Transthoracic and transoesophageal echocardiography was performed on a 32-year-old, asymptomatic patient nine years after commissurotomy of a stenotic bicuspid aortic valve and supracoronary graft replacement of an aneurysmal ascending aorta. This exhibited increased continuous-wave (CW) Doppler-derived transaortic pressure gradients (max. / mean pressure differences 48/31 mm Hg, after correction for left ventricular outflow tract gradients; Figure 1), despite an aortic valve showing only mildly restricted opening (Figure 2 and Figure 3, videos A and B). Colour Doppler interrogation indicated supravalvular high-velocity flow, but no turbulent flow was seen in the left ventricular outflow tract or at the level of the aortic valve, indicating that the high gradients were not caused by stenosis at the subvalvular or valvular level (Figure 4 and Figure 5, videos C and D). Thoracic magnetic resonance (MR) angiography revealed a patent, but small-for-size 22-mm Dacron graft (Figure 6, video D).
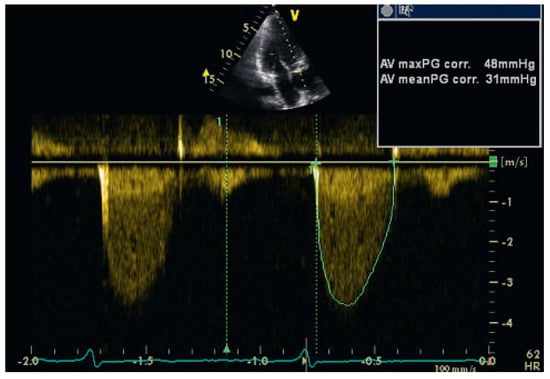
Figure 1.
Transthoracic echocardiogram showing the continuous-wave Doppler signal across the aortic valve recorded in the apical long-axis view. Doppler-derived velocities and gradients are considerably increased.
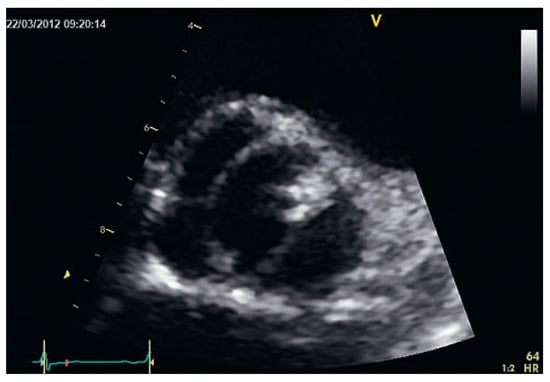
Figure 2 and video A.
Transthoracic basal short-axis view of the bicuspid aortic valve. In this view, only mildly restricted opening is seen.
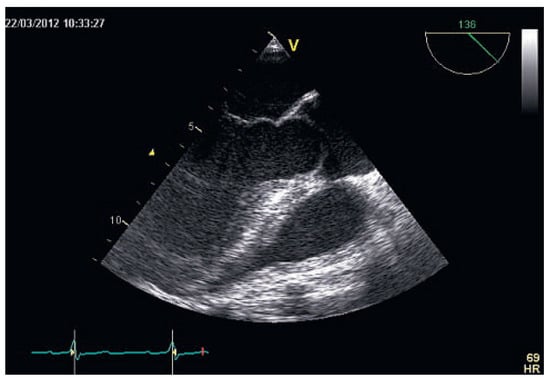
Figure 3 and video B.
Transoesophageal long-axis view showing the bicuspid aortic valve with typical systolic doming (Figure 3, video B) and asymmetric closure line (video B).
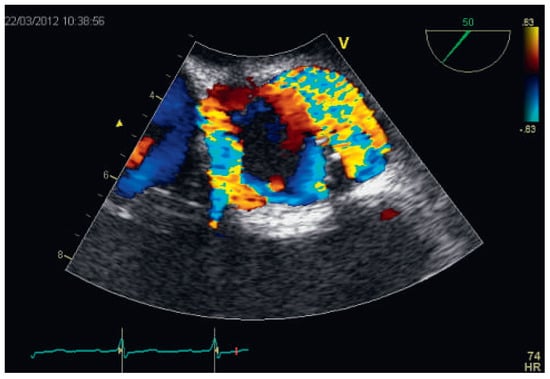
Figure 4 and video C.
Colour Doppler imaging recorded in the transoesophageal short-axis view reveals turbulent systolic flow in the sinus portion of the aorta, but not in the left ventricular outflow tract or at the level of the aortic valve (see also Figure 5). The video additionally shows presence of mild aortic regurgitation.
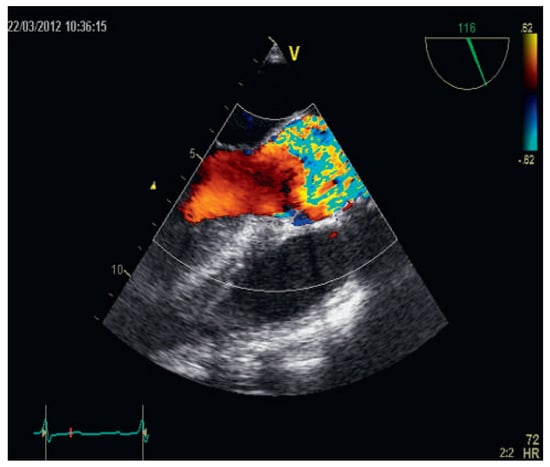
Figure 5 and video D.
Colour Doppler imaging recorded in the transoesophageal long-axis view reveals turbulent systolic flow in the sinus portion of the aorta, but not in the left ventricular outflow tract or at the level of the aortic valve (see also Figure 4). The video additionally shows presence of mild aortic regurgitation.

Figure 6 and video E.
Contrast-enhanced magnetic resonance angiography of the thoracic aorta shows ectasia of the aortic root, a patent 22-mm Dacron graft in the ascending aorta, and an enlargement of the ascending aorta distal to the graft (maximum diameter measured 41 mm).
Doppler echocardiography is widely used to assess cardiac valve function. Under- or overestimation of transvalvular gradients may occur with this technique. In the case presented, the observed transvalvular gradient overestimation is most likely of multifactorial genesis. The colour Doppler images showing high velocity turbulent flow in the aortic root suggest that the causative factors are mainly of supravalvular origin. Although MR imaging (MRI) of the thoracic aorta revealed no signs of graft obstruction, the noncompliant, small-for-size Dacron graft has almost certainly contributed to the increased Doppler gradients. Moreover, the pressure recovery phenomenon may have played an important role. Pressure recovery – the increase in pressure downstream from the valve caused by the reconversion of kinetic energy to potential energy – is a potential reason for gradient overestimation and, consequently, of valve area underestimation [1,2]. Usually, it can be neglected if the ascending aortic diameter exceeds 30 mm, but it has to be considered in the case of smaller diameters, such as in our patient due to the 22-mm graft.
To separate these two factors using echocardiography, and to evaluate their individual impact on Doppler measurements is challenging. One possibility, which was not performed in our case, would be the use of pulsed wave Doppler measurements within the graft with the high pulse repetition frequency (PRF) technique. However, it may be difficult to place the high PRF samples at an adequate interrogation angle and in such a way that only the flow within the graft would be interrogated.
This case shows that interpretation of elevated Doppler gradients across an aortic valve may be challenging. If implausibly high Doppler gradients are found, factors such as supravalvular obstruction or the pressure recovery phenomenon have to be considered.
Echo and MRI loops (AVI video files) can be viewed on the website of “Cardiovascular Medicine” http://www.cardiovascular-medicine.ch.
Author Contributions
CF wrote the initial manuscript. AB edited the manuscript. CH and AB performed echocardiography and made the diagnosis. All authors read and approved the final manuscript.
Funding / potential competing interests
No financial support and no other potential conflict of interest relevant to this article was reported.
References
- Garcia, D.; Pibarot, P.; Dumesnil, J.G.; Sakr, F.; Durand, L.G. Assessment of aortic valve stenosis severity: a new index based on the energy loss concept. Circulation 2000, 101, 765–771. [Google Scholar] [CrossRef] [PubMed]
- Bahlmann, E.; Cramariuc, D.; Gerdts, E.; Gohlke-Baerwolf, C.; Nienaber, C.A.; et al. Impact of pressure recovery on echocardiographic assessment of asymptomatic aortic stenosis: a SEAS substudy. JACC Cardiovasc Imaging. 2010, 3, 555–562. [Google Scholar] [CrossRef] [PubMed]
© 2013 by the author. Attribution - Non-Commercial - NoDerivatives 4.0.