Radiomic Machine-Learning Analysis of Multiparametric Magnetic Resonance Imaging in the Diagnosis of Clinically Significant Prostate Cancer: New Combination of Textural and Clinical Features

 ,
,  , ,
, ,  ,
,
Abstract
:1. Introduction
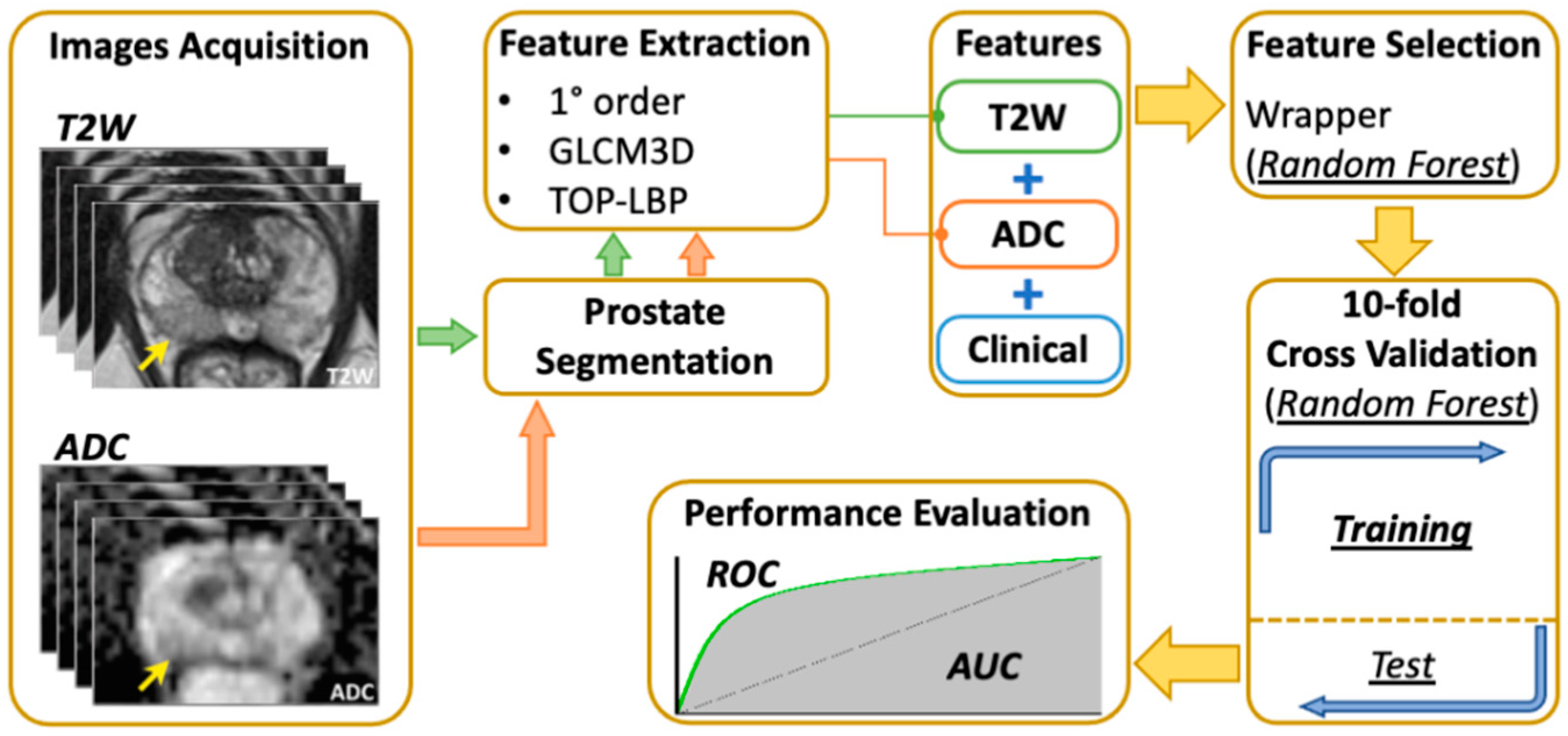
2. Materials and Methods
2.1. Patient Cohort
- Serum PSA ≤ 20 ng/mL;
- Patients who underwent mpMRI and fusion prostate biopsy plus standard 12-core systematic TRUS biopsy within a month from the MRI;
- Suspicious prostate lesion areas (PIRADS ≥ 3);
- Prostate lesions with definite boundaries (regular margins) and classified according to the latest version of PI-RADS score [9];
- Clinical stage ≤ T2 at mpMRI (organ-confined PCa).
- Exclusion criteria were defined as follows:
- Prior treatment for PCa;
- Poor MRI image quality due to serious image artefacts;
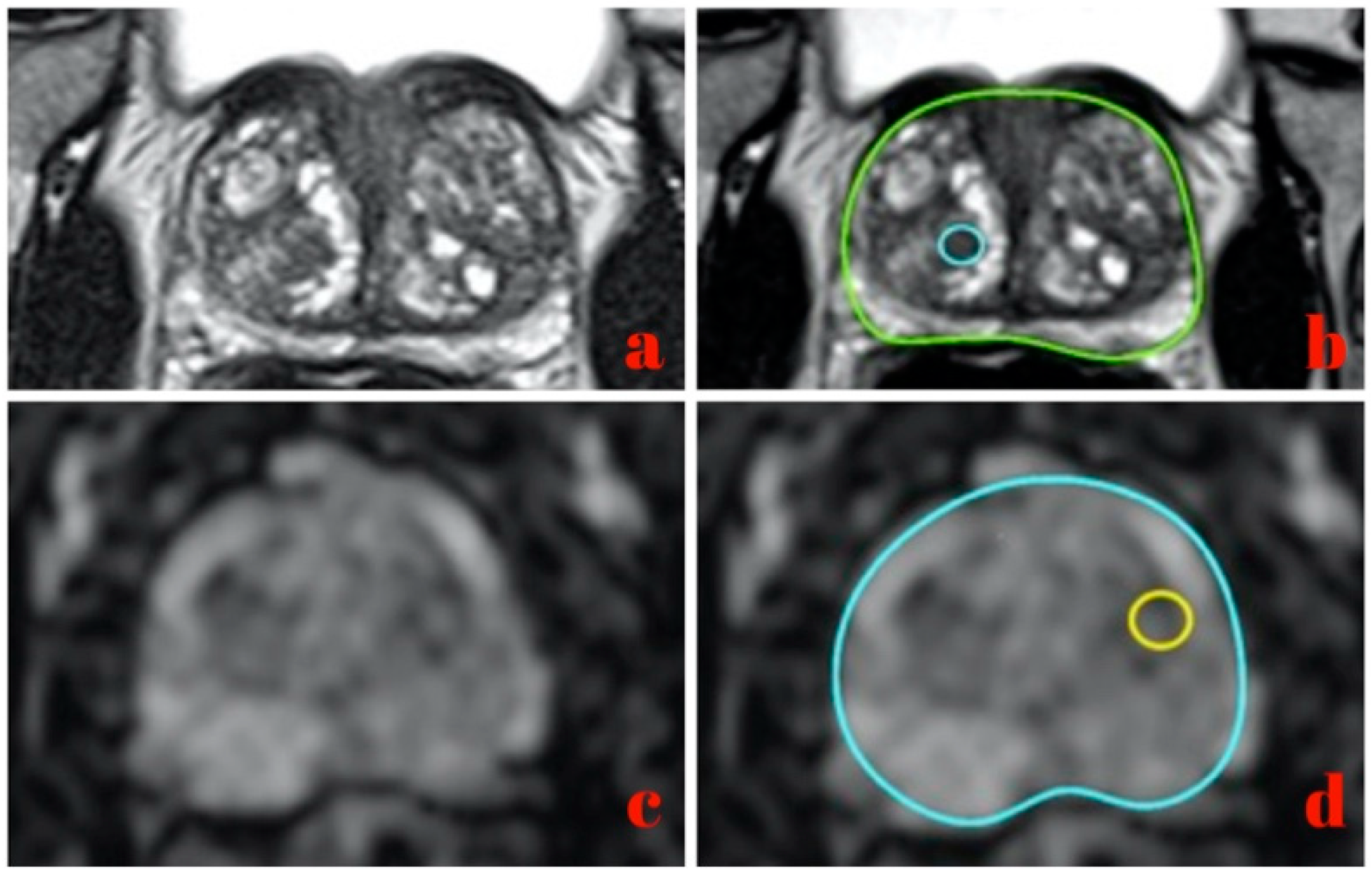
2.2. MRI Image Acquisition and Region of Interest Delineation
- Sagittal T2-weighted turbo spin echo (slice thickness TR 4000.0 ms, 3.0 mm; TE 114.0 ms; Voxel size 0.7 × 0.7 × 3 mm; field of view (FoV) 180 × 180 mm; nex 2; concatenation 2);
- Coronal T2-weighted turbo spin echo (slice thickness TR 4400.0 ms, 3.0 mm; TE 114.0 ms; voxel size 0.7 × 0.7 × 3 mm; field of view (FoV) 180 × 180 mm; nex 2; concatenation 2);
- Axial T2- weighted turbo spin echo (lice thickness TR 4000.0 ms, 3.0 mm; TE 114.0 ms; voxel size 0.7 × 0.7 × 3 mm; field of view (FoV) 180 × 180 mm; nex 2; concatenation 2);
- Axial T1-weighted turbo spin echo (slice thickness TR 568.0 ms, 3.0 mm; TE 11.0 ms; voxel size 0.8 × 0.8 × 3 mm; field of view (FoV) 200 × 200 mm; nex 2; concatenation 2);
- Axial T2-weighted spectral attenuated inversion recovery (slice thickness TR 5310.0 ms, 3.0 mm; TE 95.0 ms; voxel size 0.8 × 0.8 × 3 mm; field of view (FoV) 200 × 200 mm; nex 2; concatenation 2);
- Axial single-shot echo-planar (SSEP) diffusion-weighted sequence with diffusion-sensitizing gradient applied along the x, y, z axes and with a b value of 50, 500, 800 and 1000 s/mm2 (slice thickness TR 4300.0 ms, 4.0 mm; TE 73.0 ms; voxel size 0.9 × 0.9 × 0.9 mm; field of view (FoV) 240 × 240 mm; concatenation 1);
- Axial T1-weighted dynamic volumetric interpolated breath-hold examination (VIBE) fat suppressed sequence (slice thickness TR 4.46 ms, 4.0 mm; TE 1.63 ms; voxel size 1.2 × 1.2 × 4 mm; field of view (FoV) 260 × 260 mm; nex 1; concatenation 1). The contrast agent, gadobenate-dimeglumine (Multihance®, Bracco Imaging, Milan, Italy), was administered in a concentration of 0.2 mmol/kg; it was injected with an automatic injector through a 20 G intravenous cannula at the rate of 4 mL/s, followed by the infusion of 15 mL of saline solution at the same speed. The contrast agent and the sequence started simultaneously to assess the perfusion of the organ. The sequence was acquired once before and 18 times after the contrast injection (echo trains) for a total duration of 3.7 ± 0.5 min. Subtracted images were automatically derived from DCE-MRI.
- Axial T1-weighted VIBE fat suppressed sequence (slice thickness TR 4.76 ms, 2.0 mm; TE 1.82 ms; oxel size 1 × 1 × 1 mm; field of fiew (FoV) 200 × 200 mm; nex 2; concatenation 1).
2.3. Fusion Biopsy and Pathological Examination
2.4. Local Binary Pattern Features of Three Orthogonal Planes
2.5. 3D Gray Level Co-Occurrence Matrix Features
2.6. Quantitative Analysis and Features Selection
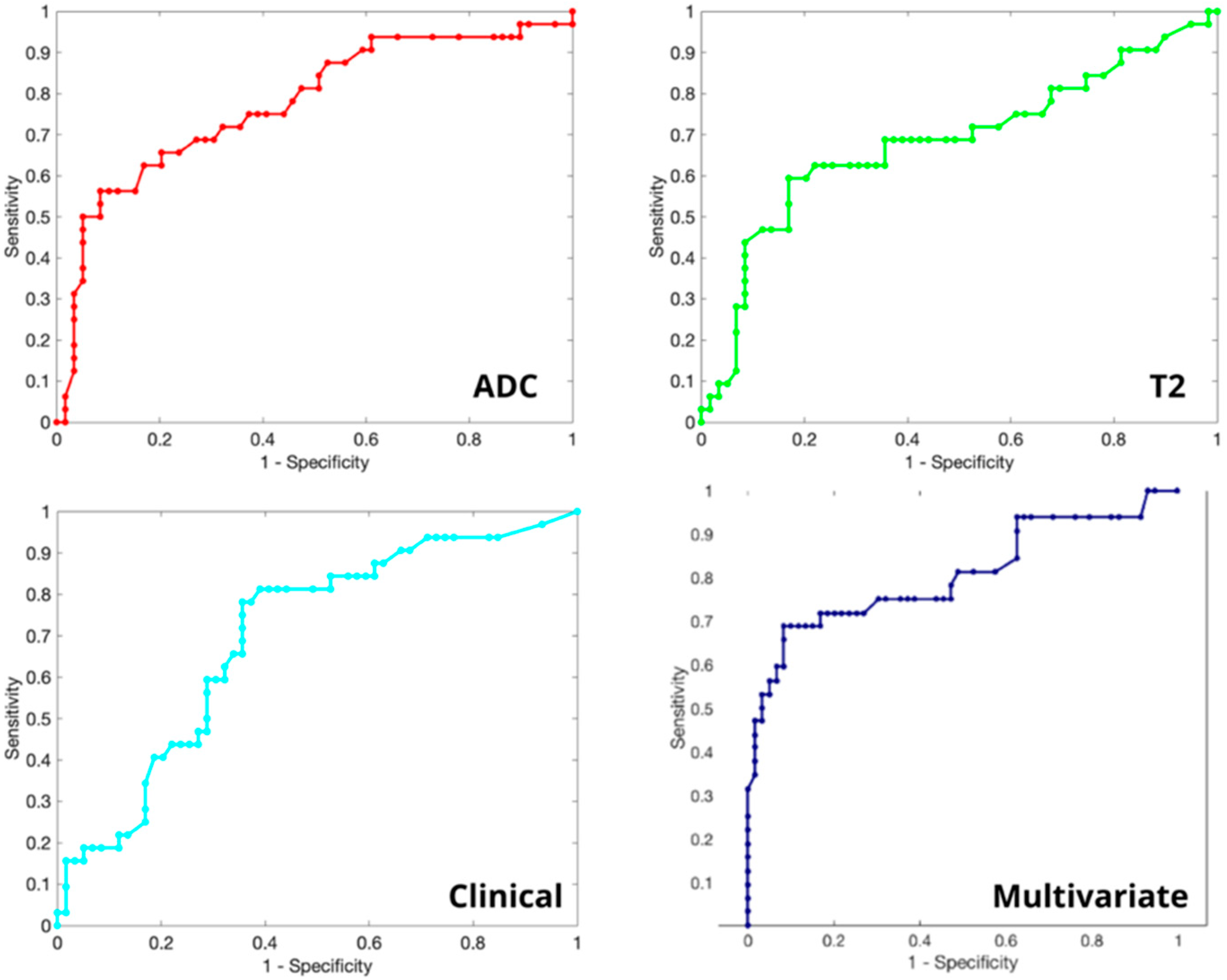
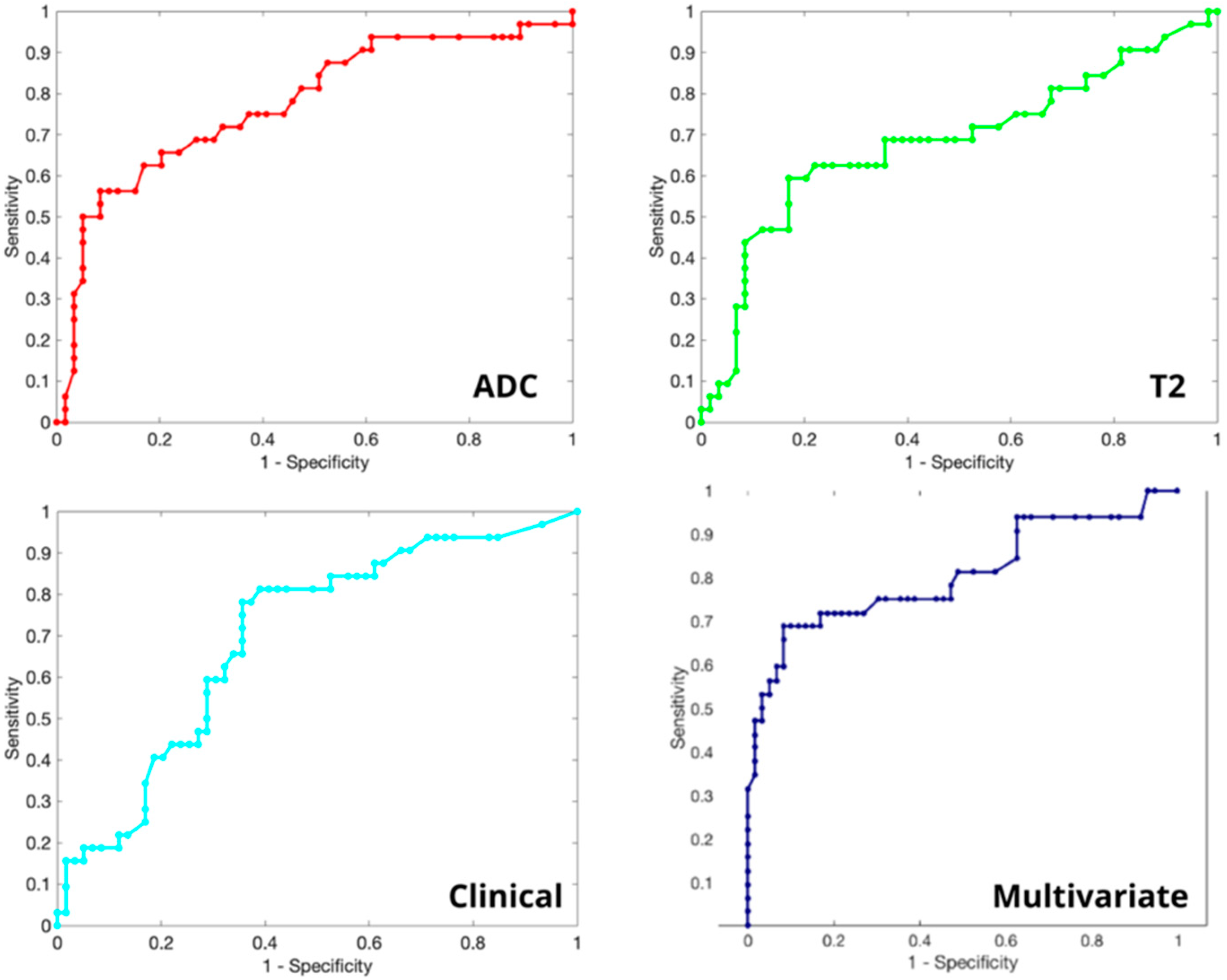
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mottet, N.; van den Bergh, R.C.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer-2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2021, 79, 243–262. [Google Scholar] [CrossRef] [PubMed]
- Thompson, I.M.; Pauler, D.K.; Goodman, P.J.; Tangen, C.M.; Lucia, M.S.; Parnes, H.L.; Minasian, L.M.; Ford, L.G.; Lippman, S.M.; Crawford, E.D.; et al. Prevalence of prostate cancer among men with a prostate-specific antigen level. N. Engl. J. Med. 2004, 350, 2239–2246. [Google Scholar] [CrossRef]
- Chou, R.; Croswell, J.M.; Dana, T.; Bougatsos, C.; Blazina, I.; Fu, R.; Gleitsmann, K.; Koenig, H.C.; Lam, C.; Maltz, A.; et al. Screening for prostate cancer: A review of the evidence for the U.S. Preventive Services Task Force. Ann. Intern. Med. 2011, 155, 762–771. [Google Scholar] [CrossRef]
- Turkbey, B.; Rosenkrantz, A.B.; Haider, M.A.; Padhani, A.R.; Villeirs, G.; Macura, K.J.; Tempany, C.M.; Choyke, P.L.; Cornud, F.; Margolis, D.J.; et al. Prostate Imaging Reporting and Data System Version 2.1: 2019 Update of Prostate Imaging Reporting and Data System Version 2. Eur. Urol. 2019, 76, 340–351. [Google Scholar] [CrossRef] [PubMed]
- Yakar, D.; Debats, O.A.; Bomers, J.G.; Schouten, M.G.; Vos, P.C.; van Lin, E.; Fütterer, J.J.; Barentsz, J.O. Predictive value of MRI in the localization, staging, volume estimation, assessment of aggressiveness, and guidance of radiotherapy and biopsies in prostate cancer. J. Magn. Reson. Imaging 2011, 35, 20–31. [Google Scholar] [CrossRef] [PubMed]
- Chesnais, A.; Niaf, E.; Bratan, F.; Mège-Lechevallier, F.; Roche, S.; Rabilloud, M.; Colombel, M.; Rouvière, O. Differentiation of transitional zone prostate cancer from benign hyperplasia nodules: Evaluation of discriminant criteria at multiparametric MRI. Clin. Radiol. 2013, 68, e323–e330. [Google Scholar] [CrossRef] [PubMed]
- Rosenkrantz, A.B.; Ginocchio, L.; Cornfeld, D.; Froemming, A.T.; Gupta, R.T.; Turkbey, B.; Westphalen, A.C.; Babb, J.; Margolis, D.J. Interobserver Reproducibility of the PI-RADS Version 2 Lexicon: A Multicenter Study of Six Experienced Prostate Radiologists. Radiology 2016, 280, 793–804. [Google Scholar] [CrossRef] [PubMed]
- Matoso, A.; Epstein, J.I. Defining clinically significant prostate cancer on the basis of pathological findings. Histopathology 2019, 74, 135–145. [Google Scholar] [CrossRef]
- Wang, J.; Wu, C.J.; Bao, M.L.; Zhang, J.; Wang, X.N.; Zhang, Y.D. Machine learning-based analysis of MR radiomics can help to improve the diagnostic performance of PI-RADS v2 in clinically relevant prostate cancer. Eur. Radiol. 2017, 27, 4082–4090. [Google Scholar] [CrossRef]
- Neri, P.; Heeger, D.J. Spatiotemporal mechanisms for detecting and identifying image features in human vision. Nat. Neurosci. 2002, 5, 812–816. [Google Scholar] [CrossRef]
- Cordelli, E.; Maulucci, G.; de Spirito, M.; Rizzi, A.; Pitocco, D.; Soda, P. A decision support system for type 1 diabetes mellitus diagnostics based on dual channel analysis of red blood cell membrane fluidity. Comput. Methods Programs Biomed. 2018, 162, 263–271. [Google Scholar] [CrossRef]
- Ramella, S.; Fiore, M.; Greco, C.; Cordelli, E.; Sicilia, R.; Merone, M.; Molfese, E.; Miele, M.; Cornacchione, P.; Ippolito, E.; et al. A radiomic approach for adaptive radiotherapy in non-small cell lung cancer patients. PLoS ONE 2018, 13, e0207455. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, N.C.; Sicilia, R.; Cordelli, E.; Valbusa, G.; Grossi, E.; Zanetti, I.B.; Fazzini, D.; Scotti, G.; Beltramo, G.; Iannello, G.; et al. Early radiomics experiences in predicting CyberKnife response in acoustic neuroma. ACM SIGBioinformatics Rec. 2019, 8, 11–13. [Google Scholar] [CrossRef]
- Zhao, G.; Pietikäinen, M. Dynamic texture recognition using local binary patterns with an application to facial expressions. IEEE Trans. Pattern Anal. Mach. Intell. 2007, 29, 915–928. [Google Scholar] [CrossRef] [PubMed]
- Ojala, T.; Pietikäinen, M.; Mäenpää, T. Multiresolution gray-scale and rotation invariant texture classification with local binary patterns. IEEE Trans. Pattern Anal. Mach. Intell. 2002, 24, 971–987. [Google Scholar] [CrossRef]
- Sebastian, V.B.; Unnikrishnan, A.; Balakrishnan, K. Grey Level Co-Occurrence Matrices: Generalisation and Some New Features. Int. J. Comput. Sci. Eng. Inf. Technol. 2012, 2, 151–157. [Google Scholar]
- Sicilia, R.; Cordelli, E.; Merone, M.; Luperto, E.; Papalia, R.; Iannello, G.; Soda, P. Early radiomic experiences in classifying prostate cancer aggressiveness using 3D local binary patterns. In Proceedings of the 2019 IEEE 32nd International Symposium on Computer-Based Medical Systems (CBMS), Cordaoba, Spain, 5–7 June 2019; pp. 355–360. [Google Scholar]
- Ayer, T.; Chhatwal, J.; Alagoz, O.; Kahn, C.E., Jr.; Woods, R.W.; Burnside, E.S. Informatics in radiology: Comparison of logistic regression and artificial neural network models in breast cancer risk estimation. Radiographics 2010, 30, 13–22. [Google Scholar] [CrossRef]
- Xu, L.; Yan, P.; Chang, T. Best first strategy for feature selection. In Proceedings of the 9th International Conference on Pattern Recognition, Rome, Italy, 14 May–17 November 1988; IEEE Computer Society: Los Alamitos, CA, USA, 1988; pp. 706–708. [Google Scholar]
- Bradley, A.P. The use of the area under the ROC curve in the evaluation of machine learning algorithms. Pattern Recognit. Pergamon 1997, 30, 1145–1159. [Google Scholar] [CrossRef]
- Srivastava, S.; Koay, E.J.; Borowsky, A.D.; De Marzo, A.M.; Ghosh, S.; Wagner, P.D.; Kramer, B.S. Cancer overdiagnosis: A biological challenge and clinical dilemma. Nat. Rev. Cancer 2019, 19, 349–358. [Google Scholar] [CrossRef]
- Wibmer, A.; Hricak, H.; Gondo, T.; Matsumoto, K.; Veeraraghavan, H.; Fehr, D.; Zheng, J.; Goldman, D.; Moskowitz, C.; Fine, S.W.; et al. Haralick texture analysis of prostate MRI: Utility for differentiating non-cancerous prostate from prostate cancer and differentiating prostate cancers with different Gleason scores. Eur. Radiol. 2015, 25, 2840–2850. [Google Scholar] [CrossRef]
- Vignati, A.; Mazzetti, S.; Giannini, V.; Russo, F.; Bollito, E.; Porpiglia, F.; Stasi, M.; Regge, D. Texture features on T2-weighted magnetic resonance imaging: New potential biomarkers for prostate cancer aggressiveness. Phys. Med. Biol. 2015, 60, 2685–2701. [Google Scholar] [CrossRef] [PubMed]
- Hegde, J.V.; Mulkern, R.V.; Panych, L.P.; Fennessy, F.M.; Fedorov, A.; Maier, S.E.; Tempany, C.M. Multiparametric MRI of prostate cancer: An update on state-of-the-art techniques and their performance in detecting and localizing prostate cancer. J. Magn. Reson. Imaging 2013, 37, 1035–1054. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, A.; Watson, G.; Myint, E.; Sved, P.; McEntee, M.; Bourne, R. Changes in Epithelium, Stroma, and Lumen Space Correlate More Strongly with Gleason Pattern and Are Stronger Predictors of Prostate ADC Changes than Cellularity Metrics. Radiology 2015, 277, 751–762. [Google Scholar] [CrossRef] [PubMed]
- Rozenberg, R.; Thornhill, R.E.; Flood, T.A.; Hakim, S.W.; Lim, C.; Schieda, N. Whole-Tumor Quantitative Apparent Diffusion Coefficient Histogram and Texture Analysis to Predict Gleason Score Upgrading in Intermediate-Risk 3 + 4 = 7 Prostate Cancer. Am. J. Roentgenol. 2016, 206, 775–782. [Google Scholar] [CrossRef] [PubMed]
- Sung, Y.S.; Kwon, H.-J.; Park, B.-W.; Cho, G.; Lee, C.K.; Cho, K.-S.; Kim, J.K. Prostate cancer detection on dynamic contrast-enhanced MRI: Computer-aided diagnosis versus single perfusion parameter maps. Am. J. Roentgenol. 2011, 197, 1122–1129. [Google Scholar] [CrossRef]
- Chaddad, A.; Kucharczyk, M.J.; Niazi, T. Multimodal Radiomic Features for the Predicting Gleason Score of Prostate Cancer. Cancers 2018, 10, 249. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Zhang, J.; Tang, M.; Lei, X.Y.; Li, L.C. MRI-Based Radiomics Nomogram for Predicting Prostate Cancer with Gray-Zone Prostate-Specific Antigen Levels to Reduce Unnecessary Biopsies. Diagnostics 2022, 12, 3005. [Google Scholar] [CrossRef]
- Li, T.; Sun, L.; Li, Q.; Luo, X.; Luo, M.; Xie, H.; Wang, P. Development and Validation of a Radiomics Nomogram for Predicting Clinically Significant Prostate Cancer in PI-RADS 3 Lesions. Frontl. Oncol. 2022, 11, 825429. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Number of Patients | 91 |
|---|---|
| Age, median (IQR) (years) | 67 (12) |
| PSA (mean ± SD) (ng/mL) | 8.59 (±6.29) |
| PSA density (mean ± SD) (ng/mL/cc) | 0.163 (±0.134) |
| Prostate volume (mean ± SD) (mL) | 63.3 (±27.7) |
| PI-RADS 3 | 45 |
| PI-RADS 4 | 27 |
| PI-RADS 5 | 19 |
| Total target cores | 279 |
| Total random cores | 1092 |
| Target cores, median (IQR) | 3 (1) |
| Positive biopsies | 9 (65%) |
| CS PCa | 39 (43%) |
| NCS PCa CS PCa PI-RADS 3 CS PCa PI-RADS 4 CS PCa PI-RADS 5 | 20 (22%) 5 (12.8%) 11 (28.2%) 23 (59%) |
| GS 3 + 3 | 20 (22%) |
| GS 3 + 4 | 17 (19%) |
| GS 4 + 3 | 10 (11%) |
| GS 4 + 4 | 9 (10%) |
| GS 4 + 5 | 2 (2%) |
| GS 5 + 4 | 1 (1%) |
| Negative (non-cancerous) biopsies | 32 (35%) |
| Univariate AUC | Feature Name | Feature Description |
|---|---|---|
| 0.659 | DRE | digital rectal exploration |
| 0.675 | PIRADSmax | Maximum PI-RADS value assigned to the tissue’s sample |
| 0.563 | T2 Histogram—kurtosis | The amount of voxels in T2w acquisition that differs >2 standard deviations from its average value |
| 0.426 | T2 Histogram—number of maximum relatives | The number of relative maximums in the gray level distribution of a T2w acquisition |
| 0.426 | T2 Histogram—energy around maximum relatives | The homogeneity of the pattern around the relative maximums of a T2w acquisition |
| 0.469 | T2 Range—TOP-LBP rotation invariant | The difference between the higher and the lower value of the LBP transformation in a T2 acquisition (without considering their rotation) |
| 0.461 | ADC Histogram—skewness | The asymmetry in the gray level distribution of an ADC acquisition |
| 0.469 | ADC Range—TOP-LBP uniform rotation invariant | The difference between the higher and the lower value of the LBP transformation in an ADC acquisition without considering their rotation and noisy patterns |
| 0.452 | ADC Histogram—TOP-LBP uniform rotation invariant | The number of relative maximums in the distribution of the LBP transformation in an ADC acquisition not considering their rotation and noisy patterns |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prata, F.; Anceschi, U.; Cordelli, E.; Faiella, E.; Civitella, A.; Tuzzolo, P.; Iannuzzi, A.; Ragusa, A.; Esperto, F.; Prata, S.M.; et al. Radiomic Machine-Learning Analysis of Multiparametric Magnetic Resonance Imaging in the Diagnosis of Clinically Significant Prostate Cancer: New Combination of Textural and Clinical Features. Curr. Oncol. 2023, 30, 2021-2031. https://doi.org/10.3390/curroncol30020157
Prata F, Anceschi U, Cordelli E, Faiella E, Civitella A, Tuzzolo P, Iannuzzi A, Ragusa A, Esperto F, Prata SM, et al. Radiomic Machine-Learning Analysis of Multiparametric Magnetic Resonance Imaging in the Diagnosis of Clinically Significant Prostate Cancer: New Combination of Textural and Clinical Features. Current Oncology. 2023; 30(2):2021-2031. https://doi.org/10.3390/curroncol30020157
Chicago/Turabian StylePrata, Francesco, Umberto Anceschi, Ermanno Cordelli, Eliodoro Faiella, Angelo Civitella, Piergiorgio Tuzzolo, Andrea Iannuzzi, Alberto Ragusa, Francesco Esperto, Salvatore Mario Prata, and et al. 2023. "Radiomic Machine-Learning Analysis of Multiparametric Magnetic Resonance Imaging in the Diagnosis of Clinically Significant Prostate Cancer: New Combination of Textural and Clinical Features" Current Oncology 30, no. 2: 2021-2031. https://doi.org/10.3390/curroncol30020157
APA StylePrata, F., Anceschi, U., Cordelli, E., Faiella, E., Civitella, A., Tuzzolo, P., Iannuzzi, A., Ragusa, A., Esperto, F., Prata, S. M., Sicilia, R., Muto, G., Grasso, R. F., Scarpa, R. M., Soda, P., Simone, G., & Papalia, R. (2023). Radiomic Machine-Learning Analysis of Multiparametric Magnetic Resonance Imaging in the Diagnosis of Clinically Significant Prostate Cancer: New Combination of Textural and Clinical Features. Current Oncology, 30(2), 2021-2031. https://doi.org/10.3390/curroncol30020157