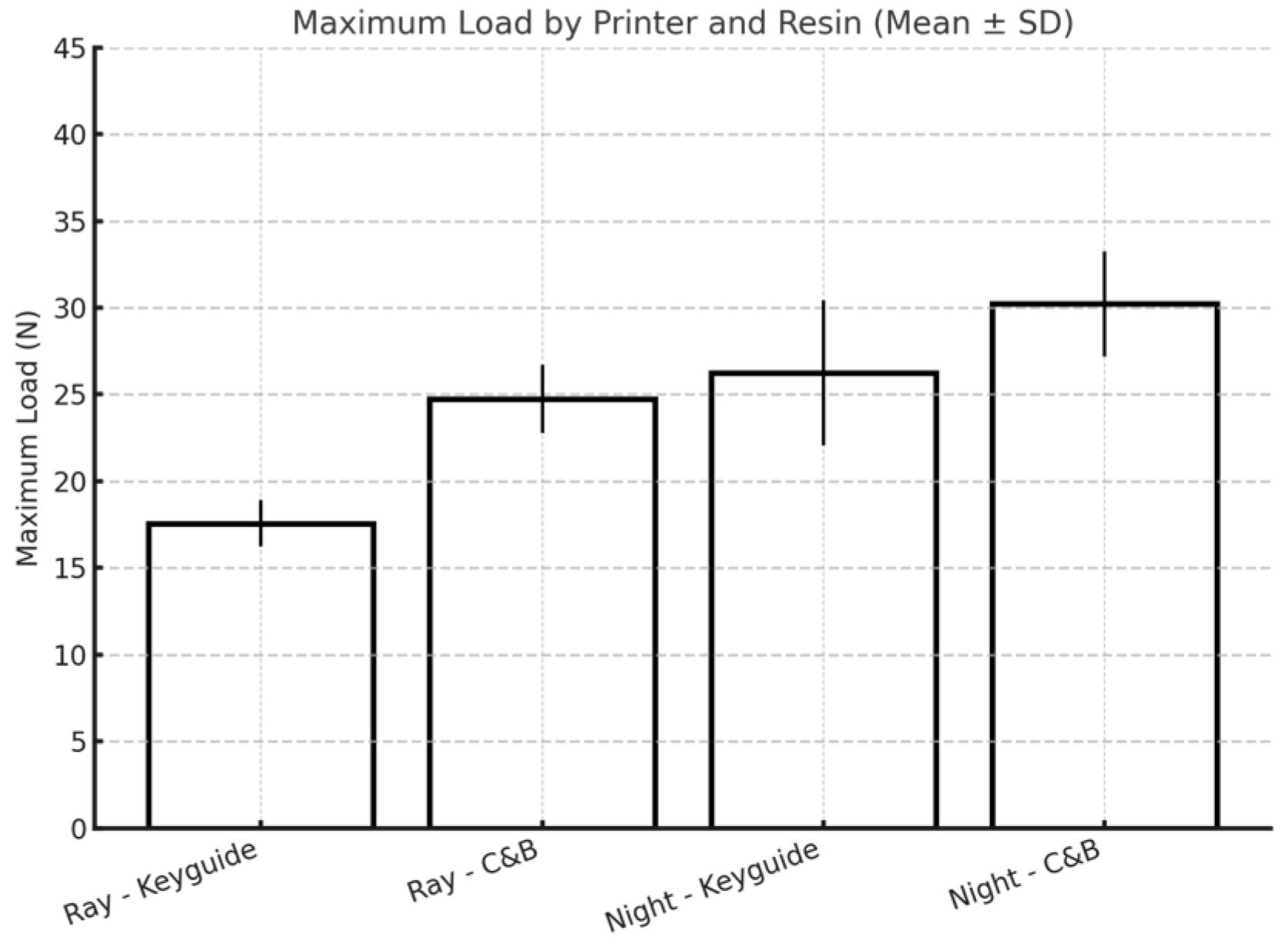
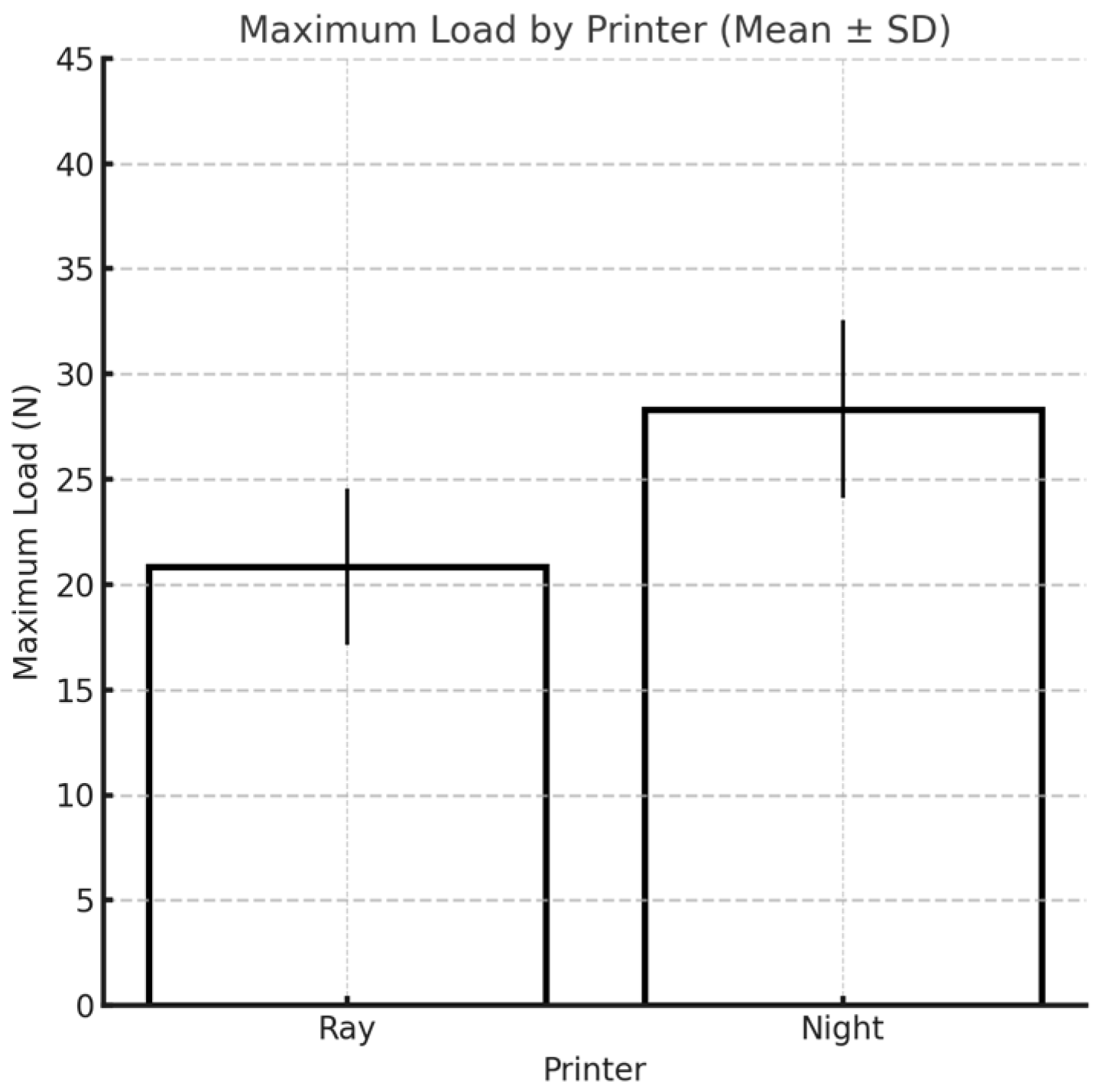
42]. This study was carried out by printing specimens using two different 3D printers (Sprintray Moonray S and Moon Night), with two different materials each (Keyguide and C&B), at three different angles (0°, 45°, and 90°). In light of the linear regressions obtained, it would appear that the printing orientation of the specimens does not affect the flexural strength of the two materials examined in any way. However, from Tukey’s post hoc test, at the maximum load, some differences emerged for both materials printed with the Moon Night printer depending on their build angle, specifically, between Keyguide at 0° and 90°, between C&B at 0° and 45°, and between Keyguide at 45° and 90°. Although significant differences in the maximum load were observed among Moon Night-printed specimens with different build orientations, these differences did not consistently translate into significant variations in flexural stress (MPa), which accounts for the cross-sectional dimensions. Notably, the significantly lower maximum load observed in Moon Night-printed Keyguide specimens at 90° may be attributed to the layer orientation being perpendicular to the direction of the applied load. This configuration can reduce interlayer cohesion and create weak planes that are more susceptible to delamination under bending stress. This observation is consistent with previous findings that vertically printed specimens often exhibit lower mechanical resistance due to suboptimal layer-to-layer bonding. Therefore, while the printing orientation appears to influence the absolute breaking force in some conditions, its effect on normalized mechanical performance remains limited within the scope of this study. This finding may support greater clinical flexibility in selecting build orientations based on practical factors—such as model geometry, print efficiency, or post-processing ease—without compromising mechanical reliability. This improved mechanical performance suggests that Moon Night-printed resins may be particularly well-suited for clinical applications requiring enhanced strength and dimensional stability, such as temporary crowns, bridges, and surgical guides that must withstand repetitive occlusal loading and insertion forces. In terms of flexural strength, the C&B resin showed consistently higher mean values compared to Keyguide, with the highest values recorded for specimens printed with the Moon Night printer at a 0° orientation (136.5 MPa). For the elastic modulus, the values also varied between resins and printers, with the highest value observed for C&B at 45° printed with the Moon Night printer (2353.3 MPa). These findings establish the mechanical trends among groups prior to inferential statistical evaluation. The most interesting results of this study concern the influence of printer type on all the variables tested: from the linear regressions, it would appear that printer type has an influence on the deflection at 0.1 mm and 0.2 mm; however, no statistically significant results emerged from Tukey’s post hoc test. Based on the results, it would appear that the type of printer has a statistically significant effect on the maximum load. The finding of such a result could depend on the better-performing construction characteristics of the Moon Night printer compared to the Sprintray printer. The Moon Night printer may incorporate improved light distribution systems, higher-resolution LCD components, or more efficient software calibration algorithms.
Recent studies have confirmed that the mechanical performance of 3D-printed orthodontic aligners is significantly influenced by both the printing technology and post-processing protocols employed. In particular, variables such as printing orientation (0°, 45°, and 90°) and resin thickness have been shown to affect flexural strength. A 2025 study by Khalil et al. demonstrated that although no statistically significant differences were found among the various printing orientations, aligners printed with a greater thickness (0.7 mm) exhibited significantly higher flexural strength compared to those with a thickness of 0.5 mm [
45]. Additional research has highlighted the role of post-curing conditions (particularly curing in an oxygen-free environment) in enhancing the degree of conversion and the resulting mechanical properties of the material [
46]. Neoh et al. reported that centrifugation prior to post-curing in glycerin led to specimens with reduced surface roughness, improved light transmittance, greater hardness, and enhanced color stability. However, this method also resulted in an increase in material thickness, which may necessitate design modifications to ensure proper fit to the dental model [
47].
It is necessary to take into account a number of variables not directly related to printer properties that might have influenced the results obtained. When analyzing the differences between the two printers more closely, it would seem that it is the software that matters the most, while the hardware of the two printers is almost identical. There are studies that have evaluated the differences between 3D printers with different hardware. For example, Tsolakis IA et al. compared the accuracy, in terms of truthfulness and precision, of a 3D printer with a liquid crystal display (LCD) versus a Direct Light Processing (DLP) 3D printer for printing dental models. Therefore, two different printers were used in that study in terms of 3D printing technology. It was seen that the DLP 3D printer is more accurate in terms of printing the dental model than the LCD 3D printer; however, both DLP and LCD printers can be used accurately to print dental models for the fabrication of orthodontic appliances [
48]. Few studies, however, have investigated the difference in accuracy between two printers with the same hardware but different printing software. The use of two different software programs for sample design and printing may have affected the dimensional calibration of printed specimens, leading to the printing of specimens of different sizes, depending on their degree of expansion or contraction [
49,
50]. The tolerance and dimensional accuracy tests to be performed with the RayWare software and the printing and tolerance parameters preset with the Chitubox software could have resulted in inaccuracies in the size of the printed specimens. Using one software to design and print the samples with the two different printers could have made the dimensional calibration of the samples more uniform [
51]. In summary, the linear regressions performed in this study showed no effect of the printing angle; rather, there was an effect of the printer and an effect of the material only at the maximum load. The observed differences in mechanical performance between Keyguide and C&B resins, as well as between the MoonRay and Moon Night printers, may be partly attributed to variations in resin composition and slicing software calibration. Previous studies have shown that differences in monomer formulation and filler content can significantly influence flexural strength and polymerization behavior [
33,
52]. Moreover, the use of different slicing software, with their unique exposure settings and layer processing algorithms, can impact dimensional accuracy and interlayer bonding quality. These factors highlight the importance of standardizing not only materials but also software parameters in future investigations.
A limitation of this study involves the use of different slicing and printer software—RayWare and Chitubox—for the two printers. Since each printer is compatible with its own software, it was not possible to isolate the effect of the software from that of the printer itself. Differences in dimensional calibration or print parameters introduced by the software may have influenced the mechanical performance of the printed specimens. Future studies should aim to evaluate the independent impact of slicing software on the quality of the final parts. Printing orientation is another factor that could have affected printing accuracy: for example, the first layers of the 0° specimens require additional exposure time to be light-cured to ensure their secure adhesion to the substrates; the same is true for the 90° specimens, which need to be cured longer to help achieve the predetermined length. Only three printing angles (0°, 45°, and 90°) were tested. Although they represent standard reference orientations, future investigations will aim to assess additional build orientations, such as 30° and 60°, to provide a more detailed understanding of how intermediate angles may influence the mechanical performance of 3D-printed dental resins. Alterations in specimen size could also arise as a result of the removal of support structures, particularly for the 0° and 45° groups, a procedure that inevitably damages specimens of these sizes. Regarding alterations in specimen size, it must be considered that for both printers, the layer height was set to 0.05 mm, which means that variations less than 0.05 mm are not controllable by either printer [
53]. All of these variables could have impacted the final measurements of the specimens by causing relatively large deviations that could have resulted in overlapping effects with those of printing. This study focused exclusively on flexural strength and maximum load, which are important indicators of mechanical performance. Other relevant mechanical properties, such as surface hardness, tensile strength, and fatigue resistance (important for dental applications), were not assessed. These aspects should be included in future studies to provide a more comprehensive mechanical characterization of 3D-printed dental materials. A small sample size is commonly used in preliminary in vitro studies, and it may reduce the statistical power and limit the generalizability of the findings, especially when considering the variability of the 3D printing process. Future studies with larger sample sizes, involving other printers and materials, are recommended to confirm and strengthen these observations.
5. Conclusions
This in vitro study evaluated the flexural strength of 3D-printed specimens produced using two different resin materials and printed with two printer models and three build orientations. Within the limitations of this study, the results suggest that while printing orientation did not have a consistent effect across all groups, significant differences were observed in specific conditions (particularly with the Moon Night printer), where build angle influenced maximum load values. We found that 90° printing generally exhibited less favorable mechanical performance, particularly with the Keyguide resin, while 0° and 45° orientations often yielded higher flexural strength and better deformation resistance. Flexural strength is a key determinant of the clinical performance of 3D-printed dental devices, particularly those exposed to repetitive mechanical stress, such as temporary crowns, bridges, and aligners. Intraorally, these restorations must endure bending forces resulting from occlusion, parafunctional habits, and the mechanical demands of insertion and removal. Inadequate flexural resistance may lead to deformation, fracture, or premature failure, ultimately compromising fit, function, and patient comfort. As such, evaluating how processing parameters—especially, build orientation—affect flexural behavior is essential to optimize material selection and anticipate clinical longevity.
The C&B resin consistently demonstrated superior mechanical properties compared to the Keyguide resin, regardless of orientation. Furthermore, specimens printed with the Moon Night printer showed higher maximum load and flexural stress values across both materials compared to those printed with the Sprintray MoonRay S. These differences may be attributed to more advanced construction features of the Moon Night printer or a more accurate dimensional calibration during the printing process. Taken together, these findings highlight the importance of selecting the appropriate combination of resin, printer, and printing orientation to ensure the optimal mechanical performance of 3D-printed dental components. Further research should investigate the long-term behavior and clinical relevance of these materials under functional loading conditions. Additionally, future studies should evaluate the mechanical performance of these materials under simulated oral conditions (thermal cycling, humidity, and dynamic loading) to better approximate clinical use. Furthermore, standardizing dimensional calibration through the use of a single slicing software or external calibration references for both printers should be considered in future studies to minimize variability introduced by different software environments.



 ,
, 




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}