Risk Factors for Nodal Failure in Patients with FIGO IIIC Cervical Cancer Receiving Definitive Image-Guided Radiotherapy


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Collection
- 1.
- Biopsy-proven cervical cancer;
- 2.
- Imaging confirmed pelvic or para-aortic lymph node metastasis (FIGO 2018 IIIC);
- 3.
- Complete information on positive lymph nodes, including information before treatment and during follow-up:
- (1)
- For patients with pelvic LNM (PLNM), pelvic MRIs before and one month after treatment were required;
- (2)
- For patients with para-aortic LNM (PALNM), abdominal CTs before and one month after treatment were required;
- 4.
- Follow-up period exceeding six months;
- 5.
- No evidence of distant metastasis (DM) before the treatment;
- 6.
- Treatment with definitive radiotherapy.
2.2. Radiotherapy
2.3. Chemotherapy
2.4. Lymph Node Characteristics
2.5. Statistics
3. Results
3.1. Patients’ Characteristics
3.2. Lymph Node Characteristics
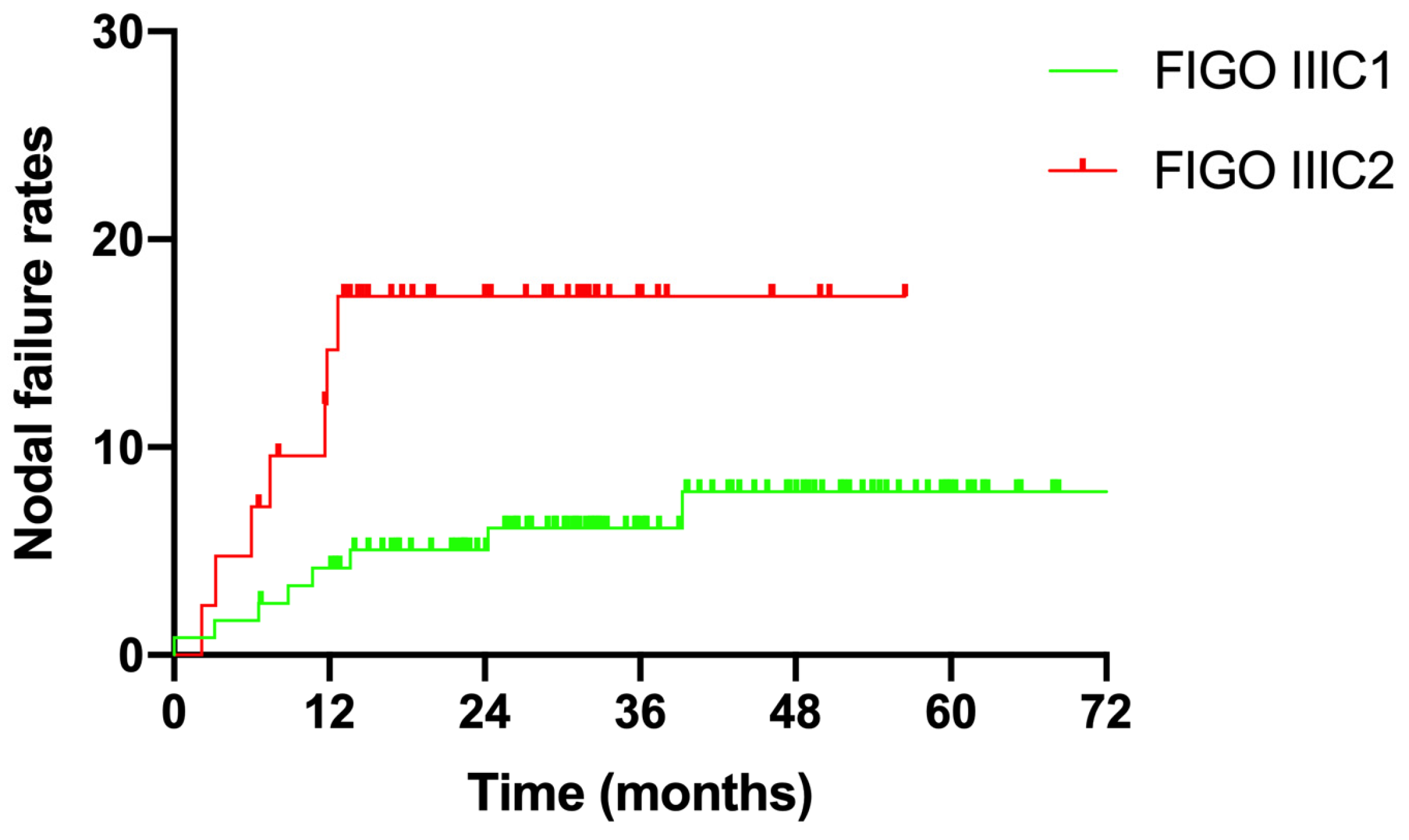
3.3. Nodal Failure
3.4. Risk Factors for Nodal Failure
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stehman, F.B.; Bundy, B.N.; DiSaia, P.J.; Keys, H.M.; Larson, J.E.; Fowler, W.C. Carcinoma of the cervix treated with radiation therapy. I. A multi-variate analysis of prognostic variables in the Gynecologic Oncology Group. Cancer 1991, 67, 2776–2785. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Wei, L.C.; Zhang, Y.; Zhao, L.N.; Li, W.W.; Ping, L.J.; Dang, Y.Z.; Hu, J.; Shi, M. The Prognosis and Risk Stratification Based on Pelvic Lymph Node Characteristics in Patients With Locally Advanced Cervical Squamous Cell Carcinoma Treated With Concurrent Chemoradiotherapy. Int. J. Gynecol. Cancer 2016, 26, 1472–1479. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Zhang, F.; Hu, K.; Hou, X. Image-guided, intensity-modulated radiation therapy in definitive radiotherapy for 1433 patients with cervical cancer. Gynecol. Oncol. 2018, 151, 444–448. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Wang, W.; Meng, Q.; Zhang, F.; Hu, K. Extended-field intensity-modulated radiation therapy combined with concurrent chemotherapy for cervical cancer with para-aortic lymph nodes metastasis. Jpn. J. Clin. Oncol. 2019, 49, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Nomden, C.N.; Potter, R.; de Leeuw, A.A.C.; Tanderup, K.; Lindegaard, J.C.; Schmid, M.P.; Fortin, I.; Haie-Meder, C.; Mahantshetty, U.; Hoskin, P.; et al. Nodal failure after chemo-radiation and MRI guided brachytherapy in cervical cancer: Patterns of failure in the EMBRACE study cohort. Radiother. Oncol. 2019, 134, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Bacorro, W.; Dumas, I.; Escande, A.; Gouy, S.; Bentivegna, E.; Morice, P.; Haie-Meder, C.; Chargari, C. Dose-volume effects in pathologic lymph nodes in locally advanced cervical cancer. Gynecol. Oncol. 2018, 148, 461–467. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J.; Kim, J.Y.; Yoo, S.H.; Min, B.J.; Chung, K.Z.; Seo, S.S.; Kang, S.B.; Lim, M.C.; Hwang, J.H.; Yoo, H.J.; et al. High control rate for lymph nodes in cervical cancer treated with high-dose radiotherapy using helical tomotherapy. Technol. Cancer Res. Treat. 2013, 12, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Rash, D.L.; Lee, Y.C.; Kashefi, A.; Durbin-Johnson, B.; Mathai, M.; Valicenti, R.; Mayadev, J.S. Clinical response of pelvic and para-aortic lymphadenopathy to a radiation boost in the definitive management of locally advanced cervical cancer. Int. J. Radiat. Oncol. Biol. Phys. 2013, 87, 317–322. [Google Scholar] [CrossRef] [PubMed]
- Wakatsuki, M.; Ohno, T.; Kato, S.; Ando, K.; Noda, S.E.; Kiyohara, H.; Shibuya, K.; Karasawa, K.; Kamada, T.; Nakano, T. Impact of boost irradiation on pelvic lymph node control in patients with cervical cancer. J. Radiat. Res. 2014, 55, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Schernberg, A.; Bockel, S.; Annede, P.; Fumagalli, I.; Escande, A.; Mignot, F.; Kissel, M.; Morice, P.; Bentivegna, E.; Gouy, S.; et al. Tumor Shrinkage During Chemoradiation in Locally Advanced Cervical Cancer Patients: Prognostic Significance, and Impact for Image-Guided Adaptive Brachytherapy. Int. J. Radiat. Oncol. Biol. Phys. 2018, 102, 362–372. [Google Scholar] [CrossRef] [PubMed]
- Song, S.; Kim, J.Y.; Kim, Y.J.; Yoo, H.J.; Kim, S.H.; Kim, S.K.; Lim, M.C.; Kang, S.; Seo, S.S.; Park, S.Y. The size of the metastatic lymph node is an independent prognostic factor for the patients with cervical cancer treated by definitive radiotherapy. Radiother. Oncol. 2013, 108, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Schmid, M.P.; Franckena, M.; Kirchheiner, K.; Sturdza, A.; Georg, P.; Dorr, W.; Potter, R. Distant metastasis in patients with cervical cancer after primary radiotherapy with or without chemotherapy and image guided adaptive brachytherapy. Gynecol. Oncol. 2014, 133, 256–262. [Google Scholar] [CrossRef] [PubMed]
- Meng, Q.; Liu, X.; Hu, K.; Hou, X.; Zhang, F.; Wang, W.; Yan, J.; Yang, B.; Li, W. Image-guided intensity-modulated radiotherapy in patients with FIGO IIIC1 cervical cancer: Efficacy, toxicity and prognosis. J. Cancer 2023, 13, 1003–1010. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, K.; Shimada, M.; Aoki, Y.; Sakamoto, M.; Takeshima, N.; Fujiwara, H.; Matsumoto, T.; Mikami, M.; Sugiyama, T. Comparison of adjuvant therapy for node-positive clinical stage IB-IIB cervical cancer: Systemic chemotherapy versus pelvic irradiation. Int. J. Cancer 2017, 141, 1042–1051. [Google Scholar] [CrossRef] [PubMed]
- Verma, J.; Sulman, E.P.; Jhingran, A.; Tucker, S.L.; Rauch, G.M.; Eifel, P.J.; Klopp, A.H. Dosimetric predictors of duodenal toxicity after intensity modulated radiation therapy for treatment of the para-aortic nodes in gynecologic cancer. Int. J. Radiat. Oncol. Biol. Phys. 2014, 88, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Kelly, P.; Das, P.; Pinnix, C.C.; Beddar, S.; Briere, T.; Pham, M.; Krishnan, S.; Delclos, M.E.; Crane, C.H. Duodenal toxicity after fractionated chemoradiation for unresectable pancreatic cancer. Int. J. Radiat. Oncol. Biol. Phys. 2013, 85, e143–e149. [Google Scholar] [CrossRef] [PubMed]
- Bacorro, W.; Dumas, I.; Levy, A.; Rivin Del Campo, E.; Canova, C.H.; Felefly, T.; Huertas, A.; Marsolat, F.; Haie-Meder, C.; Chargari, C.; et al. Contribution of image-guided adaptive brachytherapy to pelvic nodes treatment in locally advanced cervical cancer. Brachytherapy 2017, 16, 366–372. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Characteristics | Cut-Off Value | Sensitivity | Specificity | AUC 95%CI | p Value |
|---|---|---|---|---|---|
| Dpre | 1.15 cm | 79.4% | 41.9% | 0.65 (0.55–0.74) | 0.005 |
| Vpre | 2.85 cm3 | 82.4% | 51.8% | 0.70 (0.60–0.80) | <0.001 |
| D20F | 0.95 cm | 88.2% | 64.4% | 0.78 (0.70–0.86) | <0.001 |
| V20F | 3.45 cm3 | 64.7% | 82.3% | 0.79 (0.72–0.87) | <0.001 |
| ΔD20F | 0.245 | 76.5% | 75.4% | 0.78 (0.68–0.88) | <0.001 |
| ΔV20F | 0.435 | 76.5% | 75.2% | 0.77 (0.67–0.87) | <0.001 |
| Characteristics | N. (%) |
|---|---|
| Age | |
| Median: 50.5 years (26–73 years) | |
| Histology | |
| Squamous cell carcinoma | 150 (92.6%) |
| Adenocarcinoma | 7 (4.3%) |
| Adenosquamous carcinoma | 3 (1.9%) |
| Others | 2 (1.2%) |
| Lymph node metastasis | |
| PLNM only | 120 (74.1%) |
| PALNM only | 4 (2.5%) |
| PLN + PALNM | 38 (23.4%) |
| FIGO stage (2018) | |
| IIIC1 | 120 (74.1%) |
| IIIC2 | 42 (25.9%) |
| Radiation dose of LNM | |
| Median: 60.2 Gy | |
| ≥60 Gy | 121 (74.7%) |
| <60 Gy | 41 (25.3%) |
| Cycles of concurrent chemotherapy | |
| 0 | 8 (4.9%) |
| 1–3 | 17 (10.5%) |
| ≥4 | 137 (84.6%) |
| Total | 162 (100%) |
| Characteristics | N. (%) |
|---|---|
| Distribution | |
| Positive pelvic LN | 307 (83.4%) |
| Common iliac region | 46 (15.0%) |
| External iliac region | 201 (65.5%) |
| Internal iliac region | 18 (5.8%) |
| Obturator region | 38 (12.4%) |
| Presacral region | 1 (0.3%) |
| Perirectal region | 3 (1.0%) |
| Positive para-aortic LN | 61 (16.6%) |
| LPA | 41 (67.2%) |
| AC | 19 (31.2%) |
| RPC | 1 (1.6%) |
| Dpre (cm) | |
| Median 1.2 (1.0–3.4) | |
| <1.15 | 147 (39.9%) |
| ≥1.15 | 221 (60.1%) |
| Vpre (cm3) | |
| Median 3.0 (1.0–54.1) | |
| <2.85 | 179 (48.6%) |
| ≥2.85 | 189 (51.4%) |
| D20F (cm) | |
| Median 0.8 (0.2–2.7) | |
| <0.95 | 219 (59.5%) |
| ≥0.95 | 149 (40.5%) |
| V20F (cm3) | |
| Median 1.2 (0.1–38.5) | |
| <3.45 | 287 (78.0%) |
| ≥3.45 | 81 (22.0%) |
| ΔD20F | |
| Median 0.36 (−0.67–0.80) | |
| ≥0.245 | 260 (70.7%) |
| <0.245 | 108 (29.3%) |
| ΔV20F | |
| Median 0.61 (−2.03–0.95) | |
| ≥0.435 | 259 (70.4%) |
| <0.435 | 109 (29.6%) |
| Radiation dose (95% PGTVnd) | |
| 56 Gy/28 F | 17 (4.6%) |
| 59.36 Gy/28 F | 49 (13.3%) |
| 59.92 Gy/28 F | 20 (5.5%) |
| 60.2 Gy/28 F | 276 (75.0%) |
| 66.2 Gy/31 F | 6 (1.6%) |
| Total | 368 (100%) |
| Risk Factors | Nodal Failure Rate | Univariate Analysis (χ2 Test) | Multivariate Analysis (Logistic Test) | |
|---|---|---|---|---|
| p Value | HR (95%CI) | p Value | ||
| Dpre (cm) | ||||
| ≥1.15 vs. <1.15 | 12.2% vs. 4.8% | 0.016 | — | — |
| Vpre (cm3) | ||||
| ≥2.85 vs. <2.85 | 14.8% vs. 3.4% | <0.001 | — | — |
| D20F (cm) | ||||
| ≥0.95 vs. <0.95 | 20.1% vs. 1.8% | <0.001 | 6.855 (1.402–33.518) | 0.017 |
| V20F (cm3) | ||||
| ≥3.45 vs. <3.45 | 27.2% vs. 4.2% | <0.001 | — | — |
| ΔD20F | ||||
| <0.245 vs. ≥0.245 | 24.1% vs. 3.1% | <0.001 | — | — |
| ΔV20F | ||||
| <0.435 vs. ≥0.435 | 23.9% vs. 3.1% | <0.001 | 3.069 (1.027–9.170) | 0.045 |
| Histology | ||||
| Non-SCC vs. SCC | 20.0% vs. 8.3% | 0.034 | — | — |
| Radiation dose (Gy) | ||||
| <60 vs. ≥60 | 18.4% vs. 6.4% | 0.001 | — | — |
| Cycles of CT | ||||
| <4 vs. ≥4 | 22.8% vs. 5.5% | <0.001 | 3.635 (1.441–9.166) | 0.006 |
| Distribution of LNs | ||||
| PALNM vs. PLNM | 16.4% vs. 7.8% | 0.035 | — | — |
| Risk Factors | Nodal Failure Rate | Univariate Analysis (χ2 Test) | Multivariate Analysis (Logistic Test) | |
|---|---|---|---|---|
| p Value | HR (95%CI) | p Value | ||
| Dpre (cm) | ||||
| ≥1.15 vs. <1.15 | 10.9% vs. 2.6% | 0.009 | — | — |
| Vpre (cm3) | ||||
| ≥2.85 vs. <2.85 | 13.6% vs. 2.0% | <0.001 | — | — |
| D20F (cm) | ||||
| ≥0.95 vs. <0.95 | 16.2% vs. 2.2% | <0.001 | — | — |
| V20F (cm3) | ||||
| ≥3.45 vs. <3.45 | 23.4% vs. 3.7% | <0.001 | — | — |
| ΔD20F | ||||
| <0.245 vs. ≥0.245 | 21.7% vs. 2.7% | <0.001 | — | — |
| ΔV20F | ||||
| <0.435 vs. ≥0.435 | 21.4% vs. 2.7% | <0.001 | 3.737 (1.009–13.845) | 0.048 |
| Histology | ||||
| Non-SCC vs. SCC | 16.7% vs. 7.1% | 0.093 | — | — |
| Radiation dose (Gy) | ||||
| <60 vs. ≥60 | 12.7% vs. 6.4% | 0.082 | — | — |
| Cycles of CT | ||||
| <4 vs. ≥4 | 20.7% vs. 4.9% | <0.001 | 5.087 (1.897–13.641) | 0.001 |
| Risk Factors | Nodal Failure Rate | Univariate Analysis (χ2 Test) | Multivariate Analysis (Logistic Test) | |
|---|---|---|---|---|
| p Value | HR (95%CI) | p Value | ||
| Dpre (cm) | ||||
| ≥1.15 vs. <1.15 | 20.7% vs. 12.5% | 0.388 | — | — |
| Vpre (cm3) | ||||
| ≥2.85 vs. <2.85 | 20.0% vs. 11.5% | 0.377 | — | — |
| D20F (cm) | ||||
| ≥0.95 vs. <0.95 | 40.0% vs. 0 | <0.001 | — | — |
| V20F (cm3) | ||||
| ≥3.45 vs. <3.45 | 41.2% vs. 6.8% | 0.001 | — | — |
| ΔD20F | ||||
| <0.245 vs. ≥0.245 | 32.0% vs. 5.6% | 0.006 | — | — |
| ΔV20F | ||||
| <0.435 vs. ≥0.435 | 32.0% vs. 5.6% | 0.006 | 11.000 (1.603–75.502) | 0.015 |
| Histology | ||||
| Non-SCC vs. SCC | 33.3% vs. 14.5% | 0.238 | — | — |
| Radiation dose (Gy) | ||||
| <60 vs. ≥60 | 43.8% vs. 6.7% | 0.001 | — | — |
| Cycles of CT | ||||
| <4 vs. ≥4 | 28.6% vs. 10.0% | 0.063 | — | — |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, X.; Hou, X.; Hu, K.; Zhang, F.; Wang, W.; Ren, K. Risk Factors for Nodal Failure in Patients with FIGO IIIC Cervical Cancer Receiving Definitive Image-Guided Radiotherapy. Curr. Oncol. 2023, 30, 10385-10395. https://doi.org/10.3390/curroncol30120756
Liu X, Hou X, Hu K, Zhang F, Wang W, Ren K. Risk Factors for Nodal Failure in Patients with FIGO IIIC Cervical Cancer Receiving Definitive Image-Guided Radiotherapy. Current Oncology. 2023; 30(12):10385-10395. https://doi.org/10.3390/curroncol30120756
Chicago/Turabian StyleLiu, Xiaoliang, Xiaorong Hou, Ke Hu, Fuquan Zhang, Weiping Wang, and Kang Ren. 2023. "Risk Factors for Nodal Failure in Patients with FIGO IIIC Cervical Cancer Receiving Definitive Image-Guided Radiotherapy" Current Oncology 30, no. 12: 10385-10395. https://doi.org/10.3390/curroncol30120756
APA StyleLiu, X., Hou, X., Hu, K., Zhang, F., Wang, W., & Ren, K. (2023). Risk Factors for Nodal Failure in Patients with FIGO IIIC Cervical Cancer Receiving Definitive Image-Guided Radiotherapy. Current Oncology, 30(12), 10385-10395. https://doi.org/10.3390/curroncol30120756