Abstract
The term “foot drop” is defined as the loss of active dorsiflexion at the tibiotalar joint. Surgical procedures such as tendon transfer may be considered in patients who have had foot drop for more than a year. The most commonly reported tendon transfer in the treatment of drop foot is the tibialis posterior tendon. In cases where the tibialis posterior tendon is non-functional, transfer of one of the non-standard tendons such as FHL tendon to the dorsum of the foot is performed. In the presented case, the surgical technique of endoscopic transfer of the FHL tendon was illustrated. The patient’s AOFAS score was 50 points preoperatively and 78 points at the sixth postoperative month. The active dorsiflexion angle of the foot was increased to 0 degree from −30 degree.
1. Introduction
The term “foot drop” is defined as the loss of active dorsiflexion at the tibiotalar joint [1]. The gait disturbances associated with this dorsiflexion deficit adversely impact mobility and quality of life due to increased stumbling and falling risks [1,2]. Foot drop often hinders individuals from driving, participating in various sports, or engaging in regular exercise, and in severe cases, it restricts walking normal distances [3].
For patients with foot drop persisting for more than a year and with minimal chances of motor function recovery, surgical procedures such as tendon transfers may be considered [1]. The most commonly reported tendon transfer in the treatment of drop foot is the tibialis posterior tendon [1,4]. In cases where the tibialis posterior tendon is non-functional, transfer of one of the non-standard tendons to the dorsum of the foot is performed [5]. Transfer of the flexor hallucis longus (FHL) tendon is one of these non-standard tendon transfers [4,5]. Boszczyk et al. presented a case where the FHL tendon was transferred to the dorsum of the foot in the surgical management of foot drop [4].
Foot drop cases can also occur after lumbar decompression surgery [6]. Specific transfer procedures present the option of transferring the tendon subcutaneously or under the retinaculum. When transferred under a retinaculum, this acts as a pulley and increases effective tendon movement (range of motion); however, it brings the tendon closer to the ankle or subtalar axis and reduces the lever arm and therefore the strength of the transfer [5]. Transfer of the FHL (and FDL) as a dorsiflexion motor has been described in the pediatric cerebral palsy population by Hiroshima [7]. They transferred the Hiroshima FHL (and FDL in 62% of cases) by passing it under the extensor retinaculum. Hiroshima observed limited functional transformation in the transferred tendons and attributed the results obtained to the tenodesis effect [7]. Boszczyk et al. described the first FHL transfer in an adult patient. Hiroshima et al. stated that FHL may be due to compression of the tendon under the retinaculum during the procedure performed under the retinaculum. Therefore, in their FHL transfer technique, they transferred the tendon over the retinaculum [4]. In this surgical technique, we modified the technique described by Boszczyk et al. with endoscopic methods [4]. This article evaluates a case where a bilateral drop foot developed after lumbar decompression surgery. In this case, the FHL tendon was transferred to the dorsum of the foot with endoscopic assistance. We aim to present and assess this surgical technique.
2. Case Presentation
A 48-year-old male patient presented with bilateral dropped foot following lumbar disc herniation surgery. Due to the absence of a suitable tendon for transfer in the right ankle during the first year of lumbar surgery, the patient underwent arthroscopic tibiotalar arthrodesis surgery. Left extremity muscle function test: No function was observed in the tibialis anterior and extensor hallucis longus. Tibialis posterior muscle strength was 3/5. The preoperative flexion strength of the left big toe was assessed as 5/5. Approximately 8 months after arthrodesis, endoscopy-assisted flexor hallucis longus (FHL) transfer was performed on the patient’s left ankle.
The patient’s AOFAS (American Orthopedic Foot & Ankle Society) score on the left side was 50 points preoperatively and 78 points at the sixth postoperative month. The active dorsiflexion angle of the foot was increased to 0 degree from −30 degree.
3. Surgical Technique
The patient was positioned in the prone position under spinal anesthesia. Standard posteromedial (PM) and posterolateral (PL) portals, commonly used in posterior ankle arthroscopy, were employed (Figure 1). Utilizing the PL portal as the viewing portal, the retrocalcaneal space was debrided using a 4-mm arthroscopic shaver (Stryker Corporation, Kalamazoo, MI, USA) introduced through the PM portal. The subtalar joint was visualized, and the flexor hallucis longus (FHL) retinaculum was opened just medial to the lateral talar process. Subsequently, the FHL tendon was identified and visualized. The FHL muscle belly posterior to the talus and distal tibia was exposed. Following the method described by Boszczyk et al. [4], a window was created in the interosseous membrane, and the distal portion of the FHL muscle belly was resected using a shaver to prevent impingement (Figure 2).

Figure 1.
The patient was operated in the prone position. Posterolateral (PL), Posteromedial (PM) and Proximal posterolateral portals were used (PPL). PL was used as a viewing portal.
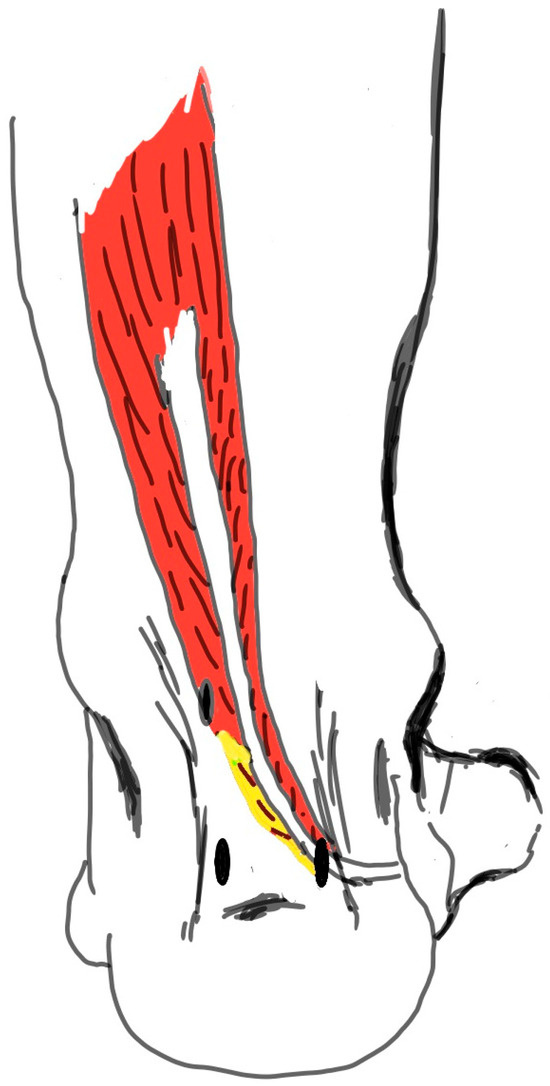
Figure 2.
The distal body of the muscle (the area marked with yellow) was resected using the shaver to prevent the FHL muscle body from being entrapped in the window opened in the interosseous membrane. FHL: Flexor Hallucis Longus.
Subsequently, a curved-tip clamp, inserted through the PL portal, was used to pass a suture tape around the FHL tendon. The tape was then retrieved through the PL portal, and the tendon was suspended (Figure 3). The camera was then repositioned, and the suspension was transferred to the PM portal. A three-point percutaneous achillesoplasty was performed on the achilles tendon. Following this, a medial approach to the midfoot was employed, and the FHL was identified at the henry notch. The FHL was then transected at this level (Figure 4). Subsequently, with the assistance of the suspension, the FHL tendon was retrieved through the PM portal (Figure 5).

Figure 3.
The tendon was suspended by passing the suture tape around the FHL tendon.

Figure 4.
The FHL tendon was found through a medial incision applied to the midfoot via navicular bone. Tendon was released from this level.

Figure 5.
After the FHL tendon was released, the tendon was pulled out of the PM portal.
While this procedure was being performed, the suture tape removed from the PL portal was replaced with the camera. FHL: Flexor Hallucis Longus, PL: Posterolateral portal, PM: Posteromedial portal.
Approximately 10 cm proximal to the PL portal, a 0.5 cm portal was created (Proximal Posterolateral Portal: PPL). Through this hole, a curved-tip clamp was inserted, and a percutaneous window was created in the interosseous membrane. At the level where the tendon would pass through the interosseous membrane, a 0.5 cm skin incision was made on the anterior aspect of the ankle. The FHL tendon was sutured distally, and using a thread, it was first moved to the PPL (Figure 6). Then, with the aid of the clamp, it was passed through the percutaneous window in the interosseous membrane and transferred from the skin incision on the anterior aspect of the ankle to the anterior aspect of the ankle (Figure 7).

Figure 6.
The FHL tendon extracted from the PM portal was moved to the PPL with a clamp.

Figure 7.
After a small skin incision made from the anterior of the interosceous membrane, the FHL tendon was moved from the PPL portal to the anterior of the ankle. Then, it was passed under the skin and tenodesis was performed to the middle kuneiforma using bioscrew.
Under fluoroscopy, the position of the middle cuneiform was determined. A 1 cm skin incision was made at the level where the tenodesis would be applied. Using a clamp, a tunnel was created beneath the skin and over the extensor retinaculum for the passage of the FHL tendon. The FHL was passed through this tunnel. Subsequently, a 6 mm-wide bone tunnel was created dorsally to plantarly on the middle cuneiform using a drill. The FHL tendon was passed through the tunnel with the aid of sutures. With the ankle in a neutral position, tenodesis of the FHL to the middle cuneiform was achieved using biovida. The skin incisions were closed using non-absorbable monofilament sutures, and a short leg cast was applied to the patient.
4. Postoperative Rehabilitation
In the second week postoperatively, the sutures were removed. The patient’s ambulation was transitioned to a short leg brace walking boot. For the initial 6 weeks postoperatively, weight-bearing was restricted on the operated side. Physical therapy and weight-bearing activities were initiated after the sixth postoperative week.
5. Discussion
Transfer of FHL to the dorsum of the foot is one of the non-conventional tendon transfers employed in the treatment of flatfoot. Endoscopy-assisted FHL transfer can render this surgery minimally invasive by reducing the size of skin incisions. Consequently, it helps minimize soft tissue damage associated with surgery. Additionally, endoscopy-assisted FHL transfer has been described for repairing Achilles tendon ruptures [8,9]. In this case, the procedure of cutting the FHL distally was performed using open surgery, which we designed as a modification of the technique of Bozscik et al. [4]. However, similar to its application in Achilles tendon cases, the process of cutting the FHL distally can be conducted using an endoscopic technique, making it even more minimally invasive.
Author Contributions
Conceptualization, A.Y. and M.Y.; methodology, A.Y.; software, N.E.; validation, A.Y., N.E. and M.Y.; formal analysis, N.E.; investigation, A.Y.; resources, M.Y.; data curation, M.Y.; writing—original draft preparation, A.Y.; writing—review and editing, N.E.; visualization, M.Y.; supervision, A.Y.; project administration, A.Y.; funding acquisition, N.E. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Prof. Dr. Cemil Taşcıoğlu City Hospital (protocol code 209 and 09/10/2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Stevoska, S.; Pisecky, L.; Stadler, C.; Gahleitner, M.; Klasan, A.; Klotz, M.C. Tendon transfer in foot drop: A systematic review. Arch. Orthop. Trauma Surg. 2023, 143, 773. [Google Scholar] [CrossRef] [PubMed]
- Stewart, J.D. Foot drop: Where, why and what to do? Pract. Neurol. 2008, 8, 158. [Google Scholar] [CrossRef] [PubMed]
- El-Osta, B.; Wilson, R. Concepts in Foot Drop Management—Review of the Current Literature. Acta Sci. Orthop. 2019, 2, 37. [Google Scholar] [CrossRef]
- Boszczyk, A.M.; Kordasiewicz, B. Flexor Hallucis Longus Transfer for Foot Drop without Functioning Tibialis Posterior. Přenos šlachy m. flexor hallucis longus u peroneální parézy bez využití m. tibialis posterior. Acta Chir. Orthop. Traumatol. Cech. 2017, 84, 466–468. [Google Scholar] [CrossRef] [PubMed]
- Jeng, C.; Myerson, M. The uses of tendon transfers to correct paralytic deformity of the foot and ankle. Foot Ankle Clin. 2004, 9, 319. [Google Scholar] [CrossRef] [PubMed]
- Macki, M.; Syeda, S.; Kerezoudis, P.; Gokaslan, Z.L.; Bydon, A.; Bydon, M. Preoperative motor strength and time to surgery are the most important predictors of improvement in foot drop due to degenerative lumbar disease. J. Neurol. Sci. 2016, 361, 133–136. [Google Scholar] [CrossRef] [PubMed]
- Hiroshima, K.; Hamada, S.; Shimizu, N.; Ohshita, S.; Ono, K. Anterior transfer of the long toe flexors for the treatment of spastic equinovarus and equinus foot in cerebral palsy. J. Pediatr. Orthop. 1988, 8, 164. [Google Scholar] [CrossRef] [PubMed]
- Lui, T.H. Endoscopic-Assisted Flexor Hallucis Longus Transfer: Harvest of the Tendon at Zone 2 or Zone 3. Arthrosc. Tech. 2015, 4, e811. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Lui, T.H.; Chan, W.C.; Maffulli, N. Endoscopic Flexor Hallucis Longus Tendon Transfer for Chronic Achilles Tendon Rupture. Sports Med. Arthrosc. Rev. 2016, 24, 38. [Google Scholar] [CrossRef] [PubMed]







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Published by MDPI on behalf of the American Podiatric Medical Association (APMA). Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.