Abstract
We report on the worldwide first implantation of a transcatheter valve in mitral position using a surgical approach to treat severe combined mitral valve disease, complicated by massive calcifications of the whole mitral anulus. The management of such calcification is demanding because prior to valve repair or replacement, “en bloc decalcification” followed by reconstruction of the annulus is necessary. This method is superior to passing sutures through the calcium which may end with perivalvular leakage and atrioventricular rupture. In this 81-year-old female, the “off-label” implantation of a transcatheter valve allowed to greatly accelerate the procedure and eliminate the risk of atrioventricular rupture. Postoperative function of the transcatheter valve was excellent and the patient underwent uneventful recovery.
Introduction
Surgical treatment of isolated mitral regurgitation has evolved from mitral valve replacement to repair, that produces superior long-term outcome. However, in some instances, mitral valve disease combines regurgitation and some degree of stenosis and is complicated by extensive calcification of the mitral valve annulus. Usually calcification involves the posterior annulus in a semi-circumferential pattern, but variable extension to the anterior part of the annulus and to a limited portion of the leaflet tissue may be observed.
The management of extensive mitral calcification is a surgical challenge. When mitral repair is planned, calcium may prevent plication of the annulus and safe fixation of an annuloplasty ring. On the other side, passing the sutures through the calcium to secure a ring or a prosthetic valve in case of mitral valve replacement may be hazardeous, since it carries the risk of calcium fragmentation, annular dehiscence, perivalvular leakage and atrioventricular rupture as the most serious complication. The technique of annular reconstruction was developed by David and Carpentier to minimise these potential complications: the main principles are “en bloc” decalcification and reconstruction of the annulus using living tissue or xeno-pericardium [1,2].
We report on the first surgical implantation of a transcatheter valve in mitral position to treat severe combined mitral valve disease, complicated by massive circular calcifications of the mitral annulus.
Case report
A 81-year-old female suffering from severe exertional dyspnoea and strong coughing episodes during night for several months was referred because of severe combined mitral valve disease. Personal previous history was uneventful regarding heart disease. Transthoracic echocardiography showed moderate mitral valve stenosis and severe regurgitation but transoesophageal echocardiography, which was possible using a paediatric probe only because of oesophageal narrowing, confirmed these main findings. In addition, echography demonstrated that the mitral valve annulus was calcified on the whole circumference as well as both leaflets. The coaptation zone between the anterior and posterior mitral leaflets was only 2 mm. The mean pressure gradient was 9 mm Hg, the opening valve area approximately 1.2 cm2. There was a large eccentric regurgitation jet over the posterior leaflet. The left atrium was enlarged with a end-systolic diameter of 50 mm. There was minimal central aortic regurgitation and LV function was slightly impaired with a systolic ejection fraction of 55%. Coronary angiography did not reveal significant coronary artery disease and confirmed the circular calcifications of the mitral leaflet (fig. 1).
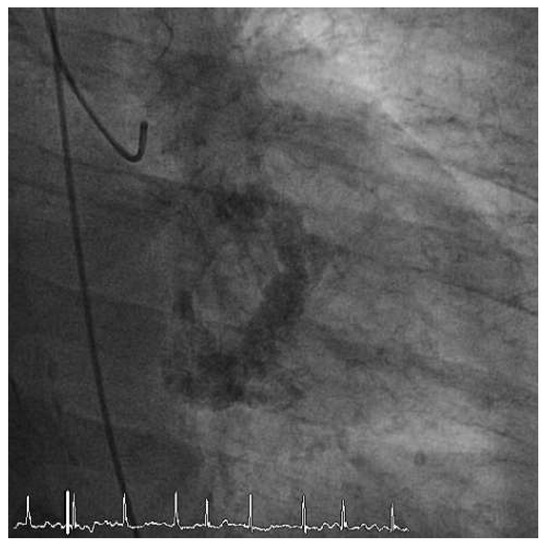
Figure 1.
Circular calcifications of the mitral valve annulus demonstrated before LV-angiography.
Surgery was performed through median sternotomy and cardiopulmonary bypass was conducted in moderate hypothermia. The mitral valve was approached through a left atriotomy. Inspection confirmed the massive calcifications of the valve leaflets and the anulus. Repair was not considered as an option, since combined stenosis and insufficiency were present. Following resection of the anterior and part of the posterior leaflets, the orifice was still very narrowed and a sizer of 19 mm only could be introduced through the orifice. The extent of calcifications was very deep into the myocardium and the papillary muscles. This would have required an extensive debridement and circular reconstruction of the annulus with xenopericardium.
To simplify and accelerate the procedure, we decided to replace the valve with a 26 mm transcatheter SAPIEN XT aortic valved stent. For this purpose, the mitral orifice was gently dilated using a 20 mm and then with a 24 mm balloon. Then the transcatheter SAPIEN valve was introduced in an antegrade way through the left atriotomy into the annulus (fig. 2A) and expanded under direct vision: after deployment of the valve into the calcified annulus, digital pulling on the valve did not allow to tear it out of the annulus; nevertheless the valve was fixed with 4 sutures to the atrial tissue adjacent to the annulus (fig. 2B). Water probe into the left ventricle demonstrated a slight paravalvular insufficiency at the level of the posterior commissure which was closed with an additional stitch. Left atrial appendage was closed and pulmonary vein ablation performed. Weaning from cardiopulmonary bypass was uneventful and the postoperative echocardiography showed a normal valve function with a mean pressure gradient of 2 mm Hg (fig. 3A–C). There was no obstruction nor protrusion of the SAPIEN valve into the left ventricular outflow tract. Chest X-ray before discharge showed normal position of the mitral valve implant (fig. 4A,B)
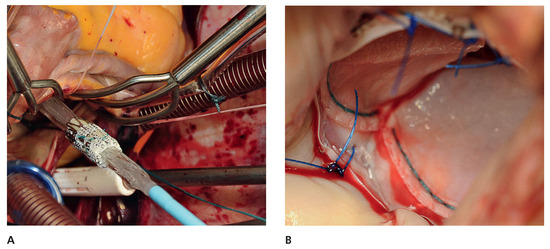
Figure 2.
Surgical introduction of the Sapien XT 26 mm valve mounted for antegrade transventricular use through the left atrial incision (A) and videoscopic view of the valve after attachment with polypropylene sutures to the atrial tissue close to the mitral annulus (B).
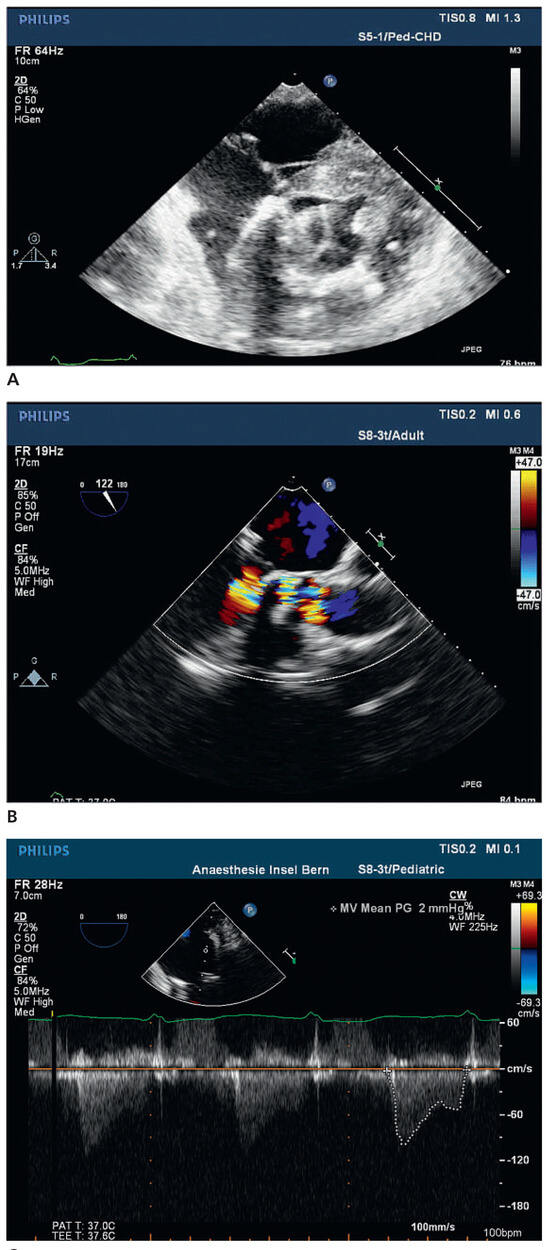
Figure 3.
3 Post-implantation echocardiography shows optimal position of the transcatheter valve in the mitral anulus by intraoperative epicardial (A) and postoperative TEE examination with unobstructed LVOTO and in the color doppler unobstructed flow to the aortic valve (B). Assessment of the transprothetic mean pressue gradient at the end of the procedure (C).
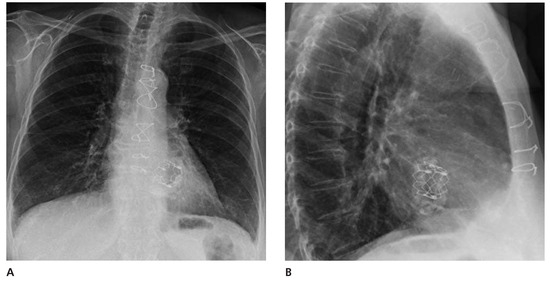
Figure 4.
Antero-posterior (A) and lateral (B) chest X-ray demonstrates position of the transcatheter Sapien valve.
Recovery was uneventful and the patient could be discharged on postoperative day 8. Echocardiography before discharge showed a normal function of the SAPIEN XT aortic valved stent in the mitral position. Four months after the procedure, the patient is doing very well: symptoms of heart failure have disappeared and the patient describes a better exercise capacity.
Comment
Massive calcification of the mitral valve annulus represents a major surgical challenge when mitral valve repair or replacement is considered. In the present patient, the calcifications extended to the whole circumference of the annulus, the leaflet tissue, and invaded the ventricular myocardium and the papillary muscles. Therefore the question was raised whether or not the calcium should be completely excised before valve replacement would be performed.
Usually, the annulus requires specific techniques of reconstruction, the surgical management of which proceeds in two steps: annular decalcification followed by anular reconstruction. Depending upon the extent of anular decalcification, three different techniques are used to restore atrioventricular continuity [1,2,3]:
- Direct reconstruction with the residual fibrous tissue using sutures without pledgets to avoid myocardial ischaemia by compression and reattaching the leaflet to be repaired.
- The sliding atrium technique to cover the myocardial area without fibrous tissue coverage. In this case the atrial edge is dissected from surrounding tissue to mobilise a 2–3 cm atrial rim that is used to cover the decalcified and exposed area of myocardium.
- Following large anular débridement extending to the underlying myocardium, use of a large patch of autologous or xenopericardium may greatly facilitate the annular reconstruction and avoid atrioventricular disconnection. Once the annulus has been reconstructed, the annuloplasty ring, a tissue valve or a mechanical heart valve prosthesis can be implanted and attached to the patch that covers the decalcified area.
In the patient described here, mitral valve reconstruction was not considered because of the combined etiology (stenosis and regurgitation) and because the calcifications were circumferentially invading the mitral annulus and involved the anterior and the posterior mitral valve leaflets. For this reason and in order to simplify the procedure, we decided to deploy a transcatheter aortic SAPIEN XT valved stent under direct vision into the mitral anulus. Assessment of the annulus size was the most difficult part of the procedure; after partial excision of the leaflets, we used first a sizer for surgical prothesis (19 mm) and then inflated gently 2 ballons (20 and 24 mm). Since inflation at 24 mm appeared to be safe under direct vision (no overstreching, no disruption of the annulus), we decided to implant a 26 mm valve. Due to the massive calcifications of the anulus, the latter had lost its typical oval shape and was looking more circular than usual.
Transcatheter mitral valve implantation has been already described in experimental animal models and in humans to treat degenerated tissue valves or failed annuloplasty with ring [4,5,6,7,8]. However implantation in a native mitral annulus has not been reported so far. Deployment was performed smoothly under direct vision and because no experience was available about self-expansion at lone fixation mechanism, the valve was secured with 4 sutures, 2 at the anterior and posterior portion of the annulus each.
Sutureless valve technology has been developed for aortic valve replacement and designed to simplify the procedure and to shorten ischaemic time during which the heart is arrested [9]. Some implants are already available on the market while others are still in development; however, there is no prosthetic implant for mitral position, yet. In this older female patient, the “offlabel” use of a transcatheter aortic valve allowed to significantly accelerate the procedure and to eliminate considerably the risk of atrio-ventricular rupture.
Since our team had experience with more than 500 TAVI procedures, we felt comfortable to apply this technology as an alternative for a difficult and risky mitral valve replacement. Postoperative function of the transcatheter valve was excellent and the patient underwent uneventful recovery. This approach may become a simpler a nd more expedient alternative for older patients in whom mitral valve replacement would necessitate a potentially dangerous decalcification of the mitral annulus.
Funding/potential competing interests
T. Carrel: conference fees from Edwards, Sorin Medtronic. P. Wenaweser: proctor for Edwards Life sciences and Medtronic Corevalve Inc. B. Eberle: lecture honoraria from Medtronic Corevalve Inc. S. Windecker: consulting fees from Medtronic and Edwards.
References
- Carpentier, A.F.; Pellerin, M.; Fuzellier, J.F.; Relland, J.Y. Extensive decalcification of the mitral valve annulus: pathology and surgical management. J Thorac Cardiovasc Surg. 1996, 111, 718–730. [Google Scholar] [CrossRef] [PubMed]
- David, T.E.; Feindel, C.M. Reconstruction of the mitral anulus. Circulation 1987, 76 (Suppl. III), III102–7. [Google Scholar] [CrossRef] [PubMed]
- Feindel, C.M.; Tufail, Z.; David, T.E.; Ivanov, J.; Armstrong, S. Mitral valve surgery in patients with extensive calcification of the mitral anulus. J Thorac Cardiovasc Surg. 2003, 126, 777–782. [Google Scholar] [CrossRef] [PubMed]
- Lozonschi, L.; Lutter, G. Transcatheter mitral valve stent implantation. EuroIntervention 2011, 9, 1036. [Google Scholar] [CrossRef] [PubMed]
- Lozonschi, L.; Bombien, R.; Osaki, S.; Hu, J.; Snell, D.; Edwards, N.M.; et al. Transapical mitral valved stent implantation: a survival series in swine. J Thorac Cardiovasc Surg. 2010, 140, 422–426. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Gurvitch, R.; Cheung, A.; Ye, J.; Wood, D.A.; Willson, A.B.; Toggweiler, S.; et al. Transcatheter valve-in-valve implantation for failed surgical bioprosthetic valves. J Am Coll Cardiol. 2011, 58, 2196–2209. [Google Scholar] [CrossRef] [PubMed]
- Montorfano, M.; Latib, A.; Chieffo, A.; Moshiri, S.; Franco, A.; Grimaldi, A.; et al. Successful percutaneous antegrade transcatheter valve-in-valve implantation in the mitral position. JACC Cardiovasc Interv. 2011, 4, 1246–1247. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Himbert, D.; Brochet, E.; Radu, C.; Iung, B.; Messika-Zeitoun, D.; Enguerrand, D.; et al. Transseptal implantation of a transcatheter heart valve in a mitral annuloplasty ring to treat mitral repair failure. Circ Cardiovasc Interv. 2011, 4, 396–398. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Martens, S.; Sadowski, J.; Eckstein, F.; Bartus, K.; Kapelak, B.; Sievers, H.H.; et al. Clinical experience with the ATS 3f Enable sutureless bioprosthesis. Eur J Cardio-Thorac Surg. 2011, 40, 749–755. [Google Scholar] [CrossRef] [PubMed][Green Version]
© 20212 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).