The Experience of Patients with Endocrine Therapy for Breast Cancer: A Patient Journey Map Based on Qualitative Research

Abstract
1. Introduction
2. Materials and Methods
2.1. Evidence Consolidation
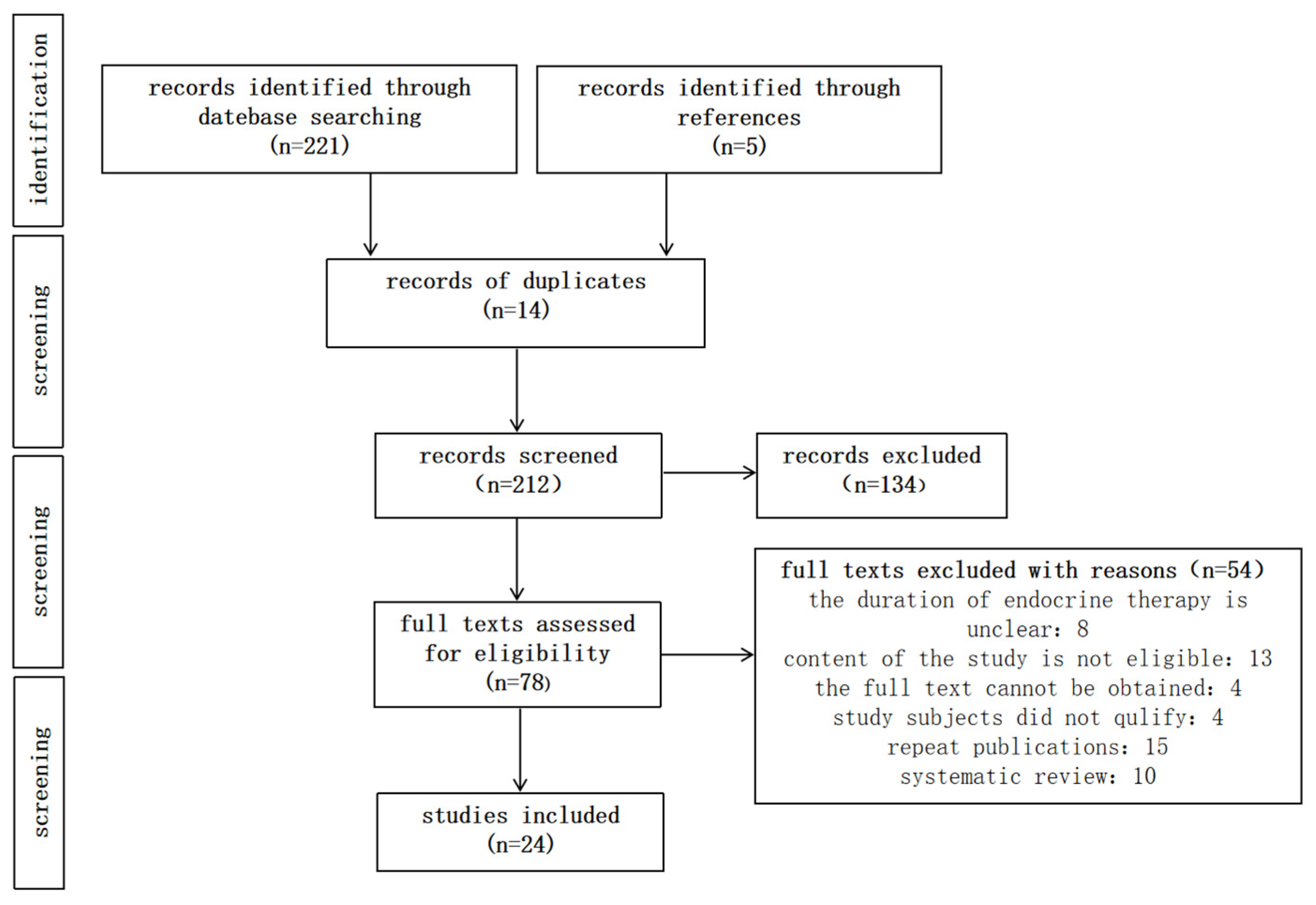
2.1.1. Search Strategy
2.1.2. Literature Selection Criteria
2.1.3. Data Extraction and Data Analysis
2.2. Qualitative Interviews
2.2.1. Participant Selection and Interview Process
2.2.2. Data Collection
2.2.3. Data Analysis
3. Results
3.1. Review
3.2. Interview
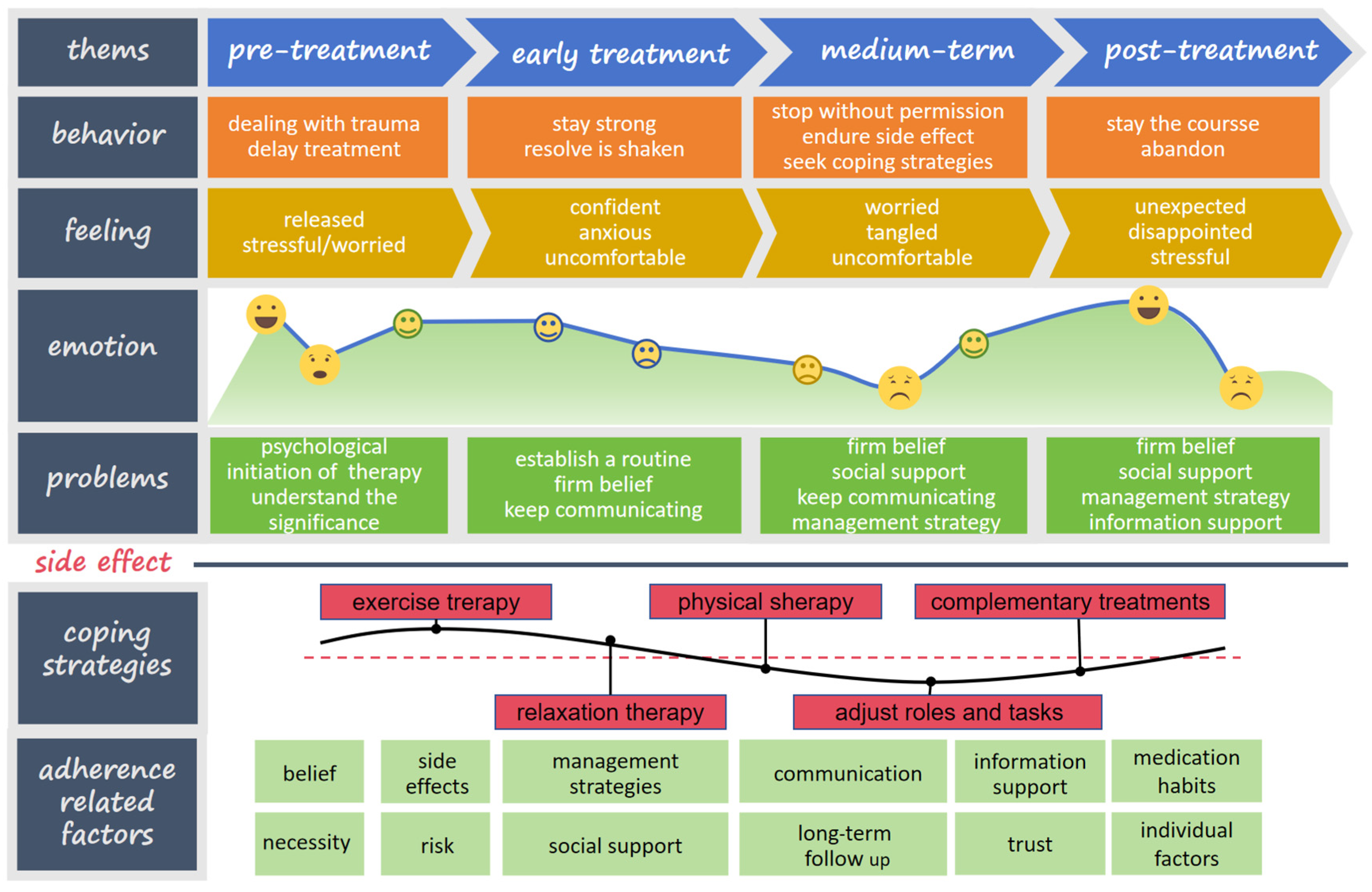
3.3. Patient Journey Map
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Katsura, C.; Ogunmwonyi, I.; Kankam, H.K.; Saha, S. Breast cancer: Presentation, investigation and management. Br. J. Hosp. Med. 2022, 83, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F.; Bsc, M.F.B.; Me, J.F.; Soerjomataram, M.I.; et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Clancy, C.; Lynch, J.; Oconnor, P.; Dowling, M. Breast cancer patients’ experiences of adherence and persistence to oral endocrine therapy: A qualitative evidence synthesis. Eur. J. Oncol. Nurs. 2020, 44, 101706. [Google Scholar] [CrossRef] [PubMed]
- Huppert, L.A.; Gumusay, O.; Idossa, D.; Rugo, H.S. Systemic therapy for hormone receptor-positive/human epidermal growth factor receptor 2-negative early stage and metastatic breast cancer. CA Cancer J. Clin. 2023, 73, 480–515. [Google Scholar] [CrossRef] [PubMed]
- Cella, D.; Fallowfield, L.J. Recognition and management of treatment-related side effects for breast cancer patients receiving adjuvant endocrine therapy. Breast Cancer Res. Treat. 2008, 107, 167–180. [Google Scholar] [CrossRef] [PubMed]
- AlOmeir, O.; Patel, N.; Donyai, P. Adherence to adjuvant endocrine therapy among breast cancer survivors: A systematic review and meta-synthesis of the qualitative literature using grounded theory. Support. Care Cancer 2020, 28, 5075–5084. [Google Scholar] [CrossRef]
- Cucciniello, L.; Garufi, G.; Di Rienzo, R.; Martinelli, C.; Pavone, G.; Giuliano, M.; Arpino, G.; Montemurro, F.; Del Mastro, L.; De Laurentiis, M.; et al. Estrogen deprivation effects of endocrine therapy in breast cancer patients: Incidence, management and outcome. Cancer Treat. Rev. 2023, 120, 102624. [Google Scholar] [CrossRef]
- Zong, X.; Wu, F.; Huang, Q.; Yang, R.; Yuan, C. Application of patient journey map based on patient experience in patient management. China Hosp. Manag. 2019, 44, 61–65. (In Chinese) [Google Scholar]
- Treloar, C.; Champness, S.; Simpson, P.L.; Higginbotham, N. Critical appraisal checklist for qualitative research studies. Indian. J. Pediatr. 2000, 67, 347–351. [Google Scholar] [CrossRef]
- Lewin, S.; Glenton, C.; Munthe-Kaas, H.; Carlsen, B.; Colvin, C.J.; Gülmezoglu, M.; Noyes, J.; Booth, A.; Garside, R.; Rashidian, A. Using qualitative evidence in decision making for health and social interventions: An approach to assess confidence in findings from qualitative evidence syntheses (GRADE-CERQual). PLoS Med. 2015, 12, e1001895. [Google Scholar] [CrossRef]
- Sun, X. An empirical analysis of in-depth interview research methods. J. Xi’an Jiaotong Univ. (Soc. Sci. Ed.) 2012, 32, 101–106. (In Chinese) [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Flanagan, J.; Tetler, D.; Winters, L.; Post, K.; Habin, K. The Experience of Initiating Oral Adjuvant Treatment for Estrogen Receptor-Positive Breast Cancer. Oncol. Nurs. Forum 2016, 43, E143–E152. [Google Scholar] [CrossRef] [PubMed]
- Toivonen, K.I.; Oberoi, D.; King-Shier, K.; Piedalue, K.-A.L.; Rash, J.A.; Carlson, L.E.; Campbell, T.S. Both “Vitamin L for Life” and “One Milligram of Satan”: A Multi-Perspective Qualitative Exploration of Adjuvant Endocrine Therapy Use after Breast Cancer. Curr. Oncol. 2021, 28, 2496–2515. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Wang, A. Health belief about adjuvant endocrine therapy in premenopausal breast cancer survivors: A qualitative study. Patient Prefer. Adherence 2019, 13, 1519–1525. [Google Scholar] [CrossRef] [PubMed]
- Harrow, A.; Dryden, R.; McCowan, C.; Radley, A.; Parsons, M.; Thompson, A.M.; Wells, M. A hard pill to swallow: A qualitative study of women’s experiences of adjuvant endocrine therapy for breast cancer. BMJ Open 2014, 4, e0052856. [Google Scholar] [CrossRef]
- Humphries, B.; Collins, S.; Guillaumie, L.; Lemieux, J.; Dionne, A.; Provencher, L.; Moisan, J.; Lauzier, S. Women’s Beliefs on Early Adherence to Adjuvant Endocrine Therapy for Breast Cancer: A Theory-Based Qualitative Study to Guide the Development of Community Pharmacist Interventions. Pharmacy 2018, 6, 53. [Google Scholar] [CrossRef]
- Karlsson, S.A.; Wallengren, C.; Olofsson Bagge, R.; Henoch, I. “It is not just any pill”-Women’s experiences of endocrine therapy after breast cancer surgery. Eur. J. Cancer Care 2019, 28, e130093SI. [Google Scholar]
- Bluethmann, S.M.; Murphy, C.C.; Tiro, J.A.; Mollica, M.A.; Vernon, S.W.; Bartholomew, L.K. Deconstructing Decisions to Initiate, Maintain, or Discontinue Adjuvant Endocrine Therapy in Breast Cancer Survivors: A Mixed-Methods Study. Oncol. Nurs. Forum 2017, 44, E101–E110. [Google Scholar] [CrossRef]
- Moon, Z.; Moss-Morris, R.; Hunter, M.S.; Hughes, L.D. Understanding tamoxifen adherence in women with breast cancer: A qualitative study. British J. Health Psychol. 2017, 22, 978–997. [Google Scholar] [CrossRef]
- Rooth, K.; Sundberg, K.; Gustavell, T.; Langius-Eklöf, A.; Gellerstedt, L. Symptoms and need for individualised support during the first year after primary treatment for breast cancer-A qualitative study. J. Clin. Nurs. 2024, 33, 2298–2308. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, J.M.; Walsh, E.A.; Park, E.R.; Berger, J.; Peppercorn, J.; Partridge, A.; Horick, N.; Safren, S.A.; Temel, J.S.; Greer, J.A. The Patient’s Voice: Adherence, Symptoms, and Distress Related to Adjuvant Endocrine Therapy After Breast Cancer. Int. J. Behav. Med. 2020, 27, 687–697. [Google Scholar] [CrossRef]
- van Londen, G.J.; Donovan, H.S.; Beckjord, E.B.; Cardy, A.L.; Bovbjerg, D.H.; Davidson, N.E.; Morse, J.Q.; Switzer, G.E.; Verdonck-de Leeuw, I.M.; Dew, M.A. Perspectives of Postmenopausal Breast Cancer Survivors on Adjuvant Endocrine Therapy-Related Symptoms. Oncol. Nurs. Forum 2014, 41, 660–668. [Google Scholar] [CrossRef]
- Pieters, H.C.; Green, E.; Khakshooy, S.; Sleven, M.; Stanton, A.L. A qualitative comparison of how older breast cancer survivors process treatment information regarding endocrine therapy. PLoS ONE 2019, 14, e02109721. [Google Scholar] [CrossRef]
- Eraso, Y.; Stefler, D.; Moon, Z.; Rossi, L.; Assefa, S. Extending Adjuvant Endocrine Therapy for 10 Years: A Mixed-Methods Analysis of Women’s Decision Making in an Online Breast Cancer Forum. Healthcare 2021, 9, 688. [Google Scholar] [CrossRef]
- Brett, J.; Boulton, M.; Fenlon, D.; Hulbert-Williams, N.J.; Walter, F.M.; Donnelly, P.; Lavery, B.; Morgan, A.; Morris, C.; Watson, E.K. Adjuvant endocrine therapy after breast cancer: A qualitative study of factors associated with adherence. Patient Prefer. Adherence 2018, 12, 291–300. [Google Scholar] [CrossRef]
- Yussof, I.; Mohamed Shah, N.; Ab Muin NF, I.; Abd Rahim, S.; Hatah, E.; Mohd Tahir, N.A.; Loganathan, K.; Munisamy, M. Challenges in Obtaining and Seeking Information Among Breast Cancer Survivors in an Asian Country: A Qualitative Study. J. Cancer Educ. 2024, 39, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Gomaa, S.; Lopez, A.; Slamon, R.; Smith, R.; Lapitan, E.; Nightingale, G.; Miller, S.M.; Wen, K.-Y. The lived experience of patients with breast cancer on adjuvant endocrine therapy: Side effects and coping strategies during the first year of medication initiation. Support. Care Cancer 2023, 31, 71912. [Google Scholar] [CrossRef]
- Wickersham, K.; Happ, M.B.; Bender, C.M. “Keeping the Boogie Man Away”: Medication Self-Management among Women Receiving Anastrozole Therapy. Nurs. Res. Pract. 2012, 2012, 462121. [Google Scholar] [CrossRef]
- Wen, K.; Smith, R.; Padmanabhan, A.; Goldstein, L. Patient experience of taking adjuvant endocrine therapy for breast cancer: A tough pill to swallow. Patient Exp. J. 2017, 4, 104–114. [Google Scholar] [CrossRef]
- Pellegrini, I.; Sarradon-Eck, A.; Ben Soussan, P.; Lacour, A.; Largillier, R.; Tallet, A.; Tarpin, C.; Julian-Reynier, C. Women’s perceptions and experience of adjuvant tamoxifen therapy account for their adherence: Breast cancer patients’ point of view. Psychooncology 2010, 19, 472–479. [Google Scholar] [CrossRef]
- Brauer, E.R.; Ganz, P.A.; Pieters, H.C. “Winging It”: How Older Breast Cancer Survivors Persist with Aromatase Inhibitor Treatment. J. Oncol. Pract. 2016, 12, e991–e1000. [Google Scholar] [CrossRef]
- Bourmaud, A.; Rousset, V.; Regnier-Denois, V.; Collard, O.; Jacquin, J.-P.; Merrouche, Y.; Lapoirie, J.; Tinquaut, F.; Lataillade, L.; Chauvin, F. Improving Adherence to Adjuvant Endocrine Therapy in Breast Cancer Through a Therapeutic Educational Approach: A Feasibility Study. Oncol. Nurs. Forum 2016, 43, E94–E103. [Google Scholar] [CrossRef]
- Roche, N.; Le Provost, J.; Borinelli-Franzoi, M.-A.; Boinon, D.; Martin, E.; Menvielle, G.; Dumas, A.; Rivera, S.; Conversano, A.; Matias, M.; et al. Facing points of view: Representations on adjuvant endocrine therapy of premenopausal patients after breast cancer and their healthcare providers in France. The FOR-AD study. Eur. J. Oncol. Nurs. 2023, 62, 102259. [Google Scholar] [CrossRef] [PubMed]
- Edwards, T.; Norcross, L.; Fine, J.; Martin, S.; Coulouvrat, C.; Spears, P.; Herold, C.I.; Ferrari, G.; Onwudiwe, N. Side effects and impacts of extended adjuvant endocrine therapy: A qualitative study among women with HR+/HER2-breast cancer. J. Clin. Oncol. 2023, 41S, e12509. [Google Scholar] [CrossRef]
- AlOmeir, O.; Patel, N.; Donyai, P. Hobson’s choice or a horned dilemma: A grounded theory on adherence to adjuvant endocrine therapy verified with breast cancer survivors. Support. Care Cancer 2022, 30, 10127–10136. [Google Scholar] [CrossRef]
- Groarke, A.; Curtis, R.; Groarke, J.M.; Hogan, M.J.; Gibbons, A.; Kerin, M. Post-traumatic growth in breast cancer: How and when do distress and stress contribute? Psychooncology 2017, 26, 967–974. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Item | Interview Questions |
|---|---|
| 1 | Are you familiar with what endocrine therapy entails? |
| 2 | What are your feelings or experiences after taking endocrine therapy medications? |
| 3 | In what ways has endocrine therapy impacted your work and personal life? |
| 4 | How have you coped with the challenges associated with endocrine therapy? |
| 5 | How confident do you feel about managing your own health during endocrine therapy? |
| 6 | What strategies do you use to manage your health while undergoing endocrine therapy? |
| 7 | Have you encountered any difficulties in managing your health during this treatment? |
| 8 | What types of support do you feel you need for effective health management during endocrine therapy? |
| Steps | Process |
|---|---|
| Step1: Collation | Convert audio recordings into text and organize the resulting content. |
| Step2: Familiarization | Read the transcribed text thoroughly, noting down initial impressions and ideas. |
| Step 3: Encoding | Systematically code features of the data across the entire dataset, collating relevant data under each code. |
| Step 4: Generate themes | Collect codes into potential themes, ensuring that all data pertinent to each theme is gathered. |
| Step 5: Check | Evaluate whether the themes are coherent and aligned with the categories, creating a thematic map to visualize the analysis. |
| Step 6: Refining | Refine the specifics of each theme and clarify the overall narrative that the analysis conveys. |
| Step 7: Finalization | Ensure that each theme accurately represents the data, including typical quotes to illustrate key points, and compile the findings into a comprehensive report. |
| Studies | Location | Sample Size | Data Collection | Characteristics of Participants | CASP | ||
|---|---|---|---|---|---|---|---|
| Age (Years) | Cancer Stage | Duration of Medication | |||||
| Flanagan 2016 [13] | Boston | 14 | individual interview | 48–81 | I–III | 0–2 years | 9 |
| Toivonen 2021 [14] | Alberta | 38 | individual interview | 56, 64 | I–II | 2–4 years | 9 |
| Xu, L. 2019 [15] | Northeast China | 30 | individual interview | 40.9 ± 8.09 | I–III | ≥1.5 years | 8 |
| Harrow 2014 [16] | Scotland | 30 | individual interview | 1–5 years | 8 | ||
| Humphries 2018 [17] | Canada | 43 | individual/focus group | ≥18 | I–III | 0–2 years | 10 |
| Karlsson 2019 [18] | Sweden | 25 | focus group interview | 42–80 | 3 years | 9 | |
| Bluethmann 2017 [19] | Texas | 30 | individual interview | 49–86 | I–III | 2–6 years | 9 |
| Moon 2017 [20] | London | 32 | Individual interview | 36–77 | 2 months–6 years | 9 | |
| Rooth 2024 [21] | Sweden | 17 | individual/focus group | 37–78 | 0–III | ≤1 years | 9 |
| Jacobs 2020 [22] | Boston | 30 | Individual interview | 27–76 | 0–III | 3 months–3 years | 9 |
| Van Londen 2014 [23] | Pittsburgh | 14 | focus group interview | ≥50 | 0–III | ≥1 years | 9 |
| Pieters 2019 [24] | California | 54 | Individual interview | 65–93 | I–III | 4 months–3 years | 10 |
| Eraso 2021 [25] | London | 61 | Online forum | 0–IV | ≤10 years | 10 | |
| Brett 2018 [26] | England Wales | 32 | Individual interview | 37–77 | 2–4 years | 8 | |
| Yussof 2024 [27] | Malaysian | 25 | Individual interview | I–III | ≥3 months | 9 | |
| Gomaa 2023 [28] | Philadelphia | 35 | Individual interview | 52.5 | I–III | ≤1 years | 8 |
| Wickersham 2012 [29] | Pittsburgh | 12 | Individual interview | 58–67 | ≤3 years | 10 | |
| Wen, K. 2017 [30] | Philadelphia | 12 | Individual interview | 33–72 | I–III | ≤5 years | 9 |
| Pellegrini 2010 [31] | Marseille, Nice | 34 | Individual interview | 35–64 | ≤5 years | 10 | |
| Brauer 2016 [32] | California | 27 | Individual interview | ≥65 | I–III | 4 months–3 years | 10 |
| Bourmaud 2016 [33] | France | 11 | Individual interview | 44–75 | I–III | 10–35 months | 9 |
| Roche 2023 [34] | Paris | 28 | focus group interview | 31–56 | I–III | 2.5 years | 9 |
| Edwards 2023 [35] | USA | 20 | Individual interview | 52.8 | 0–III | ≥4 years | 9 |
| AlOmeir 2022 [36] | UK | 14 | Individual interview | ≥40 | 2 months–16 years | 8 | |
| Time -Frame (Years) | Category | Sub-Category | Quotes | Related Studies | Overall CERQual |
|---|---|---|---|---|---|
| ≤2 | Challenges | Feelings of Abandonment and Distress | “I thought I would be through after [primary treatment].… I was upset that it’s going to drag on and on and on, but I do it.” | [13,14,17,20,21,22,23,24,31,36] | Moderate Confidence (High Relevance, Moderate coherence, and adequacy) |
| Processing the Trauma | “I need to work with someone who could help me redefine who I am, what’s important … really, in every aspect of my life.” | ||||
| Keeping Up the Facade | “I tried to act like nothing had happened. I dressed nice, did my makeup, all of it. I had to … for my family.” | ||||
| Toward Healing | “I need a GPS. I need a nurse. … I’m afraid I will just not do the work I need to do to really be better.” | ||||
| Establishing a Routine | “When I am out maybe on the weekend or at a conference. I did not bring my pill bottle with me. It is like a break of my normal routine.” | ||||
| Adherence | Belief and Necessity | “Taking tamoxifen just kind of pales into insignificance and it seems like a very small price to pay for not getting breast cancer again.” | [16,17,18,20,22,29,30,31,33,36] | Moderate Confidence (High Relevance and Adequacy, Moderate coherence) | |
| Communication and Follow-up | “I didn’t want to take [adjuvant ET] at this point, so [my oncologist] suggested taking half the tablet, and after 3 months I went back to see him and I had a smile on my face.” | [17,20,22,23,24,27,29,30,31,32,33,34,36] | |||
| Side Effects | “… the hot flashes. I would wake up during the night and be drenched.” | [17,20,21,22,23,24,27,28,29,30,31,32] | |||
| Common symptoms | Joint Pain (AI) | “…I think the stiffness I get, I feel very tight. My body. So when I go to get up after sitting for a little while, I feel like an old lady….” | [20,28,29,30,31,32] | High Confidence (High Relevance, coherence, and adequacy) | |
| Menopausal (Tamoxifen) | “…. Almost everything that I do, it doesn’t seem like I have the tolerance to actually do it more than 15 min because these hot flashes are coming every 10, 15 min….” “……Sometimes I can feel myself getting agitated…not sure it is from the pill.” | ||||
| Management Strategies | “…… Yes. I try to do yoga. Oh, um and workout… Walking helps tremendously. Yeah. I try to walk my dogs twice a day….” “…. so I take it at night, so it occurs during the night, and I don’t have it so much during the day….” | ||||
| 1–5 | Adherence | Side Effects and risk | “the medicine can lead to serious side effects, such as uterine cancer, vaginal bleeding. I was frightened by these side effects, so I didn’t dare to take the medicine.” “I was just exhausted… I realized that I wouldn’t be able to work and I couldn’t see myself getting through five years of that.” | [14,15,16,17,18,19,20,21,22,23,24,25,26,27,29,30,31,32,34,36] | High Confidence (High Relevance, coherence, and adequacy) |
| Management Strategies | “I think it could come down to almost, like, you need to be prescribed exercise.” “About two months of being on the medication, I began to have chronic diarrhea. I started to take a probiotic and it helped.” “I go to a homeopathic specialist who gives me trace elements to reduce the side effects.” | [14,16,18,19,20,21,22,23,24,25,26,27,29,30,31,32,34] | |||
| Belief and Necessity | “The doctor told me to take the medicine, but I think the surgery went very well, and it is not necessary to take medicine, so I did not take it.” “I guess the benefits, in my opinion, outweigh the risk and the side effects.” | [14,15,16,17,18,21,25,26,29,31,33,36] | |||
| Information Support | “I didn’t know anything about it. Really no one’s sort of explained what it is. They just said tamoxifen will help stopping recurrence.” “I have a friend who went through treatment five years ago…she can relate to the challenges of post-breast cancer treatment…she is a sounding board for me…” | [14,15,16,17,18,19,20,21,22,23,24,25,26,27,29,30,31,32,33,34,36] | |||
| Trust | “because I trust the clinical advice I’m being given.” | [16,19,21,25,33,36] | High Confidence (High Relevance, coherence, and adequacy | ||
| Individual Factors | I’m over the hill and so I didn’t feel the need to struggle with it as the same as I would’ve if I was younger.” “What a pity it would be for a woman to have no child. It’s imperfect for women. I will feel very sorry for my husband if I cannot give birth to a child for him.” | [14,15,17,20,22,25,26,30,31,36] | |||
| Habits and Illusion | “I have a pillbox, and basically, my reminder is when I give my husband his insulin at 9 and I take my pill.” “I stopped taking them for a couple of weeks while I was on holiday. I’d not taken them before, when I had flu for a week, and realised I felt better not taking them.” | [16,17,19,26,29,32,34,36] | |||
| Source of Energy | Social Support | “My husband and two children are a motivation for me to live.” “he really cared. He swapped me on to this one—I know he is doing what he can. If you feel someone cares, it kind of encourages you to keep going.” | [14,15,16,17,18,20,21,22,23,25,26,29,30,31,32,34,36] | High Confidence (High Relevance, coherence, and adequacy | |
| Return to Social Roles | “I do not like to stay at home doing nothing. I feel good when going to work” | [15,26,32] | |||
| Religious Beliefs | “I didn’t cry or scream as much as anyone else on the day I knew I was sick. I take death lightly, but I am not indifferent. I feel that everything I do in my life will be reversed in my next life.” | [15,30] | |||
| Mental journey | Impressions | “Tamoxifen has a truly bad reputation.” | [15,18,20,23,24,29,31,33] | Low Confidence (moderate Relevance, coherence, and adequacy ) | |
| Frustration and Anxiety | “And if you do get aches in your joints, I mean, you get scared, you know? What is going on with my body?” “The doctor frightened me so much with all the possible side effects that I asked myself, “Where are you going with this treatment?” | ||||
| The Last Link | “it went well this breast cancer journey. I don’t want to do this journey again … That’s why I take the pill every day.” | ||||
| Confronting or Surrender | “… and then when the side effects came then I felt like, no I can’t eat this. Because I have to live.” | [15,18,20,23,24,29,31,33] | Low Confidence: moderate relevance, coherence, and adequacy | ||
| Helplessness and Loneliness | “it’s so hard to explain it to someone else which; yes, you eat a pill. Really hard I think.” “So, if we forget [to ask], then they won’t tell you. sometimes, when we see the doctors, our mind gets blank.” | ||||
| Common symptoms | Menopausal symptoms, joint pain, weight gain | “Nothing really worked for my extreme joint pain. We tried all kinds of things.” “But when I started… in my hips, and it was at night and I was having trouble sleeping.” “I still have problems concentrating at work, I’m tired after 2–3 h, I have to take a break because I can’t do it anymore” | [16,18,19,21,22,25,26,30,31,34,35] | Moderate Confidence: high relevance, coherence, moderate adequacy | |
| ≥5 | Mental journey | Disappointment | “I was resigned to the side effects as I expected to be done after 5 years, only to be told current research and statistics indicate 10 years to be better than 5.” | [35] | Low Confidence: moderate relevance, low coherence, and adequacy |
| Hold on or give up | “When I was about to complete my 5 years, I had mixed feelings. On the one hand, it would have been great to give up all medication and return to my former self . On the other, I’m not happy taking the drug, but it beats the alternative.” | ||||
| Adherence | Individual factors | “I had a child of 13 years old then. I am a single mum, and looking into her heartbroken eyes, made me realized I needed to do the tamoxifen, whether I liked it or not.” “I am 68 and without family. My quality of life is very important.” | [15,19,20,25,36] | Moderate Confidence: high relevance, moderate coherence, and adequacy | |
| quality of life | “I’ve been on Tamoxifen for 7 years and I decided to come off. I’m 52, but felt like an old woman. I even struggled to get out of the bath. So I discussed to stop taking TAM with my consultant and he said yes.” | [15,19,20,25,35,36] | |||
| Information support | “I wonder why, since the oncologists knew about doing 10 years before my diagnosis, which they did, why wait until now? when I am about to complete my treatment. Now they say ‘oh, do more years” | [15,19,20,25,36] |
| Patient | Age (Years) | Marital Status | Fertility Status | Level of Education | Working Status | Duration of Medication |
|---|---|---|---|---|---|---|
| P1 | 60 | Married | Gravida | Primary school | Unemployed | 2 years |
| P2 | 54 | Married | Gravida | Primary school | Unemployed | 2.5 years |
| P3 | 49 | Married | Gravida | Secondary school | Employed | 3 years |
| P4 | 50 | Married | Gravida | Secondary school | Employed | 26 months |
| P5 | 27 | Single | Nulligravid | University | Employed | 54 months |
| P6 | 45 | Married | Gravida | Secondary school | Self-employed | 11.5 years |
| P7 | 42 | Married | Gravida | Secondary school | Employed | 28 months |
| P8 | 37 | Married | Gravida | university | Employed | 16 months |
| P9 | 44 | Divorced | Gravida | university | Employed | 6 years |
| P10 | 32 | Married | Nulligravid | university | Employed | 42 months |
| P11 | 50 | Married | Gravida | Secondary school | Unemployed | 3 years |
| P12 | 48 | Married | Gravida | Secondary school | Unemployed | 44 months |
| P13 | 23 | Single | Nulligravid | university | Employed | 1 years |
| P14 | 47 | Divorced | Gravida | university | Employed | 38 months |
| P15 | 52 | Married | Gravida | Secondary school | Self-employed | 55 months |
| P16 | 49 | Married | Gravida | Secondary school | Unemployed | 2 years |
| P17 | 62 | Married | Gravida | Secondary school | Retired | 6 months |
| P18 | 60 | Married | Gravida | Primary school | Unemployed | 10 months |
| P19 | 64 | Married | Gravida | Primary school | Retired | 14 months |
| P20 | 68 | Widowed | Gravida | illiteracy | Unemployed | 11 months |
| Category | Sub-Category | Quotes |
|---|---|---|
| Initiating treatment while experiencing stress. | Brief relaxation | “The hardest time was when I had chemo. I couldn’t sleep before every chemo. Now I’m fine. “I feel that taking this medicine should not be so uncomfortable; the most uncomfortable time has been survived.” |
| Concerns regarding treatment adherence | “I’m experiencing hot flashes that come on suddenly, leaving my whole body soaked and giving me a feeling of emptiness. I just don’t know how much longer I can hold on to this.” | |
| Limited understanding of endocrine therapy | Insufficient understanding | “I understand that taking this medication is beneficial for this area (pointing to the surgical site), but I’m not sure about the other effects. We’re not professionals, so when the doctor advised me to take it, I wasn’t aware of the potential negative reactions that could occur.” |
| Struggling to manage the side effects of medication | “The most noticeable issue is the discomfort in my bones, particularly joint pain in my hips and knees. For instance, after sitting for a long time, I have to get up slowly, and if I try to rise quickly, it causes pain in my bones. Sometimes, I find myself trying to avoid movement altogether.“ | |
| Feeling weak on the inside but unable to express it | Insufficient support system | “At first, my husband accompanied me to the hospital, but now I come alone. I feel anxious about the review results and worry that they might not be favorable. The thought of facing the situation alone is quite daunting for me.” |
| Altered body image | “I lost all my hair during chemotherapy, and now taking this medication is really uncomfortable. I’ve become very thin and can’t seem to gain weight, which makes me feel unattractive.” | |
| Experiencing feelings of guilt | “My parents are quite elderly and still have to take care of my needs. I feel really sorry for them.” “My daughter is still very young, and I need to be there for her as she grows up” | |
| Self-management behaviors and their influencing factors | Modifying roles and lifestyle | “I run every day, and my time off work is fairly consistent. I find that it really helps my physical condition and boosts my mood. If I don’t exercise, I feel like I’ve wasted the day.” “Our work pressure is quite high, and we often have to put in overtime. I’ve decided to look for a job that is less intense. Most family responsibilities have been handed over to my husband to help balance things out.” |
| Elderly patients exhibit positive and higher levels of self-efficacy | “I try to drink less water before going to bed so I won’t have to get up to use the bathroom. I also avoid looking at my phone before sleep because it makes me feel more energized. Instead, I don’t set an alarm clock and let myself wake up naturally. If I can’t fall asleep, I sometimes just lie down and rest.” | |
| Related factors: Improved recovery, Open-minded attitude Return to work… | “Based on my current health status and the results of my recent re-examination, everything appears to be quite stable. If I need to take medication, I will definitely make sure to stick with it.” “My state of mind is very positive. I’m over 60 years old, and my examinations have come back fine. The most challenging part of chemotherapy is behind me, and now I’m eating and sleeping well. I definitely need to maintain my confidence.” “Maintaining a regular work routine while allowing myself time off can sometimes be confusing. However, I find that I feel better when I’m at work, and it boosts my confidence to stay committed.” | |
| Self-management challenges | insufficient information | “I feel that I especially need guidance on some important precautions, particularly detailed advice. Since we are also relying on the internet, it would be helpful to receive better recommendations on how to manage this disease effectively.” |
| disruption of services | “… At first, I wasn’t sure what questions I should ask, but after some time, I started to have concerns. However, when I left the hospital, the nurse only briefly reminded me to continue taking my medication and to attend follow-up appointments on time. Sometimes, I feel like the interns forget who I am.” |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yao, Y.; He, T.; Tian, X. The Experience of Patients with Endocrine Therapy for Breast Cancer: A Patient Journey Map Based on Qualitative Research. Curr. Oncol. 2024, 31, 5873-5888. https://doi.org/10.3390/curroncol31100437
Yao Y, He T, Tian X. The Experience of Patients with Endocrine Therapy for Breast Cancer: A Patient Journey Map Based on Qualitative Research. Current Oncology. 2024; 31(10):5873-5888. https://doi.org/10.3390/curroncol31100437
Chicago/Turabian StyleYao, Yingyan, Ting He, and Xiaoying Tian. 2024. "The Experience of Patients with Endocrine Therapy for Breast Cancer: A Patient Journey Map Based on Qualitative Research" Current Oncology 31, no. 10: 5873-5888. https://doi.org/10.3390/curroncol31100437
APA StyleYao, Y., He, T., & Tian, X. (2024). The Experience of Patients with Endocrine Therapy for Breast Cancer: A Patient Journey Map Based on Qualitative Research. Current Oncology, 31(10), 5873-5888. https://doi.org/10.3390/curroncol31100437