Case report
A 61-year-old lady was admitted to the emergency department because of atypical chest pain lasting for several days. Her ECG on admission is shown in Figure 1. After cardiac troponin level was found to be normal, she was discharged. Because she was a smoker and had a positive family history for coronary artery disease, an exercise stress test (EST) was scheduled some days later. Her ECG obtained immediately before the EST is shown in Figure 2.
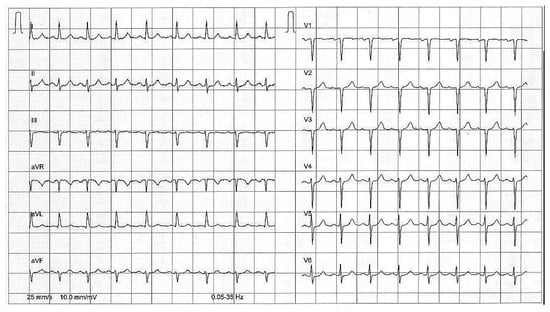
Figure 1.
Standard 12-lead ECG obtained in the emergency department showing sinus tachycardia and left axis deviation of the QRS complex in the frontal plane.
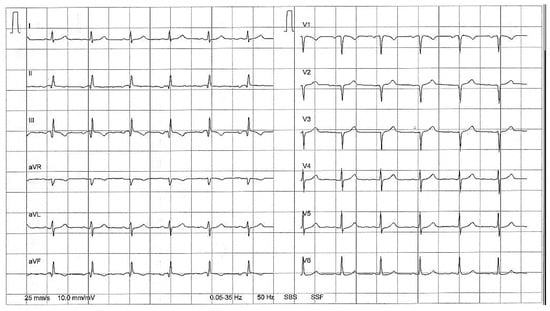
Figure 2.
Modified 12-lead ECG obtained immediately before the exercise test revealing Q waves in II, III, and aVF, and discordant T waves in III and aVF.
(1.) What happened in between the registration of the two ECGs, and (2.) what should be done?
Explanatory answers
The ECG in Figure 1 shows sinus tachycardia (105 bpm), left axis deviation, and normal repolarisation. In contrast, the ECG in Figure 2 reveals Q waves in leads II, aVF and most prominently in III and discordant T waves in leads III and aVF, which could be interpreted as a previous inferior myocardial infarction. In contrast to the ECG shown in Figure 1, there is a more rightward mean QRS axis. As the ECG was normal a few days ago, and the patient had continued chest pain, the ECG finding could represent a subacute stage of a myocardial infarction. As a consequence, transthoracic echocardiography was urgently performed, showing completely normal systolic left ventricular function without wall motion abnormalities especially in the inferior wall. Of note, the ECG shown in Figure 2 was performed while the patient was in standing position on the treadmill before EST. A subsequent ECG obtained in the supine position was very similar to that obtained in the emergency department. In particular, Q waves were absent, and T waves were concordant (Figure 3). During exercise, the patient had not complaints, and no ST segment changes were observed.
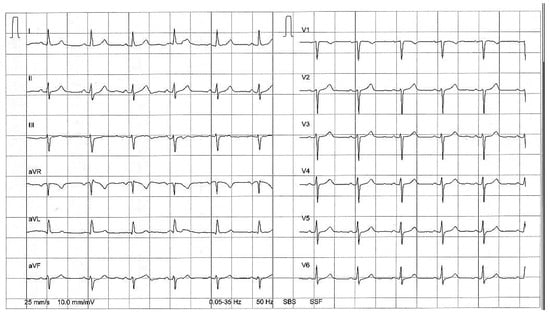
Figure 3.
Standard 12-lead ECG obtained in the supine position without Q waves.
To reduce motion artefacts during exercise testing, the standard 12-lead ECG is modified with moving the extremity electrodes towards the torso, which results in a right axis shift of the mean QRS axis, increased voltage in II, III, and aVF and reduced voltage in leads I and aVL. The more the leg electrodes are placed towards the body, the greater the degree of change [,]. In addition, the axis of the heart is influenced by postural changes and respiration. In the present case, not only Q waves but also discordant T waves occurred in the standing position with the modified 12-lead ECG, mimicking an older inferior myocardial infarction. Interestingly, a recent study found that ECGs obtained in the supine, sitting, and standing position do not significantly differ, leading to the conclusion that ECGs in these three positions are interchangeable []. However, some exceptions do obviously exist as illustrated by the present case.
References
- Kleiner, J.P.; Nelson, W.P.; Boland, M.J. The 12-lead electrocardiogram in exercise testing. A misleading baseline? Arch Intern Med. 1978, 138, 1572–1573. [Google Scholar] [CrossRef] [PubMed]
- Papouchado, M.; Walker, P.R.; James, M.A.; Clarke, L.M. Fundamental differences between the standard 12-lead electrocardiogram and the modified (Mason-Likar) exercise lead system. Eur Heart J. 1987, 8, 725–733. [Google Scholar] [CrossRef] [PubMed]
- Madias, J.E. Comparability of the standing and supine standard electrocardiograms and standing sitting and supine stress electrocardiograms. J Electrocardiol. 2006, 39, 142–149. [Google Scholar] [CrossRef] [PubMed]
© 2007 by the authors. Attribution—Non-Commercial—NoDerivatives 4.0.