Abstract
Trend and characteristics of maxillofacial fractures in 2,636 patients over 32 years were analyzed retrospectively. Patients comprised 1,764 males and 872 females with ages ranging from 0 to 99 years. Patients younger than 30 years consisted of 60% maxillofacial fractures in the early period but decreased to 40% in the late period. In contrast, patients older than 60 years gradually increased to 30%. In terms of cause, traffic accidents consisted of more than 50%, predominantly motorcycle accidents, but gradually decreased to 40%. In contrast, falls markedly increased from less than 10 to 30%. Fractures occurred in the midface in 938 patients, in the mandible in 1,490, and in both in 208. In the midface, zygoma fractures consisted of 50% throughout the period. In the mandible, condyle fractures were observed in 40%, followed by fractures of the symphysis and angle. The ratio of condylar fractures slightly increased. Open reduction and internal fixation (ORIF) were performed in 782 patients, followed by observation in 716, maxillomandibular fixation (MMF) in 605, intramaxillary splinting (IMS) in 294, transcutaneous reduction (TCR) in 126, and others in 113. MMF markedly decreased from more than 30 to less than 5% and observation increased from 20 to 40%.
Maxillofacial fractures can result from various causes, such as traffic accidents, falls, assaults, sports, and others, in isolation or in combination with other injuries [,,,,,,,,,,,]. Epidemiology of these fractures varies depending on the geographic area, socioeconomic status, and period of investigation. Most studies have shown that traffic accidents are the most common cause of maxillofacial fractures in many countries [,,,,,,,], whereas interpersonal violence is most common in others [,,,]. However, there have been no studies in which the trend of maxillofacial fractures was analyzed in terms of demographics, cause and site of fractures, and treatment modalities during a long period.
In the present study, we retrospectively analyzed the trend and characteristics of maxillofacial fractures in our department over 32 years.
Subjects and Methods
The subjects of the present study were 2,636 patients with maxillofacial fractures treated at the Department of Oral and Maxillofacial Surgery, Nara Medical University over 32 years, between 1982 and 2013. Data on these patients were obtained from their clinical records and radiographs, and were analyzed retrospectively for age and gender distribution, cause and site of fractures, and treatment modalities. Cause of fractures was classified into sports, assault, traffic accident, fall, work-related accident, and striking an object or unidentified. Traffic accident was further divided into automobile, motorcycle, bicycle, pedestrian, and others. Fall was also divided into simple fall (fall on a level surface) and fall from a height. Sites of fractures were basically determined by radiographs. Panoramic, posteroanterior, and Waters views were generally used. Computed tomography (CT) was also available in selected cases in the early period and was routinely used in the late period. Midfacial fractures were classified into five patterns according to the involved structures as follows: (1) nasal: nasal bone fracture only; (2) alveolus: alveolar bone fracture only or with nasal bone fracture; (3) zygoma: unilateral fracture of the zygoma (zygomaticomaxillary complex) only or with nasal bone fracture and/or alveolar bone fracture; (4) maxilla: maxillary wall fracture and/or Le Fort type I fracture and/or sagittal fracture of the maxilla, or with nasal bone fracture and/or alveolar bone fracture; (5) multiple: bilateral fractures of the zygoma, Le Fort type II or III fracture, naso-orbital ethmoid fractures, or other multiple or comminuted fractures of the midface. Sites of the mandibular fractures were classified into symphysis, body, angle, ramus, coronoid process, condyle, and alveolus. Bilateral fractures were counted separately, except for symphyseal fractures. Alveolar fractures at the site of symphyseal and body fractures were included in the fractures of these sites. Treatment modalities were classified into open reduction and internal fixation (ORIF), maxillomandibular fixation (MMF), intramaxillary splinting (IMS) using arch bar or acrylic cap, transcutaneous reduction (TCR), others, and observation. The study protocol was approved by the institutional review board and in accordance with the principles of the Declaration of Helsinki.
Results
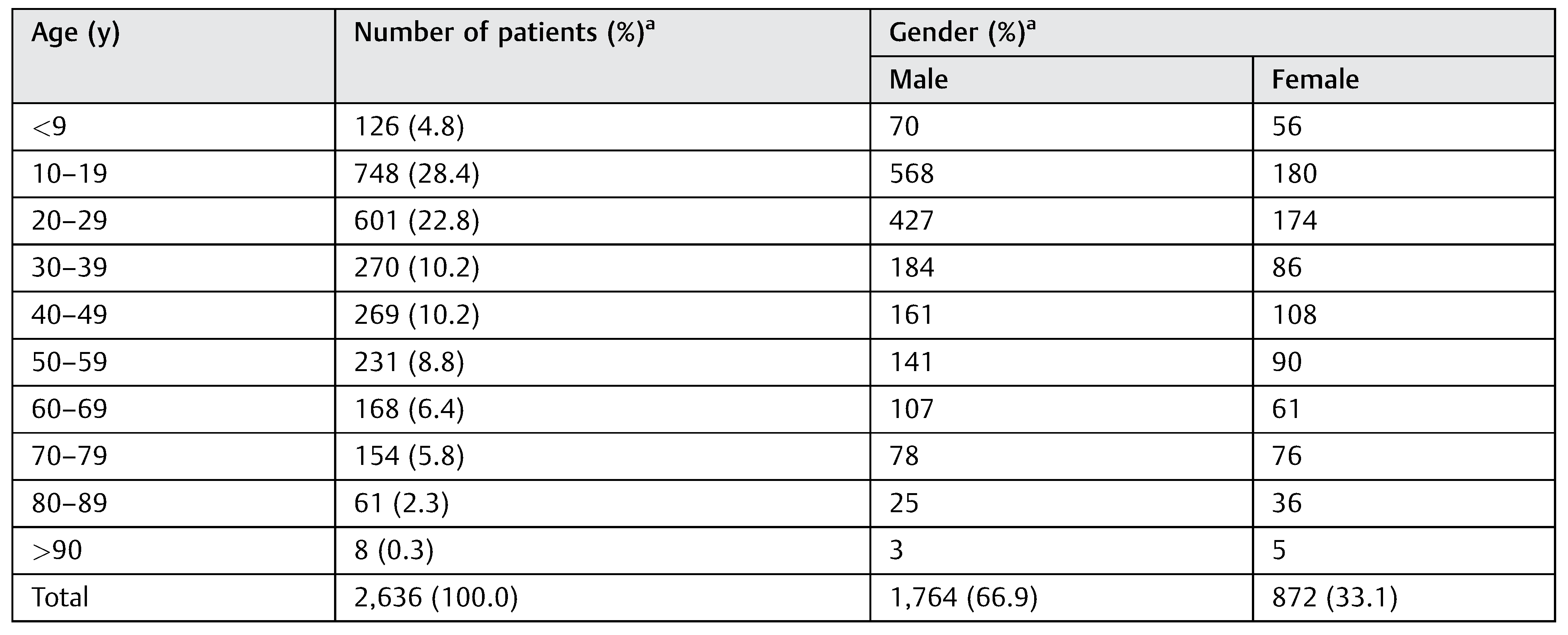
Of the 2,636 patients, 1,764 were males (66.9%) and 872 females (33.1%) (Table 1). The age of the patients ranged from 9 months to 99 years with an average of 33.6 years. The age distribution showed 748 patients (28.4%) in the second decade of life and 601 (22.8%) in the third. The average number of patients per year was 82.4 years, but the annual number of patients changed during the period. In the late 80s and the mid-90s, more than 100 patients were observed each year (Figure 1). However, the number has decreased to approximately 60 in the past 15 years. The male to female ratio has slightly changed from 7:3 in the early period to 6:4 in the late period. The age of the patients has shifted to older age during the 32 years (Figure 2). Patients younger than 30 years consisted of approximately 60% in the early period but have decreased to around 40% in recent years. In reverse, patients aged 60 years or older were fewer than 10% in the 80s but have reached around 30% in recent years.

Table 1.
Age and gender of the patients.
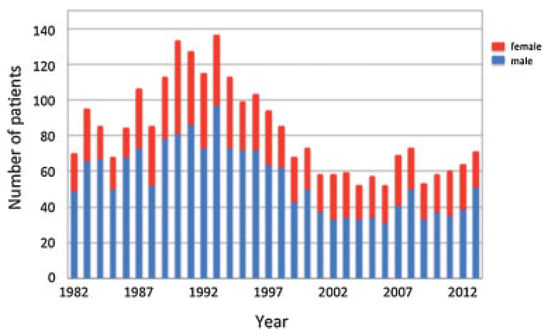
Figure 1.
Yearly distribution of the patients.
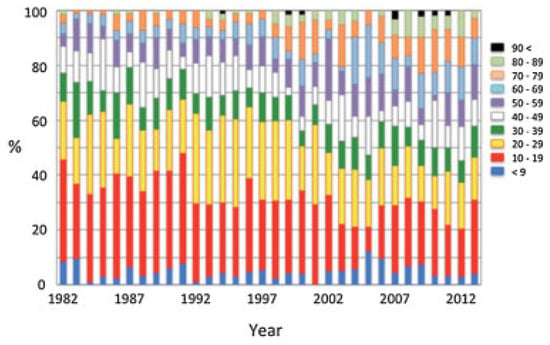
Figure 2.
Yearly ratio of the age.
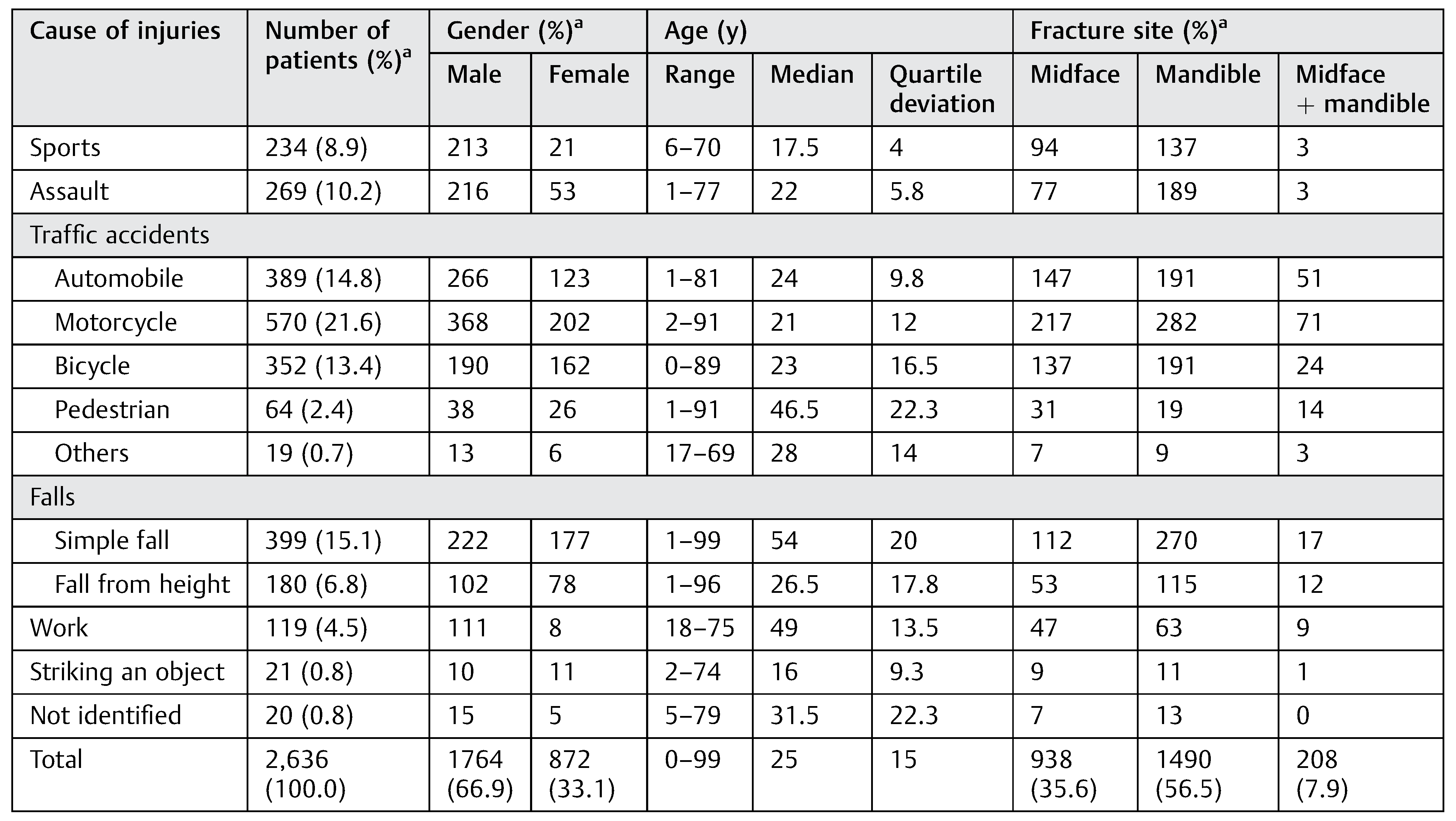
Cause of the fractures is shown according to gender and age of patients (Table 2). Overall, 1,394 patients (52.9%) were injured in traffic accidents. Among these, 389 patients (14.8%) were in an automobile, 570 (21.6%) were on a motorcycle, 352 (13.4%) were on a bicycle, 64 (2.4%) were pedestrians, and 19 (0.7%) were in other vehicles or unidentified. In total, 579 patients (22.0%) were injured in falls. Falls occurred on a level surface in 399 patients (15.1%) (simple fall) and from a height in 180 (6.8%) (fall from height). Other fractures occurred by assaults in 269 patients (10.2%), in sports activity in 234 (8.9%), in work-related accidents in 119 (4.5%), and in striking an object in 21 (0.8%). In 20 patients (0.8%), the cause was not identified. Fractures sustained in sports activity, in assaults, and in work-related accidents were dominantly observed in male patients. Age of the patients was distributed widely but was somewhat different in each cause. The median ages of patients injured by most of the causes were in their 20s or less, but those injured in pedestrian accidents, simple falls, and work-related accidents were in their late 40s or more. Cause of fractures has changed during the period (Figure 3). Fractures in automobile and motorcycle accidents decreased from 40 to 20%. In reverse, fractures by simple falls gradually increased from 10 to 30%.
Table 2.
Cause of injuries according to gender and age of patients and fracture site.
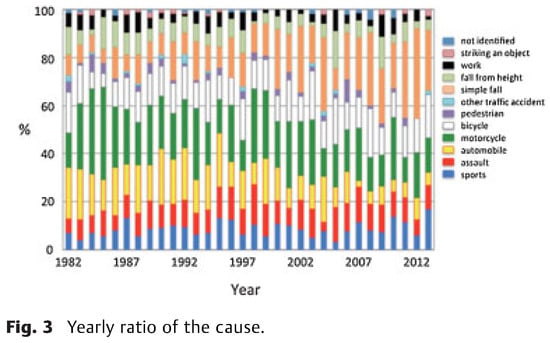
Figure 3.
Yearly ratio of the cause.
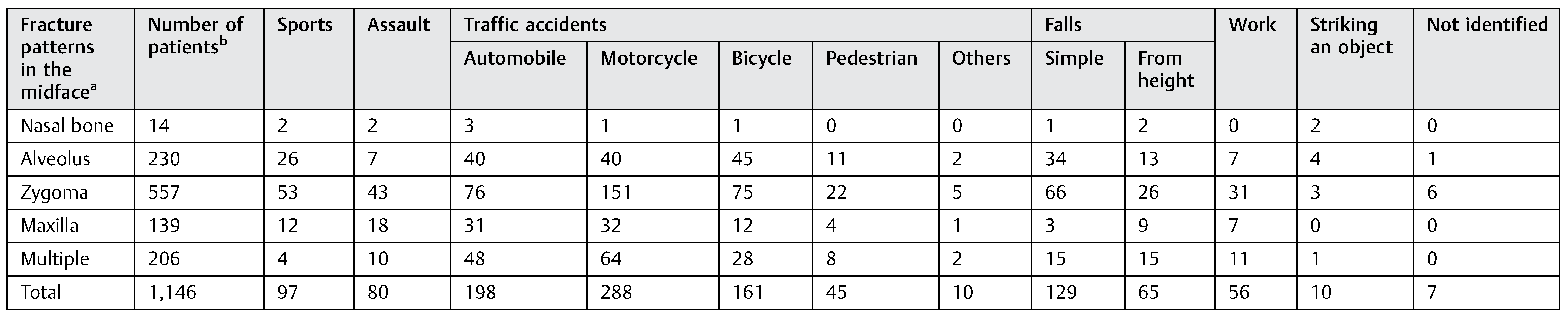
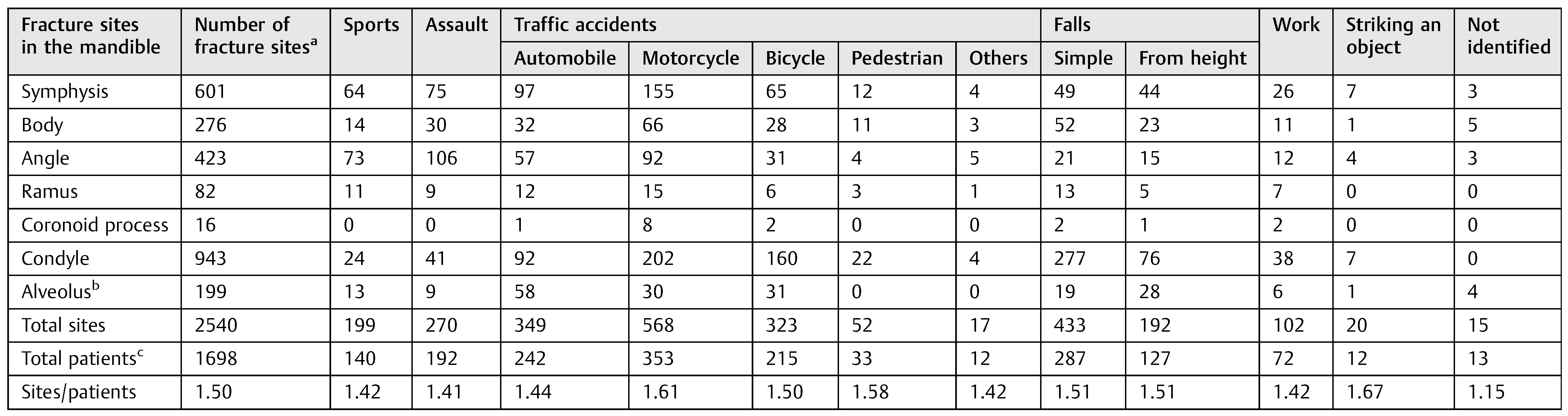
Fractures occurred in the midface in 938 patients (35.6%), in the mandible in 1,490 patients (56.5%), and in both in 208 patients (7.9%) (Table 2). Number of mandibular fractures decreased after the late 90s. The ratio of midfacial and mandibular fractures was 0.63 (938/1490) in the entire period but has increased to 0.88 (256/291) in the past 10 years (Figure 4). Fractures in both the midface and mandible were observed in patients injured in traffic accidents involving automobiles (13.1%, 51/389) and motorcycles (12.5%, 71/570). In 1,146 patients (938 + 208) with midfacial fractures, unilateral fractures of the zygoma were most commonly observed in 557 patients (48.6%), followed by alveolar fractures in 230 (20.1%), multiple fractures in 206 (18.0%), and maxillary fractures in 139 (12.1%) (Table 3). Isolated nasal bone fractures were observed in 14 patients (1.2%) only. Unilateral fracture of the zygoma was most frequently observed in any causes. Multiple fractures were observed at a higher rate in automobile and motorcycle accidents, falls from a height, and work-related accidents. Fracture patterns did not show a marked change during the period (Figure 5). In 1,698 patients (1,490 + 208) with mandibular fractures, the fracture site was single in 812 patients (47.8%), double in 561 (33.0%), triple in 125 (7.4%), and quadruple or more in 10 (0.6%). Isolated alveolar bone fractures were observed in 190 patients (11.2%). Among 2,540 fractures sites, the condyle was most frequently involved in 943 sites (37.1%), followed by the symphysis in 601 (23.7%), the angle in 423 (16.7%), the body in 276 (10.9%), the alveolus in 199 (7.8%), the ramus in 82 (3.2%), and the coronoid process in 16 (0.6%) (Table 4). Condylar fractures were observed in about two-thirds of the injuries by a simple fall and in about half of those injured in bicycle accidents. Mandibular angle fractures were common in injuries from assaults and in sports activity. Fractures of the symphysis have gradually decreased and those of the condyle gradually increased during the period (Figure 6).
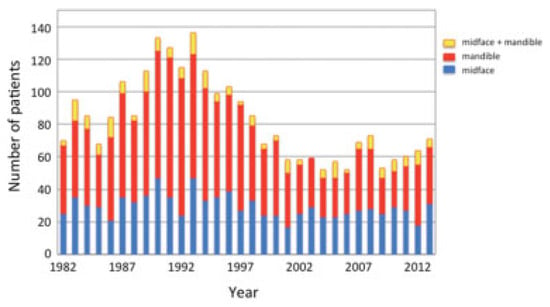
Figure 4.
Yearly distribution of midfacial and mandibular fractures.
Table 3.
Fracture patterns in the midface according to the cause.
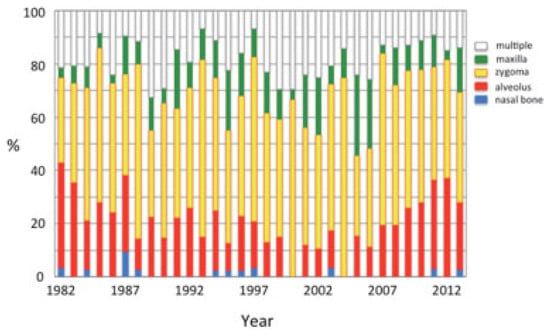
Figure 5.
Yearly ratio of fracture patterns of the midface.
Table 4.
Fracture sites in the mandible according to the cause.
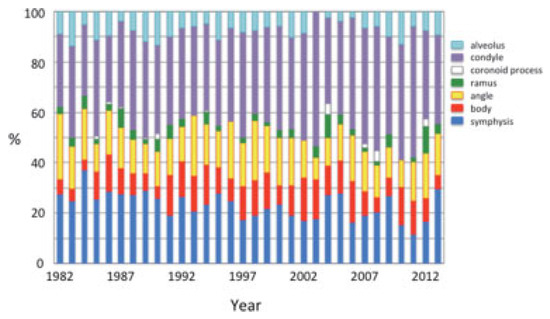
Figure 6.
Yearly ratio of fracture sites of the mandible.
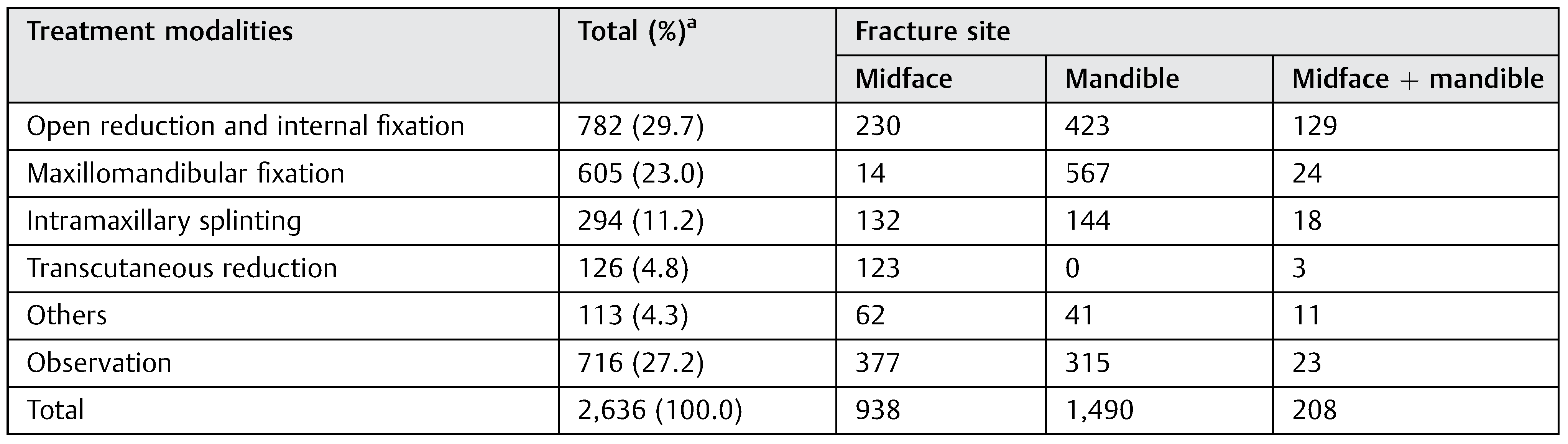
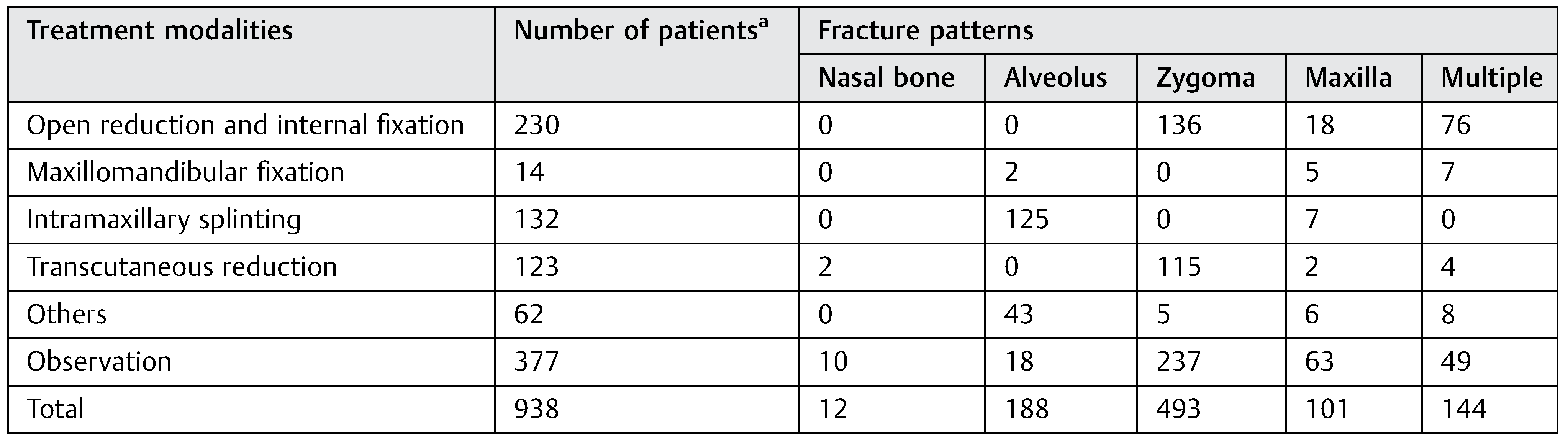
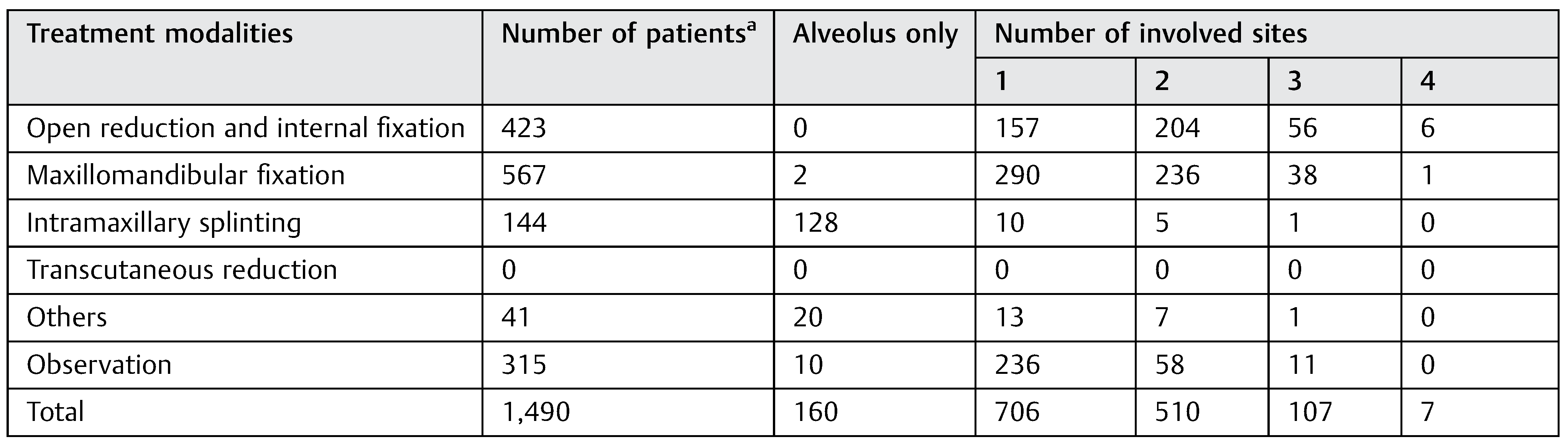
Treatment for the fractures is shown according to fracture site (Table 5). Treatment of each patient was defined as the most aggressive treatment chosen for fractures if they were observed at multiple sites. ORIF was performed in 782 patients (29.7%), followed by observation in 716 (27.2%), MMF in 605 (23.0%), IMS in 294 (11.2%), TCR in 126 (4.8%), and others in 113 (4.3%). More than 60% of the patients with fractures in both the midface and mandible were treated by ORIF, although about one-fourth of the patients with fractures in either the midface or mandible were treated by ORIF. More than 90% of MMF was performed for mandibular fractures. All TCR were performed for midfacial fractures. IMS was chosen for approximately 10% of midfacial and mandibular fractures. Others included tooth extraction and/or gingival suture at the site of alveolar fractures. Observation was chosen in 40% in the midface and in 20% in the mandible. In the midface, TCR was exclusively chosen for fractures of the zygoma, and IMS was chosen for alveolar fractures (Table 6). ORIF was performed for more than 50% of multiple fractures. Observation was also common for fractures of the nasal bone, zygoma, and maxilla. In the mandible, IMS was exclusively chosen for alveolar fractures (Table 7). MMF was performed in approximately 40% of patients. ORIF was chosen at a higher rate as the number of involved sites increased. Observation was relatively common in fractures of a single site. During the 32 years, treatment modalities have changed markedly (Figure 7). MMF has decreased from 30% in the early 90s to less than 5% in the past 15 years. In reverse, observation has increased from 20% in the early period to 40% in the past 10 years.
Table 5.
Treatment modalities according to fracture site.
Table 6.
Treatment of midfacial fractures according to fracture patterns.
Table 7.
Treatment of mandibular fractures according to fracture sites.
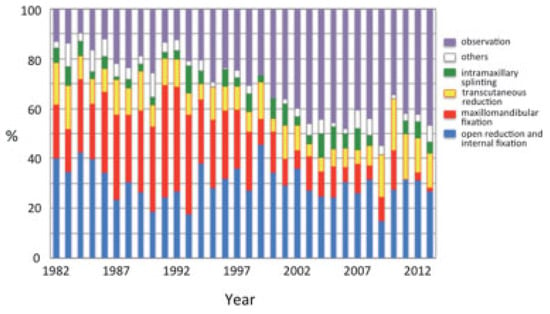
Figure 7.
Yearly ratio of treatment modalities.
Discussion
The present study was conducted in a university hospital located in a suburban city serving a suburban population (1.1 millions) and a surrounding rural population (0.3 million) in Nara prefecture, Japan. Some of the suburban inhabitants commute to the Osaka metropolitan area, but most rural inhabitants are engaged in local industries. According to census data for Nara prefecture, 3 and 30% workers were employed in the agriculture or forestry industries and construction or manufacturing industries, respectively, and the rest were engaged in industries such as information, finance, education, health care, service, and so on.
The present study clearly showed that the characteristics of maxillofacial fractures changed during 32 years in terms of age and gender distribution, cause and site of fractures, and treatment modalities. These results are considered to primarily reflect the change in population and social environment. The increase in annual number of the patients in the first 10 years is probably because our department became known as a medical institution for treating maxillofacial fractures. The decrease after the late 90s is primarily due to the opening of the new hospitals in the vicinity in which maxillofacial fractures can be managed. The population in our neighborhood has been stable over the period, but getting older. The population at 65 years or older was approximately 10% in 1982 and it increased to approximately 25% in 2012.
Maxillofacial fractures are typically a problem in the young population, especially in men, since they are physically and socially active and have a higher chance of being injured in traffic accidents, assaults, and sports activities [,,,,,,,,,,,]. The present study showed that more than one-half of the patients were in their 10s and 20s, consistent with previous studies [,,,]. Maxillofacial fractures in the elderly are considered less frequent and are mostly related to age-related changes and systemic pathologic conditions. However, traumatic injuries in the elderly have been increasing [,,]. In the 1980s, patients 60 years or older were fewer than 10% of all patients. In recent years, these patients consisted of approximately 30%. This result is considered due to a consequence of the increased life span with advances in medicine, resulting in a higher percentage of the elderly in the population and their more active lifestyle [,,]. The ratio of female patients slightly increased. This may also in part be attributed to the more active lifestyle of women in recent years as well as their increased life span.
Causes of injuries showed that traffic accidents were the most common cause of fractures throughout the period and consisted of more than half of the patients [,,,,,,,]. However, fractures in traffic accidents have been gradually decreasing in recent years, especially those in automobile and motorcycle accidents. These results may reflect the spread of safety equipment in these vehicles and the decreased population of motorcycle riders. Bicycle accidents were observed throughout the period because bicycles are commonly used for transportation by people of all ages, especially by young students []. Injuries in sports and by assaults were also observed throughout the period and were dominant in male patients [,,]. On the other hand, fractures by simple falls increased markedly and consisted of approximately 30% of all patients in recent years. These results were considered to reflect the increase of the older population. Older patients are likely to be injured by falling in daily life, probably because of the physiological consequences of aging, such as a reduced ability to balance and to avoid environmental hazards, the presence of systemic pathological conditions, and the use of psychotropic drugs [,,].
Fractures were more frequently observed in the mandible than in the midface, consistent with other studies [,,,,,,]. Recently, the ratio of midfacial fractures has been increasing. The reason for this change is not known, but it may be related to the age distribution and the cause of the injuries. Fractures in both the midface and mandible were observed frequently in patients injured in automobile and motorcycle accidents, probably because injuries in these accidents were more severe and occurred by high-velocity impact [].
In the midface, the zygoma was frequently involved because it is a prominent bone structure in the midface and therefore susceptible to various types of impact [,]. Fractures of the alveolar bone were also relatively common in the maxilla, because of the anterior alveolar bone is anatomically more protruded than the mandible. Although nasal bone fractures are also considered common midfacial fractures [,], only 13 isolated nasal bone fractures were observed. This was probably because most patients with nasal bone fractures were treated in otolaryngology and seldom consulted oral and maxillofacial surgery. Fractures of the maxilla were not so frequent and were observed in 139 patients (12.1%), because only the maxillary wall, Le Fort type I, and sagittal fractures were included in this category, and Le Fort type II or III fractures were classified into multiple fractures in the present study. The higher rate of multiple fractures in automobile and motorcycle accidents, falls from a height and work-related accidents may reflect that traumatic impact occurred more severely and at higher velocity [].
In the mandible, fractures were most frequently observed in the condyle, followed by the symphysis and the body. These results reflect that trauma force was applied in the symphyseal region, causing indirect fractures of the condyle with or without fractures in the symphyseal region, especially in patients injured by a simple fall [].The increase in condylar fractures in the recent period is considered due to the increase in the older population and in simple falls as the cause of the injuries. Mandibular angle fractures were commonly observed in patients injured in sports and by assaults [,,]. One of the reasons for these results is that the trauma force was applied laterally. The other is the presence of the third molar tooth at the site of the impact, because angle fractures were mostly observed in patients around 20 years old []. Symphyseal fractures were also common in patients injured in various causes and consisted of more than 20%, because the symphyseal region is also anatomically susceptible to traumatic impact. The recent decrease in symphyseal fractures may result from decreased automobile and motorcycle accidents.
Treatment was chosen according to the site and severity of the fracture and general condition of the patients. ORIF was performed in approximately 30% of the patients. In patients with fractures in both the midface and mandible, ORIF was chosen for more than 60% (129/208) of patients. This result is considered to reflect the severity of injuries in such patients. In midfacial and mandibular fractures, ORIF was performed in one-fourth of patients. However, ORIF was chosen for more than one-half of multiple fractures of the midface and of mandibular fractures with three and more sites, because these are also considered a severe condition. MMF was primarily chosen for mandibular fractures with one or two sites. The marked decrease in MMF in recent years may reflect the increase in older patients with a small number of residual teeth, the uses of prostheses, and nondisplaced fractures. Alveolar fractures were mostly treated by IMS. Although these fractures were not so severe, the rate of surgical intervention was relatively high because of concerns regarding occlusal disturbance and preservation of involved teeth. Observation was chosen for mandibular fractures with a single site at a higher rate, reflecting their less severe condition. However, in midfacial fractures, observation was also chosen at a relatively high rate in zygoma, maxilla, and multiple fractures. The necessity for reduction and/or fixation is dependent on the degree of displacement and impairment of function; however, the choice of treatment is not always determined by these factors. Some patients were reluctant to undergo surgery because they were not so concerned about a slight facial deformity or hypoesthesia unless function was seriously impaired [,], especially in older and medically compromised patients. Furthermore, when life-threatening injuries are complicated at the other sites of the body, the patients need to be primarily treated in another medical department [,,,]. Therefore, their maxillofacial fractures have to be minimally treated or sometimes untreated if they are not so severe.
Most patients were followed up from 6 months to 2 years. In patients treated by ORIF, plates and screws were principally removed within 1 year. Esthetic and functional outcomes of these patients were mostly satisfactory. However, objective evaluation of the outcomes of maxillofacial fractures was difficult because not all of the patients made the required visit after treatment, especially those followed by observation. Therefore, further studies were needed to evaluate the outcome of these patients.
In conclusion, the characteristics of maxillofacial fractures have changed over the years in terms of age and gender distribution, cause and site of fractures, and treatment modalities. Understanding the trend and characteristics of maxillofacial fractures is important to properly manage patients and to develop effective preventive measures.
Conflicts of Interest
None declared.
References
- Iida, S.; Kogo, M.; Sugiura, T.; Mima, T.; Matsuya, T. Retrospective analysis of 1502 patients with facial fractures. Int. J. Oral Maxillofac. Surg. 2001, 30, 286–290. [Google Scholar] [PubMed]
- Motamedi, M.H. An assessment of maxillofacial fractures: A 5-year study of 237 patients. J. Oral. Maxillofac. Surg. 2003, 61, 61–64. [Google Scholar]
- Al Ahmed, H.E.; Jaber, M.A.; Abu Fanas, S.H.; Karas, M. The pattern of maxillofacial fractures in Sharjah, United Arab Emirates: A review of 230 cases. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2004, 98, 166–170. [Google Scholar]
- Erol, B.; Tanrikulu, R.; Görgün, B. Maxillofacial fractures. Analysis of demographic distribution and treatment in 2901 patients (25-year experience). J. Craniomaxillofac. Surg. 2004, 32, 308–313. [Google Scholar] [PubMed]
- Brasileiro, B.F.; Passeri, L.A. Epidemiological analysis of maxillofacial fractures in Brazil: A 5-year prospective study. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2006, 102, 28–34. [Google Scholar]
- Cheema, S.A.; Amin, F. Incidence and causes of maxillofacial skeletal injuries at the Mayo Hospital in Lahore, Pakistan. Br. J. Oral. Maxillofac. Surg. 2006, 44, 232–234. [Google Scholar] [PubMed]
- Bakardjiev, A.; Pechalova, P. Maxillofacial fractures in Southern Bulgaria—A retrospective study of 1706 cases. J. Craniomaxillofac. Surg. 2007, 35, 147–150. [Google Scholar]
- Erdmann, D.; Follmar, K.E.; Debruijn, M.; et al. A retrospective analysis of facial fracture etiologies. Ann. Plast. Surg. 2008, 60, 398–403. [Google Scholar]
- Lee, J.H.; Cho, B.K.; Park, W.J. A 4-year retrospective studyof facial fractures on Jeju, Korea. J. Craniomaxillofac Surg. 2010, 38, 192–196. [Google Scholar]
- Gandhi, S.; Ranganathan, L.K.; Solanki, M.; Mathew, G.C.; Singh, I.; Bither, S. Pattern of maxillofacial fractures at a tertiary hospital in northern India: A 4-year retrospective study of 718 patients. Dent. Traumatol. 2011, 27, 257–262. [Google Scholar]
- van den Bergh, B.; Karagozoglu, K.H.; Heymans, M.W.; Forouzanfar, T. Aetiology and incidence of maxillofacial trauma in Amsterdam: A retrospective analysis of 579 patients. J. Craniomaxillofac. Surg. 2012, 40, e165–e169. [Google Scholar]
- Naveen Shankar, A.; Naveen Shankar, V.; Hegde, N.; Sharma Prasad, R. The pattern of the maxillofacial fractures—A multicentre retrospective study. J. Craniomaxillofac. Surg. 2012, 40, 675–679. [Google Scholar] [PubMed]
- Gerbino, G.; Roccia, F.; De Gioanni, P.P.; Berrone, S. Maxillofacial trauma in the elderly. J. Oral. Maxillofac. Surg. 1999, 57, 777–782, discussion 782–783. [Google Scholar] [PubMed]
- Chrcanovic, B.R.; Souza, L.N.; Freire-Maia, B.; Abreu, M.H. Facial fractures in the elderly: A retrospective study in a hospital in Belo Horizonte, Brazil. J. Trauma. 2010, 69, E73–E78. [Google Scholar]
- Yamamoto, K.; Matsusue, Y.; Murakami, K.; Horita, S.; Sugiura, T.; Kirita, T. Maxillofacial fractures in older patients. J. Oral. Maxillofac. Surg. 2011, 69, 2204–2210. [Google Scholar] [PubMed]
- Yamamoto, K.; Matsusue, Y.; Horita, S.; Murakami, K.; Sugiura, T.; Kirita, T. Maxillofacial fractures sustained in bicycle accidents. J. Oral. Maxillofac. Surg. 2011, 69, e155–e160. [Google Scholar] [CrossRef]
- Delilbasi, C.; Yamazawa, M.; Nomura, K.; Iida, S.; Kogo, M. Maxillofacial fractures sustained during sports played with a ball. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2004, 97, 23–27. [Google Scholar]
- Mourouzis, C.; Koumoura, F. Sports-related maxillofacial fractures: A retrospective study of 125 patients. Int. J. Oral. Maxillofac. Surg. 2005, 34, 635–638. [Google Scholar]
- Lee, K.H. Interpersonal violence and facial fractures. J. Oral. Maxillofac. Surg. 2009, 67, 1878–1883. [Google Scholar]
- Gomes, P.P.; Passeri, L.A.; Barbosa, J.R., Jr. A 5-year retrospective study of zygomatico-orbital complex and zygomatic arch fractures in Sao Paulo State, Brazil. J. Oral. Maxillofac. Surg. 2006, 64, 63–67. [Google Scholar]
- Rosado, P.; de Vicente, J.C. Retrospective analysis of 314 orbital fractures. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. 2012, 113, 168–171. [Google Scholar] [CrossRef]
- Rhee, S.C.; Kim, Y.K.; Cha, J.H.; Kang, S.R.; Park, H.S. Septal fracture in simple nasal bone fracture. Plast. Reconstr. Surg. 2004, 113, 45–52. [Google Scholar] [PubMed]
- Fattahi, T.; Steinberg, B.; Fernandes, R.; Mohan, M.; Reitter, E. Repair of nasal complex fractures and the need for secondary septo-rhinoplasty. J. Oral. Maxillofac. Surg. 2006, 64, 1785–1789. [Google Scholar] [CrossRef]
- Yamamoto, K.; Kuraki, M.; Kurihara, M.; et al. Maxillofacial fractures resulting from falls. J. Oral. Maxillofac. Surg. 2010, 68, 1602–1607. [Google Scholar] [PubMed]
- Subhashraj, K. A study on the impact of mandibular third molars on angle fractures. J. Oral. Maxillofac. Surg. 2009, 67, 968–972. [Google Scholar] [CrossRef]
- Down, K.E.; Boot, D.A.; Gorman, D.F. Maxillofacial and associated injuries in severely traumatized patients: Implications of a regional survey. Int. J. Oral. Maxillofac. Surg. 1995, 24, 409–412. [Google Scholar] [CrossRef]
- Tung, T.C.; Tseng, W.S.; Chen, C.T.; Lai, J.P.; Chen, Y.R. Acute life-threatening injuries in facial fracture patients: A review of 1,025 patients. J. Trauma. 2000, 49, 420–424. [Google Scholar] [CrossRef] [PubMed]
- Alvi, A.; Doherty, T.; Lewen, G. Facial fractures and concomitant injuries in trauma patients. Laryngoscope 2003, 113, 102–106. [Google Scholar] [CrossRef]
- Thorén, H.; Snäll, J.; Salo, J.; et al. Occurrence and types of associated injuries in patients with fractures of the facial bones. J. Oral. Maxillofac. Surg. 2010, 68, 805–810. [Google Scholar] [CrossRef]
© 2015 by the author. The Author(s) 2015.