A 54-year-old man was hospitalised because of an inferior ST-elevation myocardial infarction. The vital signs of the patient on admission were: normal blood pressure, sinustachycardia and oxygen saturation 97% while breathing oxygen.
The electrocardiogram (ECG) on admission showed a sinustachycardia, ST-segment elevations inferior. His medical history consisted of chronic obstructive pulmonary disease (COPD), alcohol abuse, arterial hypertension and a pulmonary embolism in 1995.
The coronary angiography showed, as the culprit lesion, a relevant proximal stenosis of the arteria coronary dextra which was stented with a drug-eluting stent. A coronary aneurysm of the left circumflex coronary artery (LCX) with normal blood flow was shown (Figure 1) and left untreated. The patient was treated with aspirin, clopidogrel and a GPIIb/IIIa-antagonist for 4 hours. The follow-up echocardiography after 2 months showed a hypokinetic segment inferior. The aneurysm could not be represented.
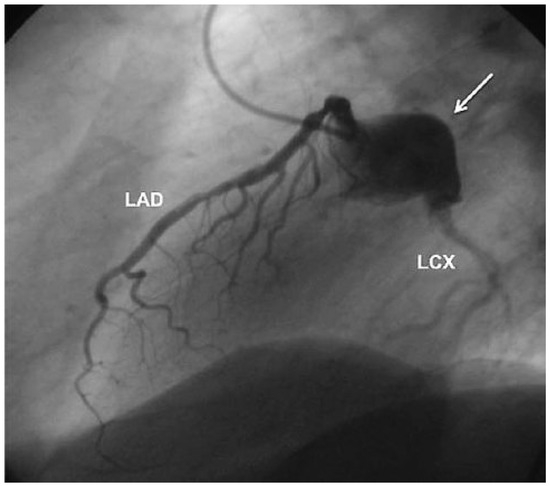
Figure 1.
Coronary angiogram. Coronary aneurysm of the left circumflex coronary artery (arrow) with normal blood flow. LAD = left anterior descending artery; LCX = left circumflex coronary artery.
One and a half years later, the patient presented to his general practitioner with reoccurring progressive chest pain, which had been occurring for 8 days. The ECG showed an inferior ST-elevation with positive cardiac biomarkers. The coronary angiography showed a complete thrombotic obstruction of the LCX within the known coronary aneurysm (Figure 2) which was dilated with balloons (Figure 3) and finally stented with covered stents (Jomed 4.0 × 16 mm). The patient was treated afterwards with aspirin, clopidogrel, eptifibatid for 24 hours and heparin in therapeutic dosage.
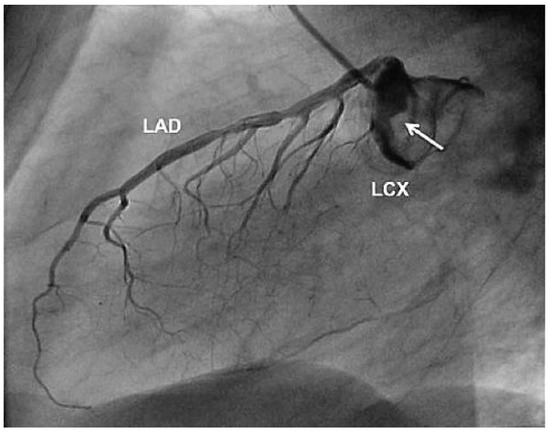
Figure 2.
Complete thrombotic obstruction of the left circumflex coronary artery (LCX) and partial obstruction of the coronary aneurysm (arrow). LAD = left anterior descending artery.
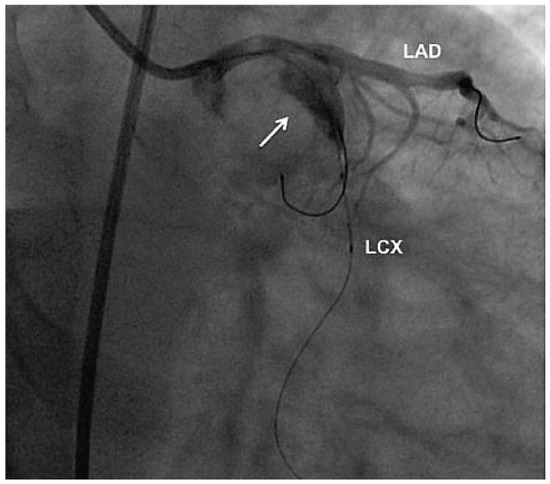
Figure 3.
Percutaneous coronary intervention. Balloon angioplasty and implantation of covered stents into the thrombotic obstruction of the aneurysm (arrow) and left circumflex coronary artery (LCX). LAD = left anterior descending artery.
Three months later the patient was asymptomatic. The control coronary angiography showed a well perfused LCX with open covered stents (Figure 4).
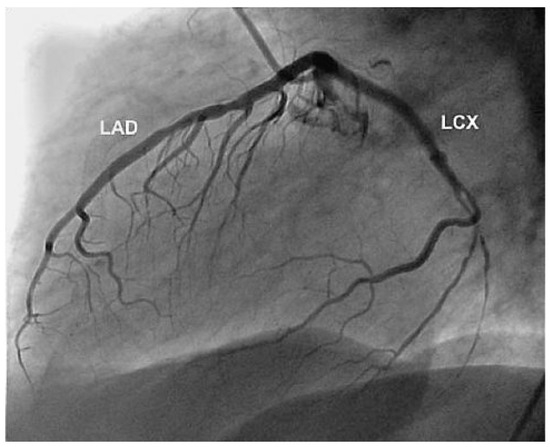
Figure 4.
Result 3 months later. Open covered stents and normal flow of the left circumflex coronary artery (LCX). LAD = left anterior descending artery.
Coronary aneurysms are rare. Based on multiple angiographic studies, its overall incidence varies between 0.15–4.9% [1].
At present, an aneurysm, including coronary aneurysm, is described as dilation of blood vessel lumen, exceeding the diameter of the adjacent normal segment more than 1.5-fold [2]. The right coronary artery is the most commonly affected (40–87%), followed by the left circumflex or left anterior descending artery [3]. Aneurysm of the saphenous vein coronary artery bypass graft has been described in a case report [4]. The etiologies of coronary aneurysm are diverse: Atherosclerosis has been estimated for 50% of the cases, congenital in 20–30%. Inflammatory and connective tissue disorders have also been associated with coronary aneurysm. Most known is the association with Kawasaki disease. The natural history of coronary aneurysms may be complicated by thromboembolism, rupture, or vasospasm. Baman and colleagues [5] analysed over 30,000 angiograms retrospectively with matched controls and found no association between aneurysm size and multiple variables including age, sex, survival rate, obstructive atherosclerotic coronary artery disease, hypertension, hyperlipidaemia, or diabetes. Patients with aneurysms have a 5-year mortality rate of 29.1%, irrespective of concomitant coronary artery disease.
Treatment options consist of surgical, percutaneous and medical approaches. In adults, surgical management is favoured as the therapeutic option, and it normally includes bypass grafting. Covered stents effectively seal the aneurysm and offer a safe and less invasive alternative in the treatment of large coronary aneurysms [6]. One large retrospective study compared patients treated either surgically or with polytetrafluoroethylene (PTFE) covered stents [7]. The authors suggest that these stents should be limited to patients whose aneurysms are <10 mm in diameter because of a greater re-stenosis risk. Regarding medical management, it generally consists of antiplatelet and/or antithrombotic agents.
This case illustrates a large coronary aneurysm of the LCX which was successfully treated by covered stents and showed no re-stenosis at 3 months followup. An inflammatory cause could not be identified; therefore we concluded that atherosclerosis was the underlying aetiology.
Conflicts of Interest
No conflict of interest to disclose.
References
- Befeler, B.; Aranda, J.M.; Embi, A.; et al. Coronary artery aneurysms. Study of their etiology, clinical course and effect on left ventricular function and prognosis. Am J Med. 1977, 62, 597–607. [Google Scholar] [CrossRef]
- Syed, M.; Lesch, M. Coronary artery aneurysm: a review. Progr Cardiovasc Dis. 1997, 40, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Villines, T.C.; Avedissian, L.S.; Elgin, E.E. Diffuse nonatherosclerotic coronary aneurysms. Cardiol Rev. 2005, 13, 309–311. [Google Scholar] [CrossRef] [PubMed]
- Jamshidi, P.; Resink, T.; Erne, P. Staged stenting of a long aneurysm of a saphenous vein coronary artery bypass graft. J Invasive Cardiol. 2008, 20(1), E1–E5. [Google Scholar] [PubMed]
- Baman, T.S.; Cole, J.H.; Devireddy, C.M.; et al. Risk factors and outcomes in patients with coronary artery aneurysms. Am J Cardiol. 2004, 93, 1549–1551. [Google Scholar] [CrossRef] [PubMed]
- Jamshidi, P.; Mahmoody, K.; Erne, P. Covered stents: a review. Int J Cardiol. 2008, 130(3), 310–318. [Google Scholar] [CrossRef] [PubMed]
- Szalat, A.; Durst, R.; Cohen, A.; Lotan, C. Use of polytatrafluoroethylenecovered stent for treatment of coronary artery aneurysm. Catheter Cardiovasc Interv. 2005, 66, 203–208. [Google Scholar] [PubMed]




© 2010 by the author. Attribution - Non-Commercial - NoDerivatives 4.0.