Case presentation
A 53-year-old woman patient presented with multiple episodes of syncope occurring at rest, associated with chest pain. These episodes had been recurring approximately every two days for the previous month. Her medical history was unremarkable, apart from active smoking, and the physical examination was normal. The resting ECG was normal. During a 24-hour Holter recording the patient experienced malaise preceded by chest pain (see Figure 1).
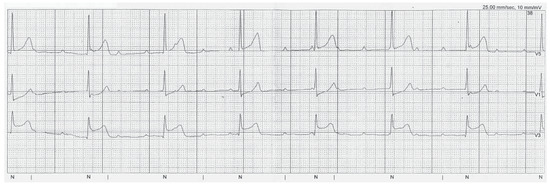
Figure 1.
Holter recording showing complete atrioventricular block corresponding to the clinical episode of chest pain and malaise.
Question
What is the most likely aetiology of the atrioventricular block?
Commentary
The Holter recording showed complete atrioventricular (AV) block with AV dissociation and a junctional escape rhythm at 37 bpm (Figure 1). The conduction disorder was accompanied by ST-segment elevation, which was absent during an asymptomatic period (Figure 2). This finding, along with the concomitant chest pain occurring at rest in a smoker, strongly suggests variant (Prinzmetal) angina as trigger for the conduction disorder, most probably secondary to spasm of the right coronary artery which supplies the AV node in about 90% of patients. A coronary angiogram was performed and revealed the presence of non-significant plaques on the right, anterior descending and circumflex coronary arteries. Cold-pressor and hyperventilation tests were performed during the coronary angiogram and did not show evidence of spasm. Nifedipine 30 mg/d was prescribed, and the patient remained asymptomatic during a 3-month follow-up despite continuing smoking (albeit at reduced levels).
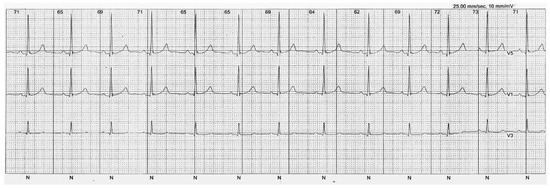
Figure 2.
Holter recording during an asymptomatic period.
Prinzmetal (otherwise known as variant) angina was first described in 1959 [1]. This syndrome may be associated with myocardial infarction and life-threatening cardiac arrhythmias, including ventricular tachycardia/fibrillation (which we previously reported in this journal [2]) and complete atrioventricular block [3,4]. Pharmacological treatment (calcium channel blocking agents and long-acting nitrates) and cessation of smoking may be effective in preventing or at least reducing coronary spasm recurrence. Stenting of the coronary arteries is usually not necessary, as clinical response to drug therapy and smoking cessation is usually favourable. Furthermore, coronary spasm may be multivessel or migratory, suggesting that the exact site of the spasm must be clearly identified before stent implantation, usually with provocative tests [3,5]. Nevertheless, there have been case reports of a favourable effect of stenting in patients with drug-refractory variant angina [6,7].
In our patient a pacemaker was not implanted in view of the reversible cause of AV block and favourable response to medical therapy.
Funding
No financial support.
Conflicts of Interest
no other potential conflict of interest relevant to this article was reported.
References
- Prinzmetal, M.; Kennamer, R.; Merliss, R.; Wada, T.; Bor, N. Angina pectoris. I. A variant form of angina pectoris; preliminary report. Am J Med. 1959, 27, 375–388. [Google Scholar] [CrossRef] [PubMed]
- Noble, S.; Carballo, D.; Burri, H. Malignant arrhythmia associated with chest pain and a diagnosis of myocarditis. Cardiovasc Med. 2011, 14, 27–28. [Google Scholar]
- Onaka, H.; Hirota, Y.; Shimada, S.; Kita, Y.; Sakai, Y.; Kawakami, Y.; et al. Clinical observation of spontaneous anginal attacks and multivessel spasm in variant angina pectoris with normal coronary arteries: evaluation by 24-hour 12-lead electrocardiography with computer analysis. J Am Coll Cardiol. 1996, 27, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Miller, D.; Waters, D.; Szlachcic, J.; Theroux, P. Clinical characteristics associated with sudden death in patients with variant angina. Circulation. 1982, 66, 588–592. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, H.; Lee, J.D.; Yamamoto, M.; Satake, K.; Tsubokawa, A.; Kawasaki, N.; et al. Induction of coronary artery spasm by combined cold pressor and hyperventilation test in patients with variant angina. J Cardiol. 1994, 24, 257–261. [Google Scholar] [PubMed]
- Khitri, A.; Jayasuriya, S.; Habibzadeh, M.R.; Movahed, M.R. Coronary stenting in patients with medically resistant vasospasm. Rev Cardiovas Med. 2010, 11, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, A.; Morino, Y.; Ikari, Y. Stent implantation for diffuse and multiple coronary spasm in a patient with variant angina refractory to optimal medical therapy. J Invasive Cardiol. 2007, 19, E320–E323. [Google Scholar] [PubMed]
© 2012 by the author. Attribution - Non-Commercial - NoDerivatives 4.0.