Case presentation
A 70-year-old lady presented to the emergency room due to palpitations. She reported occasional self-limiting tachycardias occurring for more than 15 years. Her past medical history was unremarkable otherwise. A 12-lead ECG obtained at presentation revealed a narrow complex tachycardia with a heart rate of 196 bpm (Figure 1). Intravenous administration of adenosine led to termination of the tachycardia (Figure 2). Following a pause of 2.2 seconds, an irregular atrial activity with irregular AV conduction started before spontaneously converting to sinus rhythm after a few minutes (Figure 3). The patient was admitted for a diagnostic electrophysiologic study and possible catheter ablation therapy. The following morning, she again complained about palpitations. A 12 lead ECG at that time showed a narrow complex tachycardia with irregular atrial activity and irregular AV conduction with a heart rate of 166 bpm (Figure 4).
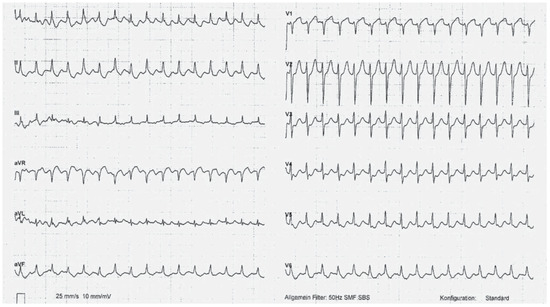
Figure 1.
12-lead ECG obtained at presentation to the emergency room.
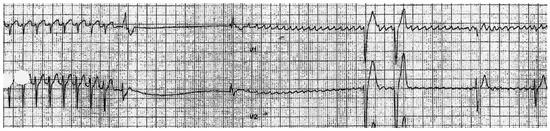
Figure 2.
Termination of tachycardia after administration of adenosin followed by the beginning of an irregular atrial activation with irregular AV conduction.
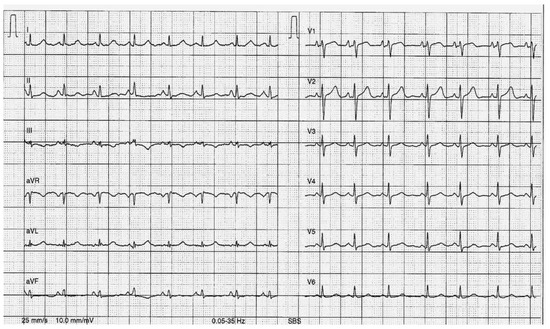
Figure 3.
12-lead ECG in Sinus rhythm.
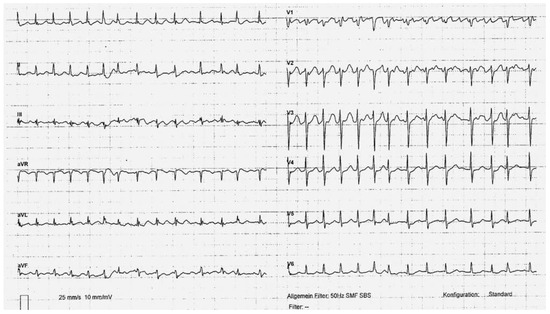
Figure 4.
12-lead ECG the next morning in the setting of another episode of palpitations.
What is your diagnosis? How should this patient be managed?
Figure 1 shows a regular narrow complex tachycardia with negative retrograde P-waves following the QRS complexes in the peripheral infero-lateral leads caused by a low-to-high activation of the atria. Figure 2 captures the events during administration of adenosine. After administration of adenosine, the tachycardia stops. Several effects of adenosine can be seen in this ECG sequence: the blocking effect of adenosine on the AV node leading to termination of the tachycardia, the suppressing effect on the Sinus node leading to an intermittent sinus arrest and finally the shortening of the atrial refractory period leading to atrial fibrillation, an effect not uncommonly observed with the administration of adenosine in the emergency room. Figure 3 depicts a normal sinus rhythm ECG of the patient described. There is no clear evidence of delta waves, a preexcited QRS complex with a negative delta wave in leads I and aVL can however not be ruled out (4th QRS complex). Figure 4 finally depicts atrial fibrillation with a rapid ventricular response.
A diagnostic electrophysiologic study was performed and showed normal AH- and HV-intervals. A narrow complex tachycardia with a rate of 175 bpm was induced by means of programmed atrial stimulation. Septal VA time was measured at 120 ms and eccentric activation in the coronary sinus was present with earliest activation being recorded at the distal coronary sinus electrodes. After ruling out atrial tachycardia with an entrainment maneuver from the ventricle, the diagnosis of an orthodromic atrioventricular reentrant tachycardia (AVRT) with a left free wall atrioventricular accessory pathway (AP) was made. During the electrophysiologic study, we found no evidence of antegrade conduction over the pathway. Ablation of the pathway by transseptal approach during tachycardia led to termination of the tachycardia and abolished conduction over the AP. The morning following the ablation, another self-limiting episode of atrial fibrillation (AF) was recorded.
Discussion
Patients with an atrioventricular AP have an increased risk of up to 30% for developing AF [1]. The mechanisms discussed for the association of these two arrhythmias include spontaneous degeneration of AVRT into AF, electric properties of the AP, effects of the AP on atrial architecture and intrinsic atrial muscle vulnerability [2]. In patients with antegrade AP conduction, AF represents a potentially life threatening arrhythmia due to the risk of induction of ventricular fibrillation. Successful AP ablation may substantially reduce the risk for subsequent AF. The recurrence rate of AF after successful ablation of an AP however shows an age-related increase: it seems to be low in patients younger than 50 years (12% over 2 years), but significantly higher in older patients (35% in patients older than 50 years and 55% in patients older than 60 years) [3].
These observations should be taken into account when making decisions about AF management in patients after successful AP ablation. In young patients with otherwise structurally normal hearts, AF is most likely related to the AP and no medical treatment seems warranted given the low risk of AF recurrence. In elderly patients such as the one described in this case however, medical treatment should be tailored according to current AF guidelines [4]. In our patient, echocardiography showed a normal ejection fraction and a moderately dilated left atrium. Given the above considerations, her echocardiographic findings and the CHA2DS2-VASc-Score of 2 points, oral anticoagulation therapy for stroke prevention and betablocker therapy for rate control were started. Holter monitoring after 3 and 6 months of follow-up revealed short episodes of atrial bursts, but no further manifest episodes of paroxysmal AF so far.
In conclusion, if AF occurs in the presence of an accessory pathway, AF may be eliminated by abolishing conduction over the pathway in some, but not all patients.
Funding/potential competing interests
No financial support and no other potential conflict of interest relevant to this article were reported.
References
- Schwieler, J.H.; Zlochiver, S.; Pandit, S.V.; Berenfeld, O.; Jalife, J.; Bergfeldt, L. Reentry in an accessory AV pathway as a trigger for AF initiation in manifest WPW syndrome: a matter of reflection? Heart Rhythm. 2008, 5, 1238–1247. [Google Scholar] [CrossRef] [PubMed]
- Centurión, O.A.; Shimizu, A.; Isomoto, S.; Konoe, A. Mechanisms for the genesis of paroxysmal atrial fibrillation in the Wolff Parkinson-White syndrome: intrinsic atrial muscle vulnerability vs. electrophysiological properties of the accessory pathway. Europace. 2008, 10, 294–302. [Google Scholar] [CrossRef] [PubMed]
- Dagres, N.; Clague, J.R.; Lottkamp, H.; Hindricks, G.; Breithardt, G.; Borggrefe, M. Impact of radiofrequency catheter ablation of accessory pathways on the frequency of atrial fibrillation during long-term follow-up; high recurrence rate of atrial fibrilltion in patients older than 50 years of age. Eur Heart J. 2001, 22, 423–427. [Google Scholar] [CrossRef] [PubMed]
- European Heart Rhythm Association; European Association for CardioThoracic Surgery. Camm, A.J.; Kirchhof, P.; Lip, G.Y.H.; Schotten, U.; Savelieva, I.; Ernst, S.; et al. Guidelines for the management of atrial fibrillation. Eur Heart J. 2010, 31, 2369–2429. [Google Scholar]
© 2012 by the author. Attribution - Non-Commercial - NoDerivatives 4.0.