Chemotherapy-Induced Neuropathy and Diabetes: A Scoping Review




Abstract
:1. Introduction
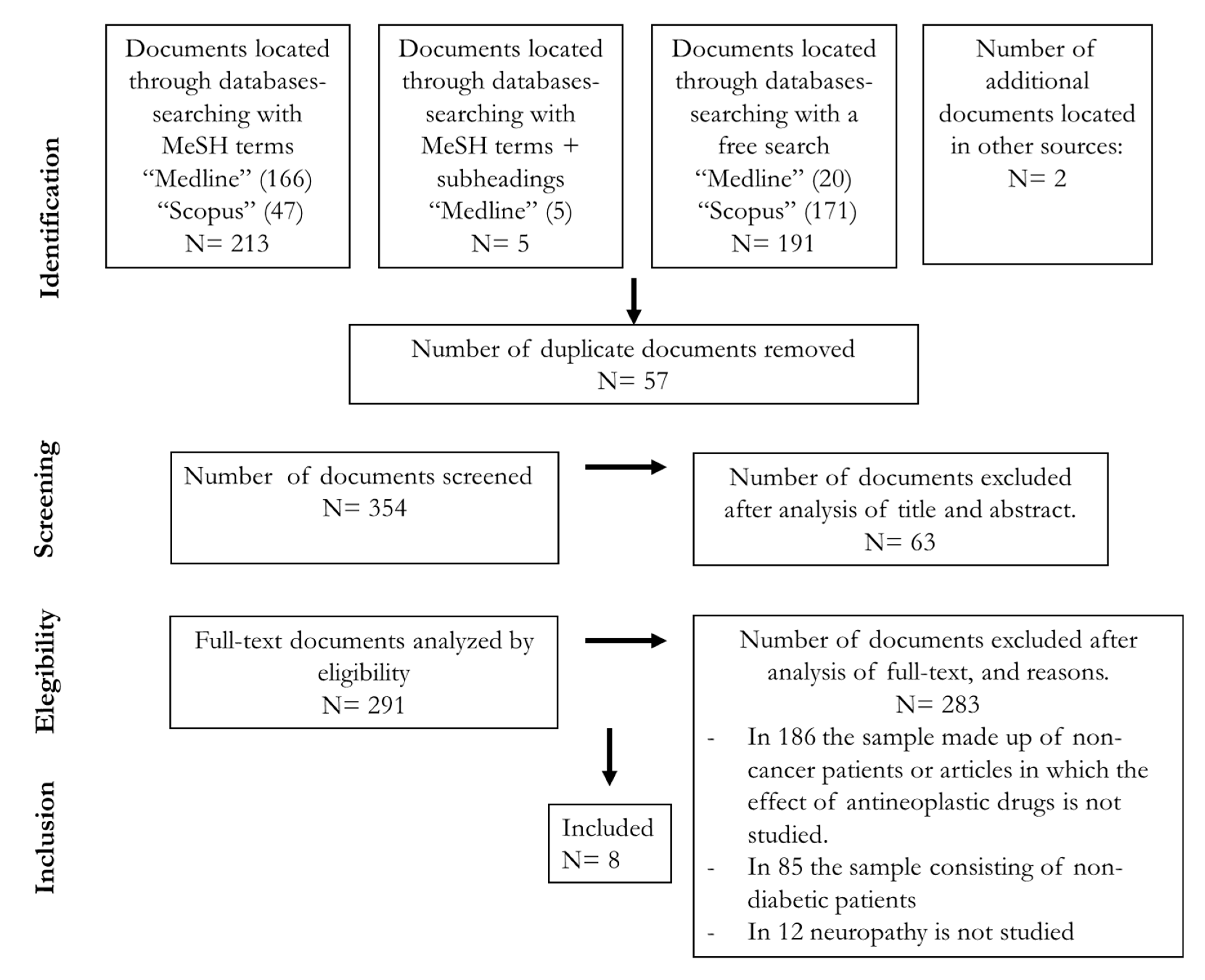
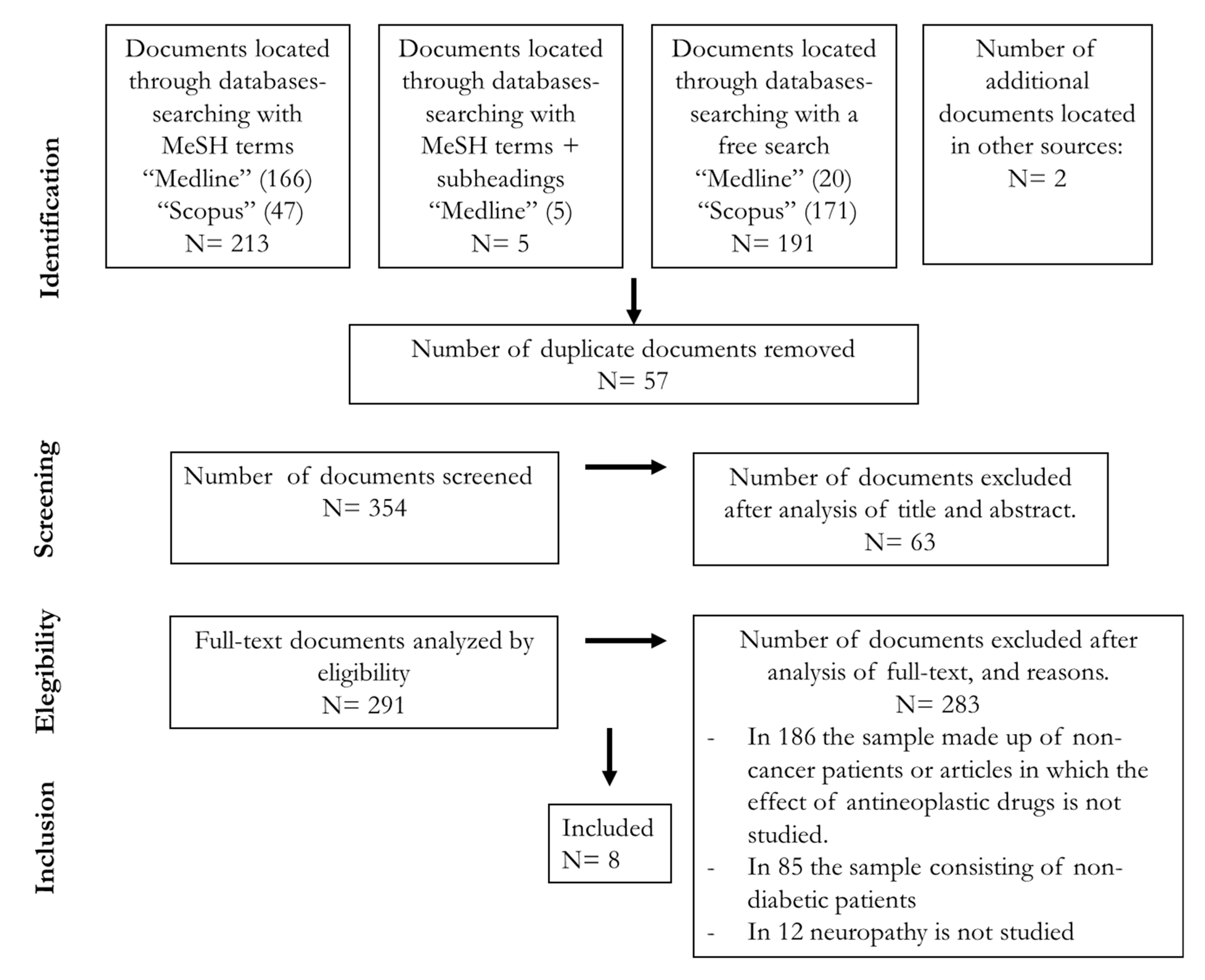
2. Methods
2.1. Literature Search
- -
- PubMed: (((antineoplastic agents) AND (diabetes mellitus)) AND (peripheral neuropathy)) NOT (review)
- -
- Scopus: “antineoplastic agents” AND “diabetes mellitus” AND “peripheral neuropathy” AND NOT review AND NOT animals
- -
- Studies carried out in humans.
- -
- Articles of the type: review, meta-analysis and systematic review were excluded.
- -
- Studies available in English or Spanish.
- -
- PubMed: (((“diabetes mellitus”[All Fields]) AND (“chemotherapy”[All Fields])) AND (“neuropathy”[All Fields])) NOT (review)
- -
- Scopus: “diabetes mellitus” AND chemotherapy AND “peripheral neuropathy” AND NOT review AND NOT animals
2.2. Inclusion and Exclusion Criteria
2.3. Analysis
3. Results
3.1. Characteristics of the Studies Analyzed
3.2. Neuropathy Prevalence/Incidence after Chemotherapy in Diabetic Patients
3.3. Effects of Diabetes on Different Types of Neuropathic Alterations Induced by Chemotherapy
3.4. Neuropathy Onset and Influence on Chemotherapeutic Drugs and Dosage in Diabetic Patients with Cancer
3.5. Diabetes Control and Treatment during Chemotherapy Treatment
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Shapiro, C.L. Highlights of recent findings on quality-of-life management for patients with cancer and their survivors. JAMA Oncol. 2016, 2, 1401–1402. [Google Scholar] [CrossRef]
- Schloss, J.M.; Colosimo, M.; Airey, C.; Masci, P.; Linnane, A.W.; Vitetta, L. A randomised, placebo-controlled trial assessing the efficacy of an oral B group vitamin in preventing the development of chemotherapy-induced peripheral neuropathy (CIPN). Support. Care Cancer 2017, 25, 195–204. [Google Scholar] [CrossRef] [PubMed]
- Vissers, P.A.J.; Mols, F.; Thong, M.S.Y.; Pouwer, F.; Vreugdenhil, G.; van de Poll-Franse, L.V. The impact of diabetes on neuropathic symptoms and receipt of chemotherapy among colorectal cancer patients: Results from the PROFILES registry. J. Cancer Surviv. 2015, 9, 523–531. [Google Scholar] [CrossRef] [PubMed]
- Nurgalieva, Z.; Xia, R.; Liu, C.C.; Burau, K.; Hardy, D.; Du, X.L. Risk of chemotherapy-induced peripheral neuropathy in large population-based cohorts of elderly patients with breast, ovarian, and lung cancer. Am. J. Ther. 2010, 17, 148–158. [Google Scholar] [CrossRef]
- Uwah, A.N.; Ackler, J.; Leighton, J.C.; Pomerantz, S.; Tester, W. The effect of diabetes on oxaliplatin-induced peripheral neuropathy. Clin. Colorectal Cancer 2012, 11, 275–279. [Google Scholar] [CrossRef] [PubMed]
- Giovannucci, E.; Harlan, D.M.; Archer, M.C.; Bergenstal, R.M.; Gapstur, S.M.; Habel, L.A.; Pollak, M.; Regensteiner, J.G.; Yee, D. Diabetes and cancer: A consensus report. Diabetes Care 2010, 33, 1674–1685. [Google Scholar] [CrossRef] [Green Version]
- Vona-Davis, L.; P. Rose, D. Type 2 Diabetes and Obesity Metabolic Interactions: Common Factors for Breast Cancer Risk and Novel Approaches to Prevention and Therapy. Curr. Diabetes Rev. 2012, 8, 116–130. [Google Scholar] [CrossRef]
- Tuccori, M.; Convertino, I.; Galiulo, M.T.; Marino, A.; Capogrosso-Sansone, A.; Blandizzi, C. Diabetes drugs and the incidence of solid cancers: A survey of the current evidence. Expert Opin. Drug Saf. 2017, 16, 1133–1148. [Google Scholar] [CrossRef]
- Wilde, L.; Roche, M.; Domingo-Vidal, M.; Tanson, K.; Philp, N.; Curry, J.; Martinez-Outschoorn, U. Metabolic coupling and the Reverse Warburg Effect in cancer: Implications for novel biomarker and anticancer agent development. Semin. Oncol. 2017, 44, 198–203. [Google Scholar] [CrossRef]
- Soroku, Y.; Mizukami, H.; Sugimoto, K. Mechanism of diabetic neuropathy: Where are we now and where to go? J. Diabetes Investig. 2011, 2, 18–32. [Google Scholar] [CrossRef] [Green Version]
- Dewanjee, S.; Das, S.; Das, A.K.; Bhattacharjee, N.; Dihingia, A.; Dua, T.K.; Kalita, J.; Manna, P. Molecular mechanism of diabetic neuropathy and its pharmacotherapeutic targets. Eur. J. Pharmacol. 2018, 833, 472–523. [Google Scholar] [CrossRef] [PubMed]
- Hershman, D.L.; Till, C.; Wright, J.D.; Awad, D.; Ramsey, S.D.; Barlow, W.E.; Minasian, L.M.; Unger, J. Comorbidities and risk of chemotherapy-induced peripheral neuropathy among participants 65 years or older in southwest oncology group clinical trials. J. Clin. Oncol. 2016, 34, 3014–3022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneider, B.P.; Zhao, F.; Wang, M.; Stearns, V.; Martino, S.; Jones, V.; Perez, E.A.; Saphner, T.; Wolff, A.C.; Sledge, G.W.; et al. Neuropathy is not associated with clinical outcomes in patients receiving adjuvant taxane-containing therapy for operable breast cancer. J. Clin. Oncol. 2012, 30, 3051–3057. [Google Scholar] [CrossRef] [Green Version]
- Alhowail, A.H.; Bloemer, J.; Majrashi, M.; Pinky, P.D.; Bhattacharya, S.; Yongli, Z.; Bhattacharya, D.; Eggert, M.; Woodie, L.; Buabeid, M.A.; et al. Doxorubicin-induced neurotoxicity is associated with acute alterations in synaptic plasticity, apoptosis, and lipid peroxidation. Toxicol. Mech. Methods 2019, 29, 457–466. [Google Scholar] [CrossRef]
- Argyriou, A.A.; Kyritsis, A.P.; Makatsoris, T.; Kalofonos, H.P. Chemotherapy-induced peripheral neuropathy in adults: A comprehensive update of the literature. Cancer Manag. Res. 2014, 6, 135–147. [Google Scholar] [CrossRef] [Green Version]
- Winer, E.P.; Berry, D.A.; Woolf, S.; Duggan, D.; Kornblith, A.; Harris, L.N.; Michaelson, R.A.; Kirshner, J.A.; Fleming, G.F.; Perry, M.C.; et al. Failure of higher-dose paclitaxel to improve outcome in patients with metastatic breast cancer: Cancer and leukemia group B trial 9342. J. Clin. Oncol. 2004, 22, 2061–2068. [Google Scholar] [CrossRef]
- Grisold, W.; Cavaletti, G.; Windebank, A.J. Peripheral neuropathies from chemotherapeutics and targeted agents: Diagnosis, treatment, and prevention. Neuro. Oncol. 2012, 14 (Suppl. S4), iv45–iv54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kruijtzer, C.M.F.; Verweij, J.; Schellens, J.H.M.; Beijnen, J.H.; Pronk, L.; Bo, M.; Lustig, V.; Van Tinteren, H.; Mackay, M.; Ten Bokkel Huinink, W.W. Docetaxel in 253 previously treated patients with progressive locally advanced or metastatic breast cancer: Results of a compassionate use program in The Netherlands. Anticancer Drugs 2000, 11, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Staff, N.P.; Cavaletti, G.; Islam, B.; Lustberg, M.; Psimaras, D.; Tamburin, S. Platinum-induced peripheral neurotoxicity: From pathogenesis to treatment. J. Peripher. Nerv. Syst. 2019, 24, S26–S39. [Google Scholar] [CrossRef] [PubMed]
- Quasthoff, S.; Hartung, H.P. Chemotherapy-induced peripheral neuropathy. J. Neurol. 2002, 249, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Argyriou, A.A.; Bruna, J.; Marmiroli, P.; Cavaletti, G. Chemotherapy-induced peripheral neurotoxicity (CIPN): An update. Crit. Rev. Oncol. Hematol. 2012, 82, 51–77. [Google Scholar] [CrossRef]
- Soularue, É.; Cohen, R.; Tournigand, C.; Zaanan, A.; Louvet, C.; Bachet, J.B.; Hentic, O.; Samalin, E.; Chibaudel, B.; de Gramont, A.; et al. Efficacité et tolérance du trastuzumab en association avec oxaliplatine et fluoropyrimidine; pour des patients avec adénocarcinome métastatique de l’estomac ou de la jonction œso-gastrique: Une étude rétrospective. Bull. Cancer 2015, 102, 324–331. [Google Scholar] [CrossRef] [PubMed]
- Park, S.B.; Goldstein, D.; Krishnan, A.V.; Lin, C.S.-Y.; Friedlander, M.L.; Cassidy, J.; Koltzenburg, M.; Kiernan, M.C. Chemotherapy-induced peripheral neurotoxicity: A critical analysis. CA Cancer J. Clin. 2013, 63, 419–437. [Google Scholar] [CrossRef] [PubMed]
- Amptoulach, S.; Tsavaris, N. Neurotoxicity Caused by the Treatment with Platinum Analogues. Chemother. Res. Pract. 2011, 2011, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Wang, Q.; Zhang, J.; Cao, J.; Wang, B.; Hu, X. Incidence of peripheral neuropathy associated with eribulin mesylate versus vinorelbine in patients with metastatic breast cancer: Sub-group analysis of a randomized phase III study. Support. Care Cancer 2020, 28, 3819–3829. [Google Scholar] [CrossRef]
- Martín, M.; Ruiz, A.; Muñoz, M.; Balil, A.; García-Mata, J.; Calvo, L.; Carrasco, E.; Mahillo, E.; Casado, A.; García-Saenz, J.Á.; et al. Gemcitabine plus vinorelbine versus vinorelbine monotherapy in patients with metastatic breast cancer previously treated with anthracyclines and taxanes: Final results of the phase III Spanish Breast Cancer Research Group (GEICAM) trial. Lancet Oncol. 2007, 8, 219–225. [Google Scholar] [CrossRef]
- Ray, J.; Mahmood, A.; Dogar, M.; Guo, J.; Nwamaghinna, F.; Salciccioli, L.; McFarlane, S.I. Simultaneous Cardiotoxicity and Neurotoxicity Associated with 5-fluorouracil Containing Chemotherapy: A Case Report and Literature Review. Am. J. Med. Case Rep. 2020, 8, 73–75. [Google Scholar] [CrossRef]
- Nguyen, M.T.; Stoianovici, R.; Brunetti, L. Chemotherapy induced stroke mimic: 5-Fluorouracil encephalopathy fulfilling criteria for tissue plasminogen activator therapy. Am. J. Emerg. Med. 2017, 35, 1389–1390. [Google Scholar] [CrossRef]
- Esin, E.; Telli, T.A.; Yuce, D.; Yalcin, S. A correlation study of fluorouracil pharmacodynamics with clinical efficacy and toxicity. Tumori 2018, 104, 157–164. [Google Scholar] [CrossRef] [Green Version]
- Moore, D.H.; Fowler, W.C.; Crumpler, L.S. 5-Fluorouracil neurotoxicity. Gynecol. Oncol. 1990, 36, 152–154. [Google Scholar] [CrossRef]
- Pellacani, C.; Eleftheriou, G. Neurotoxicity of antineoplastic drugs: Mechanisms, susceptibility, and neuroprotective strategies. Adv. Med. Sci. 2020, 65, 265–285. [Google Scholar] [CrossRef]
- Dormann, A.J.; Grünewald, T.; Wigginghaus, B.; Huchzermeyer, H. Gemcitabine-associated autonomic neuropathy. Lancet 1998, 351, 644. [Google Scholar] [CrossRef]
- Verstappen, C.C.P.; Heimans, J.J.; Hoekman, K.; Postma, T.J. Neurotoxic Complications of Chemotherapy in Patients with Cancer. Drugs 2003, 63, 1549–1563. [Google Scholar] [CrossRef]
- Khoshnoodi, M.A.; Ebenezer, G.J.; Polydefkis, M. Epidermal innervation as a tool to study human axonal regeneration and disease progression. Exp. Neurol. 2017, 287, 358–364. [Google Scholar] [CrossRef] [PubMed]
- de Gramont, A.; Figer, A.; Seymour, M.; Homerin, M.; Hmissi, A.; Cassidy, J.; Boni, C.; Cortes-Funes, H.; Cervantes, A.; Freyer, G.; et al. Leucovorin and fluorouracil with or without oxaliplatin as first-line treatment in advanced colorectal cancer. J. Clin. Oncol. 2000, 18, 2938–2947. [Google Scholar] [CrossRef] [PubMed]
- De La Morena Barrio, P.; Vicente Conesa, M.Á.; González-Billalabeitia, E.; Urrego, E.; García-Garre, E.; García-Martínez, E.; Poves, M.Z.; Vicente, V.; de la Peña, F.A. Delayed recovery and increased severity of paclitaxel-induced peripheral neuropathy in patients with diabetes. J. Natl. Compr. Cancer Netw. 2015, 13, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Van Schie, C.H.M. Neuropathy: Mobility and quality of life. Diabetes. Metab. Res. Rev. 2008, 24 (Suppl. S1), S45–S51. [Google Scholar] [CrossRef] [PubMed]
- Bruun, C.; Siersma, V.; Guassora, A.D.; Holstein, P.; de Fine Olivarius, N. Amputations and foot ulcers in patients newly diagnosed with type 2 diabetes mellitus and observed for 19 years. The role of age, gender and co-morbidity. Diabet. Med. 2013, 30, 964–972. [Google Scholar] [CrossRef] [PubMed]
- Bano, N.; Ikram, R. Effect of diabetes on neurological adverse effects and chemotherapy induced peripheral neuropathy in advanced colorectal cancer patients treated with different FOLFOX regimens. Pak. J. Pharm. Sci. 2019, 32, 125–130. [Google Scholar] [PubMed]
- Kus, T.; Aktas, G.; Kalender, M.E.; Sevinc, A.; Kul, S.; Suner, A.; Ulker, E.; Camci, C. Taxane-induced peripheral sensorial neuropathy in cancer patients is associated with duration of diabetes mellitus: A single-center retrospective study. Support. Care Cancer 2016, 24, 1175–1179. [Google Scholar] [CrossRef]
- Ramanathan, R.K.; Rothenberg, M.L.; de Gramont, A.; Tournigand, C.; Goldberg, R.M.; Gupta, S.; André, T. Incidence and evolution of oxaliplatin-induced eripheral sensory neuropathy in diabetic patients with colorectal cancer: A pooled analysis of three phase III studies. Ann. Oncol. 2009, 21, 754–758. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Rahman, O. Impact of diabetes comorbidity on the efficacy and safety of FOLFOX first-line chemotherapy among patients with metastatic colorectal cancer: A pooled analysis of two phase-III studies. Clin. Transl. Oncol. 2019, 21, 512–518. [Google Scholar] [CrossRef]
- Gogas, H.; Shapiro, F.; Aghajanian, C.; Fennelly, D.; Almadrones, L.; Hoskins, W.J.; Spriggs, D.R. The impact of diabetes mellitus on the toxicity of therapy for advanced ovarian cancer. Gynecol. Oncol. 1996, 61, 22–26. [Google Scholar] [CrossRef] [PubMed]
- Kanbayashi, Y.; Hosokawa, T.; Kitawaki, J.; Taguchi, T. Statistical identification of predictors for paclitaxel-induced peripheral neuropathy in patients with breast or gynaecological cancer. Anticancer Res. 2013, 33, 1153–1156. [Google Scholar] [PubMed]
- Tanabe, Y.; Hashimoto, K.; Shimizu, C.; Hirakawa, A.; Harano, K.; Yunokawa, M.; Yonemori, K.; Katsumata, N.; Tamura, K.; Ando, M.; et al. Paclitaxel-induced peripheral neuropathy in patients receiving adjuvant chemotherapy for breast cancer. Int. J. Clin. Oncol. 2013, 18, 132–138. [Google Scholar] [CrossRef]
- Park, S.B.; Lin, C.S.Y.; Krishnan, A.V.; Goldstein, D.; Friedlander, M.L.; Kiernan, M.C. Oxaliplatin-induced neurotoxicity: Changes in axonal excitability precede development of neuropathy. Brain 2009, 132, 2712–2723. [Google Scholar] [CrossRef] [PubMed]
- Kaba, H.; Fukuda, H.; Yamamoto, S.; Ohashi, Y. Reliability at the National Cancer Institute-Common Toxicity Criteria version 2.0. Gan To Kagaku Ryoho. 2004, 31, 1187–1192. [Google Scholar]
- Bouhassira, D.; Attal, N.; Fermanian, J.; Alchaar, H.; Gautron, M.; Masquelier, E.; Rostaing, S.; Lanteri-Minet, M.; Collin, E.; Grisart, J.; et al. Development and validation of the Neuropathic Pain Symptom Inventory. Pain 2004, 108, 248–257. [Google Scholar] [CrossRef]
- Postma, T.J.; Aaronson, N.K.; Heimans, J.J.; Muller, M.J.; Hildebrand, J.G.; Delattre, J.Y.; Hoang-Xuan, K.; Lantéri-Minet, M.; Grant, R.; Huddart, R.; et al. The development of an EORTC quality of life questionnaire to assess chemotherapy-induced peripheral neuropathy: The QLQ-CIPN20. Eur. J. Cancer 2005, 41, 1135–1139. [Google Scholar] [CrossRef]
- Velasco, R.; Bruna, J. Neuropatía inducida por quimioterapia: Un problema no resuelto. Neurologia 2010, 25, 116–131. [Google Scholar] [CrossRef]
- Seretny, M.; Currie, G.L.; Sena, E.S.; Ramnarine, S.; Grant, R.; Macleod, M.R.; Colvin, L.A.; Fallon, M. Incidence, prevalence, and predictors of chemotherapy-induced peripheral neuropathy: A systematic review and meta-analysis. Pain 2014, 155, 2461–2470. [Google Scholar] [CrossRef] [Green Version]
- Colvin, L.A.; Europe PMC Funders Group. Chemotherapy-induced peripheral neuropathy (CIPN): Where are we now? Pain 2019, 160 (Suppl. S1), S1–S10. [Google Scholar] [CrossRef]
- Gebremedhn, E.G.; Shortland, P.J.; Mahns, D.A. The incidence of acute oxaliplatin-induced neuropathy and its impact on treatment in the first cycle: A systematic review. BMC Cancer 2018, 18, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mols, F.; Beijers, T.; Lemmens, V.; van den Hurk, C.J.; Vreugdenhil, G.; van de Poll-Franse, L.V. Chemotherapy-Induced Neuropathy and Its Association with Quality of Life Among 2- to 11-Year Colorectal Cancer Survivors: Results from the Population-Based PROFILES Registry. J. Clin. Oncol. 2013, 31, 2699–2707. [Google Scholar] [CrossRef]
- Ibrahim, E.Y.; Ehrlich, B.E. Prevention of chemotherapy-induced peripheral neuropathy: A review of recent findings. Crit. Rev. Oncol. Hematol. 2020, 145, 102831. [Google Scholar] [CrossRef] [PubMed]
- Salehifar, E.; Janbabaei, G.; Alipour, A.; Tabrizi, N.; Avan, R. Taxane-induced peripheral neuropathy and quality of life in breast cancer patients. J. Oncol. Pharm. Pract. 2020, 26, 1421–1428. [Google Scholar] [CrossRef] [PubMed]
- Soveri, L.M.; Lamminmäki, A.; Hänninen, U.A.; Karhunen, M.; Bono, P.; Osterlund, P. Long-term neuropathy and quality of life in colorectal cancer patients treated with oxaliplatin containing adjuvant chemotherapy. Acta Oncol. 2019, 58, 398–406. [Google Scholar] [CrossRef] [Green Version]
- Matsuoka, H.; Nakamura, K.; Matsubara, Y.; Ida, N.; Saijo, M.; Ogawa, C.; Masuyama, H. The Influence of Chemotherapy-Induced Peripheral Neuropathy on Quality of Life of Gynecologic Cancer Survivors. Int. J. Gynecol. Cancer 2018, 28, 1394–1402. [Google Scholar] [CrossRef]
- Ceccarelli, E.; Mattaliano, C.; Brazzi, A.; Marinetti, A.C.; Nigi, L.; Chirico, C.; Corallo, C.; Fioravanti, A.; Giordano, N. Hyperglycemia and Diabetes Induced by Glucocorticoids in Nondiabetic and Diabetic Patients: Revision of Literature and Personal Considerations. Curr. Pharm. Biotechnol. 2019, 19, 1210–1220. [Google Scholar] [CrossRef]
- Hwang, J.L.; Weiss, R.E. Steroid-induced diabetes: A clinical and molecular approach to understanding and treatment. Diabetes. Metab. Res. Rev. 2014, 30, 96–102. [Google Scholar] [CrossRef]
- Navari, R.M.; Aapro, M. Antiemetic Prophylaxis for Chemotherapy-Induced Nausea and Vomiting. N. Engl. J. Med. 2016, 374, 1356–1367. [Google Scholar] [CrossRef]
- Phillips, R.S.; Friend, A.J.; Gibson, F.; Houghton, E.; Gopaul, S.; Craig, J.V.; Pizer, B. Antiemetic medication for prevention and treatment of chemotherapy-induced nausea and vomiting in childhood. Cochrane Database Syst. Rev. 2016, 2016, CD007786. [Google Scholar] [CrossRef]
- Vardy, J.; Chiew, K.S.; Galica, J.; Pond, G.R.; Tannock, I.F. Side effects associated with the use of dexamethasone for prophylaxis of delayed emesis after moderately emetogenic chemotherapy. Br. J. Cancer 2006, 94, 1011–1015. [Google Scholar] [CrossRef]
- Schwartz, J.R. Dexamethasone premedication for prophylaxis of taxane toxicities: Can the doses be reduced when paclitaxel or docetaxel are given weekly? J. Oncol. Pharm. Pract. 2012, 18, 250–256. [Google Scholar] [CrossRef]
- Crawford, E.D.; Shore, N.D.; Petrylak, D.P.; Higano, C.S.; Ryan, C.J. Abiraterone acetate and prednisone in chemotherapy-naïve prostate cancer patients: Rationale, evidence and clinical utility. Ther. Adv. Med. Oncol. 2017, 9, 319–333. [Google Scholar] [CrossRef] [PubMed]
- McKay, L.I.; Cidlowski, J.A. Corticosteroids in the Treatment of Neoplasms. Holland-Frei Cancer Medicine, 6th ed.; Kufe, D.W., Pollock, R.E., Weichselbaum, R.R., Bast, R.C., Gansler, T.S., Holland, J.F., Frei, E., Eds.; BC Decker: Hamilton, ON, Canada, 2003. [Google Scholar]
- Minetto, M.A.; D’Angelo, V.; Arvat, E.; Kesari, S. Diagnostic work-up in steroid myopathy. Endocrine 2018, 60, 219–223. [Google Scholar] [CrossRef]
- Chamberlain, M.C. Neurotoxicity of Cancer Treatment. Curr. Oncol. Rep. 2010, 12, 60–67. [Google Scholar] [CrossRef]
- Zajączkowska, R.; Kocot-Kępska, M.; Leppert, W.; Wrzosek, A.; Mika, J.; Wordliczek, J. Mechanisms of Chemotherapy-Induced Peripheral Neuropathy. Int. J. Mol. Sci. 2019, 20, 1451. [Google Scholar] [CrossRef] [Green Version]
- Comi, G.; Corbo, M. Metabolic neuropathies. Curr. Opin. Neurol. 1998, 11, 523–529. [Google Scholar] [CrossRef] [PubMed]
- Tesfaye, S.; Chaturvedi, N.; Eaton, S.E.M.; Ward, J.D.; Manes, C.; Ionescu-Tirgoviste, C.; Witte, D.R.; Fuller, J.H. Vascular Risk Factors and Diabetic Neuropathy. N. Engl. J. Med. 2005, 352, 341–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bao, T.; Basal, C.; Seluzicki, C.; Li, S.Q.; Seidman, A.D.; Mao, J.J. Long-term chemotherapy-induced peripheral neuropathy among breast cancer survivors: Prevalence, risk factors, and fall risk. Breast Cancer Res. Treat. 2016, 159, 327–333. [Google Scholar] [CrossRef]
- Visovsky, C.; Meyer, R.R.; Roller, J.; Poppas, M. Evaluation and management of peripheral neuropathy in diabetic patients with cancer. Clin. J. Oncol. Nurs. 2008, 12, 243–247. [Google Scholar] [CrossRef] [PubMed]
- Fallon, M.T.; Colvin, L. Neuropathic pain in cancer. Br. J. Anaesth. 2013, 111, 105–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoon, S.Y.; Oh, J. Neuropathic cancer pain: Prevalence, pathophysiology, and management. Korean J. Intern. Med. 2018, 33, 1058–1069. [Google Scholar] [CrossRef] [PubMed]
- Barrett, E.J.; Liu, Z.; Khamaisi, M.; King, G.L.; Klein, R.; Klein, B.E.K.; Hughes, T.M.; Craft, S.; Freedman, B.I.; Bowden, D.W.; et al. Diabetic Microvascular Disease: An Endocrine Society Scientific Statement. J. Clin. Endocrinol. Metab. 2017, 102, 4343–4410. [Google Scholar] [CrossRef]
- Callaghan, B.C.; Cheng, H.T.; Stables, C.L.; Smith, A.L.; Feldman, E.L. Diabetic neuropathy: Clinical manifestations and current treatments. Lancet Neurol. 2012, 11, 521–534. [Google Scholar] [CrossRef] [Green Version]
- Román-Pintos, L.M.; Villegas-Rivera, G.; Rodríguez-Carrizalez, A.D.; Miranda-Díaz, A.G.; Cardona-Muñoz, E.G. Diabetic Polyneuropathy in Type 2 Diabetes Mellitus: Inflammation, Oxidative Stress, and Mitochondrial Function. J. Diabetes Res. 2016, 2016, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Sandireddy, R.; Yerra, V.G.; Areti, A.; Komirishetty, P.; Kumar, A. Neuroinflammation and Oxidative Stress in Diabetic Neuropathy: Futuristic Strategies Based on These Targets. Int. J. Endocrinol. 2014, 2014, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Van Dam, P.S.; Cotter, M.A.; Bravenboer, B.; Cameron, N.E. Pathogenesis of diabetic neuropathy: Focus on neurovascular mechanisms. Eur. J. Pharmacol. 2013, 719, 180–186. [Google Scholar] [CrossRef]

{kind=link}
| Class of Chemotherapy Drugs | Drug Name | Neuropathy Incidence (%) (Classified by Neurotoxicity Degrees) | Reported Neurotoxic Doses |
|---|---|---|---|
| Anthracyclines | Doxorubicin (Adriamycin) | 75% (cognitive impairment “chemobrain”) [14] | - |
| Taxanes | Paclitaxel | All grades: 60% [15] Grade 3–4 motor: 11% Grade 3–4 sensory: 33% [16] | 1000 mg/m2 cumulative dose [17] |
| Docetaxel | All grades: 15% [15,18] Grade 3–4: 2% [18] | 400 mg/m2 cumulative dose [17] | |
| Platinum-based agents | Cisplatin | Grade 1:14–33% Grade 2: 0–33% Grade 3: 2–19% Grade 4: 0–4% [19] | 250–450 mg/m2, and all patients develop neuropathy [19,20], at cumulative dose of 500–600 mg/m2 [21] |
| Oxaliplatin | Grade 1: 21–94% Grade 2: 5–42% Grade 3–4: 3–19% [19,22] | >550 mg/m2 Severe neurotoxicity at cumulative dose of 750–850 mg/m2 [23] Chronic neuropathy with a cumulative dose between 850 mg/m2 and 1800 mg/m2 [19] | |
| Carboplatin | All grades: 4–6% [24] | >400 mg/m2 Neurotoxicity only with high doses or in combination with other drugs [20] | |
| Vinca alkaloids | Vincristine | Grade 1–2: 60% [15] | 30–50 mg [15,20] |
| Vinorelbine | All grades: 44% [25] Grade 3–4: ≈ 2% [26] | 125 mg/m2 [25] | |
| Antimetabolites | 5-fluorouracil (5-FU) | All grades: 0.6–7% [27,28] or 12.9% [29] Grade 3–4: 0% [29] | Uncertain [30] High doses and use of 5-FU in combined treatment, increase the risk of neuropathy [31] |
| Gemcitabine | All grades: 6% [32] | - | |
| Methotrexate | All grades: 3–10% [31] | - |
| Reference | Population Characteristics | Number of Patients | Type of Cancer and Chemotherapy Treatment | Measurement of Peripheral Neuropathy | Main Outcomes | |||
|---|---|---|---|---|---|---|---|---|
| DM | No DM | |||||||
| Bano and Ikram 2019 [39] | N | 38 | 6 | 32 | Colorectal cancer with metastasis Treatment: FOLFOX | Oxaliplatin Specific Neurotoxicity Scale (OSNS) [46] National Cancer Institute Common Toxicity Criteria 2.0 (NCI-CTC) [47] | It cannot be confirmed that PN induced by FOLFOX chemotherapy has a higher incidence in diabetics than in non-diabetics. However, dizziness is more common in diabetic cancer patients than in those without diabetes mellitus. Distal and transitory paresthesia after administration of oxaliplatin in patients with colorectal cancer are also more prevalent in the group of diabetic subjects. | |
| Country | Pakistan | |||||||
| Gender (%) | Unknown | |||||||
| Age (range) | Total: 20–80 | |||||||
| De la Morena Barrio et al. 2015 [36] | N | 129 | 43 | 86 | Breast cancer Treatment: paclitaxel | National Cancer Institute Common Toxicity Criteria (NCI-CTC) [47] | An increased incidence of PIPN was observed in women with breast cancer with diabetes mellitus. A substantial delay in recovery was also observed, as well as a greater frequency and severity of peripheral neurotoxicity in diabetic patients than in non-diabetic patients treated with this chemotherapy drug. | |
| Country | Spain | |||||||
| Gender (%) | ♀ | 100% | ||||||
| ♂ | 0% | |||||||
| Age (mean) | Total: 66 | |||||||
| DM: 66 | ||||||||
| No DM: 65.5 | ||||||||
| Kus et al. 2016 [40] | N | 374 | 81 | 293 | Any cancer Treatment: taxanes (docetaxel or paclitaxel) for one group and in combination with platinum for another group. | Neuropathic Pain Symptom Inventory (NPSI) [48] Clinical criteria | The incidence of PSN among cancer patients treated with taxanes was higher in patients with diabetes mellitus. The neuropathy rate was similar between non-diabetic and diabetics with less than 5 years of evolution, while those with diabetes of more than 5 years had higher neuropathy rates. The presence of diabetes with more than 5 years of evolution influences the incidence and severity of PSN in cancer patients treated with taxanes. | |
| Country | Turkey | |||||||
| Gender (%) | ♀ | 97% | ||||||
| ♂ | 3% | |||||||
| Age (n) | Total: <65 years: 337 ≥65 years: 37 | |||||||
| DM <65 years: 72 ≥65 years: 9 | ||||||||
| No DM <65 years: 265 ≥65 years: 28 | ||||||||
| Ramanathan et al. 2009 [41] | N | 3430 | 309 | 3121 | Colorectal cancer Treatment: FOLFOX, fluorouracil and leucovorin, or oxaliplatin | National Cancer Institute Common Toxicity Criteria (EFC2962 and MOSAIC) [47] and Oxaliplatin Specific Neurotoxicity Scale (EFC4584) [46]. | The presence of diabetes was not associated with an increased risk of developing PSN in any of the patients in the total sample. Diabetes did not affect the incidence, severity, and time to onset of peripheral neuropathy in patients with colon cancer treated with oxaliplatin. | |
| Country | Trials with different samples: 1. International (MOSAIC) 2. North American (EFC4584) 3. European (EFC2962) | |||||||
| Gender (%) | ♀ | 44.4% | ||||||
| ♂ | 55.6% | |||||||
| Age median | DM: 63 | |||||||
| No DM: 60 | ||||||||
| Uwah et al. 2012 [5] | N | 62 | 14 | 48 | Colorectal Cancer Treatment: oxaliplatin | National Cancer Institute Common Toxicity Criteria (NCI-CTC) [47] | No influence of diabetes mellitus on the severity of oxaliplatin-induced peripheral neuropathy was found. However, patients with diabetes developed neuropathy with a lower cumulative dose of oxaliplatin than non-diabetic patients. | |
| Country | United States | |||||||
| Gender (%) | ♀ | 50.2% | ||||||
| ♂ | 49.8% | |||||||
| Age (mean) | Total: 60.2 | |||||||
| Abdel-Rahman 2018 [42] | N | 756 | 64 | 692 | Colorectal cancer with metastasis Treatment: FOLFOX | Neurological symptoms | Diabetes did not affect the overall survival of patients with colorectal cancer treated with FOLFOX. However, diabetic patients appear to be more predisposed to developing oxaliplatin-induced peripheral neuropathy in a shorter time than non-diabetic patients, although diabetes did not influence the incidence or rate of recovery from peripheral nerve disease. | |
| Country | Unknown | |||||||
| Gender (%) | ♀ | 40.2% | ||||||
| ♂ | 59.8% | |||||||
| Age (mean) | Total: 60.5 | |||||||
| DM: 64.4 | ||||||||
| No DM: 60.1 | ||||||||
| Gogas et al. 1996 [43] | N | 33 | 33 | 0 | Celomic epithelial ovarian cancer Treatment: paclitaxel and/or cisplatin | National Cancer Institute Common Toxicity Criteria (NCI-CTC) [47] | The treatment of paclitaxel and cisplatin in combination, or paclitaxel alone, can be administered safely in diabetic patients using a standard dose and with simultaneous monitoring of blood glucose and creatinine. It must be accompanied by a previous study of the history of the patient’s neurological symptoms and a physical examination. | |
| Country | United States | |||||||
| Gender (%) | ♀ | 100% | ||||||
| ♂ | 0% | |||||||
| Age (mean) | Total: 61 | |||||||
| Vissers et al. 2015 [3] | N | 1193 | 218 | 975 | Colorectal cancer | European Organization for Research and Treatment of Cancer quality of life questionnaire-chemotherapy-induced peripheral neuropathy 20 (EORTC QLQ-CIPN20) [49] | Diabetic patients with colorectal cancer showed neuropathic symptoms more frequently than non-diabetic patients regardless of chemotherapy treatment, which suggests that diabetes mellitus rather than chemotherapy is the main factor responsible for neuropathic symptoms in colorectal cancer patients. | |
| Country | Netherlands | |||||||
| Gender (%) | ♀ | 33% | ||||||
| ♂ | 67% | |||||||
| Age (mean) | Total: 71 | |||||||
| DM: 71.3 | ||||||||
| No DM: 70.8 | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sempere-Bigorra, M.; Julián-Rochina, I.; Cauli, O. Chemotherapy-Induced Neuropathy and Diabetes: A Scoping Review. Curr. Oncol. 2021, 28, 3124-3138. https://doi.org/10.3390/curroncol28040273
Sempere-Bigorra M, Julián-Rochina I, Cauli O. Chemotherapy-Induced Neuropathy and Diabetes: A Scoping Review. Current Oncology. 2021; 28(4):3124-3138. https://doi.org/10.3390/curroncol28040273
Chicago/Turabian StyleSempere-Bigorra, Mar, Iván Julián-Rochina, and Omar Cauli. 2021. "Chemotherapy-Induced Neuropathy and Diabetes: A Scoping Review" Current Oncology 28, no. 4: 3124-3138. https://doi.org/10.3390/curroncol28040273
APA StyleSempere-Bigorra, M., Julián-Rochina, I., & Cauli, O. (2021). Chemotherapy-Induced Neuropathy and Diabetes: A Scoping Review. Current Oncology, 28(4), 3124-3138. https://doi.org/10.3390/curroncol28040273