This 55-year-old male patient was referred to our institution because of mild exertional dyspnoea. Surgical repair of an aortic root aneurysm with severe aortic regurgitation using a composite graft with a 27 mm mechanical bileaflet prosthesis had been performed 5 months earlier.
Transthoracic echocardiography showed partial annulo-aortic disconnection with formation of a pseudoaneurysm and systolic graft compression (Figure 1). The extent of disconnection and pseudoaneurysm formation was further demonstrated by transoesophageal echocardiography (Figure 2 and Figure 3).
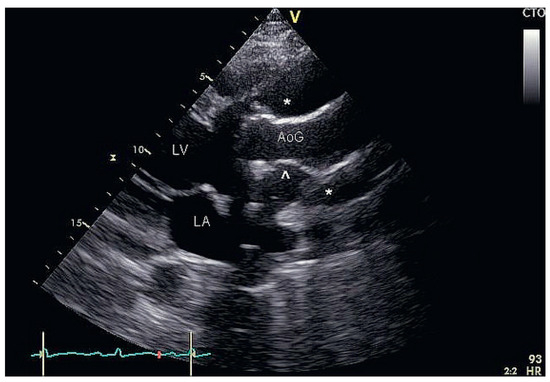
Figure 1.
(video A, You can find the videos on http://www.cardiovascmed.ch/for-readers/multimedia/). Transthoracic parasternal long axis view shows annulo-aortic disconnection resulting in a large pseudoaneurysm (asterisks) with systolic compression (arrow head) of the aortic graft (AoG) due to flow from the left ventricle (LV) into the pseudoaneurysm. LA = left atrium.
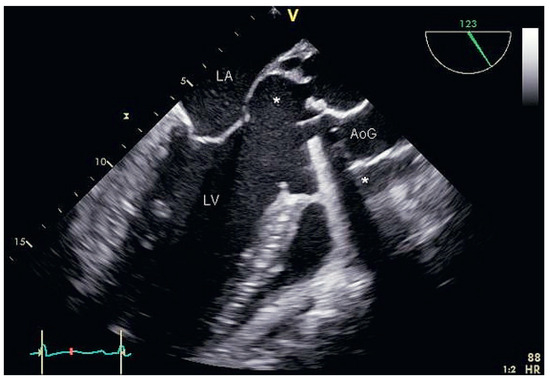
Figure 2.
(video B, You can find the videos on http://www.cardiovascmed.ch/for-readers/multimedia/). Transoesophageal long-axis view showing the extent of the pseudoaneurysm (asterisks).
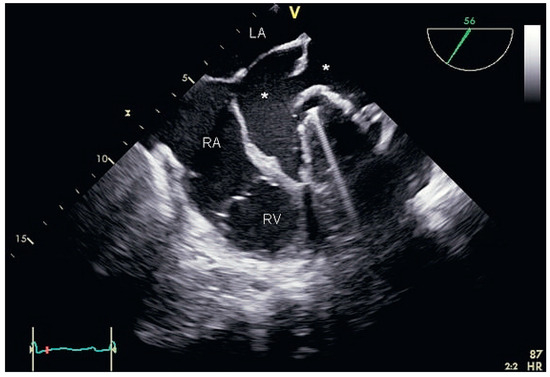
Figure 3.
(video C, You can find the videos on http://www.cardiovascmed.ch/for-readers/multimedia/). Transoesophageal short-axis view showing the extent of the pseudoaneurysm (asterisks).
Coronary angiography demonstrated dynamic systolic compression of the left main coronary artery within the pseudoaneurysm (Figure 4). The patient did not show any ischaemic symptoms, which can be explained by the fact that coronary flow during diastole, where most myocardial perfusion occurs, was not impaired (Figure 5).
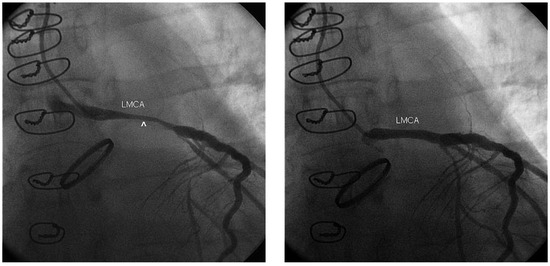
Figures 4 and 5.
(video D, You can find the videos on http://www.cardiovascmed.ch/for-readers/multimedia/). Blood flow into the pseudaneurysm resulted in dynamic systolic compression of the left main coronary artery (LMCA) within the pseudoaneurysm (arrow head in Figure 4), while diastolic coronary flow was not impaired (Figure 5).
The patient underwent successful reoperation with insertion of a 29 mm Medtronic Freestyle Aortic Root Heart Valve (intraoperative findings are shown in Figure 6). Examination of intraoperative tissue and blood cultures showed the presence of Propionibacterium acnes, and prosthetic endocarditis as the underlying cause of partial graft disconnection was diagnosed. Antibiotic therapy in accordance with resistance testing was administered.
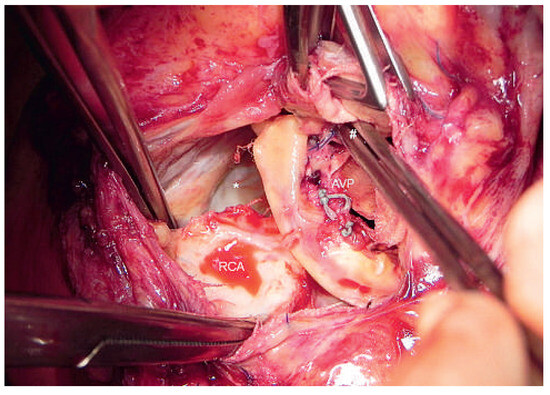
Figure 6.
Intraoperative findings after surgical opening of the aortic graft with the aortic valve prosthesis in situ. The annular dehiscence causing the large pseudaneurym (asterisk) is indicated by a forceps (hashtag). AVP = aortic valve prosthesis; RCA = right coronary artery.
Pseudoaneurysm formation of the ascending aorta is a well described, but rare, complication after composite graft surgery for combined disorders of the aortic valve and ascending aorta [1]. If this serious complication occurs, graft infection must be suspected. Propioni bacterium species are constituents of the normal human skin microflora. They are a very rare cause of endocarditis. A retrospective review revealed only a small number of published cases (70 patients, for 58 of them clinical details available). In 79% of the cases prosthetic material was involved, as was the case in our patient [2].
Funding/potential competing interests
No financial support and no other potential conflict of interest relevant to this article was reported.
References
- Barbetseas, J.; Crawford, E.S.; Safi, H.J.; Coselli, J.S.; Quinones, M.A.; Zoghbi, W.A. Doppler echocardiographic evaluation of pseudoaneurysms complicating composite grafts of the ascending aorta. Circulation. 1992, 85, 212–222. [Google Scholar] [CrossRef] [PubMed]
- Sohail, M.R.; Gray, A.L.; Baddour, L.M.; Tlejyeh, I.M.; Virk, A. Infective endocarditis due to Propionibacterium species. Clin Microbiol Infect. 2009, 15, 387–394. [Google Scholar] [CrossRef] [PubMed]
© 2014 by the author. Attribution - Non-Commercial - NoDerivatives 4.0.