
Development of Custom Anatomic Healing Abutment Based on Cone-Beam Computer Tomography Measurement on Human Teeth Cross-Section

 ,
,
Abstract
:1. Introduction
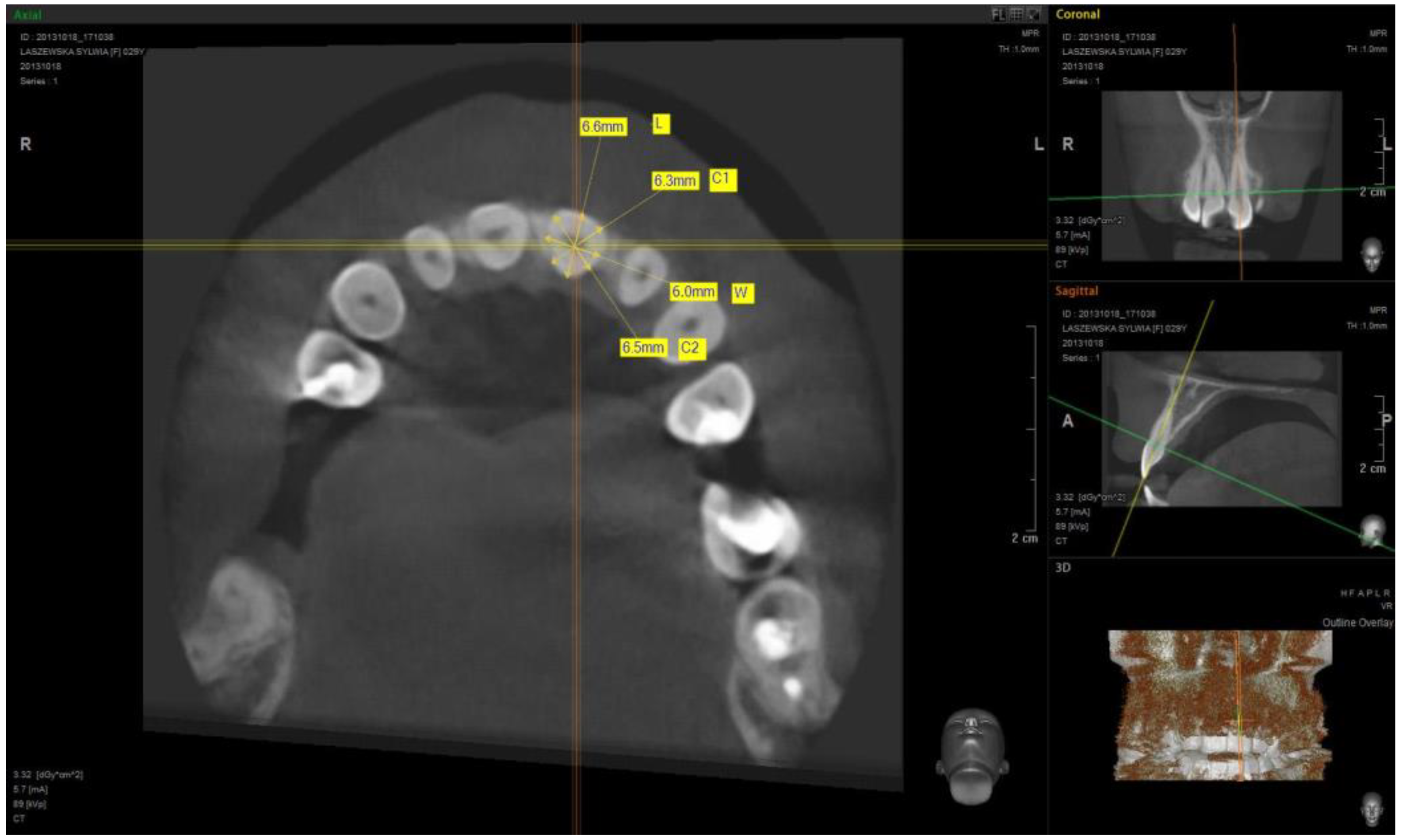
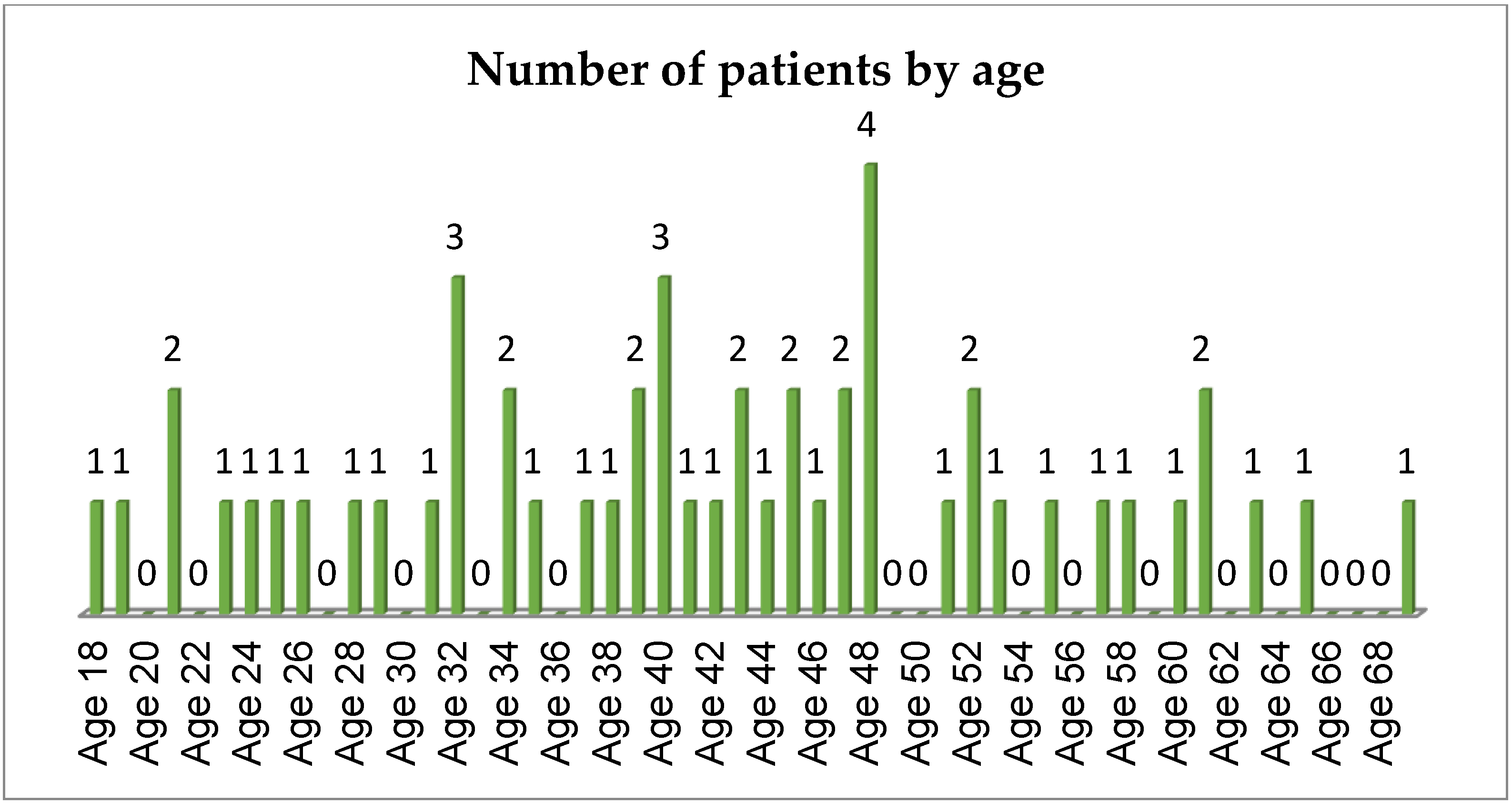
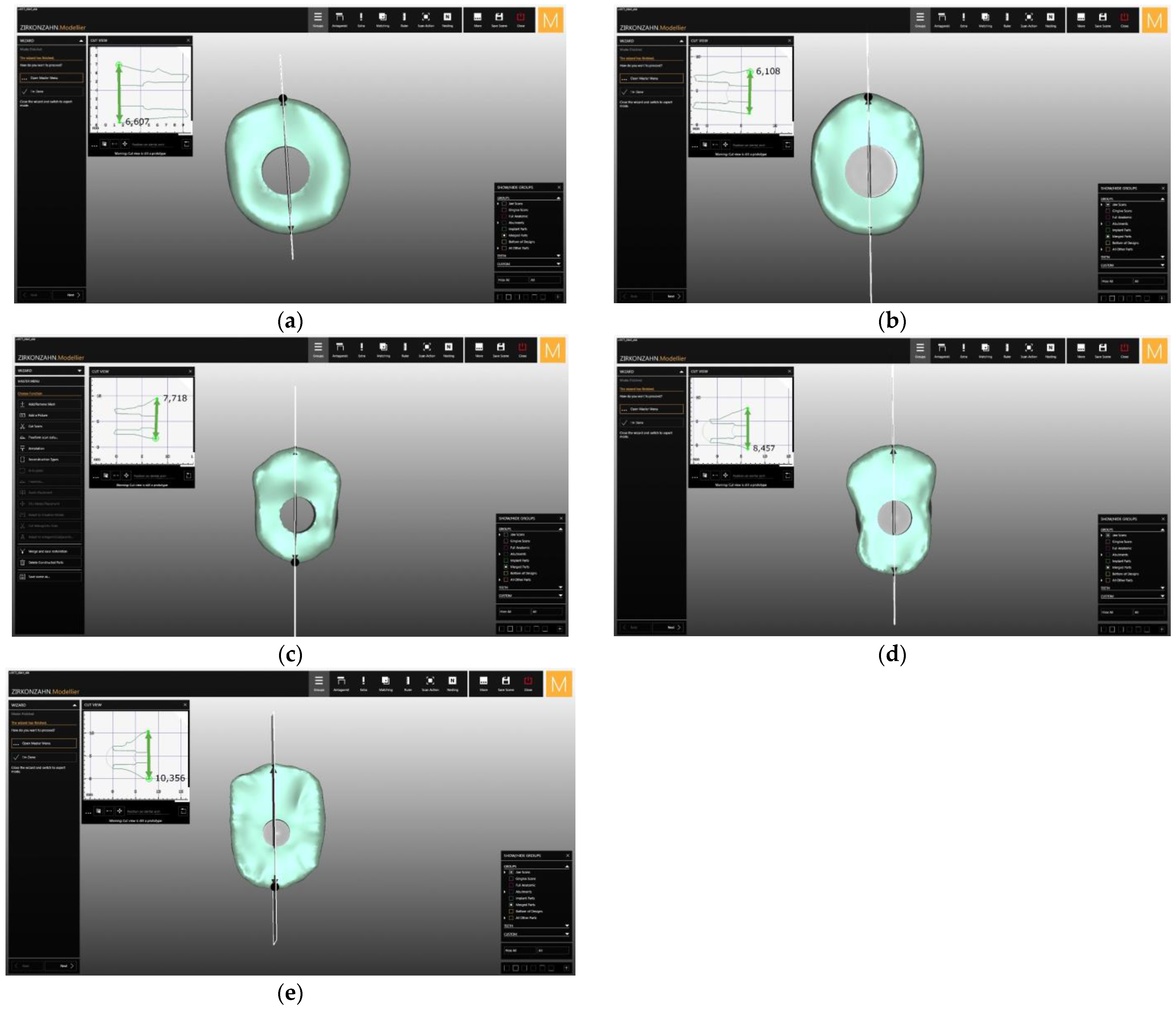
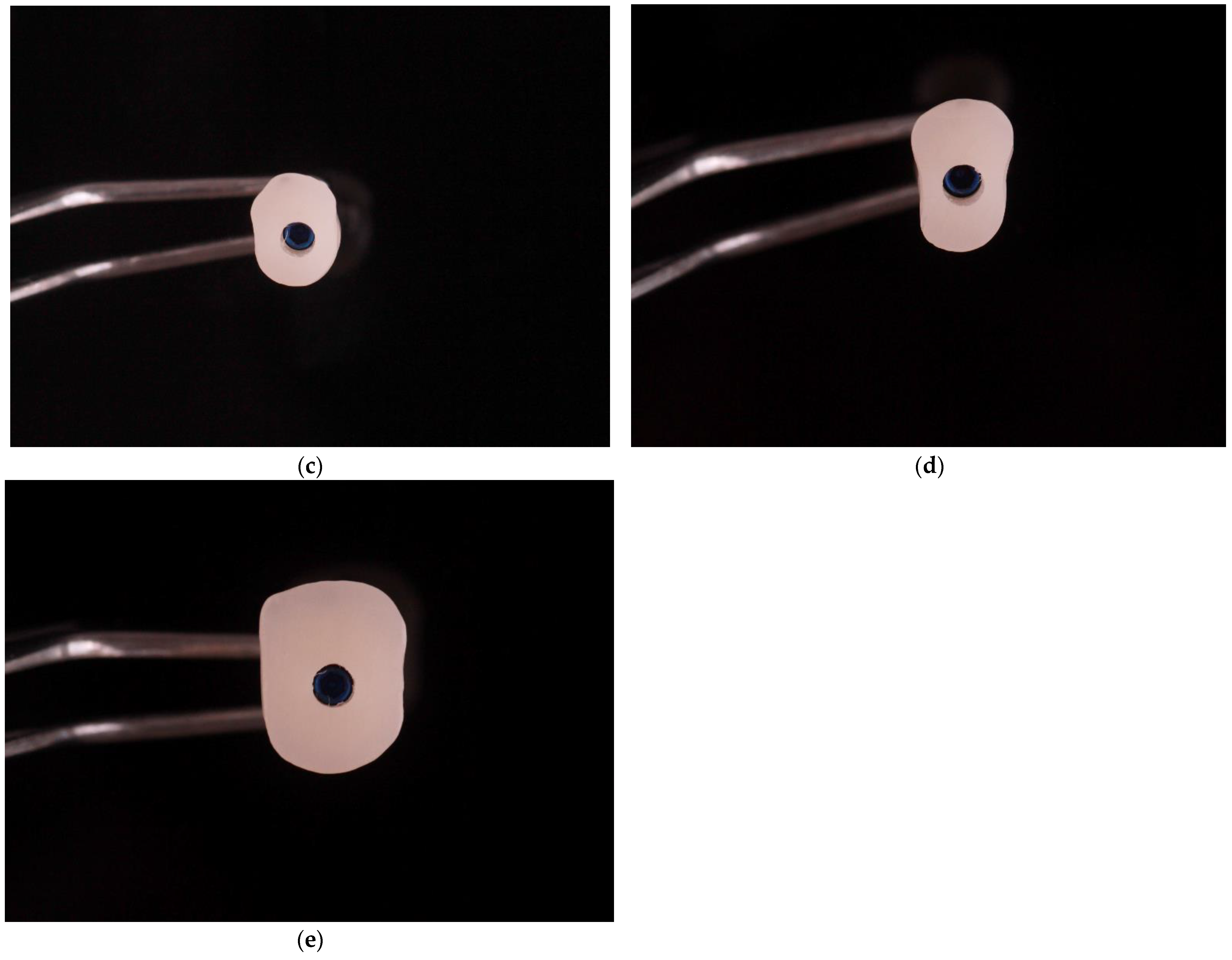
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Linkevicius, T.; Puisys, A.; Steigmann, M.; Vindasiute, E.; Linkeviciene, L. Influence of Vertical Soft Tissue Thickness on Crestal Bone Changes Around Implants with Platform Switching: A Comparative Clinical Study. Clin. Implant Dent. Relat. Res. 2015, 17, 1228–1236. [Google Scholar] [CrossRef]
- Linkevicius, T.; Puisys, A.; Linkeviciene, L.; Peciuliene, V.; Schlee, M. Crestal Bone Stability around Implants with Horizontally Matching Connection after Soft Tissue Thickening: A Prospective Clinical Trial. Clin. Implant Dent. Relat. Res. 2015, 17, 497–508. [Google Scholar] [CrossRef]
- Linkevičius, T.; Vaitelis, J. The effect of zirconia or titanium as abutment material on soft peri-implant tissues: A systematic review and meta-analysis. Clin. Oral Implants Res. 2015, 26 (Suppl. S11), 139–147. [Google Scholar] [CrossRef] [PubMed]
- Pieruska, M.; Pietruski, J. Periodontologiczno-Implantologiczna Chirurgia Plastyczna, 2nd ed.; Wydawnictwo Czelej: Lublin, Poland, 2014; pp. 22–32. [Google Scholar]
- Berglundh, T.; Lindhe, J.; Ericsson, I.; Marinello, C.P.; Liljenberg, B.; Thornsen, P. The soft tissue barrier at implants and teeth. Clin. Oral Implants Res. 1991, 2, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Kao, R.T.; Fagan, M.C.; Conte, G.J. Thick vs. think gingival biotypes: A key determinant in treatment for dental implants. J. Calif. Dent. Assoc. 2008, 36, 193–198. [Google Scholar] [PubMed]
- Kohl, J.T.; Zander, H.A. Morphology of interdental gingival tissues. Oral Surg. Oral Med. Oral Pathol. 1961, 14, 287–295. [Google Scholar] [CrossRef]
- Kois, J.C. Altering Gingival Levels: The Restorative Connection Part I: Biologic Variables. J. Esthet. Restor. Dent. 1994, 6, 3–7. [Google Scholar] [CrossRef]
- Lai, H.-C.; Zhang, Z.-Y.; Wang, F.; Zhuang, L.-F.; Liu, X.; Pu, Y.-P. Evaluation of soft-tissue alteration around implant-supported single-tooth restoration in the anterior maxilla: The pink esthetic score. Clin. Oral Implants Res. 2008, 19, 560–564. [Google Scholar] [CrossRef]
- Grunder, U.; Gracis, S.; Capelli, M. Influence of the 3-D bone-to-implant relationship on esthetics. Int. J. Periodontics Restor. Dent. 2005, 25, 113–119. [Google Scholar]
- Berglundh, T.; Lindhe, J.; Jonsson, K.; Ericsson, I. The topography of the vascular systems in the periodontal and peri-implant tissues in the dog. J. Clin. Periodontol. 1994, 21, 189–193. [Google Scholar] [CrossRef]
- Lidnhe, J.; Berglundh, T.; Ericsson, I.; Liljenberg, B.; Marinello, C.P. Experimental breakdown of periimplant and periodontal tissues. A study in the beagle dog. Clin. Oral Implants Res. 1992, 3, 9–16. [Google Scholar]
- Rojas-Vizcaya, F. BioManagement Complex: The basis for predictable esthetic transitional contour. Insight 2008, 10, 4–5. [Google Scholar]
- Rojas-Vizcaya, F. Biological aspects as a rule for single implant placement. The 3A-2B rule: A clinical report. J Prosthodont. 2013, 7, 575–580. [Google Scholar] [CrossRef]
- Priest, G. Predictability of soft tissue form around single-tooth implant restorations. Int. J. Periodontics Restor. Dent. 2003, 23, 19–28. [Google Scholar]
- Gastaldo, J.F.; Cury, P.R.; Sendyk, W.R. Effect of the Vertical and Horizontal Distances Between Adjacent Implants and Between a Tooth and an Implant on the Incidence of Interproximal Papilla. J. Periodontol. 2004, 75, 1242–1246. [Google Scholar] [CrossRef]
- Tarnow, D.P.; Magner, A.W.; Fletcher, P. The Effect of the Distance from the Contact Point to the Crest of Bone on the Presence or Absence of the Interproximal Dental Papilla. J. Periodontol. 1992, 63, 995–996. [Google Scholar] [CrossRef] [Green Version]
- Weigl, P.; Trimpou, G.; Grizas, E.; Hess, P.; Nentwig, G.-H.; Lauer, H.-C.; Lorenz, J. All-ceramic versus titanium-based implant supported restorations: Preliminary 12-months results from a randomized controlled trial. J. Adv. Prosthodont. 2019, 11, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Proussaefs, P. Custom CAD-CAM healing abutment and impression coping milled from a poly(methyl methacrylate) block and bonded to a titanium insert. J. Prosthet. Dent. 2016, 116, 657–662. [Google Scholar] [CrossRef] [PubMed]
- Alshhrani, W.M.; Al Amri, M.D. Customized CAD-CAM healing abutment for delayed loaded implants. J. Prosthet. Dent. 2016, 116, 176–179. [Google Scholar] [CrossRef] [PubMed]
- Schoenbaum, T.R. Abutment Emergence Profile and Its Effect on Peri-Implant Tissues. Compend. Contin. Educ. Dent. 2015, 36, 474–479. [Google Scholar] [PubMed]
- Blanco-Carrion, J.; Pico, A.; Caneiro, L.; Nóvoa, L.; Batalla, P.; Martín-Lancharro, P. Effect of abutment height on interproximal implant bone level in the early healing: A randomized clinical trial. Clin. Oral Implants Res. 2018, 29, 108–117. [Google Scholar] [CrossRef]
- Gerard, J. Lemongello Customized provisional abutment and provisional restoration for an immediately-placed implant. Pract. Proced. Aesthetic Dent. 2007, 19, 419–424. [Google Scholar]
- Hahnel, S.; Wieser, A.; Lang, R.; Rosentritt, M. Biofilm formation on the surface of modern implant abutment materials. Clin. Oral Implants Res. 2015, 26, 1297–1301. [Google Scholar] [CrossRef]
- Conejo, J.; Atria, P.J.; Hirata, R.; Blatz, M.B. Copy milling to duplicate the emergence profile for implant-supported restorations. J. Prosthet. Dent. 2020, 123, 671–674. [Google Scholar] [CrossRef] [PubMed]
- Hartman, M.J. A Workflow to Design and Fabricate a Customized Healing Abutment from a Dynamic Navigation Virtual Treatment Plan. Compend. Contin. Educ. Dent. 2021, 42, 86–92. [Google Scholar] [PubMed]
- Gonzalez-Martin, O.; Lee, E.; Weisgold, A.; Veltri, M.; Su, H. Contour Management of Implant Restorations for Optimal Emergence Profiles: Guidelines for Immediate and Delayed Provisional Restorations. Int. J. Periodontics Restor. Dent. 2020, 40, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Wittneben, J.-G.; Buser, D.; Belser, U.C.; Brägger, U. Peri-implant soft tissue conditioning with provisional restorations in the esthetic zone: The dynamic compression technique. Int. J. Periodontics Restor. Dent. 2013, 33, 447–455. [Google Scholar] [CrossRef] [Green Version]
- Orozco-Varo, A.; Arroyo-Cruz, G.; Martinez-De-Fuentes, R.; Jiménez-Castellanos, E. Biometric analysis of the clinical crown and the width/length ratio in the maxillary anterior region. J. Prosthet. Dent. 2015, 113, 565.e2–570.e2. [Google Scholar] [CrossRef]
- Scoble, H.O.; White, S.N. Compound complex curves: The authentic geometry of esthetic dentistry. J. Prosthet. Dent. 2014, 111, 448–454. [Google Scholar] [CrossRef]
- Janakievski, J. Case report: Maintenance of gingival form following immediate implant placement—The custom healing abutment. Adv. Esthet. Interdiscip. Dent. 2007, 3, 24–28. [Google Scholar]
- Abrahamsson, I.; Berglundh, T.; Lindhe, J. The mucosal barrier following abutment dis/reconnection. An experimental study in dogs. J. Clin. Periodontol. 1997, 24, 568–572. [Google Scholar] [CrossRef] [PubMed]
- Sailer, I.; Philipp, A.; Zembic, A.; Pjetursson, B.E.; Hämmerle, C.H.F.; Zwahlen, M. A systematic review of the performance of ceramic and metal implant abutments supporting fixed implant reconstructions. Clin. Oral Implants Res. 2009, 20 (Suppl. S4), 4–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zembic, A.; Bösch, A.; Jung, R.E.; Hämmerle, C.H.F.; Sailer, I. Five-year results of a randomized controlled clinical trial comparing zirconia and titanium abutments supporting single-implant crowns in canine and posterior regions. Clin. Oral Implants Res. 2013, 24, 384–390. [Google Scholar] [CrossRef]
- Park, S.E.; Da Silva, J.D.; Weber, H.-P.; Ishikawa-Nagai, S. Optical phenomenon of peri-implant soft tissue. Part I. Spectrophotometric assessment of natural tooth gingiva and peri-implant mucosa. Clin. Oral Implants Res. 2007, 18, 569–574. [Google Scholar] [CrossRef]
- Scarano, A.; Piattelli, M.; Caputi, S.; Favero, G.A.; Piattelli, A. Bacterial Adhesion on Commercially Pure Titanium and Zirconium Oxide Disks: An In Vivo Human Study. J. Periodontol. 2004, 75, 292–296. [Google Scholar] [CrossRef]
- Welander, M.; Abrahamsson, I.; Berglundh, T. The mucosal barrier at implant abutments of different materials. Clin. Oral Implants Res. 2008, 19, 635–641. [Google Scholar]
- Pabst, A.M.; Walter, C.; Bell, A.; Weyhrauch, M.; Schmidtmann, I.; Scheller, H.; Lehmann, K.M. Influence of CAD/CAM zirconia for implant-abutment manufacturing on gingival fibroblasts and oral keratinocytes. Clin. Oral Investig. 2016, 20, 1101–1108. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Central Incisor | Lateral Incisor | Canine | First Premolar | First Molar | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| L | C1 | H | C2 | L | C1 | H | C2 | L | C1 | H | C2 | L | C1 | H | C2 | L | C1 | H | C2 | |
| Arithemic Average | 6.633 | 6.302 | 5.889 | 6.787 | 6.085 | 5.65 | 4.447 | 5.533 | 7.693 | 7.023 | 5.358 | 6.536 | 8.509 | 7.611 | 4.569 | 6.957 | 10.320 | 9.963 | 7.577 | 10.084 |
| Standard Deviation | 0.546 | 0.478 | 0.600 | 0.538 | 0.525 | 0.545 | 0.579 | 0.506 | 0.578 | 0.599 | 0.532 | 0.679 | 0.619 | 0.634 | 0.602 | 0.704 | 0.751 | 1.023 | 0.696 | 1.159 |
| Median | 6.6 | 6.2 | 5.9 | 6.8 | 6.1 | 5.7 | 4.4 | 5.45 | 7.7 | 7 | 5.4 | 6.45 | 8.45 | 7.8 | 4.55 | 7 | 10.35 | 10.1 | 7.6 | 10.3 |
| Minimum Value | 5.8 | 5.5 | 4.5 | 5.5 | 5.1 | 4.4 | 3.4 | 4.5 | 6.4 | 5.9 | 4.5 | 5.2 | 7.2 | 6.2 | 3.1 | 5 | 8.1 | 7.3 | 6.4 | 7.1 |
| Maximum Value | 8 | 7.5 | 7.7 | 8.6 | 7.4 | 7 | 6.4 | 6.9 | 8.9 | 8.6 | 6.6 | 8.2 | 9.8 | 8.7 | 5.8 | 8.3 | 11.8 | 11.9 | 9 | 12.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Teślak, M.; Ziemlewski, A.; Foltyn, I.; Ordyniec-Kwaśnica, I.; Drogoszewska, B. Development of Custom Anatomic Healing Abutment Based on Cone-Beam Computer Tomography Measurement on Human Teeth Cross-Section. Materials 2021, 14, 4570. https://doi.org/10.3390/ma14164570
Teślak M, Ziemlewski A, Foltyn I, Ordyniec-Kwaśnica I, Drogoszewska B. Development of Custom Anatomic Healing Abutment Based on Cone-Beam Computer Tomography Measurement on Human Teeth Cross-Section. Materials. 2021; 14(16):4570. https://doi.org/10.3390/ma14164570
Chicago/Turabian StyleTeślak, Monika, Adam Ziemlewski, Igor Foltyn, Iwona Ordyniec-Kwaśnica, and Barbara Drogoszewska. 2021. "Development of Custom Anatomic Healing Abutment Based on Cone-Beam Computer Tomography Measurement on Human Teeth Cross-Section" Materials 14, no. 16: 4570. https://doi.org/10.3390/ma14164570
APA StyleTeślak, M., Ziemlewski, A., Foltyn, I., Ordyniec-Kwaśnica, I., & Drogoszewska, B. (2021). Development of Custom Anatomic Healing Abutment Based on Cone-Beam Computer Tomography Measurement on Human Teeth Cross-Section. Materials, 14(16), 4570. https://doi.org/10.3390/ma14164570