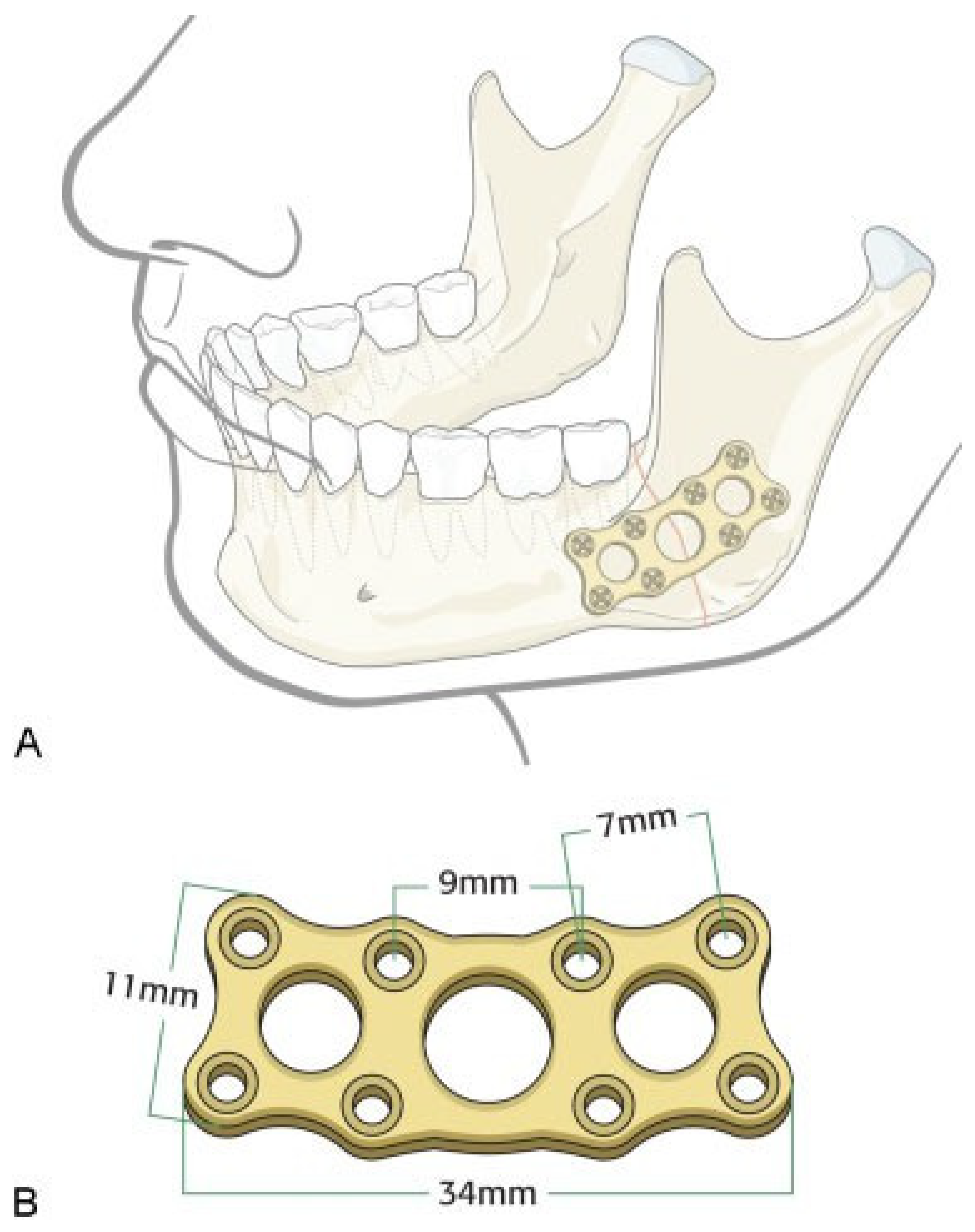
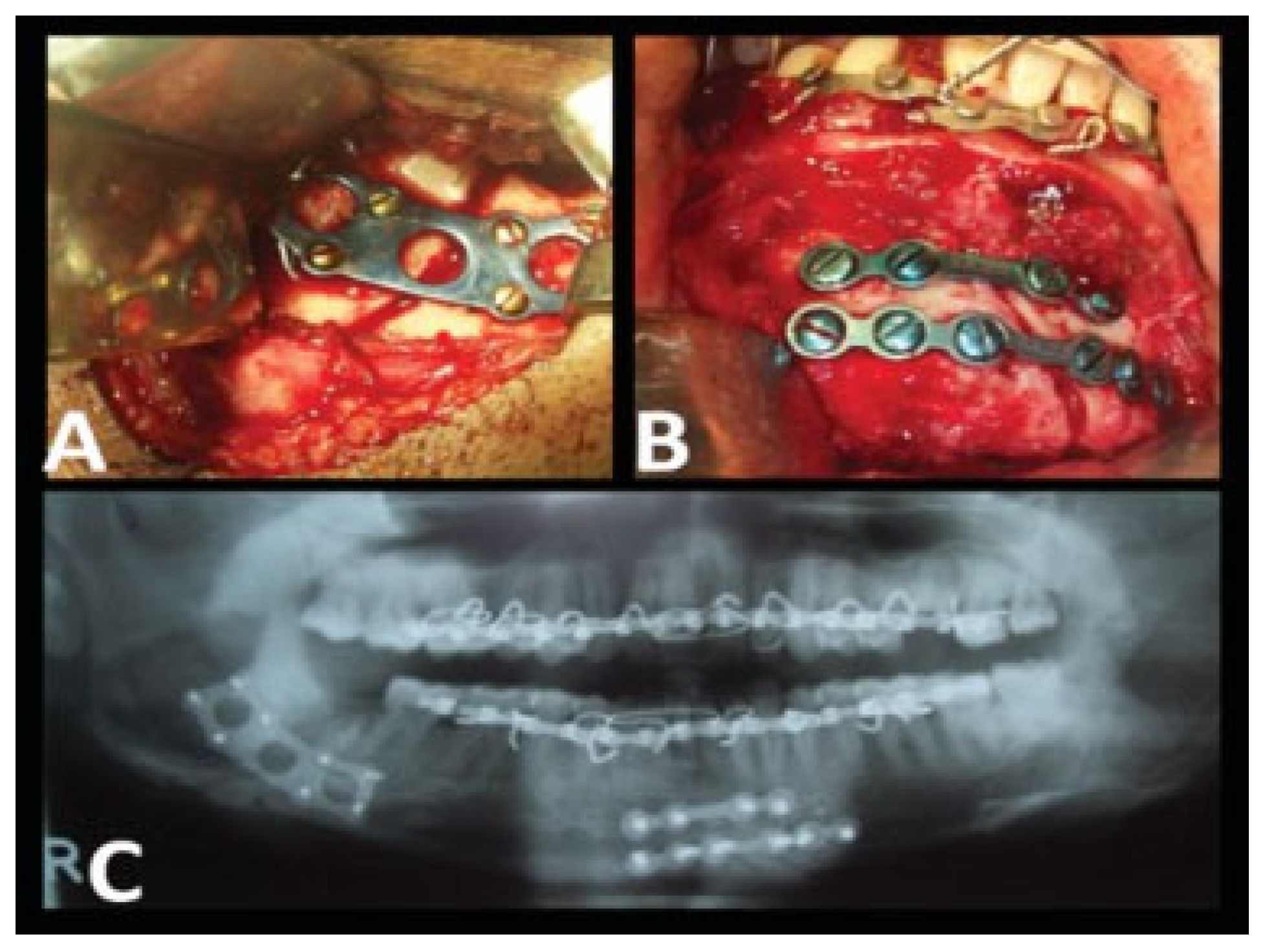
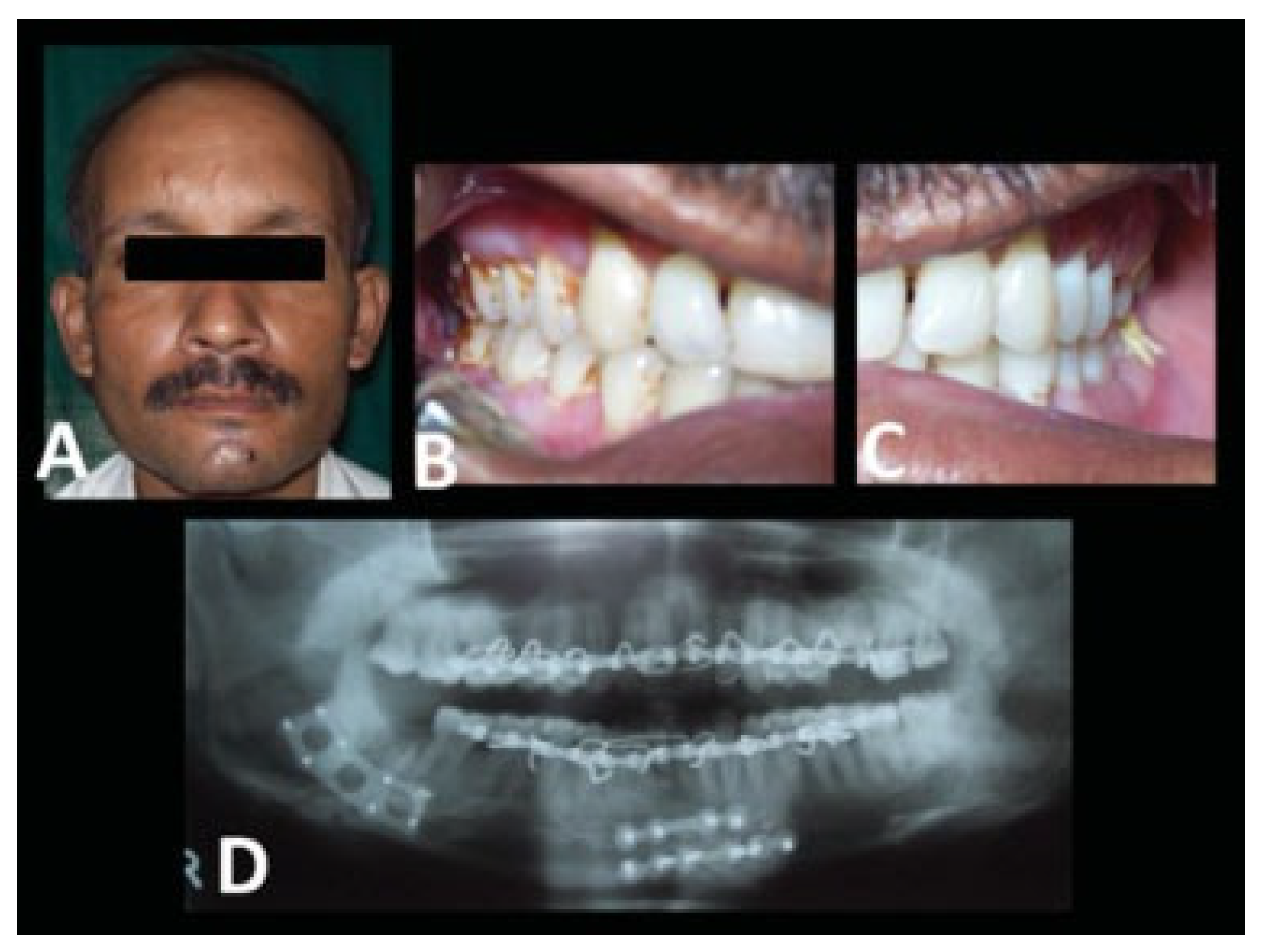
Evaluation of 2.0-mm Titanium Three-Dimensional Curved Angle Strut Plate in the Fixation of Mandibular Angle Fractures—A Prospective Clinical and Radiological Analysis
Abstract
:Materials and Methods
Results
Discussion
Sources of Support
Conflicts of Interest
References
- Michelet, F.X.; Deymes, J.; Dessus, B. Osteosynthesis with miniaturized screwed plates in maxillo-facial surgery. J Maxillofac Surg 1973, 1, 79–84. [Google Scholar] [CrossRef]
- Raveh, J.; Vuillemin, T.; Lädrach, K.; Roux, M.; Sutter, F. Plate osteosynthesis of 367 mandibular fractures. The unrestricted indication for the intraoral approach. J Craniomaxillofac Surg 1987, 15, 244–253. [Google Scholar] [CrossRef]
- Fridrich, K.L.; Pena-Velasco, G.; Olson, R.A. Changing trends with mandibular fractures: a review of 1,067 cases. J Oral Maxillofac Surg 1992, 50, 586–589. [Google Scholar] [CrossRef]
- Kroon, F.H.; Mathisson, M.; Cordey, J.R.; Rahn, B.A. The use of miniplates in mandibular fractures. An in vitro study. J Craniomaxillofac Surg 1991, 19, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Ellis, E., III; Karas, N. Treatment of mandibular angle fractures using two mini dynamic compression plates. J Oral Maxillofac Surg 1992, 50, 958–963. [Google Scholar] [CrossRef]
- Farmand, M.; Dupoirieux, L. The value of 3-dimensional plates in maxillofacial surgery [in French]. Rev Stomatol Chir Maxillofac 1992, 93, 353–357. [Google Scholar] [PubMed]
- Ellis, E., III; Walker, L. Treatment of mandibular angle fractures using two noncompression miniplates. J Oral Maxillofac Surg 1994, 52, 1032–1036, discussion 1036–1037. [Google Scholar] [CrossRef]
- Choi, B.H.; Kim, K.N.; Kang, H.S. Clinical and in vitro evaluation of mandibular angle fracture fixation with the two-miniplate system. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1995, 79, 692–695. [Google Scholar] [CrossRef] [PubMed]
- Klotch, D.W.; Gal, R.L. Repair of mandibular fractures using the 2.0. mm system. A review. J Craniomaxillofac Trauma 1995, 1, 38–42. [Google Scholar]
- Ellis, E., III; Walker, L.R. Treatment of mandibular angle fractures using one noncompression miniplate. J Oral Maxillofac Surg 1996, 54, 864–871, discussion 871–872. [Google Scholar] [CrossRef]
- Haug, R.H.; Barber, J.E.; Reifeis, R. A comparison of mandibular angle fracture plating techniques. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1996, 82, 257–263. [Google Scholar] [PubMed]
- Potter, J.; Ellis, E., III. Treatment of mandibular angle fractures with a malleable noncompression miniplate. J Oral Maxillofac Surg 1999, 57, 288–292, discussion 292–293. [Google Scholar]
- Collins, C.P.; Pirinjian-Leonard, G.; Tolas, A.; Alcalde, R. A prospective randomized clinical trial comparing 2.0-mm locking plates to 2.0-mm standard plates in treatment of mandible fractures. J Oral Maxillofac Surg 2004, 62, 1392–1395. [Google Scholar] [PubMed]
- Ellis, E., III; Graham, J. Use of a 2.0-mm locking plate/screw system for mandibular fracture surgery. J Oral Maxillofac Surg 2002, 60, 642–645, discussion 645–646. [Google Scholar] [PubMed]
- Ellis, E., III. Treatment of mandibular angle fractures using the AO reconstruction plate. J Oral Maxillofac Surg 1993, 51, 250–254, discussion 255. [Google Scholar] [CrossRef]
- Ellis, E., III; Sinn, D.P. Treatment of mandibular angle fractures using two 2.4-mm dynamic compression plates. J Oral Maxillofac Surg 1993, 51, 969–973. [Google Scholar]
- Wittenberg, J.M.; Mukherjee, D.P.; Smith, B.R.; Kruse, R.N. Biomechanical evaluation of new fixation devices for mandibular angle fractures. Int J Oral Maxillofac Surg 1997, 26, 68–73. [Google Scholar] [CrossRef]
- Haug, R.H.; Fattahi, T.T.; Goltz, M. A biomechanical evaluation of mandibular angle fracture plating techniques. J Oral Maxillofac Surg 2001, 59, 1199–1210. [Google Scholar]
- Bui, P.; Demian, N.; Beetar, P. Infection rate in mandibular angle fractures treated with a 2.0-mm 8-hole curved strut plate. J Oral Maxillofac Surg 2009, 67, 804–808. [Google Scholar]
- Guimond, C.; Johnson, J.V.; Marchena, J.M. Fixation of mandibular angle fractures with a 2.0-mm 3-dimensional curved angle strut plate. J Oral Maxillofac Surg 2005, 63, 209–214. [Google Scholar]
- Siddiqui, A.; Markose, G.; Moos, K.F.; McMahon, J.; Ayoub, A.F. One miniplate versus two in the management of mandibular angle fractures: a prospective randomised study. Br J Oral Maxillofac Surg 2007, 45, 223–225. [Google Scholar] [CrossRef] [PubMed]
- Marchena, J.M.; Padwa, B.L.; Kaban, L.B. Sensory abnormalities associated with mandibular fractures: incidence and natural history. J Oral Maxillofac Surg 1998, 56, 822–825, discussion 825–826. [Google Scholar] [CrossRef]
- Schultze-Mosgau, S.; Erbe, M.; Rudolph, D.; Ott, R.; Neukam, F.W. Prospective study on post-traumatic and postoperative sensory disturbances of the inferior alveolar nerve and infraorbital nerve in mandibular and midfacial fractures. J Craniomaxillofac Surg 1999, 27, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Thurmuller, P.; Dodson, T.B.; Kaban, L.B. Nerve injuries associated with facial trauma: Natural history, management, and outcome of treatment. OMFS Clin of N Amer 2001, 13, 283–293. [Google Scholar]
- Iizuka, T.; Lindqvist, C. Sensory disturbances associated with rigid internal fixation of mandibular fractures. J Oral Maxillofac Surg 1991, 49, 1264–1268. [Google Scholar] [CrossRef]
- Krakowiak, P.A.; Yamashita, D.D.; Yen, S. Recovery of inferior alveolar nerve function following open reduction internal fixation in traumatically induced mandibular fractures. J Oral Maxillofac Surg 2002, 60, 75–80. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case no. | Age | Sex | Etiology | Fractured sites |
| 1 | 25 | M | RTA | Rt. parasymphysis and Lt. angle |
| 2 | 22 | M | RTA | Lt. angle |
| 3 | 20 | M | RTA | Rt. parasymphysis and Lt. angle |
| 4 | 22 | M | Assault | Lt. angle |
| 5 | 25 | M | RTA | Lt. angle |
| 6 | 23 | M | RTA | Lt. body and Rt. angle |
| 7 | 27 | M | RTA | Lt. angle |
| 8 | 25 | M | Industrial | Lt. parasymphysis and Rt. angle |
| 9 | 32 | M | Fall | Lt. parasymphysis and Rt. angle |
| 10 | 27 | M | RTA | Rt. angle |
| 11 | 24 | M | RTA | Rt. angle |
| 12 | 38 | F | Fall | Lt. angle |
| 13 | 21 | M | RTA | Rt. parasymphysis and Lt. angle |
| 14 | 33 | M | RTA | B/l angle |
| 15 | 40 | M | RTA | Lt. parasymphysis and Rt. angle |
| 16 | 33 | M | RTA | Rt. parasymphysis and Lt. angle |
| 17 | 31 | M | RTA | Lt. angle |
| 18 | 50 | M | RTA | Lt. angle |
| 19 | 26 | F | Fall | Rt. angle |
| 20 | 32 | M | Assault | Lt. parasymphysis and Rt. angle |
| Case no. | Fractured sites | Displacement | Edema | Paraesthesia/anesthesia | Occlusion status |
| 1 | Rt. parasymphysis and Lt. angle | Displaced | +ve | —ve | Deranged |
| 2 | Lt. angle | Displaced | +ve | —ve | Deranged |
| 3 | Rt. parasymphysis and Lt. angle | Displaced | +ve | —ve | Deranged |
| 4 | Lt. angle | Minimally displaced | +ve | —ve | Deranged |
| 5 | Lt. angle | Minimally displaced | +ve | —ve | Deranged |
| 6 | Lt. body and Rt. angle | Displaced | +ve | +ve | Deranged |
| 7 | Lt. angle | Displaced | +ve | —ve | Deranged |
| 8 | Lt. parasymphysis and Rt. angle | Displaced | +ve | +ve | Deranged |
| 9 | Lt. parasymphysis and Rt. angle | Displaced | +ve | —ve | Deranged |
| 10 | Rt. angle | Minimally displaced | +ve | —ve | Deranged |
| 11 | Rt. angle | Displaced | +ve | —ve | Deranged |
| 12 | Lt. angle | Displaced | +ve | —ve | Deranged |
| 13 | Rt. parasymphysis and Lt. angle | Displaced | +ve | —ve | Deranged |
| 14 | B/l angle | Displaced | +ve | +ve | Deranged |
| 15 | Lt. parasymphysis and Rt. angle | Minimally displaced | +ve | —ve | Deranged |
| 16 | Rt. parasymphysis and Lt. angle | Displaced | +ve | —ve | Deranged |
| 17 | Lt. angle | Displaced | +ve | —ve | Deranged |
| 18 | Lt. angle | Displaced | +ve | —ve | Deranged |
| 19 | Rt. angle | Displaced | +ve | —ve | Deranged |
| 20 | Lt. parasymphysis and Rt. angle | Minimally displaced | +ve | —ve | Deranged |
| Case no. | Fractured site | Surgical approach | Special apparatus used |
| 1 | Rt. parasymphysis and Lt. angle | Extraoral | |
| 2 | Lt. angle | Extraoral | |
| 3 | Rt. parasymphysis and Lt. angle | Extraoral | |
| 4 | Lt. angle | Extraoral | |
| 5 | Lt. angle | Extraoral | |
| 6 | Lt. body and Rt. angle | Extraoral | |
| 7 | Lt. angle | Transbuccal | Transbuccal kit |
| 8 | Lt. parasymphysis and Rt. angle | Extraoral | |
| 9 | Lt. parasymphysis and Rt. angle | Extraoral | |
| 10 | Rt. angle | Extraoral | |
| 11 | Rt. angle | Extraoral | |
| 12 | Lt. angle | Transbuccal | Transbuccal kit |
| 13 | Rt. parasymphysis and Lt. angle | Extraoral | |
| 14 | B/l angle | Extraoral | |
| 15 | Lt. parasymphysis and Rt. angle | Extraoral | |
| 16 | Rt. parasymphysis and Lt. angle | Extraoral | |
| 17 | Lt. angle | Extraoral | |
| 18 | Lt. angle | Extraoral | |
| 19 | Rt. angle | Extraoral | |
| 20 | Lt. parasymphysis and Rt. angle | Extraoral |
| Case no. | Fractured site | Technique | Postoperative MMF | Complications |
| 1 | Rt. parasymphysis and Lt. angle | ORIF | Not required | |
| 2 | Lt. angle | ORIF | Not required | |
| 3 | Rt. parasymphysis and Lt. angle | ORIF | Not required | Transient nerve dysfunction |
| 4 | Lt. angle | ORIF | Not required | |
| 5 | Lt. angle | ORIF | Not required | |
| 6 | Lt. body and Rt. angle | ORIF | Not required | Infection |
| 7 | Lt. angle | ORIF | Not required | |
| 8 | Lt. parasymphysis and Rt. angle | ORIF | Not required | |
| 9 | Lt. parasymphysis and Rt. angle | ORIF | Not required | |
| 10 | Rt. angle | ORIF | Not required | Transient nerve dysfunction |
| 11 | Rt. angle | ORIF | Not required | |
| 12 | Lt. angle | ORIF | Not required | |
| 13 | Rt. parasymphysis and Lt. angle | ORIF | Not required | |
| 14 | B/l angle | ORIF | Not required | |
| 15 | Lt. parasymphysis and Rt. angle | ORIF | Not required | Infection |
| 16 | Rt. parasymphysis and Lt. angle | ORIF | Not required | |
| 17 | Lt. angle | ORIF | Not required | |
| 18 | Lt. angle | ORIF | Not required | Transient nerve dysfunction |
| 19 | Rt. angle | ORIF | Not required | |
| 20 | Lt. parasymphysis and Rt. angle | ORIF | Not required |
© 2014 by the author. The Author(s) 2014.
Share and Cite
Chhabaria, G.; Halli, R.; Chandan, S.; Joshi, S.; Setiya, S.; Shah, A. Evaluation of 2.0-mm Titanium Three-Dimensional Curved Angle Strut Plate in the Fixation of Mandibular Angle Fractures—A Prospective Clinical and Radiological Analysis. Craniomaxillofac. Trauma Reconstr. 2014, 7, 119-125. https://doi.org/10.1055/s-0034-1371002
Chhabaria G, Halli R, Chandan S, Joshi S, Setiya S, Shah A. Evaluation of 2.0-mm Titanium Three-Dimensional Curved Angle Strut Plate in the Fixation of Mandibular Angle Fractures—A Prospective Clinical and Radiological Analysis. Craniomaxillofacial Trauma & Reconstruction. 2014; 7(2):119-125. https://doi.org/10.1055/s-0034-1371002
Chicago/Turabian StyleChhabaria, Gaurav, Rajshekhar Halli, Sanjay Chandan, Samir Joshi, Sneha Setiya, and Anand Shah. 2014. "Evaluation of 2.0-mm Titanium Three-Dimensional Curved Angle Strut Plate in the Fixation of Mandibular Angle Fractures—A Prospective Clinical and Radiological Analysis" Craniomaxillofacial Trauma & Reconstruction 7, no. 2: 119-125. https://doi.org/10.1055/s-0034-1371002
APA StyleChhabaria, G., Halli, R., Chandan, S., Joshi, S., Setiya, S., & Shah, A. (2014). Evaluation of 2.0-mm Titanium Three-Dimensional Curved Angle Strut Plate in the Fixation of Mandibular Angle Fractures—A Prospective Clinical and Radiological Analysis. Craniomaxillofacial Trauma & Reconstruction, 7(2), 119-125. https://doi.org/10.1055/s-0034-1371002