The Effects of Radiotherapy on Pancreatic Ductal Adenocarcinoma in Patients with Liver Metastases


Abstract
1. Introduction
2. Materials and Methods
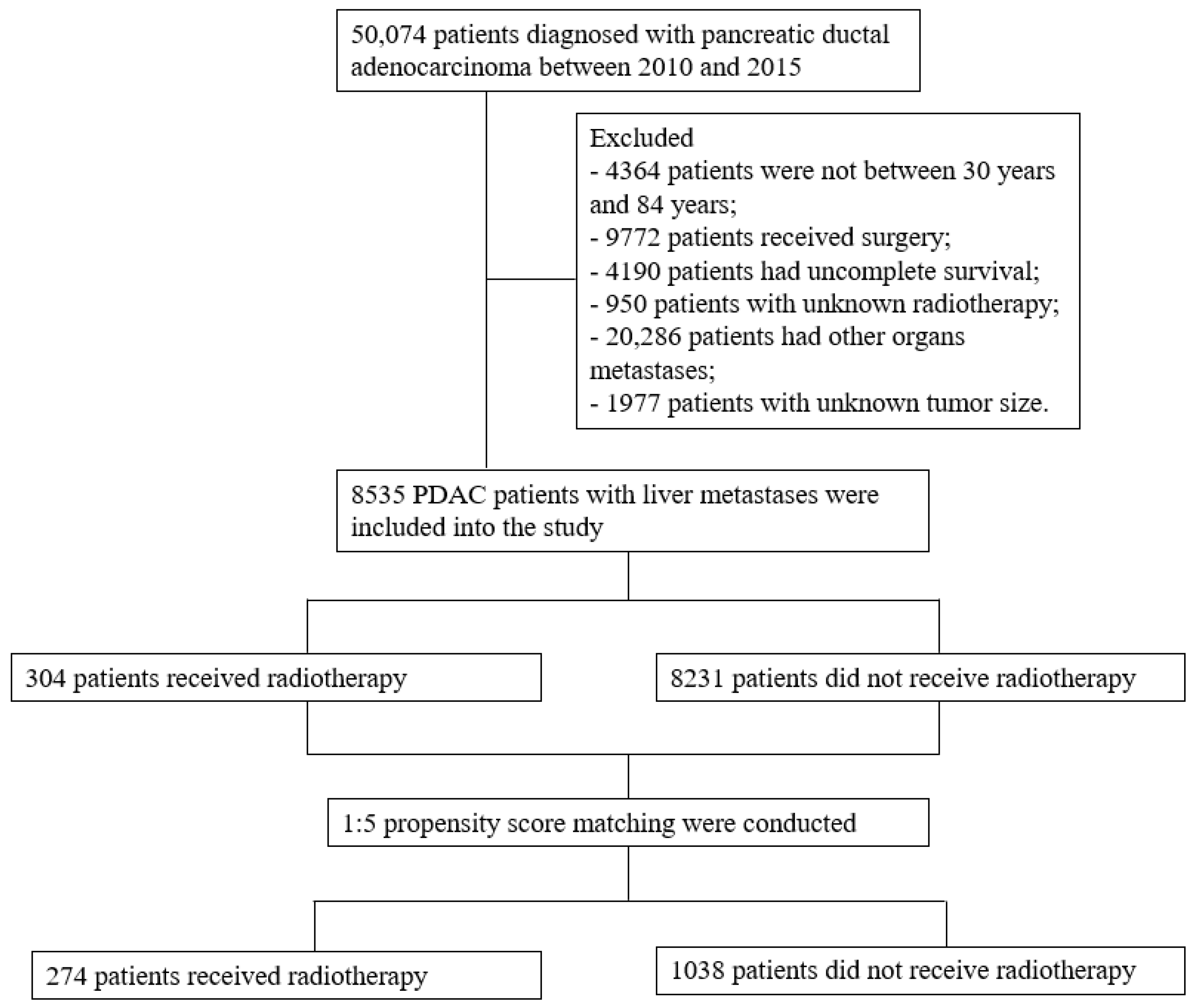
2.1. Patient Selection
2.2. Definition of the Endpoints
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Patients
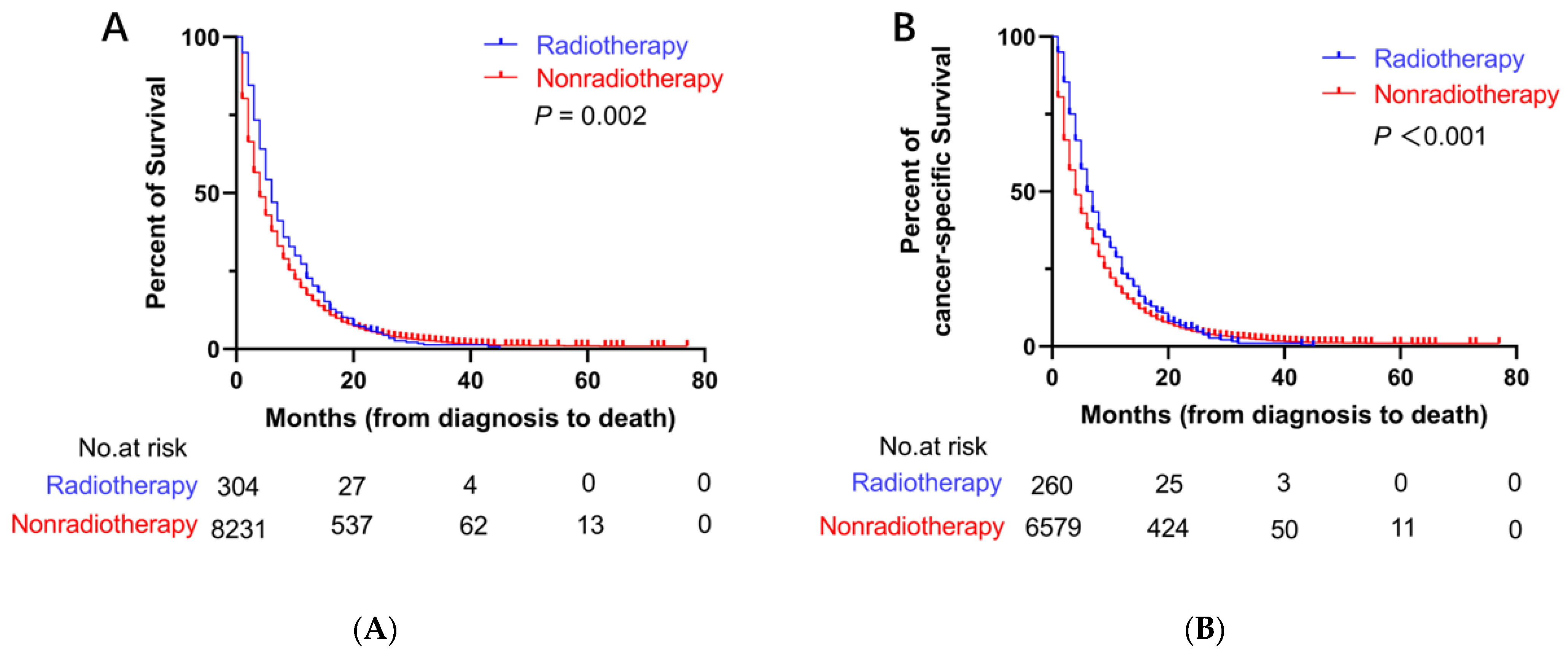
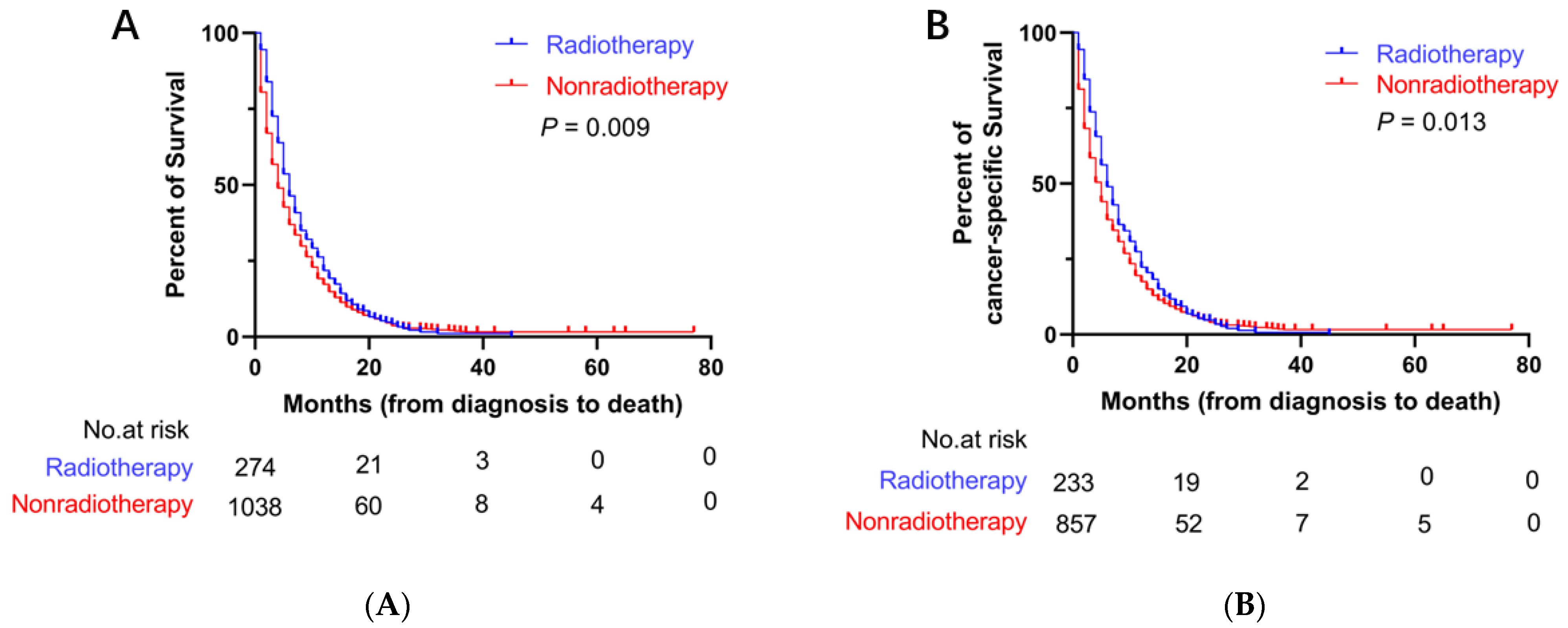
3.2. Survival Outcomes
3.3. Predictors of OS and CSS before PSM
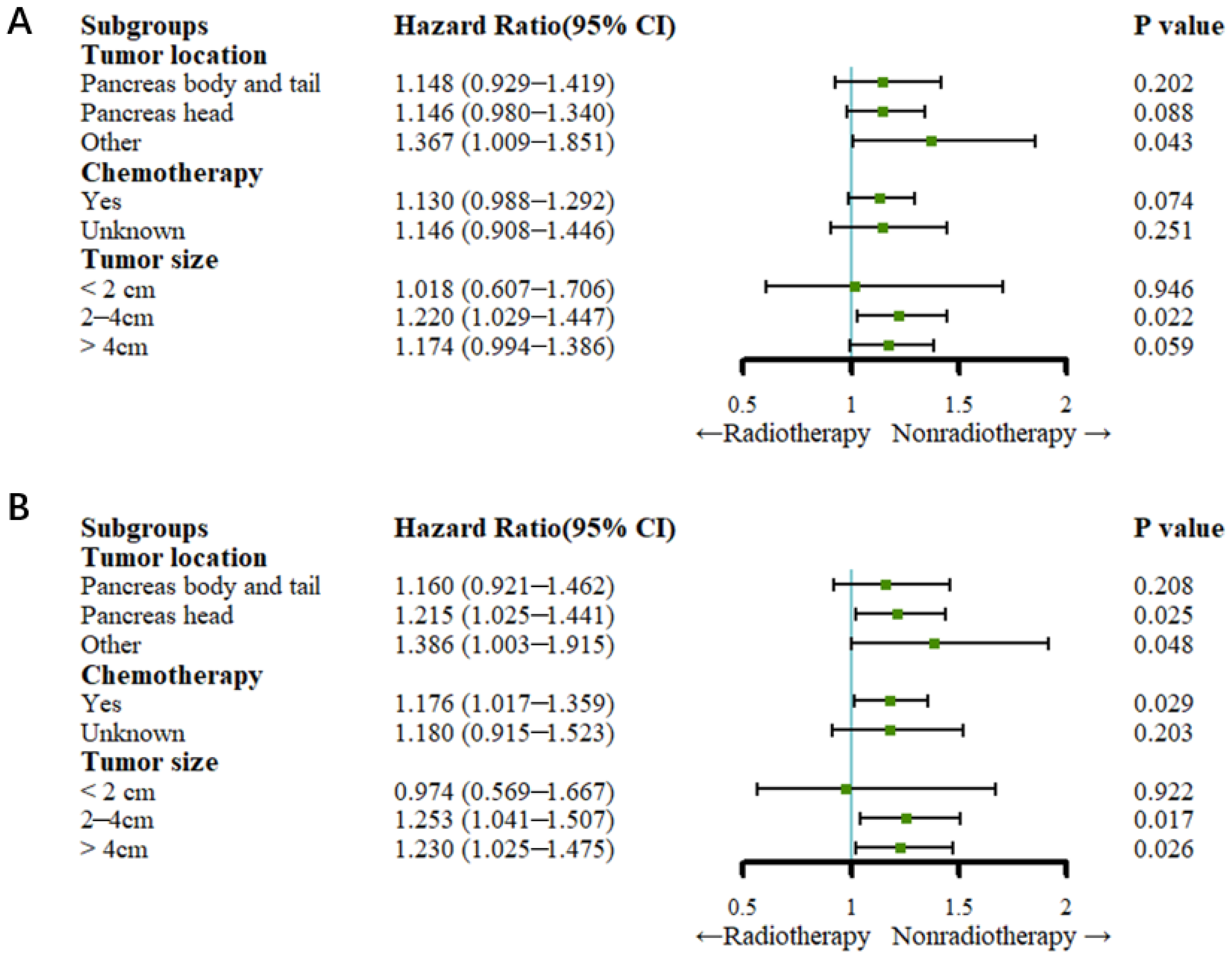
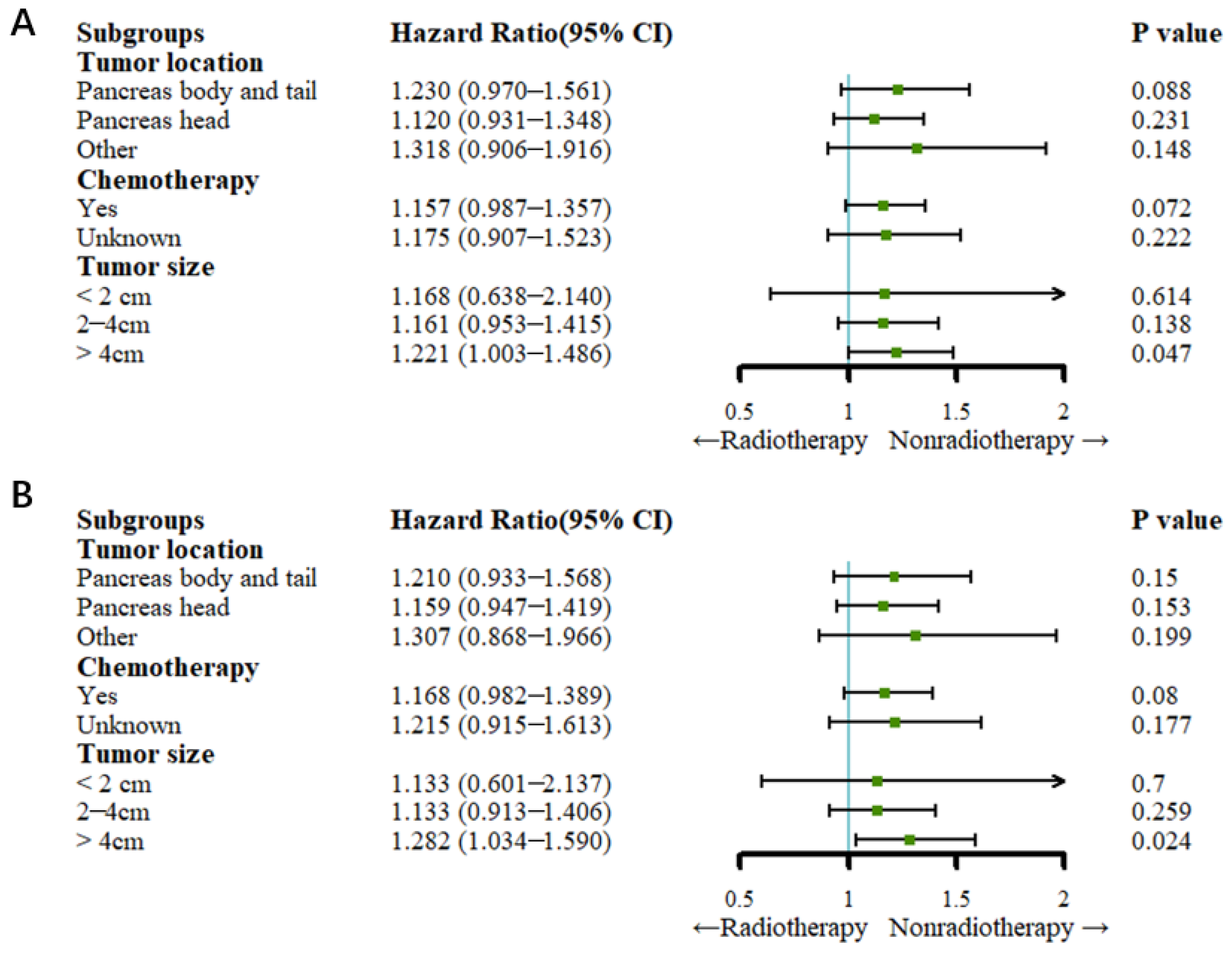
3.4. Subgroup Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Park, W.; Chawla, A.; O’Reilly, E.M. Pancreatic Cancer: A Review. JAMA 2021, 326, 851–862. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Pishvaian, M.J.; Brody, J.R. Therapeutic Implications of Molecular Subtyping for Pancreatic Cancer. Oncology 2017, 31, 159–166. [Google Scholar] [PubMed]
- Kleeff, J.; Korc, M.; Apte, M.; La Vecchia, C.; Johnson, C.D.; Biankin, A.V.; Neale, R.E.; Tempero, M.; Tuveson, D.A.; Hruban, R.H.; et al. Pancreatic cancer. Nat. Rev. Dis. Primers 2016, 2, 16022. [Google Scholar] [CrossRef] [PubMed]
- Tempero, M.A.; Malafa, M.P.; Al-Hawary, M.; Behrman, S.W.; Benson, A.B.; Cardin, D.B.; Chiorean, E.G.; Chung, V.; Czito, B.; Del Chiaro, M.; et al. Pancreatic Adenocarcinoma, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc Netw 2021, 19, 439–457. [Google Scholar] [CrossRef] [PubMed]
- Gong, L.; Zhang, Y.; Liu, C.; Zhang, M.; Han, S. Application of Radiosensitizers in Cancer Radiotherapy. Int. J. Nanomedicine 2021, 16, 1083–1102. [Google Scholar] [CrossRef]
- Ejaz, A.; Greenberger, J.S.; Rubin, P.J. Understanding the mechanism of radiation induced fibrosis and therapy options. Pharmacol. Ther. 2019, 204, 107399. [Google Scholar] [CrossRef]
- Hubenak, J.R.; Zhang, Q.; Branch, C.D.; Kronowitz, S.J. Mechanisms of injury to normal tissue after radiotherapy: A review. Plast Reconstr. Surg. 2014, 133, 49e–56e. [Google Scholar] [CrossRef]
- Han, D.; Gao, F.; Liu, J.L.; Wang, H.; Fu, Q.; Yang, G.W. Analysis of radiotherapy impact on survival in resected stage I/II pancreatic cancer patients: A population-based study. BMC Cancer 2021, 21, 560. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Liu, C.; Zhou, Y.; Yan, T.; Li, C.; Yang, Q.; Xu, Y.; Zhao, L.; Pei, Q.; Tan, F.; et al. Effect of neoadjuvant radiotherapy on survival of non-metastatic pancreatic ductal adenocarcinoma: A SEER database analysis. Radiat Oncol. 2020, 15, 107. [Google Scholar] [CrossRef]
- Versteijne, E.; Suker, M.; Groothuis, K.; Akkermans-Vogelaar, J.M.; Besselink, M.G.; Bonsing, B.A.; Buijsen, J.; Busch, O.R.; Creemers, G.M.; van Dam, R.M.; et al. Preoperative Chemoradiotherapy Versus Immediate Surgery for Resectable and Borderline Resectable Pancreatic Cancer: Results of the Dutch Randomized Phase III PREOPANC Trial. J. Clin. Oncol. 2020, 38, 1763–1773. [Google Scholar] [CrossRef]
- Murphy, J.E.; Wo, J.Y.; Ryan, D.P.; Clark, J.W.; Jiang, W.; Yeap, B.Y.; Drapek, L.C.; Ly, L.; Baglini, C.V.; Blaszkowsky, L.S.; et al. Total Neoadjuvant Therapy With FOLFIRINOX in Combination With Losartan Followed by Chemoradiotherapy for Locally Advanced Pancreatic Cancer: A Phase 2 Clinical Trial. JAMA Oncol. 2019, 5, 1020–1027. [Google Scholar] [CrossRef] [PubMed]
- Katz, M.H.; Shi, Q.; Ahmad, S.A.; Herman, J.M.; Marsh Rde, W.; Collisson, E.; Schwartz, L.; Frankel, W.; Martin, R.; Conway, W.; et al. Preoperative Modified FOLFIRINOX Treatment Followed by Capecitabine-Based Chemoradiation for Borderline Resectable Pancreatic Cancer: Alliance for Clinical Trials in Oncology Trial A021101. JAMA Surg. 2016, 151, e161137. [Google Scholar] [CrossRef]
- Hammel, P.; Huguet, F.; van Laethem, J.L.; Goldstein, D.; Glimelius, B.; Artru, P.; Borbath, I.; Bouché, O.; Shannon, J.; André, T.; et al. Effect of Chemoradiotherapy vs Chemotherapy on Survival in Patients With Locally Advanced Pancreatic Cancer Controlled After 4 Months of Gemcitabine With or Without Erlotinib: The LAP07 Randomized Clinical Trial. JAMA 2016, 315, 1844–1853. [Google Scholar] [CrossRef]
- Rackwitz, T.; Debus, J. Clinical applications of proton and carbon ion therapy. Semin. Oncol. 2019, 46, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y. The role of radiotherapy for pancreatic malignancies: A population-based analysis of the SEER database. Clin. Transl. Oncol. 2022, 24, 76–83. [Google Scholar] [CrossRef]
- Shi, X.; Peng, J.; Jiang, H.; Gao, Y.; Wang, W.; Zhou, F. Impact of Adjuvant Chemoradiotherapy on Survival of Resected Pancreatic Adenocarcinoma Cancer: A Surveillance, Epidemiology and End Results (SEER) Analysis. Front. Oncol. 2021, 11, 651671. [Google Scholar] [CrossRef] [PubMed]
- Scorsetti, M.; Comito, T.; Franceschini, D.; Franzese, C.; Prete, M.G.; D’Alessio, A.; Bozzarelli, S.; Rimassa, L.; Santoro, A. Is there an oligometastatic state in pancreatic cancer? Practical clinical considerations raise the question. Br. J. Radiol. 2020, 93, 20190627. [Google Scholar] [CrossRef] [PubMed]
- Chun, Y.S.; Pawlik, T.M.; Vauthey, J.N. 8th Edition of the AJCC Cancer Staging Manual: Pancreas and Hepatobiliary Cancers. Ann. Surg. Oncol. 2018, 25, 845–847. [Google Scholar] [CrossRef] [PubMed]
- Jokar, S.; Marques, I.A.; Khazaei, S.; Martins-Marques, T.; Girao, H.; Laranjo, M.; Botelho, M.F. The Footprint of Exosomes in the Radiation-Induced Bystander Effects. Bioengineering 2022, 9, 243. [Google Scholar] [CrossRef]
- Conroy, T.; Desseigne, F.; Ychou, M.; Bouché, O.; Guimbaud, R.; Bécouarn, Y.; Adenis, A.; Raoul, J.L.; Gourgou-Bourgade, S.; de la Fouchardière, C.; et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N. Engl. J. Med. 2011, 364, 1817–1825. [Google Scholar] [CrossRef] [PubMed]
- Von Hoff, D.D.; Ervin, T.; Arena, F.P.; Chiorean, E.G.; Infante, J.; Moore, M.; Seay, T.; Tjulandin, S.A.; Ma, W.W.; Saleh, M.N.; et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N. Engl. J. Med. 2013, 369, 1691–1703. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Zhang, J.; Lui, W.; Huo, Y.; Fu, X.; Yang, M.; Hua, R.; Wang, L.; Sun, Y. Patients with hepatic oligometastatic pancreatic body/tail ductal adenocarcinoma may benefit from synchronous resection. HPB 2020, 22, 91–101. [Google Scholar] [CrossRef] [PubMed]
- Takeda, T.; Sasaki, T.; Inoue, Y.; Mie, T.; Furukawa, T.; Kanata, R.; Kasuga, A.; Matsuyama, M.; Ozaka, M.; Takahashi, Y.; et al. Comprehensive comparison of clinicopathological characteristics, treatment, and prognosis of borderline resectable pancreatic cancer according to tumor location. Pancreatology 2020, 20, 1123–1130. [Google Scholar] [CrossRef] [PubMed]
- Winer, L.K.; Dhar, V.K.; Wima, K.; Morris, M.C.; Lee, T.C.; Shah, S.A.; Ahmad, S.A.; Patel, S.H. The Impact of Tumor Location on Resection and Survival for Pancreatic Ductal Adenocarcinoma. J. Surg. Res. 2019, 239, 60–66. [Google Scholar] [CrossRef]
- Park, H.; An, S.; Eo, S.H.; Song, K.B.; Park, J.H.; Kim, K.P.; Lee, S.S.; Cho, H.; Seo, D.W.; Kim, S.C.; et al. Survival effect of tumor size and extrapancreatic extension in surgically resected pancreatic cancer: Proposal for improved T classification. Hum. Pathol. 2014, 45, 2341–2346. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Before Matching | After Matching | |||||
|---|---|---|---|---|---|---|
| Characteristics | Radiotherapy (N = 304, %) | Nonradiotherapy (N = 8231, %) | p Value | Radiotherapy (N = 274, %) | Nonradiotherapy (N = 1038, %) | p Value |
| Age at Diagnosis (Years) | <0.001 | 0.132 | ||||
| 30–44 | 18 | 180 | 10 | 19 | ||
| 45–59 | 93 | 2095 | 78 | 274 | ||
| ≥60 | 193 | 5956 | 186 | 745 | ||
| Gender | 0.694 | 0.431 | ||||
| Male | 171 | 4536 | 153 | 607 | ||
| Female | 133 | 3695 | 121 | 431 | ||
| Race | 0.062 | 0.199 | ||||
| White | 225 | 6550 | 213 | 856 | ||
| Black | 52 | 1108 | 41 | 124 | ||
| Other | 27 | 573 | 20 | 58 | ||
| Year of Diagnosis | <0.001 | 0.098 | ||||
| 2010–2012 | 172 | 3606 | 150 | 510 | ||
| 2013–2015 | 132 | 4625 | 124 | 528 | ||
| Tumor Location | <0.001 | 0.007 | ||||
| Pancreas body and tail | 90 | 3295 | 85 | 401 | ||
| Pancreas head | 170 | 3379 | 154 | 473 | ||
| Other | 44 | 1557 | 35 | 164 | ||
| Tumor Grade | 0.230 | 0.070 | ||||
| Grade I | 4 | 96 | 3 | 6 | ||
| Grade II | 19 | 629 | 16 | 64 | ||
| Grade III | 42 | 880 | 35 | 83 | ||
| Grade IV | 3 | 36 | 3 | 3 | ||
| Unknown | 236 | 6590 | 217 | 882 | ||
| AJCC T Stage | <0.001 | 0.016 | ||||
| T1 | 8 | 257 | 8 | 22 | ||
| T2 | 92 | 2851 | 84 | 365 | ||
| T3 | 104 | 2526 | 95 | 346 | ||
| T4 | 86 | 1555 | 75 | 213 | ||
| TX | 14 | 1042 | 12 | 92 | ||
| AJCC N Stage | 0.016 | 0.726 | ||||
| N0 | 172 | 4619 | 154 | 580 | ||
| N1 | 111 | 2629 | 101 | 371 | ||
| NX | 21 | 983 | 19 | 87 | ||
| Chemotherapy | 0.001 | 0.161 | ||||
| Yes | 231 | 5530 | 203 | 724 | ||
| Unknown | 73 | 2701 | 71 | 314 | ||
| Tumor Size (cm) | 0.829 | 0.497 | ||||
| <2 | 15 | 464 | 15 | 44 | ||
| 2–4 | 140 | 3836 | 127 | 515 | ||
| >4 | 149 | 3931 | 132 | 479 | ||
| Tumor number | 0.005 | 0.896 | ||||
| 1 | 261 | 6571 | 505 | 882 | ||
| ≥2 | 43 | 1480 | 91 | 156 | ||
| Insurance | 0.060 | <0.001 | ||||
| Yes | 289 | 7882 | 234 | 1003 | ||
| No | 13 | 253 | 40 | 28 | ||
| Unknown | 2 | 96 | 1 | 7 | ||
| Marital Status | 0.134 | 0.190 | ||||
| Married | 194 | 4782 | 178 | 687 | ||
| Single | 100 | 3107 | 86 | 332 | ||
| Unknown | 10 | 342 | 10 | 19 | ||
| Univariable Analysis | Multivariable Analysis | |||
|---|---|---|---|---|
| Variables | HR (95%CI) | p Value | HR (95%CI) | p Value |
| Age at diagnosis (Years) | ||||
| 30–44 | Ref | Ref | ||
| 45–59 | 1.317 (1.131,1.534) | <0.001 | 1.272 (1.092,1.482) | 0.002 |
| ≥60 | 1.670 (1.440,1.937) | <0.001 | 1.572 (1.354,1.825) | <0.001 |
| Gender | ||||
| Male | Ref | |||
| Female | 0.973 (0.931,1.016) | 0.217 | ||
| Race | ||||
| White | Ref | Ref | ||
| Black | 1.131 (1.061,1.205) | <0.001 | 1.084 (1.016,1.156) | 0.015 |
| Other | 1.031 (0.946,1.123) | 0.488 | 0.965 (0.885,1.052) | 0.419 |
| Year of diagnosis | ||||
| 2010–2012 | Ref | Ref | ||
| 2013–2015 | 0.913 (0.874,0.953) | <0.001 | 0.948 (0.907,0.991) | 0.017 |
| Tumor location | ||||
| pancreas body and tail | Ref | |||
| pancreas head | 0.967 (0.921,1.014) | 0.167 | ||
| other | 1.048 (0.986,1.113) | 0.135 | ||
| Tumor grade | ||||
| Grade I | Ref | |||
| Grade II | 1.018 (0.819.1.265) | 0.871 | ||
| Grade III | 1.226 (0.991,1.517) | 0.061 | ||
| Grade IV | 1.070 (0.731,1.565) | 0.729 | ||
| Unknown | 1.152 (0.939,1.412) | 0.174 | ||
| AJCC T Stage | ||||
| T1 | Ref | Ref | ||
| T2 | 1.108 (0.974,1.261) | 0.118 | 0.903 (0.745,1.095) | 0.299 |
| T3 | 1.007 (0.885,1.146) | 0.914 | 0.845 (0.699,1.020) | 0.080 |
| T4 | 1.052 (0.921,1.201) | 0.458 | 0.866 (0.714,1.050) | 0.143 |
| TX | 1.157 (1.008,1.329) | 0.038 | 0.908 (0.750,1.101) | 0.327 |
| AJCC N Stage | ||||
| N0 | Ref | Ref | ||
| N1 | 0.998 (0.951,1.047) | 0.929 | 1.028 (0.979,1.079) | 0.264 |
| NX | 1.099 (1.025,1.177) | 0.008 | 1.043 (0.970,1.122) | 0.256 |
| Chemotherapy | ||||
| Yes | Ref | Ref | ||
| Unknown | 2.367 (2.256,2.482) | <0.001 | 2.280 (2.172,2.394) | <0.001 |
| Tumor size (cm) | ||||
| <2 | Ref | Ref | ||
| 2–4 | 1.076 (0.975,1.186) | 0.144 | 1.182 (1.023,1.366) | 0.024 |
| >4 | 1.204 (1.092,1.328) | <0.001 | 1.374 (1.190,1.587) | <0.001 |
| Tumor number | ||||
| 1 | Ref | |||
| ≥2 | 0.947 (0.895,1.002) | 0.061 | ||
| Insurance | ||||
| Yes | Ref | Ref | ||
| No | 1.179 (1.039,1.338) | 0.011 | 1.178 (1.036,1.339) | 0.012 |
| Unknown | 1.133 (0.924,1.388) | 0.230 | 1.064 (0.865,1.308) | 0.556 |
| Marital status | ||||
| Married | Ref | Ref | ||
| Single | 1.246 (1.191,1.304) | <0.001 | 1.151 (1.098,1.205) | <0.001 |
| Unknown | 1.094 (0.979,1.221) | 0.113 | 1.003 (0.896,1.122) | 0.962 |
| Treatment | ||||
| Radiotherapy | Ref | Ref | ||
| Nonradiotherapy | 1.184 (1.055,1.330) | 0.004 | 1.113 (0.990,1.251) | 0.073 |
| Univariable Analysis | Multivariable Analysis | |||
|---|---|---|---|---|
| Variables | HR (95%CI) | p Value | HR (95%CI) | p Value |
| Age at diagnosis (years) | ||||
| 30–44 | Ref | Ref | ||
| 45–59 | 1.278 (1.090,1.497) | 0.002 | 1.205 (1.028,1.412) | 0.022 |
| ≥60 | 1.651 (1.415,1.927) | <0.001 | 1.520 (1.301,1.776) | <0.001 |
| Gender | ||||
| Male | Ref | |||
| Female | 0.990 (0.943,1.040) | 0.688 | ||
| Race | ||||
| White | Ref | Ref | ||
| Black | 1.126 (1.049,1.208) | 0.001 | 1.095 (1.018,1.117) | 0.014 |
| Other | 1.051 (0.957,1.155) | 0.298 | 0.998 (0.908,1.097) | 0.969 |
| Year of diagnosis | ||||
| 2010–2012 | Ref | Ref | ||
| 2013–2015 | 0.905 (0.861,0.950) | <0.001 | 0.934 (0.889,0.981) | 0.006 |
| Tumor location | ||||
| Pancreas body and tail | Ref | |||
| Pancreas head | 0.984 (0.932,1.038) | 0.550 | ||
| Other | 1.063 (0.992,1.138) | 0.083 | ||
| Tumor grade | ||||
| Grade I | Ref | Ref | ||
| Grade II | 1.046 (0.818,1.338) | 0.718 | 1.214 (0.948,1.553) | 0.124 |
| Grade III | 1.336 (1.050,1.700) | 0.019 | 1.609 (1.263,2.050) | <0.001 |
| Grade IV | 1.059 (0.689,1.628) | 0.794 | 1.165 (0.757,1.794) | 0.487 |
| Unknown | 1.221 (0.969,1.538) | 0.090 | 1.442 (1.143,1.818) | 0.002 |
| AJCC T stage | ||||
| T1 | Ref | |||
| T2 | 1.096 (0.944,1.271) | 0.228 | ||
| T3 | 1.005 (0.866,1.166) | 0.948 | ||
| T4 | 1.045 (0.894,1.217) | 0.575 | ||
| TX | 1.142 (0.975,1.339) | 0.100 | ||
| AJCC N stage | ||||
| N0 | Ref | Ref | ||
| N1 | 0.997 (0.945,1.052) | 0.908 | 1.013 (0.960,1.069) | 0.626 |
| NX | 1.082 (1.001,1.170) | 0.049 | 1.030 (0.951,1.114) | 0.469 |
| Chemotherapy | ||||
| Yes | Ref | Ref | ||
| Unknown | 2.412 (2.286,2.545) | <0.001 | 2.337 (1.212,2.469) | <0.001 |
| Tumor size (cm) | ||||
| <2 | Ref | Ref | ||
| 2–4 | 1.082 (0.968,1.211) | 0.165 | 1.088 (0.973,1.218) | 0.139 |
| >4 | 1.196 (1.070,1.337) | 0.002 | 1.248 (1.116,1.396) | <0.001 |
| Tumor number | ||||
| 1 | Ref | Ref | ||
| ≥2 | 0.576 (0.437,0.759) | <0.001 | 0.581 (0.441,0.766) | <0.001 |
| Insurance | ||||
| Yes | Ref | Ref | ||
| No | 1.160 (1.014,1.328) | 0.031 | 1.137 (0.992,1.303) | 0.066 |
| Unknown | 1.050 (0.831,1.327) | 0.683 | 1.050 (0.829,1.331) | 0.686 |
| Marital status | ||||
| Married | Ref | Ref | ||
| Single | 1.279 (1.215,1.346) | <0.001 | 1.176 (1.117,1.240) | <0.001 |
| Unknown | 1.067 (0.943,1.209) | 0.303 | 0.985 (0.869,1.118) | 0.820 |
| Treatment | ||||
| Radiotherapy | Ref | Ref | ||
| Nonradiotherapy | 1.226 (1.080,1.389) | 0.002 | 1.174 (1.035,1.333) | 0.013 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, L.; Lu, Y.; Chen, L.; Yue, X.; Cen, C.; Zheng, C.; Han, P. The Effects of Radiotherapy on Pancreatic Ductal Adenocarcinoma in Patients with Liver Metastases. Curr. Oncol. 2022, 29, 7912-7924. https://doi.org/10.3390/curroncol29100625
Wu L, Lu Y, Chen L, Yue X, Cen C, Zheng C, Han P. The Effects of Radiotherapy on Pancreatic Ductal Adenocarcinoma in Patients with Liver Metastases. Current Oncology. 2022; 29(10):7912-7924. https://doi.org/10.3390/curroncol29100625
Chicago/Turabian StyleWu, Linxia, Yuting Lu, Lei Chen, Xiaofei Yue, Chunyuan Cen, Chuansheng Zheng, and Ping Han. 2022. "The Effects of Radiotherapy on Pancreatic Ductal Adenocarcinoma in Patients with Liver Metastases" Current Oncology 29, no. 10: 7912-7924. https://doi.org/10.3390/curroncol29100625
APA StyleWu, L., Lu, Y., Chen, L., Yue, X., Cen, C., Zheng, C., & Han, P. (2022). The Effects of Radiotherapy on Pancreatic Ductal Adenocarcinoma in Patients with Liver Metastases. Current Oncology, 29(10), 7912-7924. https://doi.org/10.3390/curroncol29100625