
Preparation of Absorption-Resistant Hard Tissue Using Dental Pulp-Derived Cells and Honeycomb Tricalcium Phosphate

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Experimental Animals
2.2. Honeycomb TCP Scaffolds Preparation Method
2.3. Cell Isolation and Culture
2.4. Implantation Procedure and Histological Examination
2.5. Immunohistochemical Staining of RANKL, CD68 and DSP
2.6. Histological Evaluation of Hard Tissue Specimens
2.7. Statistics Analysis
3. Results
3.1. Histology of Formed Hard Tissue
3.2. Immunohistochemistry of Formed Hard Tissue
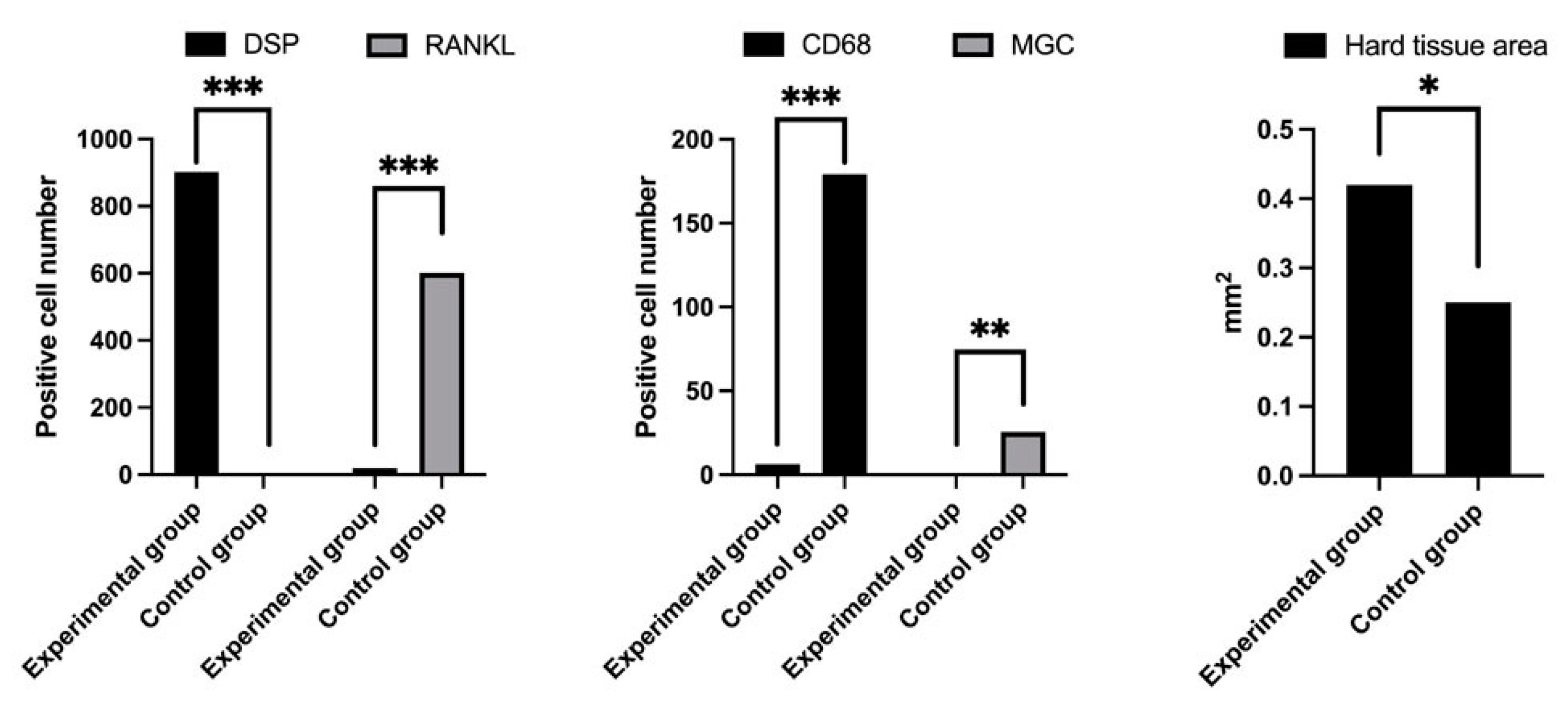
3.3. Measurement of IHC-Positive Cells, Multinucleated Giant Cells and Area of Formed Hard Tissue
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kuboki, Y.; Jin, Q.; Takita, H. Geometry of Carriers Controlling Phenotypic in BMP-Induced Osteogenesis and Chondrogenesis. J. Bone Joint Surg. 2001, 83, S105–S115. [Google Scholar] [CrossRef]
- Kiba, H.; Kuboyama, N.; Uchida, R.; Ishizaki, T.; Nishiyama, N. Bone Ingrowth into the Parallel Cylindrical Tubes with Different Sizes of Porous Hydroxyapatite Implanted into the Rabbits. J. Hard Tissue Biol. 2012, 21, 307–314. [Google Scholar] [CrossRef][Green Version]
- Baldino, L.; Cardea, S.; Maffulli, N.; Reverchon, E. Regeneration techniques for bone-to-tendon and muscle-to-tendon interfaces reconstruction. Br. Med. Bull. 2016, 117, 25–37. [Google Scholar] [CrossRef]
- Krause, D.S.; Theise, N.D.; Collector, M.I.; Henegariu, O.; Hwang, S.; Gardner, R.; Neutzel, S.; Sharkis, S.J. Multi-Organ, Multi-Lineage Engraftment by a Single Bone Marrow-Derived Stem Cell. Cell 2001, 105, 369–377. [Google Scholar] [CrossRef]
- Tsujigiwa, H.; Nishizaki, K.; Teshima, T.; Takeda, Y.; Yoshinobu, J.; Takeuchi, A.; Orita, Y.; Sugata, Y.; Nagatsuka, H.; Nagai, N. The Engraftment of Transplanted Bone Marrow-Derived Cells into the Olfactory Epithelium. Brain Res. 2005, 1052, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Friedenstein, A.J.; Gorskaja, J.F.; Kulagina, N.N. Fibroblast Precursors in Normal and Irradiated Mouse Hematopoietic Organs. Exp. Hematol. 1976, 4, 267–274. [Google Scholar]
- Jiang, Y.; Jahagirdar, B.N.; Reinhardt, R.L.; Schwartz, R.E.; Keene, C.D.; Ortiz-Gonzalez, X.R.; Reyes, M.; Lenvik, T.; Lund, T.; Blackstad, M.; et al. Pluripotency of Mesenchymal Stem Cells Derived from Adult Marrow. Nature 2002, 418, 41–49. [Google Scholar] [CrossRef]
- Ohgushi, H.; Caplan, A.I. Stem Cell Technology and Bioceramics: From Cell to Gene Engineering. J. Biomed. Mater. Res. 1999, 48, 913–927. [Google Scholar] [CrossRef]
- Pittenger, M.F.; Mackay, A.M.; Beck, S.C.; Jaiswal, R.K.; Douglas, R.; Mosca, J.D.; Moorman, M.A.; Simonetti, D.W.; Craig, S.; Marshak, D.R. Multilineage Potential of Adult Human Mesenchymal Stem Cells. Science 1999, 284, 143–147. [Google Scholar] [CrossRef] [PubMed]
- Caplan, A.I. Mesenchymal Stem Cells. J. Orthop. Res. 1991, 9, 641–650. [Google Scholar] [CrossRef] [PubMed]
- Ohgushi, H.; Dohi, Y.; Katuda, T.; Tamai, S.; Tabata, S.; Suwa, Y. In Vitro Bone Formation by Rat Marrow Cell Culture. J. Biomed. Mater. Res. 1996, 32, 333–340. [Google Scholar] [CrossRef]
- Kihara, T.; Oshima, A.; Hirose, M.; Ohgushi, H. Three-dimensional Visualization Analysis of In Vitro Cultured Bone Fabricated by Rat Marrow Mesenchymal Stem Cells. Biochem. Biophys. Res. Commun. 2004, 316, 943–948. [Google Scholar] [CrossRef] [PubMed]
- Tsujigiwa, H.; Katase, N.; Lefeuvre, M.; Yamachika, E.; Tamamura, R.; Ito, S.; Takebe, Y.; Matsuda, H.; Nagatsuka, H. Establishment of Odontoblastic Cells, Which Indicate Odontoblast Features Both In Vivo and In Vitro. J. Oral Pathol. Med. 2013, 42, 799–806. [Google Scholar] [CrossRef]
- Lee, K.S.; Park, J.W. Free Vascularized Osteocutaneous Fibular Graft to the Tibia. Microsurgery 1999, 19, 141–147. [Google Scholar] [CrossRef]
- Dimitriou, R.; Mataliotakis, G.I.; Angoules, A.G.; Kanakaris, N.K.; Giannoudis, P.V. Complications Following Autologous Bone Graft Harvesting from the Iliac Crest and Using the RIA: A Systematic Review. Injury 2011, 42 (Suppl. 2), S3–S15. [Google Scholar] [CrossRef]
- Klijn, R.J.; Meijer, G.J.; Bronkhorst, E.M.; Jansen, J.A. Sinus Floor Augmentation Surgery Using Autologous Bone Grafts from Various Donor Sites: A Meta-Analysis of the Total Bone Volume. Tissue Eng. Part B Rev. 2010, 16, 295–303. [Google Scholar] [CrossRef]
- Ducheyne, P.; Radin, S.; King, L. The Effect of Calcium Phosphate Ceramic Composition and Structure on In Vitro Behavior. I. Dissolution. J. Biomed. Mater. Res. 1993, 27, 25–34. [Google Scholar] [CrossRef]
- Yoshikawa, H.; Myoui, A. Bone Tissue Engineering with Porous Hydroxyapatite Ceramics. J. Artif. Organs 2005, 8, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Kaltreider, S.A.; Newman, S.A. Prevention and Management of Complications Associated with the Hydroxyapatite Implant. Ophthalmic Plast. Reconstr. Surg. 1996, 12, 18–31. [Google Scholar] [CrossRef] [PubMed]
- Mate-Sanchez de Val, J.E.; Mazon, P.; Guirado, J.L.; Ruiz, R.A.D.; Fernandez, M.P.R.; Negri, B.; Abboud, M.; Aza, P.N. Comparison of Three Hydroxyapatite/β-tricalcium Phosphate/Collagen Ceramic Scaffolds: An In Vivo Study. J. Biomed. Mater. Res. A 2013, 102, 1037–1046. [Google Scholar] [CrossRef] [PubMed]
- Takeshi, U.; Uryu, T.; Matsumoto, N.; Namaki, S.; Mashimo, T.; Tamagawa, T.; Yasumitsu, T.; Okudera, M.; Komiyama, K.; Chung, U.; et al. Histochemical and Radiological Study of Bone Regeneration by the Combinatorial Use of Tetrapod-Shaped Artificial Bone and Collagen. J. Hard Tissue Biol. 2015, 24, 199–210. [Google Scholar]
- Putri, T.S.; Hayashi, K.; Ishikawa, K. Bone Regeneration Using β-Tricalcium Phosphate (β-TCP) Block with Interconnected Pores Made by Setting Reaction of β-TCP Granules. J. Biomed. Mater. Res. A 2020, 108, 625–632. [Google Scholar] [CrossRef] [PubMed]
- Bohner, M.; Santoni, B.L.G.; Döbelin, N. β-Tricalcium Phosphate for Bone Substitution: Synthesis and Properties. Acta Biomater. 2020, 113, 23–41. [Google Scholar] [CrossRef] [PubMed]
- Takabatake, K.; Yamachika, E.; Tsujigiwa, H.; Takeda, Y.; Kimura, M.; Takagi, S.; Nagatsuka, H.; Iida, S. Effect of Geometry and Microstructure of Honeycomb TCP Scaffolds on Bone Regeneration. J. Biomed. Mater. Res. A 2014, 102, 2952–2960. [Google Scholar] [CrossRef]
- Nakagiri, R.; Watanabe, S.; Takabatake, K.; Tsujigiwa, H.; Watanabe, T.; Matsumoto, H.; Kimata, Y. Long-Term Effect of Honeycomb β-Tricalcium Phosphate on Zygomatic Bone Regeneration in Rats. Materials 2020, 13, 5155. [Google Scholar] [CrossRef]
- Siar, C.H.; Tsujigiwa, H.; Ishak, I.; Hussin, N.M.; Nagatsuka, H.; Ng, K.H. RANK, RANKL, and OPG in Recurrent Solid/Multicystic Ameloblastoma: Their Distribution Patterns and Biologic Significance. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2015, 119, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Song, M.; Kim, E.; Shon, W.; Chugal, N.; Bogen, G.; Lin, L.; Kim, R.H.; Park, N.H.; Kang, M.K. Pulp-dentin Regeneration: Current State and Future Prospects. J. Dent. Res. 2015, 94, 1544–1551. [Google Scholar] [CrossRef]
- Moussa, D.G.; Aparicio, C. Present and future of tissue engineering scaffolds for dentin-pulp complex regeneration. J. Tissue Eng. Regen. Med. 2019, 13, 58–75. [Google Scholar] [CrossRef]
- Tabatabaei, F.S.; Tatari, S.; Samadi, R.; Moharamzadeh, K. Different methods of dentin processing for application in bone tissue engineering: A systematic review. J. Biomed. Mater. Res. A 2016, 104, 2616–2627. [Google Scholar] [CrossRef] [PubMed]
- Ritchie, H. The Functional Significance of dentin sialoprotein-Phosphophoryn and Dentin Sialoprotein. Int. J. Oral Sci. 2018, 10, 31. [Google Scholar] [CrossRef]
- Chen, X.; Wang, Z.; Duan, N.; Zhu, G.; Schwarz, E.M.; Xie, C. Osteoblast-Osteoclast Interactions. Connect. Tissue Res. 2018, 59, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Udagawa, N.; Koide, M.; Nakamura, M.; Nakamichi, Y.; Yamashita, T.; Uehara, S.; Kobayashi, Y.; Furuya, Y.; Yasuda, H.; Fukuda, C.; et al. Osteoclast Differentiation by RANKL and OPG Signaling Pathways. J. Bone Miner. Metab. 2021, 39, 19–26. [Google Scholar] [CrossRef] [PubMed]
- El-Rashidy, A.A.; Roether, J.A.; Harhaus, L.; Kneser, U.; Boccaccini, A.R. Regenerating bone with bioactive glass scaffolds: A review of in vivo studies in bone defect models. Acta Biomater. 2017, 62, 1–28. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Number of Animals | Number of Implants |
|---|---|---|
| Experimental | 20 | 40 1 |
| Control | 20 | 40 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takabatake, K.; Nakano, K.; Kawai, H.; Inada, Y.; Sukegawa, S.; Qiusheng, S.; Fushimi, S.; Tsujigiwa, H.; Nagatsuka, H. Preparation of Absorption-Resistant Hard Tissue Using Dental Pulp-Derived Cells and Honeycomb Tricalcium Phosphate. Materials 2021, 14, 3409. https://doi.org/10.3390/ma14123409
Takabatake K, Nakano K, Kawai H, Inada Y, Sukegawa S, Qiusheng S, Fushimi S, Tsujigiwa H, Nagatsuka H. Preparation of Absorption-Resistant Hard Tissue Using Dental Pulp-Derived Cells and Honeycomb Tricalcium Phosphate. Materials. 2021; 14(12):3409. https://doi.org/10.3390/ma14123409
Chicago/Turabian StyleTakabatake, Kiyofumi, Keisuke Nakano, Hotaka Kawai, Yasunori Inada, Shintaro Sukegawa, Shan Qiusheng, Shigeko Fushimi, Hidetsugu Tsujigiwa, and Hitoshi Nagatsuka. 2021. "Preparation of Absorption-Resistant Hard Tissue Using Dental Pulp-Derived Cells and Honeycomb Tricalcium Phosphate" Materials 14, no. 12: 3409. https://doi.org/10.3390/ma14123409
APA StyleTakabatake, K., Nakano, K., Kawai, H., Inada, Y., Sukegawa, S., Qiusheng, S., Fushimi, S., Tsujigiwa, H., & Nagatsuka, H. (2021). Preparation of Absorption-Resistant Hard Tissue Using Dental Pulp-Derived Cells and Honeycomb Tricalcium Phosphate. Materials, 14(12), 3409. https://doi.org/10.3390/ma14123409