The Implantation of Bioactive Glass Granules Can Contribute the Load-Bearing Capacity of Bones Weakened by Large Cortical Defects

 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Materials and Methods
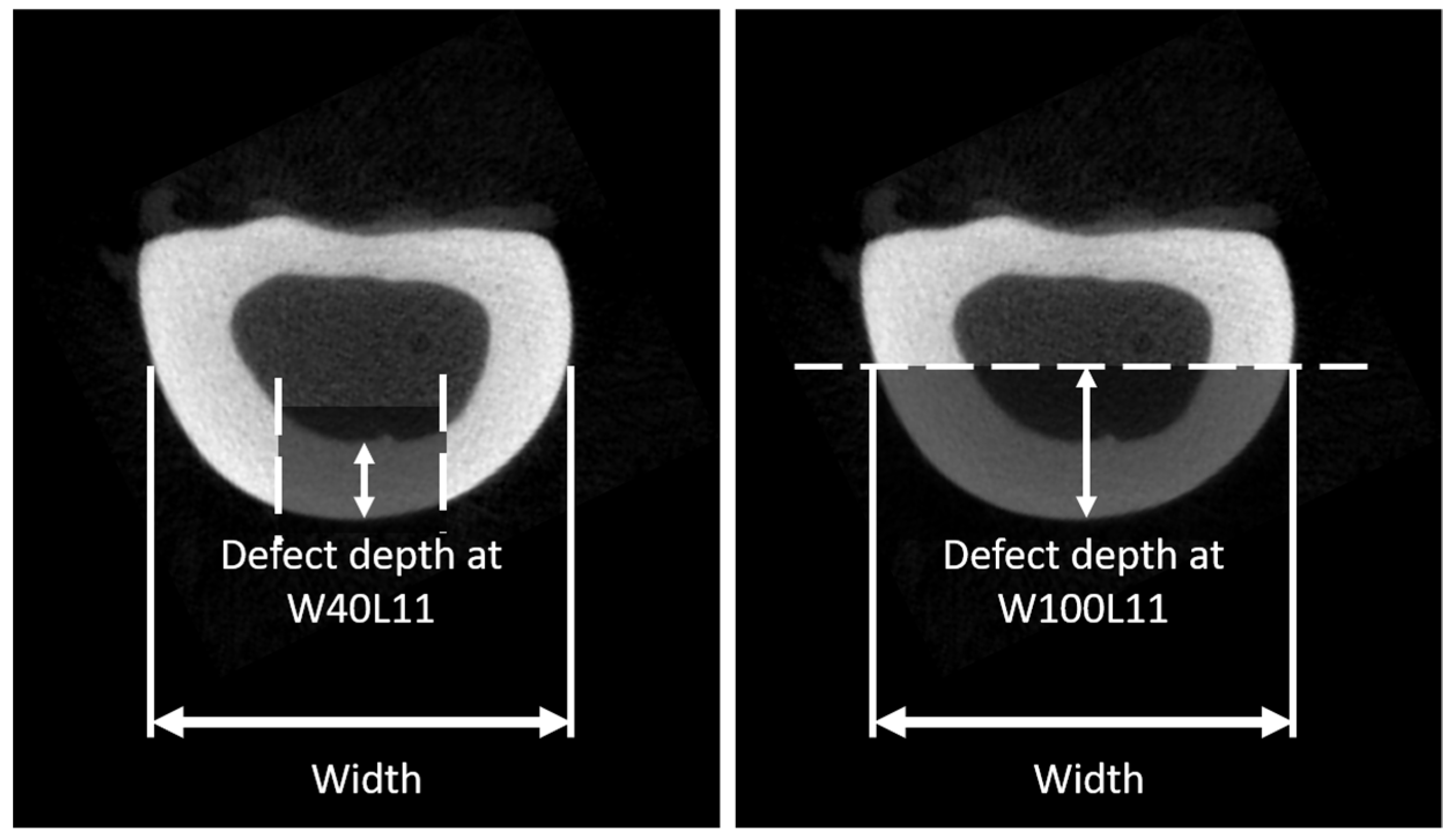
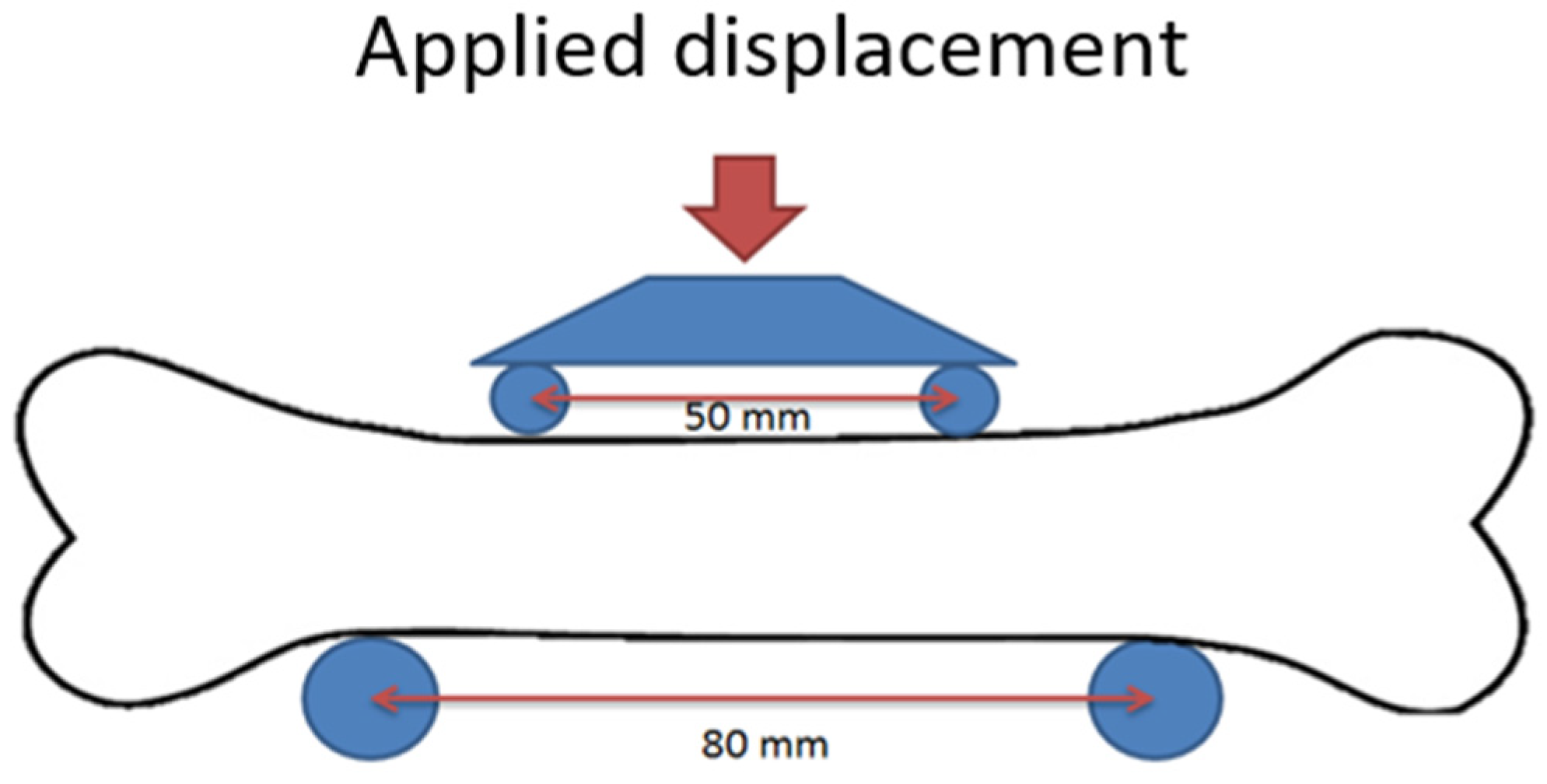
2.1. Effects of Cortical Defect Size and Geometry on Bone Stiffness and Moment of Failure
2.2. Determination of Material Properties of BAG/Bone Mixtures
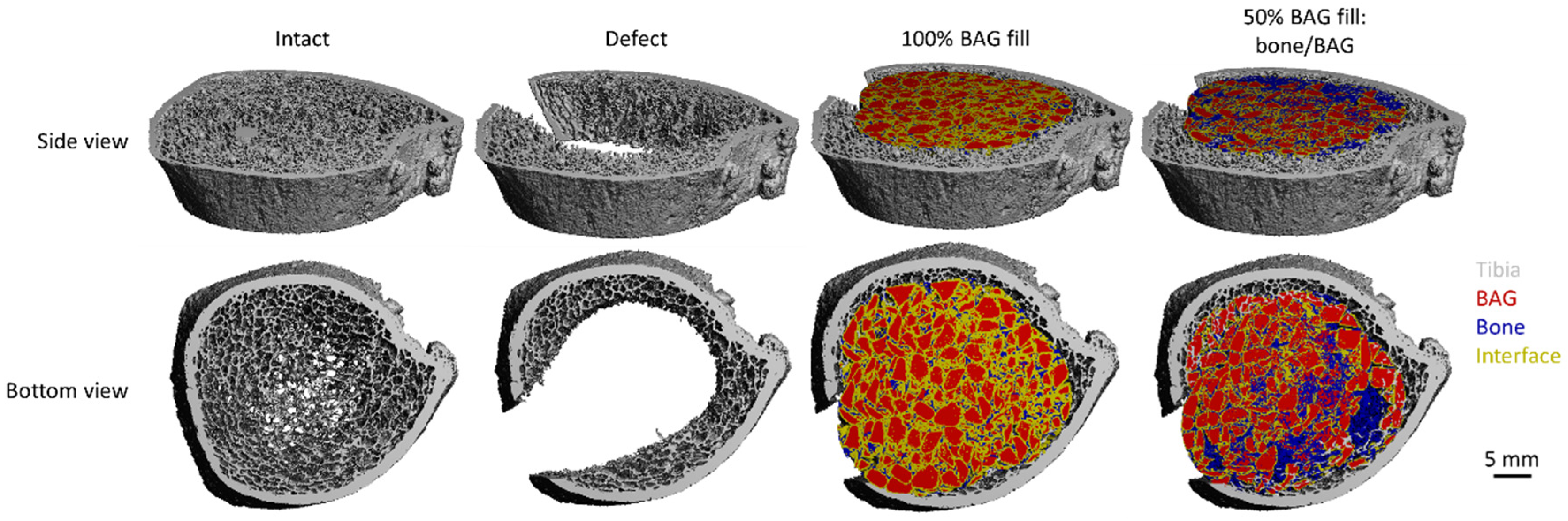
2.3. Investigation of BAG-mixture and Bone Load Sharing in the Distal Tibia
2.4. Statistical Analysis
3. Results
3.1. Effects of Cortical Defect Size and Geometry on Bone Stiffness, Stress Distribution, and Failure Moment
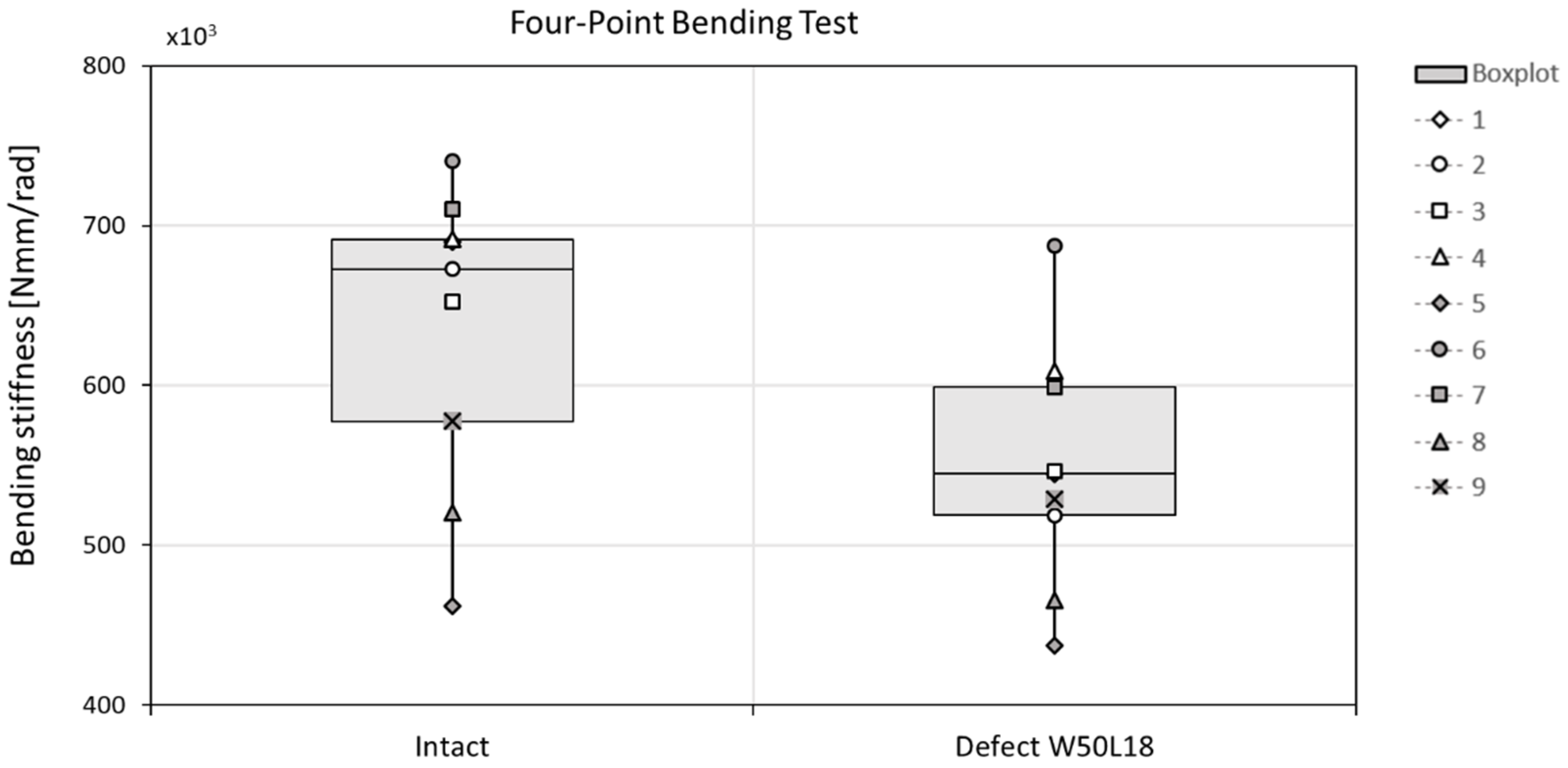
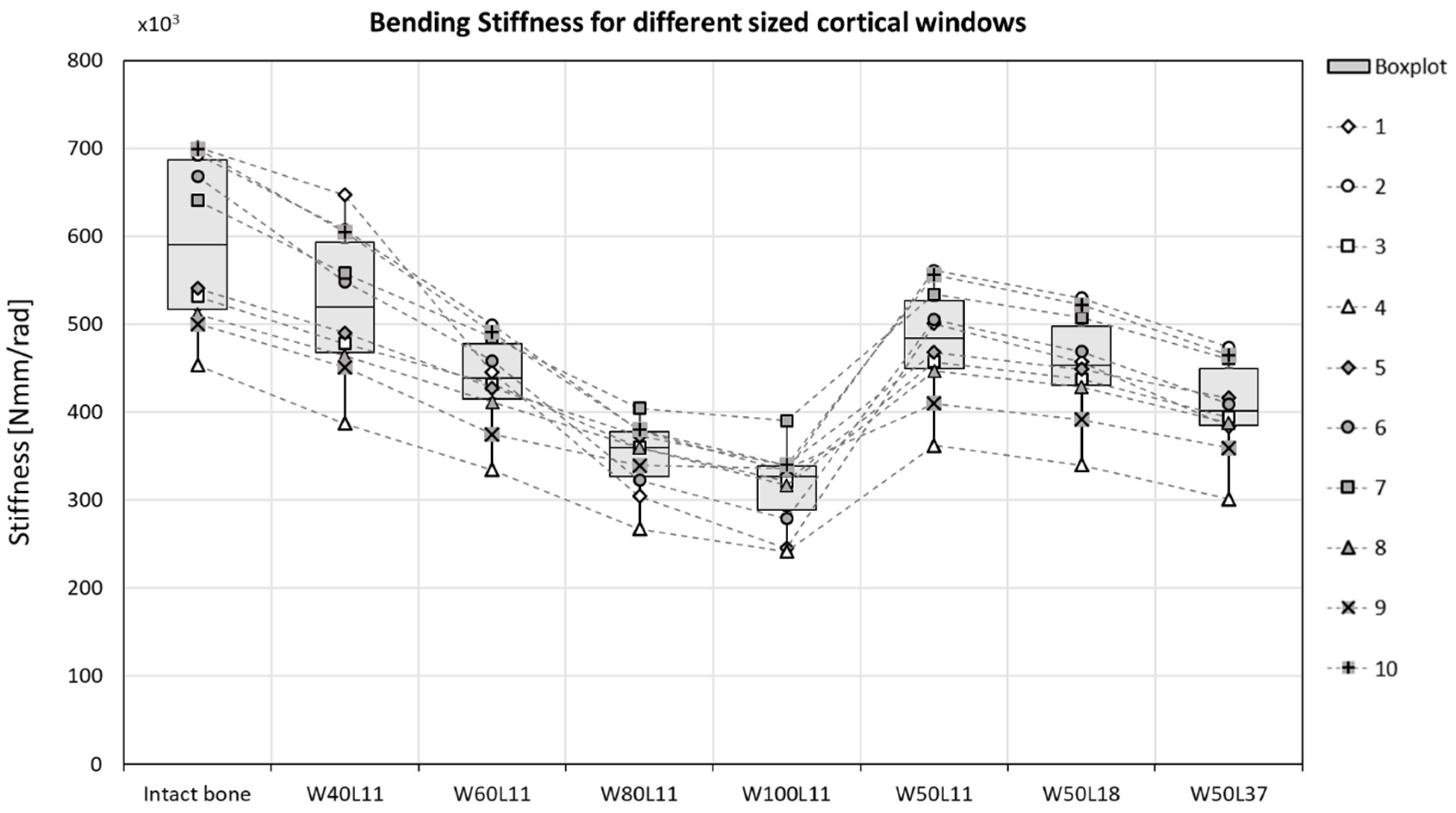
3.1.1. Bone stiffness
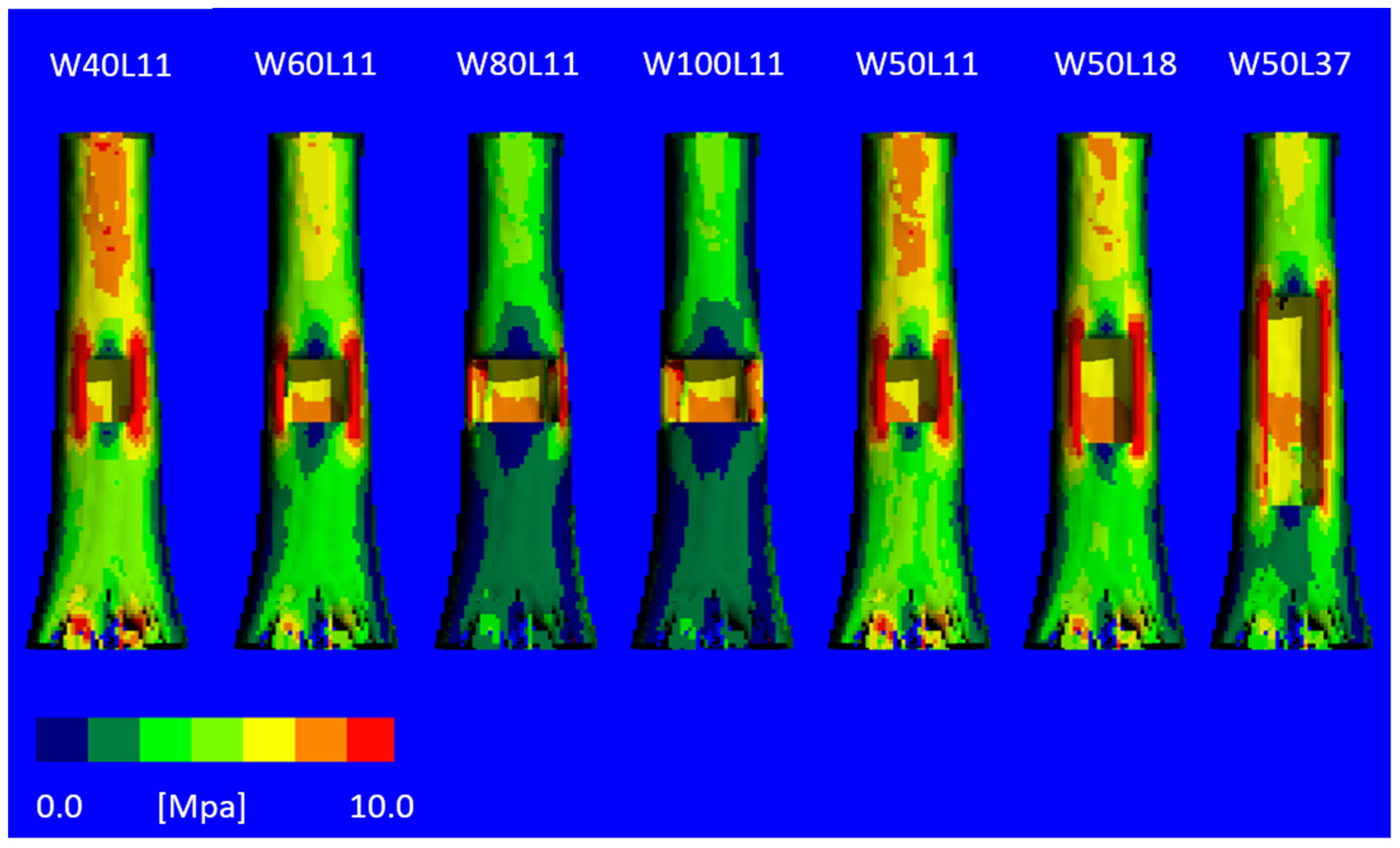
3.1.2. Stress Distribution
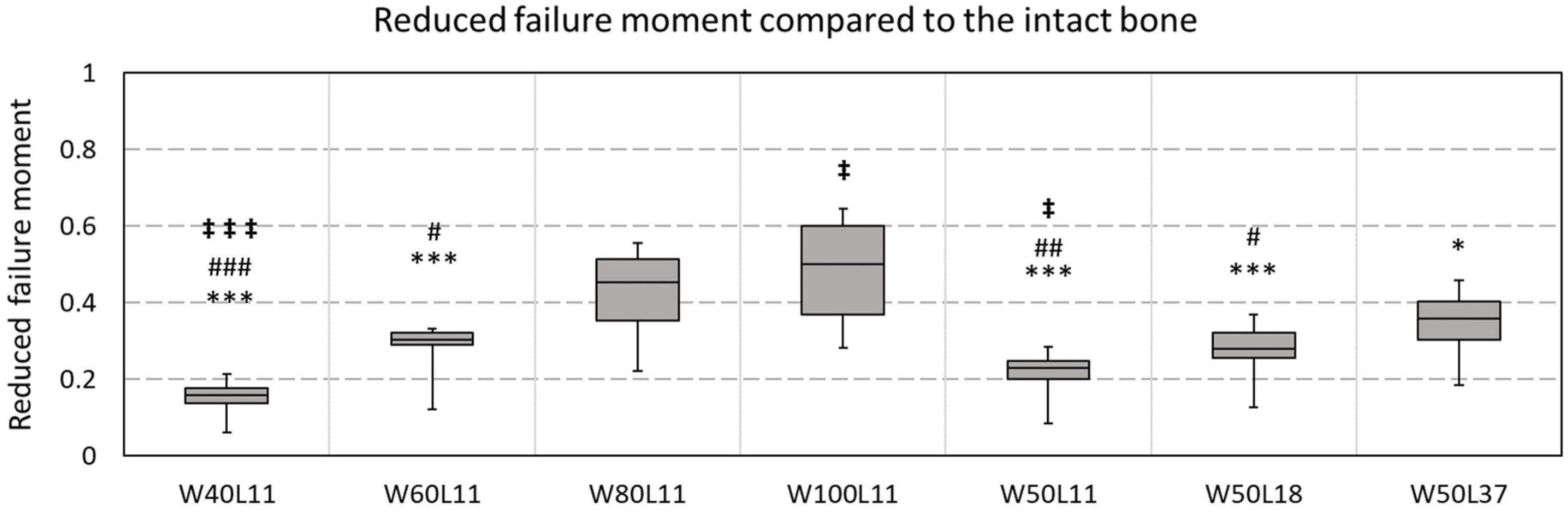
3.1.3. Failure Moment
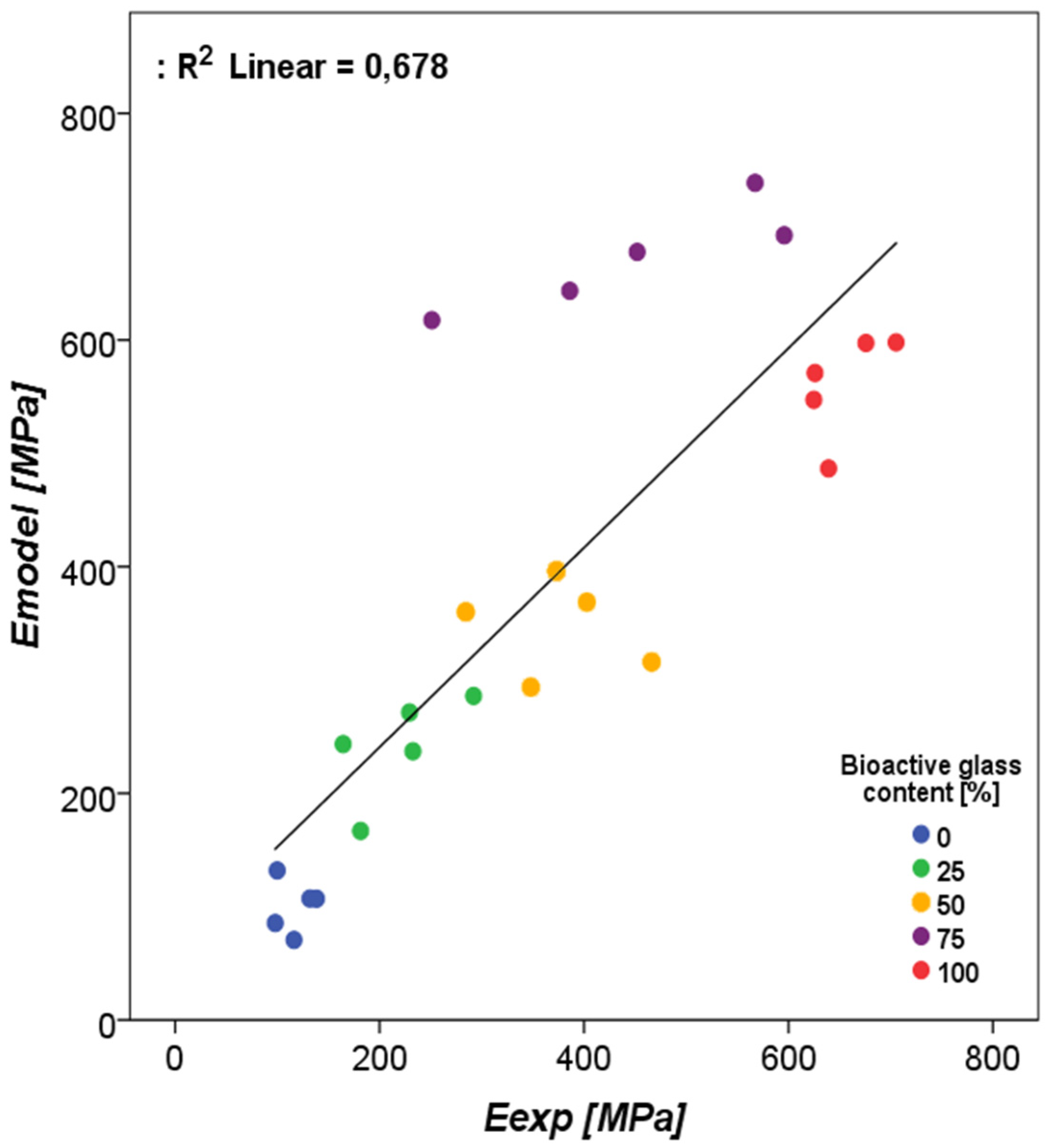
3.2. Determination of Material Properties of BAG/Bone Mixtures
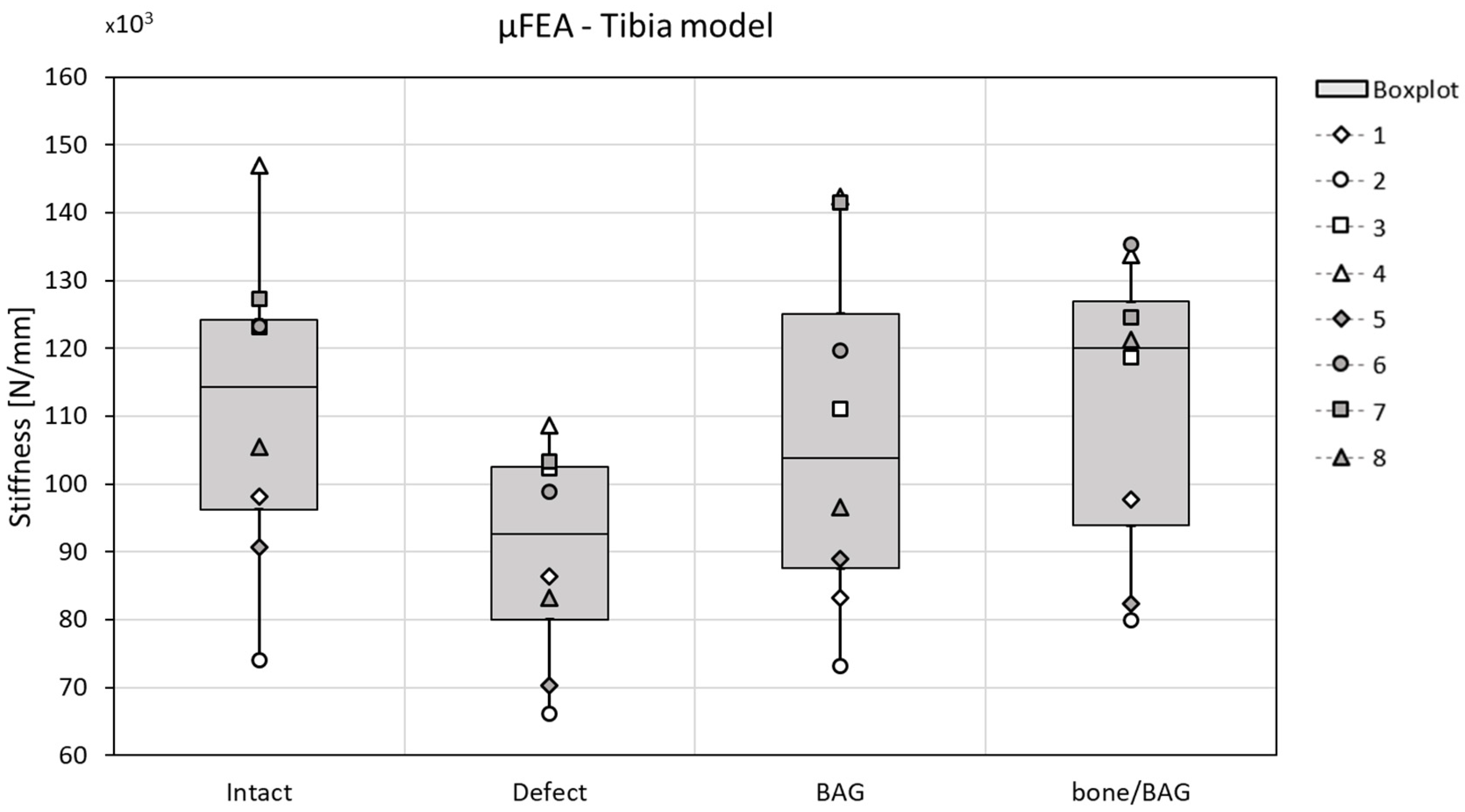
3.3. Investigation of BAG-Mixture and Bone Load Sharing in the Distal Tibia
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hench, L.L.; Splinter, R.J.; Allen, W.C.; Greenlee, T.K. Bonding mechanisms at the interface of ceramic prosthetic materials. J. Biomed. Mater. Res. 1971, 5, 117–141. [Google Scholar] [CrossRef]
- Hench, L.L. The story of Bioglass. J. Mater. Sci. Mater. Med. 2006, 17, 967–978. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.R. Reprint of: Review of bioactive glass: From Hench to hybrids. Acta Biomater. 2015, 23, S53–S82. [Google Scholar] [CrossRef]
- Van Gestel, N.A.P.; Geurts, J.; Hulsen, D.J.W.; Van Rietbergen, B.; Hofmann, S.; Arts, J.J. Clinical Applications of S53P4 Bioactive Glass in Bone Healing and Osteomyelitic Treatment: A Literature Review. Biomed Res. Int. 2015, 2015, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Munukka, E.; Leppäranta, O.; Korkeamäki, M.; Vaahtio, M.; Peltola, T.; Zhang, D.; Hupa, L.; Ylänen, H.; Salonen, J.I.; Viljanen, M.K.; et al. Bactericidal effects of bioactive glasses on clinically important aerobic bacteria. J. Mater. Sci. Mater. Med. 2008, 19, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Leppäranta, O.; Vaahtio, M.; Peltola, T.; Zhang, D.; Hupa, L.; Hupa, M.; Ylänen, H.; Salonen, J.I.; Viljanen, M.K.; Eerola, E. Antibacterial effect of bioactive glasses on clinically important anaerobic bacteria in vitro. J. Mater. Sci. Mater. Med. 2008, 19, 547–551. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Leppäranta, O.; Munukka, E.; Ylänen, H.; Viljanen, M.K.; Eerola, E.; Hupa, M.; Hupa, L. Antibacterial effects and dissolution behavior of six bioactive glasses. J. Biomed. Mater. Res.-Part A 2010, 93, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Lindfors, N.; Geurts, J.; Drago, L.; Arts, J.J.; Juutilainen, V.; Hyvonen, P.; Suda, A.J.; Domenico, A.; Artiaco, S.; Alizadeh, C.; et al. Antibacterial Bioactive Glass, S53P4, for Chronic Bone Infections—A Multinational Study. Adv. Exp. Med. Biol. 2017, 971, 81–92. [Google Scholar]
- Walenkamp, G.H.I.M.; Kleijn, L.L.A.; de Leeuw, M. Osteomyelitis treated with gentamicin-PMMA beads. Acta Orthop. Scand. 1998, 69, 518–522. [Google Scholar] [CrossRef]
- Geurts, J.; Chris Arts, J.J.; Walenkamp, G.H.I.M. Bone graft substitutes in active or suspected infection. Contra-indicated or not? Injury 2011, 42, S82–S86. [Google Scholar] [CrossRef]
- Hulsen, D.J.W.; Geurts, J.; van Gestel, N.A.P.; van Rietbergen, B.; Arts, J.J. Mechanical behaviour of Bioactive Glass granules and morselized cancellous bone allograft in load bearing defects. J. Biomech. 2016, 49, 1121–1127. [Google Scholar] [CrossRef] [PubMed]
- van Rietbergen, B.; Ito, K. A survey of micro-finite element analysis for clinical assessment of bone strength: The first decade. J. Biomech. 2014, 48, 832–841. [Google Scholar] [CrossRef] [PubMed]
- Bayraktar, H.H.; Morgan, E.F.; Niebur, G.L.; Morris, G.E.; Wong, E.K.; Keaveny, T.M. Comparison of the elastic and yield properties of human femoral trabecular and cortical bone tissue. J. Biomech. 2004, 37, 27–35. [Google Scholar] [CrossRef]
- Bevill, G.; Eswaran, S.K.; Farahmand, F.; Keaveny, T.M. The influence of boundary conditions and loading mode on high-resolution finite element-computed trabecular tissue properties. Bone 2009, 44, 573–578. [Google Scholar] [CrossRef]
- Pistoia, W.; van Rietbergen, B.; Lochmüller, E.-M.; Lill, C.; Eckstein, F.; Rüegsegger, P. Estimation of distal radius failure load with micro-finite element analysis models based on three-dimensional peripheral quantitative computed tomography images. Bone 2002, 30, 842–848. [Google Scholar] [CrossRef]
- MacNeil, J.A.; Boyd, S.K. Bone strength at the distal radius can be estimated from high-resolution peripheral quantitative computed tomography and the finite element method. Bone 2008, 42, 1203–1213. [Google Scholar] [CrossRef]
- Thompson, I.D.; Hench, L.L. Mechanical properties of bioactive glasses, glass-ceramics and composites. Proc. Inst. Mech. Eng. Part H 1998, 212, 127–136. [Google Scholar] [CrossRef]
- Burt, L.A.; Macdonald, H.M.; Hanley, D.A.; Boyd, S.K. Bone microarchitecture and strength of the radius and tibia in a reference population of young adults: an HR-pQCT study. Arch. Osteoporos. 2014, 9, 183. [Google Scholar] [CrossRef]
- Fox, J. Using the R Commander: A Point-and-Click Interface for R; Chapman and Hall/CRC Press: Boca Raton, FL, USA, 2017. [Google Scholar]
- Fox, J. The R Commander: A Basic Statistics Graphical User Interface to R. J. Stat. Softw. 2005, 14, 1–42. [Google Scholar] [CrossRef]
- Fox, J.; Bouchet-Valat, M. Rcmdr: R Commander 2019. Available online: https://cran.r-project.org/web/packages/Rcmdr/index.html (accessed on 8 May 2019).
- Calhoun, J.H.; Manring, M.M.; Shirtliff, M. Osteomyelitis of the long bones. Semin. Plast. Surg. 2009, 23, 59–72. [Google Scholar] [CrossRef]
- Dym, C.L.; Shames, I.H. Solid Mechanics; Augmented.; Springer New York: New York, NY, USA, 2013; ISBN 978-1-4614-6033-6. [Google Scholar]
- Steiner, J.A.; Hofmann, U.A.T.; Christen, P.; Favre, J.M.; Ferguson, S.J.; van Lenthe, G.H. Patient-specific in silico models can quantify primary implant stability in elderly human bone. J. Orthop. Res. 2017, 36, 954–962. [Google Scholar] [CrossRef] [PubMed]
- Marcián, P.; Wolff, J.; Horáčková, L.; Kaiser, J.; Zikmund, T.; Borák, L. Micro finite element analysis of dental implants under different loading conditions. Comput. Biol. Med. 2018, 96, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Paggiosi, M.A.; Eastell, R.; Walsh, J.S. Precision of High-Resolution Peripheral Quantitative Computed Tomography Measurement Variables: Influence of Gender, Examination Site, and Age. Calcif. Tissue Int. 2014, 94, 191–201. [Google Scholar] [CrossRef] [PubMed]
- van Gestel, N.A.P.; Schuiringa, G.H.; Hennissen, J.H.P.H.; Delsing, A.C.A.; Ito, K.; van Rietbergen, B.; Arts, J.J.; Hofmann, S. Resorption of the calcium phosphate layer on S53P4 bioactive glass by osteoclasts. J. Mater. Sci. Mater. Med. 2019, 30, 94. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Defect | Defect Width (Circumferential Direction) | Defect Length (Longitudinal Direction) |
|---|---|---|
| W40L11 | 40% of width | 11.1 mm |
| W60L11 | 60% of width | 11.1 mm |
| W80L11 | 80% of width | 11.1 mm |
| W100L11 | 100% of width | 11.1 mm |
| W50L11 | 50% of width | 11.1 mm |
| W50L18 | 50% of width | 18.5 mm |
| W50L37 | 50% of width | 37.0 mm |
| Measure | W40L11 | W60L11 | W80L11 | W100L11 | W50L11 | W50L18 | W50L37 |
|---|---|---|---|---|---|---|---|
| Width (SD) (mm) | 0.72 (0.042) | 0.90 (0.053) | 1.08 (0.063) | 1.44 (0.085) | 1.81 (0.106) | 0.90 (0.053) | 0.90 (0.053) |
| Defect area (SD) (mm2) | 8.01 (0.469) | 10.02 (0.587) | 12.02 (0.704) | 16.03 (0.939) | 20.04 (1.174) | 16.70 (0.978) | 33.40 (1.957) |
| Defect depth (mm) | 3.3 (0.27) | 3.3(0.27) | 3.4 (0.43) | 4.1 (1.35) | 6.0 (0.99) | 3.3 (0.27) | 3.3 (0.27) |
| Defect Size | Intact | W40L11 | W60L11 | W80L11 | W100L11 | W50L11 | W50L18 | W50L37 |
|---|---|---|---|---|---|---|---|---|
| Intact | x | |||||||
| W40L11 | 0.23368 | x | ||||||
| W60L11 | <0.001 a | 0.05865 | x | |||||
| W80L11 | <0.001 a | <0.001 a | 0.06319 | x | ||||
| W100L11 | <0.001 a | <0.001 a | 0.00160 b | 0.92728 | x | |||
| W50L11 | 0.00395 b | 0.79351 | 0.78240 | <0.001 a | <0.001 a | x | ||
| W50L18 | <0.001 a | 0.22967 | 0.99873 | 0.01159 b | <0.001 a | 0.98115 | x | |
| W50L37 | <0.001 a | 0.00232 b | 0.96104 | 0.51423 | 0.04416 b | 0.16915 | 0.70436 | x |
| Defect | Maintained Part of Initial Bending Stiffness (%) |
|---|---|
| W40L11 | 88.3 ± 3.1 |
| W60L11 | 74.0 ± 5.6 |
| W80L11 | 59.8 ± 9.4 |
| W100L11 | 54.0 ± 10.4 |
| W50L11 | 81.3 ± 5 |
| W50L18 | 76.8 ± 5.9 |
| W50L37 | 68.8 ± 6.9 |
| Phase | Young’s Modulus (MPa) | Poisson Ratio (-) |
|---|---|---|
| Bone morsels | 2.5 × 103 | 0.3 |
| BAG | 35 × 103 | 0.3 |
| Interface | 25 | 0.3 |
| Tibia bone | 6826 | 0.3 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Gestel, N.A.P.; Gabriels, F.; Geurts, J.A.P.; Hulsen, D.J.W.; Wyers, C.E.; van de Bergh, J.P.; Ito, K.; Hofmann, S.; Arts, J.J.; van Rietbergen, B. The Implantation of Bioactive Glass Granules Can Contribute the Load-Bearing Capacity of Bones Weakened by Large Cortical Defects. Materials 2019, 12, 3481. https://doi.org/10.3390/ma12213481
van Gestel NAP, Gabriels F, Geurts JAP, Hulsen DJW, Wyers CE, van de Bergh JP, Ito K, Hofmann S, Arts JJ, van Rietbergen B. The Implantation of Bioactive Glass Granules Can Contribute the Load-Bearing Capacity of Bones Weakened by Large Cortical Defects. Materials. 2019; 12(21):3481. https://doi.org/10.3390/ma12213481
Chicago/Turabian Stylevan Gestel, Nicole A. P., Floor Gabriels, Jan A. P. Geurts, Dennis J. W. Hulsen, Caroline E. Wyers, Joop P. van de Bergh, Keita Ito, Sandra Hofmann, Jacobus J. Arts, and Bert van Rietbergen. 2019. "The Implantation of Bioactive Glass Granules Can Contribute the Load-Bearing Capacity of Bones Weakened by Large Cortical Defects" Materials 12, no. 21: 3481. https://doi.org/10.3390/ma12213481
APA Stylevan Gestel, N. A. P., Gabriels, F., Geurts, J. A. P., Hulsen, D. J. W., Wyers, C. E., van de Bergh, J. P., Ito, K., Hofmann, S., Arts, J. J., & van Rietbergen, B. (2019). The Implantation of Bioactive Glass Granules Can Contribute the Load-Bearing Capacity of Bones Weakened by Large Cortical Defects. Materials, 12(21), 3481. https://doi.org/10.3390/ma12213481