A 79-year-old woman with chronic obstructive pulmonary disease and history of severe arterial hypertension was admitted to our hospital due to recurrent chest discomfort and dyspnea. There was no history of chest trauma.
The contrast-enhanced thoracic computed tomography on admission revealed a sub-acute aortic rupture (Figure 1A,B) at the base of the brachiocephalic trunk with subsequent false aneurysm.
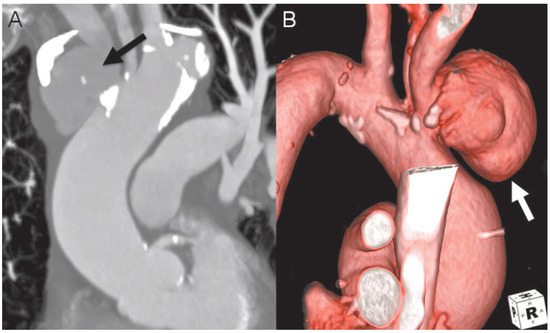
Figure 1.
Contrast-enhanced thoracic computed tomography with multi-planar reconstruction (A) and surface-rendering reconstruction (B) showing a sub-acute aortic rupture at the base of the brachiocephalic trunk (black arrow) with subsequent false aneurysm (white arrow).
Urgent surgery was performed using a cardiopulmonary bypass via arterial and venous femoral cannulation, the patient was cooled down to 28 °C (82 °F) bladder temperature and the sternum was opened. Aher deep hypothermic circulatory arrest was installed, the aorta was opened and antegrade cerebral perfusion catheters were introduced. We found a ruptured plaque at the base of the brachiocephalic trunk which subsequently had led to aortic rupture. The thickened wall of the false aneurysm including the base of the brachiocephalic trunk and the proximal part of the aortic arch were resected. An appropriately trimmed Gelweave™ grah (26 × 8 mm, Vascutek, UK) was anastomosed with an end-to-end technique (Figure 2A) and no additional grah was needed for replacement of the proximal brachiocephalic trunk. Aher de-airing, cardiopulmonary bypass was reinstalled via the Gelweave™ grah. During re-warming the prosthesis was anastomosed to the proximal part of the ascending aorta combined with a single venous bypass grah to the right coronary artery due to a relevant proximal stenosis shown in the pre-operative angiogram.
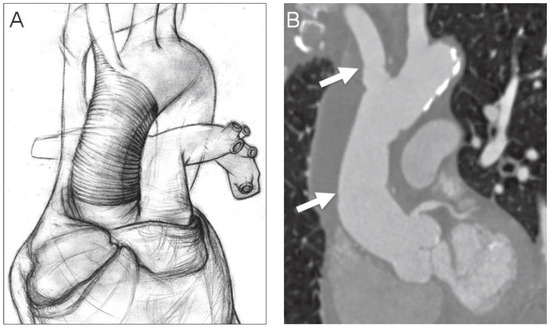
Figure 2.
A: Illustration of the repair technique showing the single Gelweave™ graft with two end-to-end anastomoses. B: Postoperative CT scan. White arrows mark the proximal and distal anastomosis of the prosthesis.
A postoperative CT scan (Figure 2B) revealed a good result. The early postoperative course was uneventful, however severe pre-existing obstructive pulmonary disease led to a delayed recovery of the patient.
Funding/Potential Competing Interests
No financial support and no other potential conflict of interest relevant to this article were reported.
© 2015 by the author. Attribution-Non-Commercial-NoDerivatives 4.0.