
Impact of the HOPE Intervention on Mental Health Literacy, Psychological Well-Being and Stress Levels amongst University Undergraduates: A Randomised Controlled Trial



Abstract
:1. Introduction
2. Methods
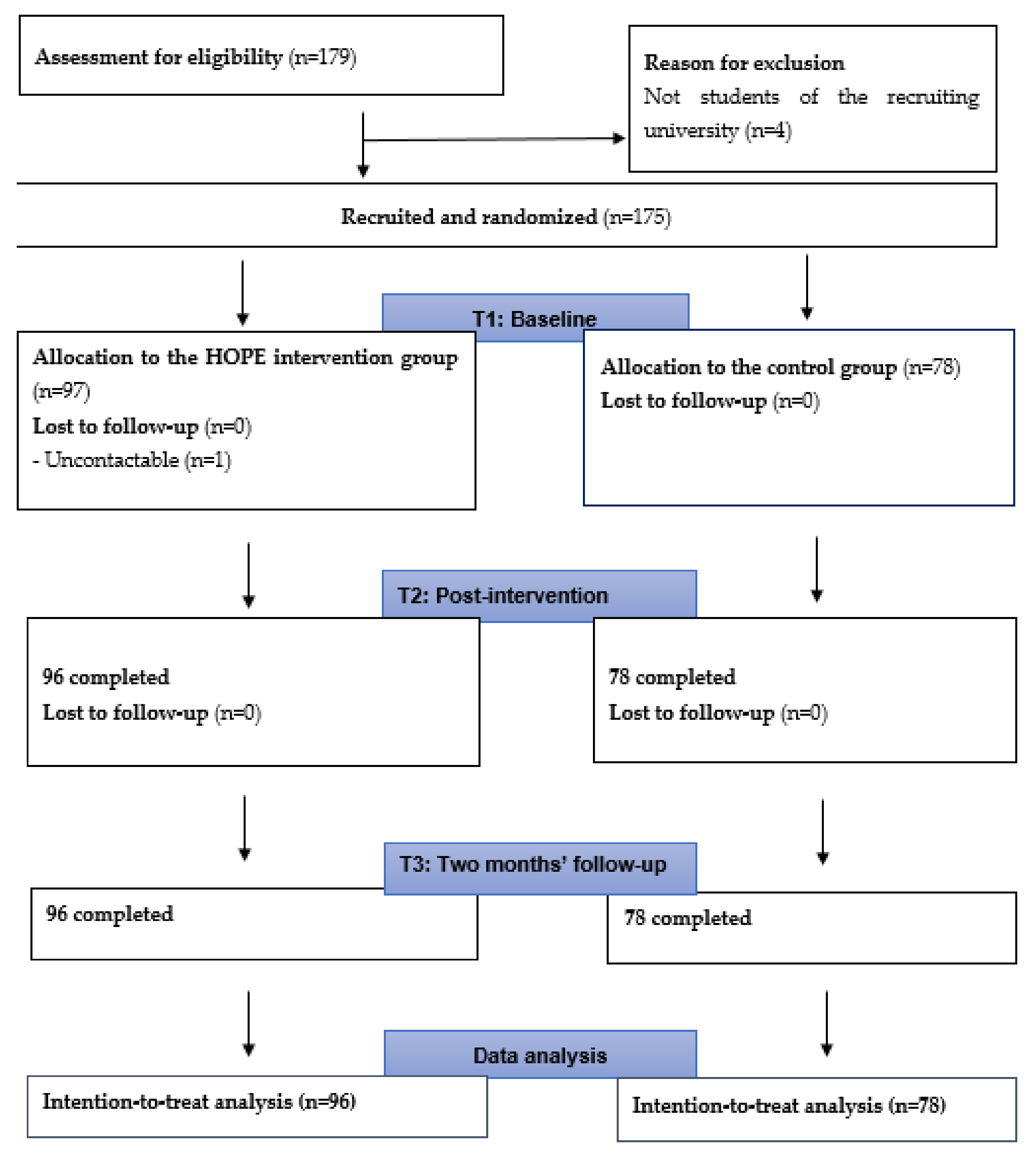
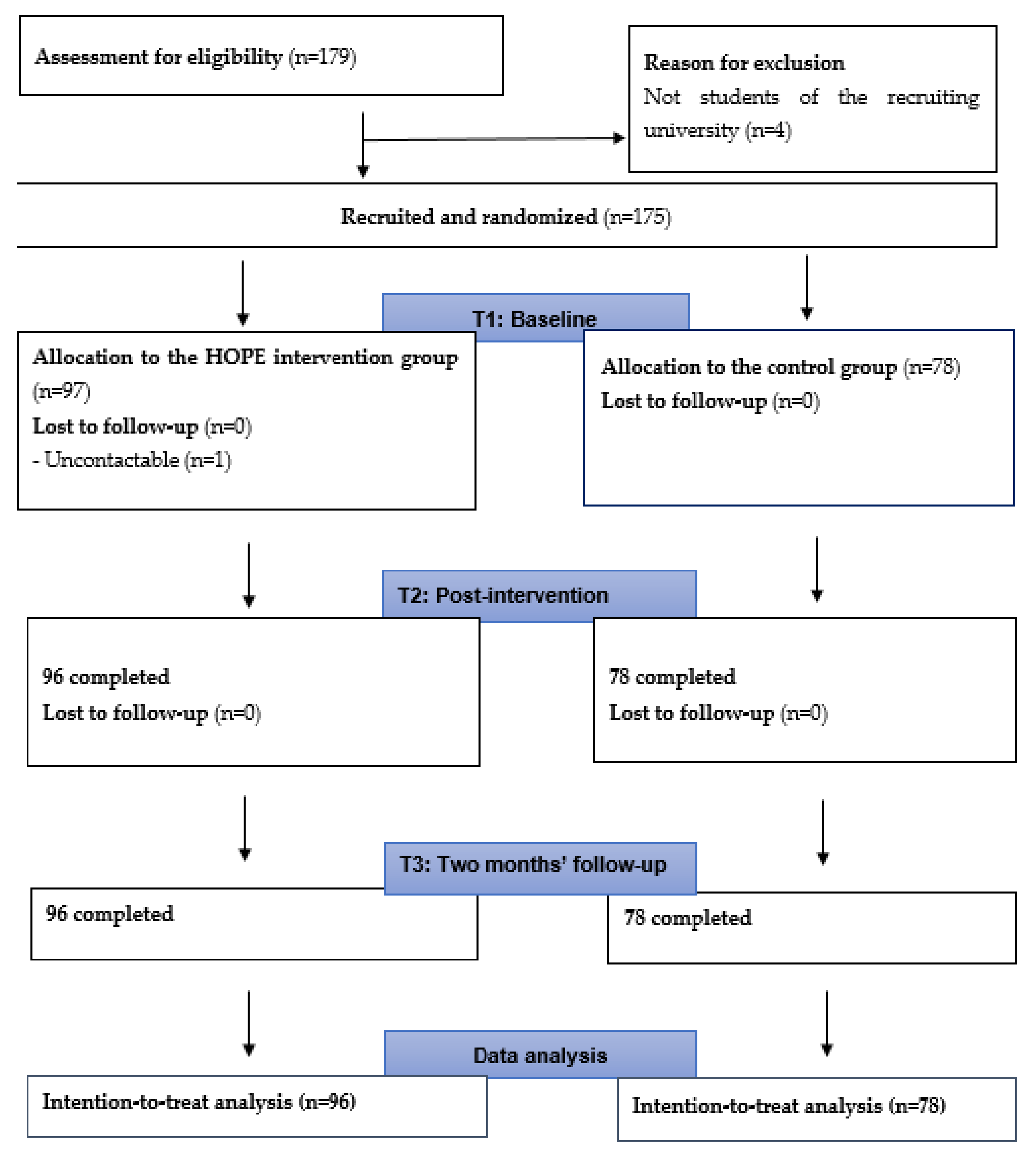
2.1. Study Design
2.2. Participants
2.3. Sample Size Calculation
2.4. Control Group
2.5. Intervention Group
2.6. Measurements
2.7. Data Collection Procedure
2.8. Data Analyses
2.9. Patient and Public Involvement
3. Results
3.1. Effects of the HOPE Interventions on Outcomes
3.1.1. Depression Literacy
3.1.2. Anxiety Literacy
3.1.3. Personal Stigma (Depression)
3.1.4. Stress and Psychological Well-Being
3.2. Factors Influencing Depression and Anxiety Literacy
4. Discussion
4.1. Depression Literacy
4.2. Factors Affecting Depression Literacy
4.3. Anxiety Literacy
4.4. Factors Affecting Anxiety Literacy
4.5. Personal Stigma (Depression)
4.6. Stress and Psychological Well-Being
5. Limitations
6. Contributions of the Study
7. Implications
8. Future Research Directions
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organisation. Child and Adolescent Mental Health. Available online: http://www.who.int/mental_health/maternal-child/child_adolescent/en/ (accessed on 1 November 2021).
- World Health Organization. The World Health Report 2001: Mental Disorders Affect One in Four People. Available online: https://www.who.int/news/item/28-09-2001-the-world-health-report-2001-mental-disorders-affect-one-in-four-people (accessed on 1 May 2021).
- Bu, D.; Chung, P.K.; Zhang, C.Q.; Liu, J.; Wang, X. Mental health literacy intervention on help-seeking in athletes: A systematic review. Int. J. Environ. Res. Public Health 2020, 17, 7263. [Google Scholar] [CrossRef] [PubMed]
- Daviu, N.; Bruchas, M.R.; Moghaddam, B.; Sandi, C.; Beyeler, A. Neurobiological links between stress and anxiety. Neurobiol. Stress 2019, 11, 100191. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer Publishing Company: Berlin/Heidelberg, Germany, 1984. [Google Scholar]
- Deci, E.L.; Ryan, R.M. Self-determination theory: A macrotheory of human motivation, development, and health. Can. Psychol./Psychol. Can. 2008, 49, 182. [Google Scholar] [CrossRef] [Green Version]
- Ryan, R.M.; Deci, E.L. On happiness and human potentials: A review of research on hedonic and eudaimonic well-being. Annu. Rev. Psychol. 2001, 52, 141–166. [Google Scholar] [CrossRef] [PubMed]
- Ryff, C.D. Happiness is everything, or is it? Explorations on the meaning of psychological well-being. J. Personal. Soc. Psychol. 1989, 57, 1069. [Google Scholar] [CrossRef]
- Browne, J.; Penn, D.L.; Meyer-Kalos, P.S.; Mueser, K.T.; Estroff, S.E.; Brunette, M.F.; Correll, C.U.; Robinson, J.; Rosenheck, R.A.; Schooler, N. Psychological well-being and mental health recovery in the NIMH RAISE early treatment program. Schizophr. Res. 2017, 185, 167–172. [Google Scholar] [CrossRef]
- Jorm, A.F.; Korten, A.E.; Jacomb, P.A.; Christensen, H.; Rodgers, B.; Pollitt, P. “Mental health literacy”: A survey of the public’s ability to recognise mental disorders and their beliefs about the effectiveness of treatment. Med. J. Aust. 1997, 166, 182–186. [Google Scholar] [CrossRef]
- Reavley, N.J.; Jorm, A.F. Public recognition of mental disorders and beliefs about treatment: Changes in Australia over 16 years. Br. J. Psychiatry 2012, 200, 419–425. [Google Scholar] [CrossRef]
- Sebastian, J.; Richards, D. Changing stigmatizing attitudes to mental health via education and contact with embodied conversational agents. Comput. Hum. Behav. 2017, 73, 479–488. [Google Scholar] [CrossRef]
- Taylor-Rodgers, E.; Batterham, P.J. Evaluation of an online psychoeducation intervention to promote mental health help seeking attitudes and intentions among young adults: Randomised controlled trial. J. Affect. Disord. 2014, 168, 65–71. [Google Scholar] [CrossRef]
- Hendriks, T.; Schotanus-Dijkstra, M.; Hassankhan, A.; De Jong, J.; Bohlmeijer, E. The efficacy of multi-component positive psychology interventions: A systematic review and meta-analysis of randomized controlled trials. J. Happiness Stud. 2020, 21, 357–390. [Google Scholar] [CrossRef] [Green Version]
- Tay, J.L.; Goh, Y.-S.S.; Klainin-Yobas, P. Online HOPE intervention on mental health literacy among youths in Singapore: An RCT protocol. J. Adv. Nurs. 2020, 76, 1831–1839. [Google Scholar] [CrossRef]
- AI-Therapy Statistics. Sample Size Calculator. Available online: https://www.ai-therapy.com/psychology-statistics/sample-size-calculator (accessed on 1 March 2018).
- Li, T.M.; Chau, M.; Wong, P.W.; Lai, E.S.; Yip, P.S. Evaluation of a web-based social network electronic game in enhancing mental health literacy for young people. J. Med. Internet Res. 2013, 15, e80. [Google Scholar] [CrossRef]
- Tay, J.L.; Tay, Y.F.; Klainin-Yobas, P. Effectiveness of information and communication technologies interventions to increase mental health literacy: A systematic review. Early Interv. Psychiatry 2018, 12, 1024–1037. [Google Scholar] [CrossRef]
- O’Reilly, C.L.; Bell, J.S.; Kelly, P.J.; Chen, T.F. Impact of mental health first aid training on pharmacy students’ knowledge, attitudes and self-reported behaviour: A controlled trial. Aust. N. Z. J. Psychiatry 2011, 45, 549–557. [Google Scholar] [CrossRef]
- Bond, K.S.; Jorm, A.F.; Kitchener, B.A.; Reavley, N.J. Mental health first aid training for Australian medical and nursing students: An evaluation study. BMC Psychol. 2015, 3, 11. [Google Scholar] [CrossRef] [Green Version]
- Gulliver, A.; Griffiths, K.M.; Christensen, H.; Mackinnon, A.; Calear, A.L.; Parsons, A.; Bennett, K.; Batterham, P.J.; Stanimirovic, R. Internet-based interventions to promote mental health help-seeking in elite athletes: An exploratory randomized controlled trial. J. Med. Internet Res. 2012, 14, e69. [Google Scholar] [CrossRef]
- Ribeiro, Z.M.T.; Spadella, M.A. Content validation of educational material on healthy eating for children under two years of age. Rev. Paul. Pediatr. 2018, 36, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Griffiths, K.M.; Christensen, H.; Jorm, A.F.; Evans, K.; Groves, C. Effect of web-based depression literacy and cognitive–behavioural therapy interventions on stigmatising attitudes to depression: Randomised controlled trial. Br. J. Psychiatry 2004, 185, 342–349. [Google Scholar] [CrossRef] [Green Version]
- Chong, S.A.; Abdin, E.; Picco, L.; Pang, S.; Jeyagurunathan, A.; Vaingankar, J.A.; Kwok, K.W.; Subramaniam, M. Recognition of mental disorders among a multiracial population in Southeast Asia. BMC Psychiatry 2016, 16, 121. [Google Scholar] [CrossRef] [Green Version]
- Yap, M.B.; Mackinnon, A.; Reavley, N.; Jorm, A.F. The measurement properties of stigmatizing attitudes towards mental disorders: Results from two community surveys. Int. J. Methods Psychiatr. Res. 2014, 23, 49–61. [Google Scholar] [CrossRef]
- Subramaniam, M.; Abdin, E.; Picco, L.; Pang, S.; Shafie, S.; Vaingankar, J.; Kwok, K.; Verma, K.; Chong, S. Stigma towards people with mental disorders and its components–a perspective from multi-ethnic Singapore. Epidemiol. Psychiatr. Sci. 2017, 26, 371–382. [Google Scholar] [CrossRef] [Green Version]
- Tay, J.L.; Xia, X.S.; Tan, C.L.R.; Qu, Y.; Loh, C.-L.J.; Lau, Y.; Klainin-Yobas, P. Evaluating predicting factors of psychological well-being among university and polytechnic students. Singap. Nurs. J. 2018, 45, 2–12. [Google Scholar]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Cohen, S. Perceived Stress in a Probability Sample of the United States. In The Social Psychology of Health; Spacapan, S., Oskamp, S., Eds.; Sage Publications, Inc.: Newbury Park, CA, USA, 1988; pp. 31–67. [Google Scholar]
- Teh, H.C.; Archer, J.A.; Chang, W.; Chen, S.A. Mental well-being mediates the relationship between perceived stress and perceived health. Stress Health 2015, 31, 71–77. [Google Scholar] [CrossRef]
- Gillespie-Lynch, K.; Brooks, P.J.; Someki, F.; Obeid, R.; Shane-Simpson, C.; Kapp, S.K.; Daou, N.; Smith, D.S. Changing college students’ conceptions of autism: An online training to increase knowledge and decrease stigma. J. Autism Dev. Disord. 2015, 45, 2553–2566. [Google Scholar] [CrossRef]
- Reavley, N.J.; Mackinnon, A.J.; Morgan, A.J.; Jorm, A.F. Stigmatising attitudes towards people with mental disorders: A comparison of Australian health professionals with the general community. Aust. N. Z. J. Psychiatry 2014, 48, 433–441. [Google Scholar] [CrossRef]
- Wright, A.; McGorry, P.D.; Harris, M.G.; Jorm, A.F.; Pennell, K. Development and evaluation of a youth mental health community awareness campaign–The Compass Strategy. BMC Public Health 2006, 6, 215. [Google Scholar] [CrossRef] [Green Version]
- Mamun, M.A.; Naher, S.; Moonajilin, M.S.; Jobayar, A.M.; Rayhan, I.; Kircaburun, K.; Griffiths, M.D. Depression literacy and awareness programs among Bangladeshi students: An online survey. Heliyon 2020, 6, e04901. [Google Scholar] [CrossRef]
- Amarasuriya, S.D.; Jorm, A.F.; Reavley, N.J. Quantifying and predicting depression literacy of undergraduates: A cross sectional study in Sri Lanka. BMC Psychiatry 2015, 15, 269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coles, M.E.; Ravid, A.; Gibb, B.; George-Denn, D.; Bronstein, L.R.; McLeod, S. Adolescent mental health literacy: Young people’s knowledge of depression and social anxiety disorder. J. Adolesc. Health 2016, 58, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Cotton, S.M.; Wright, A.; Harris, M.G.; Jorm, A.F.; McGorry, P.D. Influence of gender on mental health literacy in young Australians. Aust. N. Z. J. Psychiatry 2006, 40, 790–796. [Google Scholar] [CrossRef] [PubMed]
- Lauber, C.; Ajdacic-Gross, V.; Fritschi, N.; Stulz, N.; Rössler, W. Mental health literacy in an educational elite–an online survey among university students. BMC Public Health 2005, 5, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Townsend, L.; Musci, R.; Stuart, E.; Heley, K.; Beaudry, M.B.; Schweizer, B.; Ruble, A.; Swartz, K.; Wilcox, H. Gender differences in depression literacy and stigma after a randomized controlled evaluation of a universal depression education program. J. Adolesc. Health 2019, 64, 472–477. [Google Scholar] [CrossRef]
- Wang, J.; Adair, C.; Fick, G.; Lai, D.; Evans, B.; Perry, B.W.; Jorm, A.; Addington, D. Depression literacy in Alberta: Findings from a general population sample. Can. J. Psychiatry 2007, 52, 442–449. [Google Scholar] [CrossRef] [Green Version]
- Lambie, J.A.; Lindberg, A. The role of maternal emotional validation and invalidation on children’s emotional awareness. Merrill-Palmer Q. 2016, 62, 129–157. [Google Scholar] [CrossRef]
- Reavley, N.J.; McCann, T.V.; Jorm, A.F. Mental health literacy in higher education students. Early Interv. Psychiatry 2012, 6, 45–52. [Google Scholar] [CrossRef]
- Furnham, A.; Lousley, C. Mental health literacy and the anxiety disorders. Health 2013, 5, 521–531. [Google Scholar] [CrossRef] [Green Version]
- Paulus, D.J.; Wadsworth, L.P.; Hayes-Skelton, S.A. Mental health literacy for anxiety disorders: How perceptions of symptom severity might relate to recognition of psychological distress. J. Public Ment. Health 2015, 14, 94–106. [Google Scholar] [CrossRef] [Green Version]
- Arafat, S.Y.; Ahmed, S.; Uddin, S. Depression literacy status in Bangladesh: A cross-sectional comparative observation. J. Behav. Health 2018, 7, 91–97. [Google Scholar] [CrossRef]
- Bhuiyan, M.A.H.; Griffiths, M.D.; Mamun, M.A. Depression literacy among Bangladeshi pre-university students: Differences based on gender, educational attainment, depression, and anxiety. Asian J. Psychiatry 2020, 50, 101944. [Google Scholar] [CrossRef]
- Furnham, A.; Hamid, A. Mental health literacy in non-western countries: A review of the recent literature. Ment. Health Rev. J. 2014, 19, 84–98. [Google Scholar] [CrossRef]
- Tippin, G.K.; Maranzan, K.A. Efficacy of a Photovoice-based video as an online mental illness anti-stigma intervention and the role of empathy in audience response: A randomized controlled trial. J. Appl. Soc. Psychol. 2019, 49, 381–394. [Google Scholar] [CrossRef]
- Nasiri, S.; Akbari, H.; Tagharrobi, L.; Tabatabaee, A.S. The effect of progressive muscle relaxation and guided imagery on stress, anxiety, and depression of pregnant women referred to health centers. J. Educ. Health Promot. 2018, 7, 41. [Google Scholar]
- McGillivray, J.; Evert, H. Group cognitive behavioural therapy program shows potential in reducing symptoms of depression and stress among young people with ASD. J. Autism Dev. Disord. 2014, 44, 2041–2051. [Google Scholar] [CrossRef]
- Sizoo, B.B.; Kuiper, E. Cognitive behavioural therapy and mindfulness based stress reduction may be equally effective in reducing anxiety and depression in adults with autism spectrum disorders. Res. Dev. Disabil. 2017, 64, 47–55. [Google Scholar] [CrossRef]
- Khatamian Far, P. Challenges of recruitment and retention of university students as research participants: Lessons learned from a pilot study. J. Aust. Libr. Inf. Assoc. 2018, 67, 278–292. [Google Scholar] [CrossRef]

{kind=link}
| Intervention (n = 96) | Control (n = 78) | χ2 | p | |
|---|---|---|---|---|
| Frequency (%) | Frequency (%) | |||
| Age | 2.83 | 0.09 | ||
| 18–21 | 64 (66.67%) | 61 (78.21%) | ||
| 22–24 | 32 (33.33%) | 17 (21.79%) | ||
| Gender | 0.02 | 0.89 | ||
| Male | 28 (29.17%) | 22 (28.21%) | ||
| Female | 68 (70.83%) | 56 (71.79%) | ||
| Residential status | 2.56 | 0.28 | ||
| Singaporean | 90 (93.75%) | 68 (87.18%) | ||
| Permanent resident | 2 (2.08%) | 2 (2.56%) | ||
| Student pass | 4 (4.17%) | 8 (10.26%) | ||
| Ethnicity | 1.10 | 0.78 | ||
| Chinese | 87 (90.63%) | 68 (87.18%) | ||
| Malay | 2 (2.08%) | 1 (1.28%) | ||
| Indian | 6 (6.25%) | 8 (10.26%) | ||
| Others | 1 (1.04%) | 1 (1.28%) | ||
| Religion | 7.10 | 0.42 | ||
| Christian | 16 (16.67%) | 19 (24.36%) | ||
| Catholic | 9 (9.34%) | 3 (3.85%) | ||
| Buddhist | 25 (26.04%) | 18 (23.08%) | ||
| Taoism | 8 (8.33%) | 2 (2.56%) | ||
| Muslim | 2 (2.08%) | 3 (3.85%) | ||
| Hindu | 4 (4.17%) | 4 (5.13%) | ||
| Free-thinker | 28 (29.17%) | 27 (34.62%) | ||
| Others | 4 (4.17%) | 2 (2.56%) | ||
| Family/friends with mental health problems | 0.50 | 0.78 | ||
| Yes | 70 (72.92%) | 58 (74.36%) | ||
| No | 13 (13.54%) | 8 (10.26%) | ||
| Unsure | 13 (13.54%) | 12 (15.38%) | ||
| Personal experiences with mental health problems | 3.31 | 0.35 | ||
| Yes | 8 (8.33%) | 8 (10.26%) | ||
| No | 62 (64.58%) | 44 (56.41%) | ||
| Not sure did not seek help | 26 (27.08%) | 24 (30.77%) | ||
| Others | 0 | 2 (2.56%) | ||
| Contact with mental health professionals | 2.43 | 0.66 | ||
| Yes, for myself | 10 (10.42%) | 12 (15.38%) | ||
| Yes, for my friends/family | 10 (10.42%) | 4 (5.13%) | ||
| No | 67 (69.79%) | 55 (70.51%) | ||
| Yes, I know them personally | 7 (7.29%) | 5 (6.41%) | ||
| Others | 2 (2.08%) | 2 (2.56%) | ||
| Mean (SD) | Mean (SD) | t | p | |
| Depression literacy | 11.8 (3.59) | 12.36 (3.17) | 1.07 | 0.29 |
| Anxiety literacy | 10.39 (3.83) | 10.44 (3.23) | 0.09 | 0.93 |
| Personal stigma (depression) | 16.55 (3.99) | 15.77 (3.79) | −1.31 | 0.19 |
| PWB | 86.64 (16.24) | 88.40 (13.78) | 0.76 | 0.45 |
| Stress | 20.19 (5.69) | 20.10 (6.43) | −0.09 | 0.93 |
| Effects | Type III Sum of Squares | df | F | p Value | ηp2 | |
|---|---|---|---|---|---|---|
| Depression literacy | Group | 384.12 | 1 | 13.67 | <0.001 | 0.07 |
| Time-points | 263.29 | 2 | 33.67 | <0.001 | 0.16 | |
| Group × Time | 345.77 | 2 | 44.22 | <0.001 | 0.21 | |
| Anxiety literacy | Group | 519.87 | 1 | 17.18 | <0.001 | 0.09 |
| Time-points | 365.22 | 1.76 | 36.93 | <0.001 | 0.18 | |
| Group × Time | 287.33 | 1.76 | 29.06 | <0.001 | 0.15 | |
| Personal stigma | Group | 25.83 | 1 | 0.73 | 0.4 | 0.004 |
| Time-points | 47.46 | 2 | 5.05 | 0.007 | 0.028 | |
| Group × Time | 104.24 | 2 | 11.08 | <0.001 | 0.061 | |
| Stress | Group | 22.44 | 1 | 0.23 | 0.63 | 0.001 |
| Time-points | 0.56 | 2 | 0.03 | 0.97 | 0 | |
| Group × Time | 22.63 | 2 | 1.14 | 0.32 | 0.007 | |
| Psychological well-being | Group | 256.28 | 1 | 0.4 | 0.53 | 0.002 |
| Time-points | 9.75 | 2 | 0.15 | 0.86 | 0.001 | |
| Group × Time | 64.64 | 2 | 0.98 | 0.38 | 0.006 |
| Intervention | Control | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Time-Points | n | M (SD) | n | M (SD) | Mean Difference | t | 95% CI | p Value | |
| Depression literacy | Baseline | 96 | 11.80 (3.59) | 78 | 12.36 (3.17) | −0.56 | −1.07 | [−1.58–0.47] | 0.29 |
| Post-intervention | 96 | 15.24 (3.55) | 78 | 12.04 (3.24) | 3.2 | 6.15 | [2.17–4.23] | <0.001 | |
| 2-month follow-up | 96 | 14.81 (3.86) | 78 | 12.28 (3.15) | 2.53 | 4.66 | [1.46–3.60] | <0.001 | |
| Anxiety literacy | Baseline | 96 | 10.39 (3.83) | 78 | 10.44 (3.23) | −0.05 | −0.09 | [−1.13–1.03] | 0.93 |
| Post-intervention | 96 | 13.98 (3.94) | 78 | 10.54 (3.12) | 3.44 | 6.28 | [2.36–4.52] | <0.001 | |
| 2-month follow-up | 96 | 13.44 (4.05) | 78 | 10.81 (3.46) | 2.63 | 4.54 | [1.49–3.77] | <0.001 | |
| Personal stigma | Baseline | 96 | 16.55 (3.99) | 78 | 15.77 (3.79) | 0.78 | 1.31 | [−0.39–1.96] | 0.19 |
| Post-intervention | 96 | 14.75 (3.67) | 78 | 16.09 (4.17) | −1.34 | −2.26 | [−2.52–0.17] | 0.03 | |
| 2-month follow-up | 96 | 15.44 (3.92) | 78 | 16.22 (3.68) | −0.78 | −1.34 | [−1.93–0.37] | 0.18 | |
| Stress | Baseline | 96 | 20.19 (5.69) | 78 | 20.10 (6.43) | 0.08 | 0.09 | [−1.73–1.90] | 0.93 |
| Post-intervention | 96 | 19.94 (6.10) | 78 | 20.33 (6.73) | −0.40 | −0.41 | [−2.32–1.53] | 0.69 | |
| 2-month follow-up | 96 | 19.74 (6.48) | 78 | 20.68 (6.30) | −0.94 | −0.96 | [−2.87–0.99] | 0.34 | |
| Psychological well-being | Baseline | 96 | 86.64 (16.24) | 78 | 88.40 (13.78) | −1.76 | −0.76 | [−6.33–2.81] | 0.45 |
| Post-intervention | 96 | 87.27 (15.25) | 78 | 87.69 (16.13) | −0.42 | −0.18 | [−5.13–4.29] | 0.86 | |
| 2-month follow-up | 96 | 86.19 (16.18) | 78 | 88.23 (14.16) | −2.04 | −0.88 | [−6.65–2.56] | 0.38 | |
| Participants’ Characteristics | D-Lit | A-Lit | ||
|---|---|---|---|---|
| F | p | F | p | |
| s | 1.03 | 0.31 | 6.75 | * 0.01 |
| Ethnicity | 2.17 | 0.93 | 0.29 | 0.83 |
| Religion | 1.03 | 0.42 | 0.78 | 0.6 |
| Course of study | 2.18 | * 0.02 | 3.01 | ** 0.001 |
| Monthly household income | 0.16 | 0.99 | 0.2 | 0.98 |
| Satisfaction with monthly household income | 0.75 | 0.59 | 1.36 | 0.24 |
| Family/friends with mental health problems | 2.57 | 0.08 | 1.55 | 0.22 |
| Contact with mental healthcare professional | 4.25 | ** 0.003 | 8.33 | ** <0.001 |
| Welch | p | Welch | p | |
| Age | 1.84 | 0.18 | 2.94 | 0.09 |
| Residential status | 0.03 | 0.97 | 0.72 | 0.52 |
| Personal experiences with mental health problems | 3.36 | 0.11 | 3.43 | 0.11 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tay, J.L.; Goh, Y.S.S.; Sim, K.; Klainin-Yobas, P. Impact of the HOPE Intervention on Mental Health Literacy, Psychological Well-Being and Stress Levels amongst University Undergraduates: A Randomised Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 9772. https://doi.org/10.3390/ijerph19159772
Tay JL, Goh YSS, Sim K, Klainin-Yobas P. Impact of the HOPE Intervention on Mental Health Literacy, Psychological Well-Being and Stress Levels amongst University Undergraduates: A Randomised Controlled Trial. International Journal of Environmental Research and Public Health. 2022; 19(15):9772. https://doi.org/10.3390/ijerph19159772
Chicago/Turabian StyleTay, Jing Ling, Yong Shian Shawn Goh, Kang Sim, and Piyanee Klainin-Yobas. 2022. "Impact of the HOPE Intervention on Mental Health Literacy, Psychological Well-Being and Stress Levels amongst University Undergraduates: A Randomised Controlled Trial" International Journal of Environmental Research and Public Health 19, no. 15: 9772. https://doi.org/10.3390/ijerph19159772
APA StyleTay, J. L., Goh, Y. S. S., Sim, K., & Klainin-Yobas, P. (2022). Impact of the HOPE Intervention on Mental Health Literacy, Psychological Well-Being and Stress Levels amongst University Undergraduates: A Randomised Controlled Trial. International Journal of Environmental Research and Public Health, 19(15), 9772. https://doi.org/10.3390/ijerph19159772