Highlights
Public health relevance—How does this work relate to a public health issue?
- Having a caregiver with high vulnerability and complex needs can negatively impact child development, particularly during the early years of life.
Public health significance—Why is this work of significance to public health?
- Home visiting interventions can improve caregiver outcomes and, in turn, the caregiving environment.
- Improvements in the caregiving environment can positively impact child health and development.
Public health implications—What are the key implications or messages for practitioners, policy makers and/or researchers in public health?
- While home visiting interventions were found to improve a range of caregiver outcomes no one intervention was suitable to address all the varied needs of caregivers with high vulnerability and complex needs.
- Given the limited number of studies on each intervention and the inclusion of primarily female caregivers in participant samples, more research with diverse samples, notably male caregivers, is required.
Abstract
Past reviews have found home visiting interventions to be successful at improving caregiver outcomes. Though, no review has looked specifically at the effect of home visiting interventions on caregivers with high vulnerability and complex needs. This review aimed to examine and synthesis the literature on the impact of home visiting programs administered to caregivers with young children, high vulnerability and complex needs by professionals/paraprofessionals. Interdisciplinary databases, reference lists, and the Home Visiting Evidence of Effectiveness database were searched for articles that fit the inclusion criteria. Together searches resulted in a total of 623 articles, 34 of these articles were included in the final review, all from high-income countries. Twenty-five interventions were implemented across the 34 studies. Findings showed that these interventions were effective at improving a range of mental health, parenting, and family violence outcomes in caregivers with high vulnerability and complex needs. However, weighted mean standardized effect sizes ranged from 0.01–0.24 (small effect), with only one (i.e., practical parenting skills) of the five significantly different from 0 (standardized mean difference 0.24; 95% CI: 0.10, 0.38; z = 3.39, p = 0.00) and results favoring the control group. Missing information together with considerable variation in interventions, meant that identifying a clear pattern in treatment components that lead to effective verses non-effective interventions was not possible. Further research is therefore needed to assess the effectiveness of these interventions. Trial registration: The University of York Centre for Reviews and Dissemination (PROSPERO) registration number CRD42023460366.
1. Introduction
It is well recognised that having a caregiver who experiences high vulnerability and/or has complex needs (i.e., a caregiver with substance abuse difficulties, mentally ill health, family violence, and/or a child protection history) can have negative impacts on a child’s development [1]. This is especially the case during the early years (i.e., 0–5 years), a critical period for brain and neural development, and a time during which caregivers provide the primary care environment for a child [1,2,3,4]. Addressing caregiver mental health, psychosocial needs, and child maltreatment risk during the early years can have positive outcomes on child health and development [5,6]. Home visitation interventions are one approach administered with families who have high vulnerability and/or complex needs and young children to improve both caregiver and child health outcomes [7,8,9].
Home visiting interventions focused on families who are seen to have high vulnerability and/or complex needs are generally offered during the perinatal period, with families able to stay in the program until the child is around two to five years of age [8,9]. The term “home visiting” broadly refers to programs delivered in a home environment and therefore interventions can differ based on their objectives, population of interest, and duration of intervention [10]. There can also be differences in terms of the individuals delivering the program, with home visitors ranging from a single health professionals to teams of professionals, paraprofessionals (i.e., workers who have training in home visiting though are not registered health professionals), and/or unpaid trained laypersons (i.e., volunteer home visitors).
Numerous reviews evaluating the impact of home visiting interventions on families of young children have largely showed positive effects on parental health, attitudes, and behaviours (e.g., [10,11,12,13]). These reviews, however, have not focus exclusively on caregivers who have young children and experience high vulnerability and complex needs. Less is therefore known about what effect home visiting interventions may have on this high-risk population.
2. Aim
The aim of the current systematic meta-analytic review was to synthesise and evaluate the literature on caregiver outcomes following the delivery of home visiting interventions to families who have young children and also experience high vulnerability/complex needs. For this review, this included caregivers who experience substance abuse difficulties, mentally ill health, family violence, and/or child protection issues. The review focused on programs delivered by health professionals and/or paraprofessionals. All included studies were synthesised narratively. To get the most precise estimate of the interventions impact, meta-analyses’ were used to calculate pooled effect sizes. Given the considerable variation in home visiting programs and outcomes assessed it was not possible to undertake one meta-analysis, thus independent meta-analyses were undertaken for each outcome.
The aim of this review was to address following research questions:
- What home-visiting interventions have been administered with caregivers who have young children and high vulnerability/complex needs?
- What impacts (primary or secondary) do home-visiting interventions have on caregiver mental health, psychosocial wellbeing, and parenting practices for caregivers with young children and high vulnerability/complex needs?
3. Method
This review was registered with the University of York Centre for Reviews and Dissemination (PROSPERO; CRD42023460366). The study protocol was focused on both caregiver and child outcomes, however, given the large volume of literature identified, the authors made the decision to divide the results into two separate reviews- a review on caregiver outcomes and a review on child outcomes [14]. This paper presents the results pertaining to caregiver outcomes.
3.1. Search Strategy
The Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines [15] informed the undertaking of both systematic review and meta-analysis. To identify the relevant literature three search strategies were employed: (1) interdisciplinary research databases PsychInfo, Scopus, Embase, PubMed, and CINAHL were searched for studies from database inception up to August 2023 (see Supplementary Table S1 for the exact search terms used in each database); (2) reference lists of studies included in this review were searched manually; (3) the Home Visiting Evidence of Effectiveness (HomVEE) 2023 review and database were searched to identify interventions that were consistent with the inclusion criteria [16].
3.2. Inclusion and Exclusion Criteria
Articles were included if they: (1) administered a home visiting intervention; (2) included participants who were pregnant and/or families/caregivers of young children (children aged 0–4 years 11 months or the average study sample age was below 5.5 years); (3) had a sample comprised of caregivers experiencing mentally ill health, substance issue difficulties, family violence, and/or child protection issues; (4) were available in English; and (5) evaluated, using either a standardised measure or qualitative feedback, outcomes related to caregiver mental health, psychosocial needs, and/or parenting practices (i.e., behaviours that parents engage in to care for their child). Of note, while a home visiting intervention had to be administered and a caregiver outcome evaluated, the intervention did need to be specifically designed to target caregiver outcome. That is, the caregiver outcome could have been measured as a secondary outcome.
Articles were excluded if: (1) were not data-based (e.g., books, theoretical papers, reviews); (2) were unpublished dissertations/theses; (3) reported on individual case studies; (4) did not report on caregiver outcomes (i.e., only reported child outcomes); (5) were focused on clinical medical home interventions only; (6) only reported on physical health or birth outcomes; or (7) volunteers administered the home visiting intervention. In cases where it was unclear who delivered the intervention (e.g., the term “home visitor” or “health visitor” was used), intervention manuals and/or websites were searched to determine who generally administered the intervention. Articles were included in the review when it was clear that they were commonly administered by professionals or paraprofessionals. Studies were also excluded if they indicated that the home visiting intervention was delivered by a combination of professionals/paraprofessionals and volunteer home visitors but did not stratify results based on who administered the intervention.
3.3. Quality Assessment and Data Analysis
Randomised control trials (RCTs) were evaluated using The Cochrane Collaboration Risk of Bias Assessment Tool [17]. The tool includes seven criteria used to evaluate risk of bias. Each criterion is rated as either low risk (low risk of any bias affecting results), unclear risk (uncertainty about whether the bias will impact results), or high risk (the bias could markedly impact results). Ratings are then used to determine a study’s overall bias risk. Two reviewers individually evaluated each study’s risk of bias then came together to discuss and resolve discrepancies as well as determine the studies’ overall bias risk. Upon discussion, reviewers concluded that achieving participant and professional/paraprofessional blinding was difficult due to the nature of home visiting interventions, thus inadequate randomization and/or high attrition (≥20%) were used to determine whether studies had a high risk of bias.
Non-RCTs were evaluated using the Mixed Methods Appraisal Tool (MMAT; [18]). The MMAT uses five criteria to determine risk of bias. Reviewers indicate “yes,” “no,” or “can’t tell” for each criterion, with “can’t tell” indicating that inadequate detail was provided in the paper to determine the outcome. Two independent reviewers completed quality assessments for all the included studies. Unlike Cochrane Collaboration Risk of Bias Assessment Tool, the MMAT does not support the calculation of an overall quality score. An overall quality score was therefore not calculated, rather the consensus on bias risk was determined through discussions. Please refer to Table 1 for the detailed quality assessments of the included studies.
3.4. Data Extraction
The Cochrane Effective Practice and Organization of Care Review Qualitative Evidence Syntheses guidelines were used to guide data extraction [19]. Data was extracted by the second and third authors then checked by the first author. The retrieved information included study components (i.e., design, population, measures, and outcomes) and intervention components (i.e., type, training associated with program delivery, who delivered the intervention, and the problem targeted by the intervention).
3.5. Meta-Analysis
Following the Cochrane Collaboration guidelines, when information regarding a variable of interested was available (i.e., sample size, mean, and standard deviation/standard error/confidence intervals) [20] in two or more studies a meta-analysis was undertaken. The Review Manager (RevMan) version 5.4.1 [21] software package was used to undertake the meta-analysis. Continuous variables were calculated using a random effects model with standard mean differences and a 95% confidence interval. Chi-square tests were used to explore heterogeneity of studies. Significance was set at p < 0.05, and was quantified using the I2 statistic, maximum values of 50% identified low heterogeneity [22]. When standard deviation values were not provided, they were calculated using the method outlined by the Cochrane Collaboration [20]. Data is represented visually with forest plots and standardized mean differences are reported with 0.2 indicating a small effect size, 0.5 indicating a median effect size, and 0.8 indicating a large effect size.

Table 1.
(a) The Mixed Methods Appraisal Tool (2018) Results. (b) The Cochrane Collaboration Risk of Bias Assessment Tool Results.
Table 1.
(a) The Mixed Methods Appraisal Tool (2018) Results. (b) The Cochrane Collaboration Risk of Bias Assessment Tool Results.
| (a) Non-randomised Studies | ||||||||||
| Citation | ||||||||||
| Qualitative Studies | ||||||||||
| Is the qualitative approach appropriate to answer the research question? | Are the qualitative data collection methods adequate to address the research question? | Are the findings adequately derived from the data? | Is the interpretation of results sufficiently substantiated by data? | Is there coherence between qualitative data sources, collection, analysis and interpretation? | ||||||
| Zapart et al. (2016) [23] | Yes | Yes | Yes | Yes | Yes | |||||
| Quantitative nonrandomized | ||||||||||
| Are the participants representative of the target population? | Are measurements appropriate regarding both the outcome and intervention (or exposure)? | Are there complete outcome data? | Are the confounders accounted for in the design and analysis? | During the study period, is the intervention administered (or exposure occurred) as intended? | ||||||
| Ammerman et al. (2005) [24] | Yes | Yes | Can’t tell | Can’t tell | Can’t tell | |||||
| Ammerman et al. (2011) [25] | Yes | Yes | No | Yes | Yes | |||||
| Ammerman et al. (2012) [26] | Yes | Yes | Yes | Yes | Can’t tell | |||||
| O’Malley et al. (2021) [8] | Yes | Yes | Yes | No | Yes | |||||
| Reuter et al. (2016) [9] | Yes | Yes | Yes | Yes | Yes | |||||
| Stacks et al. (2019) [27] | Yes | Yes | No | Can’t tell | Yes | |||||
| Stacks et al. (2022) [28] | Can’t tell | Yes | Yes | Yes | Yes | |||||
| van Grieken et al. (2019) [29] | Yes | Yes | No | Yes | Can’t tell | |||||
| Mixed Methods | ||||||||||
| Is there an adequate rationale for using a mixed methods design to address the research question? | Are the different components of the study effectively integrated to answer the research question? | Are the outputs of the integration of qualitative and quantitative components adequately interpreted? | Are divergences and inconsistencies between quantitative and qualitative results adequately addressed? | Do the different components of the study adhere to the quality criteria of each tradition of the methods involved? | ||||||
| Giallo et al. (2021) [30] | Yes | Yes | Yes | Yes | Yes | |||||
| O’Donnell et al. (2023) [31] | Yes | Yes | Yes | Can’t tell | Yes | |||||
| (b) Randomised Control Trials | ||||||||||
| Random Sequence Generation | Allocation Concealment | Blinding of Participants and Researchers | Blinding of Outcome Assessment | Incomplete Outcome Data | Selective Reporting | Anything Else | Overall Bias | |||
| Bair-Merritt et al. (2010) [32] | + | + | + | + | + | + | + | Low | ||
| Barlow et al. (2007) [33] | + | + | + | + | + | + | + | Low | ||
| Bartu et al. (2006) [34] | + | + | ? | ? | + | + | + | Low | ||
| Black et al. (1994) [35] | ? | ? | ? | + | − | + | + | High | ||
| Butz et al. (2001) [36] | + | + | ? | ? | + | + | + | Low | ||
| Catherine et al. (2020) [37] | + | − | − | + | + | + | + | Low | ||
| Duggan et al. (2004) [38] | + | + | + | + | − | + | + | High | ||
| Fergusson et al. (2006) [39] | + | ? | ? | ? | + | + | + | Unclear | ||
| Fraser et al. (2000) [40] | + | + | + | + | − | + | + | High | ||
| Goldfeld et al. (2019) [41] | + | + | − | + | − | + | + | High | ||
| Goldfeld et al. (2021) [42] | + | + | − | + | − | + | + | High | ||
| Goldfeld et al. (2022) [7] | + | + | − | + | − | + | + | High | ||
| Kemp et al. (2011) [43] | + | + | − | + | − | + | + | High | ||
| LeCroy & Lopez (2020) [44] | + | + | ? | ? | − | + | + | High | ||
| Lowell et al. (2011) [45] | + | + | + | ? | + | + | + | Low | ||
| Mejdoubi et al. (2013) [46] | + | ? | ? | ? | + | + | + | Unclear | ||
| Mejdoubi et al. (2014) [46] | + | + | ? | + | + | + | + | Low | ||
| Oxford et al. (2023) [47] | + | + | ? | + | + | + | + | Low | ||
| Rosenblum et al. (2020) [48] | + | + | − | + | + | + | + | Low | ||
| Sharps et al. (2016) [49] | + | + | + | + | − | + | + | High | ||
| Tamaki (2008) [50] | + | + | + | ? | + | + | + | Low | ||
| Van Doesum et al. (2008) [51] | + | + | ? | + | + | + | + | Low | ||
| Van Horne et al. (2022) [52] | + | + | + | ? | − | + | + | High | ||
Note. All studies met MMAT screening questions criteria S1, “Are there clear research questions?”; and S2, “Do the collected data allow to address the research questions?”. The ‘Can’t tell’ response category means that the paper do not report appropriate information to answer ‘Yes’ or ‘No’. − = Low Risk, + = High Risk, ? = Unclear.
4. Results
An overview of the search strategy and number of articles identified at each stage are presented in Figure 1. A total of 584 articles were identified through database searches (0 from CINAHL, 1 from PsychInfo, 5 from Embase, 109 from PubMed, and 469 from Scopus). A total of 526 articles remained after duplicates were removed. Title/abstract screening resulted in the removal of an additional 427 articles. Of the 99 remaining articles, we were unable to locate 2. Additional searches identified a further 39 relevant articles. A total of 136 articles were read during the full text-review stage. This led to the exclusion of a further 102 articles. The remaining 34 articles met inclusion criteria and were included in the present review (see Table 2 for an overview of studies included in the review).
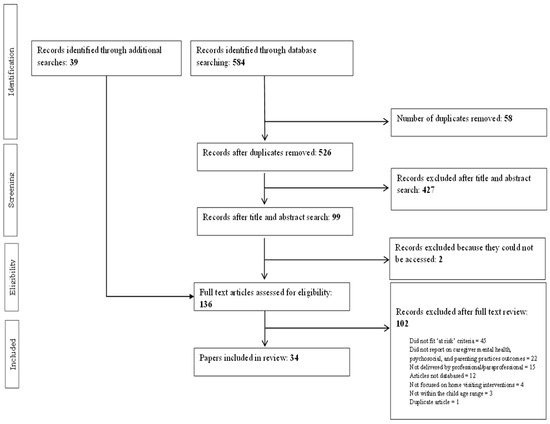
Figure 1.
PRISMA flow diagram of included studies.
Two reviewers (first author and second or third authors) independently screened all articles, completed full-text reviews, and undertook quality assessments. When disagreements regarding study selection and quality assessment arose they were discussed and resolved. A third reviewer was available in the event that disagreement could not be resolved by the primary reviewers. For title/abstract screening inter-rater agreement was 88.1% while for and full-text screening it was 66.1%.
Table 2.
Overview of included studies.
Table 2.
Overview of included studies.
| Article | Target Problem | Intervention | Study Design | Country | Demographics |
|---|---|---|---|---|---|
| Ammerman et al. (2005) [24] | Mental health (depression) | IH-CBT * | Quasi-experimental | USA | N = 26 women, M age = 22.52 (SD 3.95). |
| Ammerman et al. (2011) [25] | Mental health (depression) | IH-CBT * | Quasi-experimental | USA | N = 307 women; Intervention n = 64, M age = 22.57 (SD 4.96); Control n = 241, M age = 20.15 (SD 4.18). |
| Ammerman et al. (2012) [26] | Mental health (depression) | IH-CBT * | Quasi-experimental | USA | N = 60 women; M age = 22.4 years (SD 5.0); Child M age = 152.0 days (SD 73.0). |
| Bair-Merritt et al. (2010) [32] | Partner violence | Hawaii Healthy Start Program | RCT | USA | N = 643 women; Intervention n = 373, M age not provided; Control n = 270, M age not provided. |
| Barlow et al. (2007) [33] | Mental health (depression) | Health visiting intervention | RCT | United Kingdom | N = 131 women; Intervention n = 68, M age not provided; Control n = 63, M age not provided. |
| Bartu et al. (2006) [34] | Mental health (substance use) | Home visiting intervention | RCT | Australia | N = 152 women; Intervention n = 76 women, median age = 27 years (17–39), Control group n = 76 women, median age = 25 years (18–41). |
| Black et al. (1994) [35] | Mental health (substance use) | SPICE | RCT | USA | N = 60 women; Intervention n = 31, M age = 26.4 (SD 0.9); Control n = 29, M age = 27.9 (SD 0.7) |
| Butz et al. (2001) [36] | Mental health (substance use) | Home visiting intervention | RCT | USA | N = 117 women; Intervention n = 59, M age = 28.0 (SD 4.6); Control n = 58, M age = 28.9 (SD 4.5) |
| Catherine et al. (2020) [37] | Mental health (substance use) | Nurse-Family Partnership | RCT | Canada | N = 739 women; Intervention n = 368, M age not provided; Control n = 371, M age not provided. |
| Duggan et al. (2004) [38] | Child maltreatment | Hawaii Healthy Start Program | RCT | USA | N = 643 women; Intervention n = 373, M age = 23.7 years (SD 5.8); Control n = 270, M age = 23.3 years (SD 5.8) |
| Fergusson et al. (2005) [39] | At risk families (including mental health difficulties and domestic violence) | Early start | RCT | New Zealand | N = 391 women; Intervention n = 184 women, M age not provided; Control n = 207, M age not provided. |
| Fraser et al. (2000) [40] | Child maltreatment | Home visiting intervention | RCT | Australia | N = 181 women; Intervention n = 90 women, M age = 25.72 years (SD 5.61); Control n = 91 women, M age = 26.67 years (SD 6.08). |
| Giallo et al. (2021) [30] | Child maltreatment | HoPES | Mixed methods | Australia | N = 30 families; mother n = 29, M age = 28.9 years (SD 7.1); father n = 11, M age = 34.09 years (SD 10.8); children n = 31, M age = 14.4 months (SD 9.7), 46.7% female. |
| Goldfeld et al. (2019) [41] | Women experiencing adversity (including mental health difficulties) | right@home | RCT | Australia | N = 722 women; Intervention n = 306 women, M age = 27.6 years (SD 6.1); Control n = 359 women, M age = 27.4 years (SD 6.2). |
| Goldfeld et al. (2021) [42] | At risk women (including mental health difficulties) | right@home | RCT | Australia | N = 495 women; Intervention n = 255 women, M age = 27.6 years (SD 5.9); Control n = 240 women, M age = 28.3 years (SD 6.4). |
| Goldfeld et al. (2022) [7] | Women experiencing adversity (including mental health difficulties) | right@home | RCT | Australia | N = 426 women; Intervention n = 225 women, M age = 27.9 years (SD 6.0); Control n = 201 women, M age = 28.7 years (SD 6.4). |
| Kemp et al. (2011) [43] | Women experiencing adversity (including mental health difficulties and domestic violence) | Sustained structured nurse home visiting program | RCT | Australia | N = 208 women; Intervention n = 111 women, M age = 27.6 years (SD 6.7); Control n = 97 women, M age = 27.7 years (SD 5.9). |
| LeCroy & Lopez (2020) [44] | Mental health | Healthy Families Arizona | RCT | USA | N = 245 families; Intervention n = 98 women, M age not provided; Control n = 147 women, M age not provided. Father demographics not provided. |
| Lowell et al. (2011) [45] | Child emotional/behavioural problems and/or parent psychosocial risk | Child FIRST | RCT | USA | N = 157; Intervention n = 78 mothers, mother M age = 27.7 years (SD = 7.0), child M = 19.0 months, (SD = 9.2), 42.3% male; Control n = 79, mother M = 26.9 years, (SD = 6.9), child M = 18.0, (SD = 8.8), 45.6% male. |
| Mejdoubi et al. (2013) [46] | Partner violence | VoorZorg | RCT | Netherlands | N = 460 women; Intervention n = 237 women, M age = 19.5 years (SD 2.8); Control n = 223 women, M age = 19.2 years (SD 2.6) |
| Mejdoubi et al. (2014) [53] | At risk women (including substance use and domestic violence) | VoorZorg | RCT | Netherlands | N = 460 women; Intervention n = 223, M age = 19.5 years (SD 2.8); Control n = 237; M age = 19.2 years (SD 2.6). |
| O’Malley et al. (2021) [8] | Mental health (substance use) | TIES | Quasi-experimental | USA | N = 220 women, M age not provided. |
| O’Donnell (2023) [31] | Families with multiple risk factors (e.g., family violence, substance use, mental health concerns, Child Protection involvement) | Cradle to Kinder | Mixed methods | Australia | Quantitative component: N = 57 families, metropolitan families n = 24 (29% = Aboriginal or Torres Strait Islander), mother M age = 19.33 years (SD = 2.31), father involvement in program = 33%; rural families n = 33 (32% = Aboriginal or Torres Strait Islander), mother M = 18.44 (SD = 0.68, father involvement in program = 48%. Qualitative component: N = 14, 11 months, 3 fathers, M age = 22.5 (SD = 3.04), 29% = Aboriginal or Torres Strait Islander. |
| Oxford et al. (2023) [47] | Mental health | Moms and Babies Program (Promoting First Relationships) | RCT | USA | N = 252 women; Intervention n = 127, [low distress: n = 85, mother M age = 28.81 years (SD 5.67), child’s M age = 1.85 months (SD 0.46); high distress n = 42, mother M age = 28.64 years (SD 6.25), child’s M age = 1.83 months (SD 0.45); Control n = 125, [low distress: maternal M age = 27.94 years (SD 5.27), child M age = 1.82 months (SD 0.45); high distress: maternal M age = 26.26 years (SD 6.22), child M age = 1.92 months (SD 0.53)]. |
| Reuter et al. (2016) [9] | Mental Health | PFF | Quasi-experimental | USA | N = 215 caregivers, M age = 34.04 years (SD 9.65). Child protective services -referred families n = 84, M age = 37.85 years (SD 10.07); Prenatal-referred families n = 131, M age = 31.49 (SD 8.47). |
| Rosenblum et al. (2020) [48] | Parents with adverse childhood experiences | Michigan Model of IMH-HV | RCT | USA | N = 62 families; Intervention n = 32, mother M age = 32.38 years (SD 5.72), child M age = 23.59 months (SD 6.57). |
| Sharps et al. (2016) [49] | Partner violence | DOVE a | RCT | USA | N = 239 women, Intervention n = 124, M age = 24.3 (SD 5.6); Control n = 115, M age = 23.4 (SD 5.4). |
| Stacks et al. (2019) [27] | Child maltreatment | Michigan Model of IMH-HV | Quasi-experimental | USA | N = 16 parents, 68% female, M age = 21.69 years (SD 4.53), M child age 18.57 months (SD 7.1). |
| Stacks et al. (2022) [28] | Mental health | Michigan Model of IMH-HV | Quasi-experimental | USA | N = 75 women, M age = 26.67 years (SD 6.11); child M age = 9.64 months. |
| Tamaki (2008) [50] | Mental health (depression) | Home visiting intervention | RCT | Japan | N = 16 women; Intervention n = 7, M age = 33.86 years (SD 3.02); Control n = 9, M age = 33.78 (SD 5.33). |
| van Doesum et al. (2008) [51] | Mental health (depression) | Home visiting intervention | RCT | Netherlands | N = 85 women; Intervention n = 36 women, M age = 30.4 years (SD 4.1); Control n = 35 women, M age = 29.9 years (SD 3.6) |
| van Grieken et al. (2019) [29] | Mental health (stress) | The Supportive Parenting intervention | Quasi-experimental | Netherlands | N = 301 families; Intervention n = 124, mother M age = 31.0 years (SD 7.0), father M age = 34.0 years (SD 7.3), child M age = 7.6 months (SD 3.4), 47% child as girls; control n = 177, mother M age = 30.7 (SD 5.3), father M age = 32.6 years (SD 6.0), child M age = 5.1 months (SD 2.8). |
| van Horne et al. (2022) [52] | Mental health (depression) | Home visiting intervention | RCT | USA | N = 156 women; Intervention n = 72 women, M age = 30.65 years (SD 5.96); Control n = 46 women, M age = 29.4 years (SD 6.01). |
| Zapart et al. (2016) [23] | Women experiencing adversity (including mental health difficulties and domestic violence) | Sustained structured nurse home visiting program | Qualitative | Australia | N = 36 women, M age = 27.5 years (SD = 7.4). |
Note. * = mental health intervention delivered via home visiting; a = domestic violence intervention. DOVE: Domestic Violence Enhanced Home Visitation Program; HoPES = Home Parenting Education and Support; IH-CBT = in-home cognitive-behavioural therapy; IMH-HV: infant mental health home visiting; M = mean; N = total number of participants; n = number of participants in subgroup; PFF = partnerships for families; RCT = randomised controlled trial; SPICE = special parent/infant care and enrichment; SD= Standard Deviation; TIES = Team for Infants Exposed to Substance abuse; VoorZorg = dutch nurse-family partnership; USA = United States of America.
4.1. Overview of Included Studies
Of the included studies, 23 were randomised control trials (RCTs), eight were quasi-experimental design studies, two were mixed-methods studies, and one was a qualitative study. Seventeen studies were conducted in the United States of America (USA), nine in Australia, four in the Netherlands, and Canada, the United Kingdom, New Zealand, and Japan each had one study. Sample sizes ranged from 16 to 739. Most studies focused on specific populations including parents with mentally ill health (e.g., depression, substance abuse, stress; 50%, n = 17), child maltreatment (20%, n = 7), or intimate partner violence populations (8%, n = 3). Several studies (20%, n = 7) focused on families considered to be “at risk” or “experiencing adversity” (i.e., families with multiple risk factors). One study included children experiencing emotional/behavioral problems and/or parent psychosocial risk (2%). The majority of programs were delivered by professionals (79%, n = 27).
4.2. Interventions
In the 34 studies, 25 different interventions were evaluated (see Supplementary Table S2 for an overview). Most programs were manualised but noted including flexibility based if required by families based on needs. The Michigan Model of Infant Mental Health Home Visiting (IMH-HV), In Home Cognitive Behavioural Therapy (IH-CBT; administered with families already participating in a home visiting program), and right@home were each evaluated in three studies. VoorZorg (Dutch version of Nurse Family Partnership), Sustained Structured Nurse Home Visiting Program, and the Hawaii Healthy Start Program were each evaluated in two studies. Numerous programs were evaluated in one study only, including: the Special Parent/Infant Care and Enrichment Program (SPICE), The Domestic Violence Enhanced Home Visitation Program (DOVE) Intervention, The Partnerships for Families (PFF) Mental Health Model, The Supportive Parenting Intervention, The Team for Infants Exposed to Substance abuse (TIES) Program, Early Start, Home Parenting Education and Support (HoPES), Healthy Families Arizona, Mums and Babies Program (Family First Partnership), Child FIRST, Cradle to Kinder, and Nurse Family Partnership. Six studies reported that a “home visiting” intervention, and one study indicated that “health visiting” intervention, was administered.
4.3. Intervention Components
The majority of interventions were implemented with caregivers of children agreed 0–24 months. Only 9 of the 34 studies included an intervention description that would allow for replicability in future studies, including IH-CBT [24,25,26], HoPES [30], Child FIRST [45], IMH-HV [28], The Supportive Parenting Intervention [29], and home visiting interventions by van Doesum et al. [51] and Bartu et al. [34]. The remaining studies had missing data on program components, program length, or both. Where information was available, Aslam and Kemp’s Aslam and Kemp [54] report was used as a guide to classify program components under seven main intervention types: counselling/psychological support; problem solving; child development; social support; parenting skills; parent infant interaction; and provision of resources, including information, equipment (such as safety equipment or books), and linking into community resources. From the studies that provided information on program length, the number of home visits ranged from 6–60 sessions, with the majority of sessions were delivered weekly (for long term interventions reported sessions were administered weekly and then as treatment progressed they were spaced out to fortnightly and/or monthly) and lasted between 15 min to 2.5 h (most reported session lengths between 60–90 min).
4.4. Outcomes
Given the focus of this review was on mental health, psychosocial outcomes, and parenting practices of caregivers, physical health outcomes (e.g., birth outcomes) are not reported. Outcomes were further divided into mental health (subgroups: depression, substance use, and stress); parenting practices (subgroups: practical parenting skills, maternal sensitivity/warmth/responsiveness, breastfeeding, reflective functioning, and the parent-child relationship/bond); and intimate partner violence outcomes. Table 3 provides a summary of outcomes. The outcomes are first presented as a narrative summary of both non-RCT and RCT studies, followed by meta-analysis results of RCT studies with available data. Where available, effect sizes and odds ratios have been reported. Effect sizes indicate the strength of the association between two variables. Effect sizes ranging from 0.2–0.49 indicate small effects, those ranging from 0.5–0.79 indicate medium effects, and those ranging from 0.8–1 indicate large effects. Odds ratios (OR) indicate how likely an outcome is in one group compared to another group with an OR of 1 indicating the odds are the same in both groups and ORs deviating from 1.0 indicating that odds are greater in one group compared to another.
Thirty-four studies reported on parent outcomes. Of these, 23 reported on maternal mental health outcomes [7,8,23,24,25,27,30,31,33,34,35,36,37,38,39,40,42,44,45,50,51,52,53], 14 reported on parenting practices [7,8,23,27,31,33,34,40,41,43,44,47,52,53], and five reported on intimate partner violence [32,38,39,46,49].
4.4.1. Maternal Mental Health Outcomes
Of the 23 articles reporting on maternal mental health, the most measured outcomes were maternal depression (n = 12 articles) [7,24,25,33,38,39,40,42,44,45,50,51], substance use (n = 8) [8,34,35,37,38,39,44,53], and stress (n = 7) [24,25,30,35,36,40,45].
Depression
Seven of the 12 studies measuring maternal depression, five RCTs [7,40,42,45,50] and two quasi-experimental design [24,25] studies found a significant reduction in depressive symptoms in mothers who participated in a home visiting intervention. All studies used self-report measures of depression symptoms. RCTs were used to evaluate two “home visiting interventions” [40,50], the right@home intervention [7,42], and the child FIRST intervention [45]. The right@home intervention studies were longitudinal studies evaluating the same cohort. The quasi-experimental design studies were undertaken by the same team and evaluated IH-CBT, comparing home visiting interventions with CBT to home visiting interventions without CBT [24,25]. For the right@home intervention, the reduction in depression symptoms was maintained at the three- and five-year follow-up assessments with a small effect size (d = 0.20 for the 3 year follow up, d = 0.12 for the 5 year follow up) [7,42]. Fraser et al. [40] also completed a follow-up assessment, however, the observed reduction in depression symptoms in intervention primiparas (but not multiparae) women compared to control group was not maintained at the 12-month follow-up assessment.
Meta-analysis. Five RCTs had sufficient data for a meta-analysis to be undertaken [40,42,44,45,51]. Studies with missing data or insufficient data required to calculate means (i.e., standard error, confidence intervals) were excluded from the meta-analysis. Substantial heterogeneity was observed among studies (Tau2 = 0.03; Chi2 = 9.83, df = 4, p = 0.04, I2 = 59%). The random effects model (standardised mean difference 0.07; 95% CI: −0.12, 0.27; z = 0.73, p = 0.47) found no significant difference between home visiting and control conditions (Figure 2).
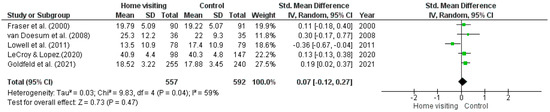
Figure 2.
Forest plot for depression outcomes. Standardised mean differences are shown with 95% CIs. Green square = point estimate of intervention effect [40,42,44,45,51].
Substance Use
Four of the eight studies measuring substance use, three RCTs [37,38,53] and one quasi-experimental design study [8], found significant reductions in substance use among mothers who participated in a home visiting intervention. All studies used self-report measures to assess substance use. The interventions evaluated included VoorZorg (focused on cigarette smoking), Hawaii Healthy Start Program (focused on illicit drug use and alcohol), TIES Program (focused on illicit drug use, alcohol, and tobacco), and the Nurse-Family Partnership Program (focused on cigarette smoking). A medium effect size (ŋp2 = 0.09) was reported for the TIES Program [8]. Small to medium odds ratios were reported for the VoorZorg program (OR = 4.4 for average number of cigarettes smoked per day and OR = 1.6 for number of cigarettes smoked near baby). Data was not available for a meta-analysis.
Stress
Five of the six studies measuring stress, two RCTs [40,45] and three quasi-experimental [24,25,30] design studies, found a significant reduction in stress symptoms in mothers who participated in a home visiting intervention. All studies used self-report measures to assess stress levels. Fraser and colleagues [40] found a reduction in stress levels of primiparas (but not multiparae) intervention group women compared to control group women, however, these results were not maintained at a 12-month follow-up. Similarly, Lowell et al. [45] found a reduction in stress levels at six months and the results were not maintained at the 12-month follow-up. The quasi-experimental design studies evaluated the HoPES [30] and IH-CBT [24,25] interventions. The HoPES intervention reported a small effect size. The IH-CBT studies were undertaken by the same team and no effect sizes were reported.
Meta-analysis. Four RCTs had sufficient data for a meta-analysis to be undertaken [35,36,42,45]. Studies with missing data or insufficient data required to calculate means (i.e., standard error, confidence intervals) were excluded from the meta-analysis. Substantial heterogeneity was observed among studies (Tau2 = 0.05; Chi2 = 9.15, df = 3, p = 0.03, I2 = 67%). The random effects model (standardised mean difference 0.01; 95% CI: −0.28, 0.27; z = 0.04, p = 0.97) found no significant difference between home visiting and control conditions (Figure 3).

Figure 3.
Forest plot for stress outcomes. Standardised mean differences are shown with 95% CIs. Green square = point estimate of intervention effect [35,36,42,45].
4.4.2. Parenting Practices
Of the 14 studies reporting on parenting practices, 12 reported on practical parenting skills (e.g., managing finances, maintaining contact with daycare providers), sense of competence, parenting self-efficacy, and/or views on motherhood [7,8,24,25,29,30,31,33,35,40,43,44]; five reported on maternal sensitivity/warmth/responsiveness [7,33,41,43,47]; four reported on breast feeding [34,43,44,53]; two reported on reflective functioning [27,49]; and one reported on parent-child bonding [52].
Practical Parenting Skills
Nine of the 12 studies reporting on practical parenting skills observed significantly improved parenting skills in women receiving a home visiting intervention. Of these studies, four were RCTs, four were quasi-experimental design studies, and one was a mixed-methods evaluation. All studies used self-report questionnaires to measure parenting skills. Two evaluated IH-CBT [24,25] and Healthy Families Arizona [44], HoPES [30], right@home [7], TIES [8], Cradle to Kinder [31], Kemp et al.’s [43] home visiting intervention, and Fraser et al.’s [40] home visiting intervention were evaluated in one study each. Both IH-CBT evaluations were undertaken by the same team, and both found that women had increased positive views of motherhood post-treatment. Effect sizes were not reported. LeCroy and Lopez [44] found that participants in the Healthy Family’s Arizona intervention, compared to control group, had significantly improved parenting practices (e.g., regular routines, reading to children) associated with moderate to large effect sizes (d range from 0.29 to 0.47). Giallo et al. [30] reported that women who took part in the HoPES intervention had increased parenting self-efficacy associated with a moderate effect size. Goldfeld et al. [7] reported improved parenting practices favoring women who took part in the right@home intervention, compared to control group, associated with small effect sizes (d ranged from 0.5 to 0.21). O’Malley et al. [8] reported a large effect size (ŋp2 = 0.32) associated with improvements in parenting practices for women who participated in the TIES program. O’Donnell et al. [31] found significant improvements in parental capabilities with a medium effect size (d = 0.72) and caregivers reported perceived improvements in parenting skills and confidence. Kemp et al. [43] reported an improvement in emotional and verbal responsiveness during the first 24 months of their child’s life in women who were in the intervention group compared to control group with small effect sizes (d = 0.26). Fraser et al. [40] reported improved parenting sense of competence at six weeks postpartum for primiparas (but not multiparae) women in the intervention group. These results were not maintained at the 12-month follow-up. In addition to the studies that found positive outcomes of intervention, it is important to note that van Grieken et al.’ s [29] RCT found unchanged or worse outcomes, compared to baseline, for both intervention and control groups in regard to parenting skills (as well as self-sufficiency and resilience).
Meta-analysis. Five RCTs had available data that could be used in a meta-analysis [35,36,40,43,44]. Heterogeneity was not significant (Tau2 = 0.00; Chi2 = 2.38, df = 4, p = 0.67, I2 = 0%). Studies with missing data or insufficient data required to calculate means (i.e., standard error, confidence intervals) were excluded from the meta-analysis. The random effects model (standardised mean difference 0.24; 95% CI: 0.10, 0.38; z = 3.39, p = 0.00) identified a significant difference between home visiting and control conditions, with results in favour of the control condition (Figure 4).
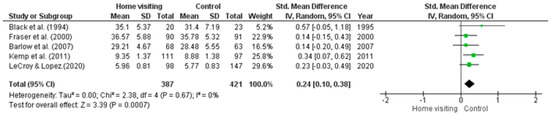
Figure 4.
Forest plot for practical parenting skills outcomes. Standardised mean differences are shown with 95% CIs. Green square = point estimate of intervention effect [33,35,40,43,44].
Maternal Sensitivity/Warmth/Responsiveness
Four of the five studies evaluating maternal sensitivity/warmth, all RCTs, found significant improvements in maternal sensitivity/warmth in women receiving home visiting interventions compared to control groups. Two studies evaluated the right@home intervention [7,41] and the Moms and Babies Program (Promoting First Relationships) [47] and Barlow et al. [33]’s health visiting intervention were evaluated in one study each. Three studies [7,33,41] used self-report questionnaires and one study used an observational measure [47] to assess maternal sensitivity/warmth. The right@home intervention studies were undertaken by the same team and reported results of a longitudinal study. Significant improvements in parental warmth were associated with a small effect size for the five-year follow-up assessment (d = 0.14) [7]. Oxford et al. [47] found that significant improvements in parental sensitivity were associated with a small effect size (d = 0.06) for women who experienced low distress and a large effect size (d = 0.63) for women who experienced high distress. Barlow et al. [33] did not report treatment effect sizes.
Meta-analysis. Four RCTs had available data that could be used in a meta-analysis [33,41,43,47]. Studies with missing data or insufficient data required to calculate means (i.e., standard error, confidence intervals) were excluded from the meta-analysis. Results showed that there was significantly high heterogeneity (Tau2 = 0.21; Chi2 = 43.57, df = 3, p ≤ 0.001, I2 = 93%) among studies. The random effects model (standardised mean difference −0.12; 95% CI: −0.58, 0.35; z = 0.50, p = 0.62) found a non-significant difference between home visiting and control conditions (Figure 5).

Figure 5.
Forest plot for Maternal sensitivity/warmth/responsiveness outcomes. Standardised mean differences are shown with 95% CIs. Green square = point estimate of intervention effect [33,41,43,47].
Breast Feeding
Three of the four studies found significant improvements in breast feeding duration as a result of participating in a home visiting intervention, all were RCTs and utilized self-report questionnaires [43,44,53]. The interventions implemented included Healthy Families Arizona, VoorZorg, and Kemp et al. [43]’s home visiting intervention. Reported effect sizes for Healthy Families Arizona (d = 0.29) and Kemp et al. [43]’s home visiting intervention (d = 0.49) were in the medium range. An odds ratio was reported for the VoorZorg intervention which indicated a small to medium association between the intervention and breast feeding (OR = 2.6). Data was not available for meta-analysis.
Reflective Functioning
Both studies that provided outcomes on parental reflective functioning evaluated IMH-HV, used a quasi-experimental design, and were undertaken by the same team. Stacks et al. [27] used an observational procedure, while Stacks et al. [28] used a clinician administered structured interview, to assess reflective functioning. Results of both studies showed significant improvements in parental reflective functioning post-treatment. Stacks et al. [27] reported an associated between intervention and reflective functioning improvement with a moderate effect size (d = 0.43).
Parent-Child Bonding/Relationship
Only one study evaluated mothers’ perceptions of her bond/relationship with her baby [52]. The study utilised an RCT to evaluate a home visiting intervention developed by van Horne et al. [52] and used self-report measures to measure the parent-child bond/relationship. No significant improvements were observed in the Parent-child bond/relationship post treatment compared to control group.
4.4.3. Intimate Partner Violence
Three out of five studies evaluating the impact of home visiting interventions on intimate partner violence reported significant reductions in intimate partner violence for women who participated in the intervention group compared to women in the control group. All studies were RCTs and used the Conflict Tactics Scale, a self-report measure, to measure intimate partner violence. Interventions implemented included the DOVE intervention [49], Mejdoubi et al. [46]’s home visiting intervention and Hawaii Healthy Start Program [32]. Sharps et al. [49] found that the DOVE intervention was associated with a moderate effect size (d = 0.50). An odds ratio was reported for Mejdoubi et al. [46]’s home visiting intervention which indicated a small association between intervention and reduced intimate partner violence (OR = 0.48). The initial association between the Hawaii Healthy Start Program and lower intimate partner violence was not maintained long term. Data was not available for meta-analysis.
Table 3.
(a) RCT Summary Table. (b): Non-RCT Summary table.
Table 3.
(a) RCT Summary Table. (b): Non-RCT Summary table.
| (a) RCT studies | ||||||
| Outcome | Citation | Target Problem | Intervention | Results | Intervention Components | |
| Sig. | Non. Sig. | |||||
| Maternal mental health | Barlow et al. (2007) [33] | Mental health (depression) | Health visiting intervention | x | Parent-infant interaction | |
| Bartu et al. (2006) [34] | Mental health (substance use) | Home visiting intervention | x | Social support Child development Parenting skills Parent-infant interaction Provision of resources | ||
| Black et al. (1994) [35] | Mental health (substance use) | SPICE | x | Social support Parenting skills and child development Parent-infant interaction Provision of resources | ||
| Butz et al. (2001) [36] | Mental health (substance use) | Home visiting intervention | x | Parenting skills Child development Parent-infant interaction Provision of resources | ||
| Catherine et al. (2020) [37] | Mental health (substance use) | Nurse-Family Partnership | x | Social support | ||
| Duggan et al. (2004) [38] | Child maltreatment | Hawaii Healthy Start Program | x | Social supports Parenting skills | ||
| Fergusson et al. (2005) [39] | At risk families (including mental health difficulties and domestic violence) | Early start | x | Social supports Problem solving Parenting skills | ||
| Fraser et al. (2000) [40] | Child maltreatment | Home visiting intervention | x | Social supports Provision of resources | ||
| Goldfeld et al. (2021) [42] | At risk women (including mental health difficulties) | right@home | x | Parenting skills Parent-infant interaction Provision of resources | ||
| Goldfeld et al. (2022) [7] | Women experiencing adversity (including mental health difficulties) | right@home | x | Parenting skills Parent-infant interaction Provision of resources | ||
| LeCroy & Lopez. (2020) [44] | Mental health | Healthy Families Arizona | x | Parent-infant interaction | ||
| Lowell et al. (2011) [45] | Child emotional/behavioural problems and/or parent psychosocial risk | Child FIRST | x | Counselling or Psychological Support | ||
| Mejdoubi et al. (2014) [53] | At risk women (including substance use and domestic violence) | VoorZorg | x | Parenting skills and child development Parent infant interaction Social supports | ||
| Tamaki (2008) [50] | Mental health (depression) | Home visiting intervention | x | Counselling or Psychological support Parenting skills and child development Parent-infant interaction Problem solving Social supports Provision of resources | ||
| van Doesum et al. (2008) [51] | Mental health (depression) | Home visiting intervention | x | Parenting skills and child development Parent-infant interaction Problem solving Provision of resources | ||
| van Horne et al. (2022) [52] | Mental health (depression) | Home visiting intervention | x | Counselling or Psychological support Parenting skills and child development Parent-infant interaction Problem solving Provision of resources | ||
| Parenting practices | Barlow et al. (2007) [33] | Mental health (depression) | Health visiting intervention | x | Parent-infant interaction | |
| Bartu et al. (2006) [34] | Mental health (substance use) | Home visiting intervention | x | Social support Child development Parenting skills Parent-infant interaction Provision of resources | ||
| Fraser et al. (2000) [40] | Child maltreatment | Home visiting intervention | x | Social supports Provision of resources | ||
| Goldfeld et al. (2019) [41] | Women experiencing adversity (including mental health difficulties) | right@home | x | Parenting skills Parent-infant interaction Provision of resources | ||
| Goldfeld et al. (2022) [7] | Women experiencing adversity (including mental health difficulties) | right@home | x | Parenting skills Parent-infant interaction Provision of resources | ||
| Kemp et al. (2011) [43] | Women experiencing adversity (including mental health difficulties and domestic violence) | Sustained structured nurse home visiting program | x | Parenting skills Parent-infant interaction Provision of resources | ||
| LeCroy & Lopez. (2020) [44] | Mental health | Healthy Families Arizona | x | Parent-infant interaction | ||
| Mejdoubi et al. (2014) [53] | At risk women (including substance use and domestic violence) | VoorZorg | x | Parenting skills and child development Parent infant interaction Social supports | ||
| Oxford et al. (2023) [47] | Mental health | Moms and Babies Program (Promoting First Relationships) | x | Parenting skills and child development Parent infant interaction | ||
| van Horne et al. (2022) [52] | Mental health (depression) | Home visiting intervention | x | Counselling or Psychological support Parenting skills and child development Parent-infant interaction Problem solving Provision of resources | ||
| Intimate partner violence | Bair-Merritt et al. (2010) [32] | Partner violence | Hawaii Healthy Start Program | x | Social support Problem solving Parenting skills Parent-infant interaction Provision of resources | |
| Duggan et al. (2004) [38] | Child maltreatment | Hawaii Healthy Start Program | x | Social supports Parenting skills | ||
| Fergusson et al. (2005) [39] | At risk families (including mental health difficulties and domestic violence) | Early start | x | Social supports Problem solving Parenting skills | ||
| Mejdoubi et al. (2013) [46] | Partner violence | VoorZorg | x | Parenting skills and child development Parent infant interaction Social supports | ||
| Sharps et al. (2016) [49] | Partner violence | DOVE | x | Social support Parenting skills and child development | ||
| (b) Non-RCT studies | ||||||
| Outcomes | Citation | Target Problem | Intervention | Results | Intervention Components | |
| Sig. | Non. Sig. | |||||
| Maternal mental health | Ammerman et al. (2011) [25] | Mental health (depression) | IH-CBT | x | Counselling or Psychological Support | |
| Ammerman et al. (2005) [24] | Mental health (depression) | IH-CBT | x | Counselling or Psychological Support | ||
| Giallo et al. (2021) [30] | Child maltreatment | HoPES | x | Parenting skills Parent-infant interaction | ||
| O’Donnell (2023) [31] | Families with multiple risk factors (e.g., family violence, substance use, mental health concerns, Child Protection involvement) | Cradle to Kinder | x | Counselling or Psychological Support Parenting skills and child development Parent infant interaction Social supports Provision of resources | ||
| O’Malley et al. (2021) [8] | Mental health (substance use) | TIES | x | Parenting skills and child development Parent infant interaction Provision of resources | ||
| Stacks et al. (2019) [27] | Child maltreatment | Michigan Model of IMH-HV | x | Social support Parenting skills and child development Parent-infant interaction Provision of resources | ||
| Parenting practices | Ammerman et al. (2011) [25] | Mental health (depression) | IH-CBT | x | Counselling or Psychological Support | |
| Ammerman et al. (2005) [24] | Mental health (depression) | IH-CBT | x | Counselling or Psychological Support | ||
| Giallo et al. (2021) [30] | Child maltreatment | HoPES | x | |||
| O’Donnell (2023) [31] | Families with multiple risk factors (e.g., family violence, substance use, mental health concerns, Child Protection involvement) | Cradle to Kinder | x | Counselling or Psychological Support Parenting skills and child development Parent infant interaction Social supports Provision of resources | ||
| O’Malley et al. (2021) [8] | Mental health (substance use) | TIES | x | Parenting skills and child development Parent infant interaction Provision of resources | ||
| Stacks et al. (2022) [28] | Mental health | Michigan Model of IMH-HV | x | Counselling or Psychological Support Social support Parent-infant interaction Parenting skills and child development | ||
| Stacks et al. (2019) [27] | Child maltreatment | Michigan Model of IMH-HV | x | Social support Parenting skills and child development Parent-infant interaction Provision of resources | ||
Note. DOVE: Domestic Violence Enhanced Home Visitation Program; IMH-HV: Infant Mental Health-Home Visiting; SPICE: Sustained Program for Improving Childhood Education. HoPES = Healthy Parenting, Healthy Families. IH-CBT = In-Home Cognitive Behavioral Therapy. Michigan Model of IMH-HV = Michigan Model of Infant Mental Health-Home Visiting. TIES = Team for Infants Exposed to Substance Abuse.
5. Discussion
This review evaluated the impact of home visiting interventions administered by professionals/paraprofessionals on caregiver outcomes. The review evaluated 34 studies to determine the impact of home visiting interventions on caregivers with high vulnerability/complex needs and young children. Overall, the review found that home visiting interventions improved a range of caregiver outcomes, although meta-analysis did not reach significance.
A total of 25 different interventions were evaluated, primarily using RCTs. Most studies included large samples and indicated positive findings across a range of outcomes: 50–80% of studies reporting on parent mental health, 75–100% reporting on parenting practices, and 60% reporting on intimate partner violence found significant improvements in outcomes. Meta-analysis effect sizes ranged from −0.01 to 0.24. Only the meta-analysis evaluating practical parenting skills was, however, significantly different from 0, with a small to medium effect size; though, results favoured the control group. Meta-analysis results need to be interpreted with caution due to high heterogeneity and the fact that most studies did not have available data that could be included in the meta-analysis.
When results of all studies are taken into consideration, findings suggest that home visiting interventions can lead to improvements in parenting outcomes. The variation in programs delivered along with a large number of studies not providing information on intervention time/dosage meant that broad stroke evaluations were unable to identify clear patterns regarding which program components led to an effective intervention and which led to an ineffective intervention. The literature was limited by the fact that only four studies collected data on fathers [29,30,31,44] and only two studies segregated some outcomes by parent gender [30,31]. Thus, the conclusions drawn from this body of work primarily pertain to mothers/female caregivers. Given that a commonly cited benefit of home visiting interventions is that the whole family can be involved in the intervention [10,55,56], it was surprising that more studies did not include fathers. While surprising, this was not entirely unexpected given the challenges associated with engaging fathers/male caregivers in health services [57]. A recent systematic review [57] on barriers associated with health service access by fathers/male caregivers found that both individual factors (e.g., narrow views of masculinity) and health service factors (e.g., service focus on mothers) are at play when it comes to fathers/male caregivers engaging with health services. The review identified several ways health services could improve father/male caregiver engagement, including providing father-specific resources/support and improving health professionals’ knowledge/confidence regarding working with fathers. Future research should aim to increase father/male caregiver participation to identify the impact of home visiting interventions on male caregivers, and the family as a whole.
5.1. Clinical Considerations
A number of home visiting interventions aimed at improving outcomes in caregivers who have young children and experience high vulnerability/complex needs were identified. While most interventions were found to be effective at improving at least one caregiver outcome and the majority of studies used the gold standard RCT to evaluate outcomes, a significant limitation of the literature was that most interventions were only evaluated in one study. IH-CBT, right@home, VoorZorg, and IMH-HV were the only interventions evaluated in two or more studies. The right@home studies reported data on one cohort and had a high risk of bias. Furthermore, IH-CBT, right@home, and VoorZorg studies were all evaluated by one team of researchers, increasing the risk of bias. The study heterogeneity and missing data did not allow for comparisons between effective and non-effective innervations. Though broad stroke evaluation did not identify differences in components between effective and non-effective interventions. Furthermore, the majority of studies focused on maternal caregivers, thus the impact of home visiting interventions on paternal caregivers and the family as a whole unit remains unclear. Thus, taking into consideration the available literature, no one intervention appears suitable to address all the varied needs of caregivers with high vulnerability and complex needs. When determining the appropriate intervention for the population, the needs of that population need to be considered. For example, right@home showed long term improvements in caregiver depression, HoPES had the greatest evidence for improving caregiver stress, while the DOVE intervention had the strongest evidence for reducing intimate partner violence.
5.2. Strengths and Limitations
The use of a systematic review strategy with broad inclusion criteria to increase the chances of including all relevant literature; trial registration; two reviewers reviewing all included studies; and detailed quality assessments are significant strengths of this review. The review also had several limitations. First, although common practice with systematic reviews, the review was restricted to studies written in the English language, limiting the generalisability of findings. Second, the inclusion of studies conducted exclusively in high-income, predominantly English-speaking countries also compromised the generalisability of the results. Third, only programs delivered by professionals/paraprofessionals were reported, the inclusion of studies in which home visiting interventions were administered by volunteer home visitors may have led to a different pattern in results. Fourth, high heterogeneity among studies was also identified. The cause of heterogeneity remains unclear and could have been the result of several factors including the fact that different interventions were administered, the duration of follow-up across studies was inconsistent, the inclusion/exclusion criteria was variable, and there was variability in outcome measures. Subgroup analysis of intervention time/dosage were not possible due to missing data. Fifth, inter-rater reliability for full-text screening was lower than 80% agreement, which is generally considered acceptable. The lower agreement on full text screenings is attributed to varying definitions of what constitutes a family with high vulnerability and/or complex needs as well as the limited information provided in some articles regarding the qualifications home visitors. Sixth, most studies used self-report measures to evaluate intervention impacts. This increases the chances of biases such as recall bias and social desirability bias around sensitive topics such as intimate partner violence and mental health challenges.
6. Conclusions
This review found that home visiting interventions delivered to caregivers who have young children and experience high vulnerability/complex needs can result in improvements in a variety of caregiver outcomes. Whilst meta-analysis of RCTs did not reach significance, positive treatment effects for one or more outcomes were observed for most home visiting programs. Further research on each intervention, with more diverse samples, and using a range of measures is needed.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/ijerph23010063/s1, Supplementary Table S1: Search strategy and search terms; Supplementary Table S2: Intervention Overview; Appendix S1: PRISMA checklist.
Author Contributions
Authors S.C., W.W., B.O.A., C.L.-C., S.W., J.K., R.G., L.K., P.J., E.M., A.D., S.R. and V.E. were involved in the conception and design of the study. S.C., W.W. and B.O.A. conducted the analyses and interpreted the data. S.C. wrote the first draft of the manuscript and all authors. contributed to the final draft. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the New South Wales Ministry of Health.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Conflicts of Interest
LK is a chief investigator on the MECSH, right@home and Volunteer Family Connect home visiting studies. LK was however not involved in the selection of studies included in this review. No other authors declared competing interests.
Abbreviations
| DOVE | The Domestic Violence Enhanced Home Visitation Program |
| HomVEE | Home Visiting Evidence of Effectiveness |
| HoPES | Program, Early Start, Home Parenting Education and Support |
| IH-CBT | In Home Cognitive Behavioural Therapy |
| IMH-HV | The Michigan Model of Infant Mental Health Home Visiting |
| MMAT | Mixed Methods Appraisal Tool |
| PFF | The Partnerships for Families |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analysis |
| RCT | Randomised control trial |
| SPICE | Special Parent/Infant Care and Enrichment Program |
| TIES | The Team for Infants Exposed to Substance abuse |
| USA | United States of America |
References
- Wickramasinghe, Y.M.; Raman, S.; Garg, P.; Hurwitz, R. Burden of adverse childhood experiences in children attending paediatric clinics in South Western Sydney, Australia: A retrospective audit. BMJ Paediatr. Open 2019, 3, e000330. [Google Scholar] [CrossRef] [PubMed]
- Burke, N.J.; Hellman, J.L.; Scott, B.G.; Weems, C.F.; Carrion, V.G. The impact of adverse childhood experiences on an urban pediatric population. Child Abus. Negl. 2011, 35, 408–413. [Google Scholar] [CrossRef]
- Grasso, D.J.; Dierkhising, C.B.; Branson, C.E.; Ford, J.D.; Lee, R. Developmental patterns of adverse childhood experiences and current symptoms and impairment in youth referred for trauma-specific services. J. Abnorm. Child Psychol. 2016, 44, 871–886. [Google Scholar] [CrossRef] [PubMed]
- Mendoza Diaz, A.; Brooker, R.; Cibralic, S.; Murphy, E.; Woolfenden, S.; Eapen, V. Adapting the ‘First 2000 Days maternal and child healthcare framework’ in the aftermath of the COVID-19 pandemic: Ensuring equity in the new world. Aust. Health Rev. 2023, 47, 72–76. [Google Scholar] [CrossRef]
- Tofail, F.; Islam, M.; Akter, F.; Zonji, S.; Roy, B.; Hossain, S.J.; Horaira, A.; Akter, S.; Goswami, D.; Brooks, A.; et al. An Integrated Mother-Child Intervention on Child Development and Maternal Mental Health. Pediatrics 2023, 151, e2023060221G. [Google Scholar] [CrossRef] [PubMed]
- Tol, W.A.; Greene, M.C.; Lasater, M.E.; Le Roch, K.; Bizouerne, C.; Purgato, M.; Tomlinson, M.; Barbui, C. Impact of maternal mental health interventions on child-related outcomes in low- and middle-income countries: A systematic review and meta-analysis. Epidemiol. Psychiatr. Sci. 2020, 29, e174. [Google Scholar] [CrossRef] [PubMed]
- Goldfeld, S.; Bryson, H.; Mensah, F.; Price, A.; Gold, L.; Orsini, F.; Kenny, B.; Perlen, S.; Bohingamu Mudiyanselage, S.; Dakin, P.; et al. Nurse home visiting to improve child and maternal outcomes: 5-year follow-up of an Australian randomised controlled trial. PLoS ONE 2022, 17, e0277773. [Google Scholar] [CrossRef] [PubMed]
- O’Malley, D.; Chiang, D.F.; Siedlik, E.A.; Ragon, K.; Dutcher, M.; Templeton, O. A promising approach in home visiting to support families affected by maternal substance use. Matern. Child Health J. 2021, 25, 42–53. [Google Scholar] [CrossRef]
- Reuter, K.E.; Melchior, L.A.; Brink, A.M. An intensive mental health home visiting model for two at-risk early childhood populations. Child. Youth Serv. Rev. 2016, 61, 22–30. [Google Scholar] [CrossRef]
- Sweet, M.A.; Appelbaum, M.I. Is home visiting an effective strategy? A meta-analytic review of home visiting programs for families with young children. Child Dev. 2004, 75, 1435–1456. [Google Scholar] [CrossRef]
- Bull, J.; McCormick, G.; Swann, C.; Mulvihill, C. Ante-and Post-Natal Home Visiting Programmes: A Review of Reviews. Lond. Health Dev. Agency 2004. Available online: https://www.researchgate.net/profile/Catherine-Swann-2/publication/242494602_Ante_and_post-natal_home-visiting_programmes_a_review_of_reviews/links/0c9605356632706f7e000000/Ante-and-post-natal-home-visiting-programmes-a-review-of-reviews.pdf (accessed on 8 December 2023).
- Turnbull, C.; Osborn, D.A. Home visits during pregnancy and after birth for women with an alcohol or drug problem. Cochrane Database Syst. Rev. 2012, 2012, Cd004456. [Google Scholar] [CrossRef] [PubMed]
- Ammerman, R.T.; Putnam, F.W.; Bosse, N.R.; Teeters, A.R.; Van Ginkel, J.B. Maternal depression in home visitation: A systematic review. Aggress. Violent Behav. 2010, 15, 191–200. [Google Scholar] [CrossRef]
- Cibralic, S.; Wu, W.T.; Ahinkorah, B.O.; Lam-Cassettari, C.; Woolfenden, S.; Kohlhoff, J.; Grace, R.; Kemp, L.; Johnson, P.; Murphy, E.; et al. Systematic review and meta-analysis of home visiting interventions aimed at enhancing child mental health, psychosocial, and developmental outcomes in vulnerable families. BMC Pediatr. 2025, 25, 314. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- HomeVEE. Early Childhood Home Visiting Models: Reviewing Evidence of Effectiveness 2023. Available online: https://homvee.acf.hhs.gov/ (accessed on 29 November 2023).
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Hong, Q.N.; Pluye, P.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B.J.R.O.C. Mixed Methods Appraisal Tool (MMAT), Version 2018; 2018. Available online: http://mixedmethodsappraisaltoolpublic.pbworks.com/w/file/fetch/127916259/MMAT_2018_criteria-manual_2018-08-01_ENG.pdf (accessed on 14 September 2023).
- Glenton, C.; Bohren, M.; Downe, S.; Paulsen, E.; Lewin, S.; EPOC. EPOC Qualitative Evidence Synthesis: Protocol and Review Template; Version 1.3; EPOC Resources for Review Authors; Norwegian Institute of Public Health: Oslo, Norway, 2022; Available online: http://epoc.cochrane.org/epoc-specific-resources-review-authors (accessed on 1 September 2023).
- Deeks, J.J.; Higgins, J.P.T.; Altman, D.G. Chapter 10: Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions Version 6.4; Higgins, J.P.T., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: West Sussex, UK, 2023. [Google Scholar]
- Review Manager (RevMan) (Version 5.4.1) [Compute Softwear]; The Cochrane Collaboration: 2020. Available online: https://www.cochrane.org/learn (accessed on 1 September 2023).
- Higgins, J.P.T.; Li, T.; Deeks, J.J. Chapter 6: Choosing effect measures and computing estimates of effect. In Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (Updated February 2022); Higgins, J.P.T., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: West Sussex, UK, 2022. [Google Scholar]
- Zapart, S.; Knight, J.; Kemp, L. ‘It Was Easier Because I Had Help’: Mothers’ Reflections on the Long-Term Impact of Sustained Nurse Home Visiting. Matern. Child Health J. 2016, 20, 196–204. [Google Scholar] [CrossRef]
- Ammerman, R.T.; Putnam, F.W.; Stevens, J.; Holleb, L.J.; Novak, A.L.; Van Ginkel, J.B. In-Home Cognitive-Behavior Therapy for depression. Best Pract. Ment. Health 2005, 1, 1–14. [Google Scholar] [CrossRef]
- Ammerman, R.T.; Putnam, F.W.; Stevens, J.; Bosse, N.R.; Short, J.A.; Bodley, A.L.; Van Ginkel, J.B. An open trial of in-home CBT for depressed mothers in home visitation. Matern. Child Health J. 2011, 15, 1333–1341. [Google Scholar] [CrossRef]
- Ammerman, R.T.; Peugh, J.L.; Putnam, F.W.; van Ginkel, J.B. Predictors of treatment tesponse in depressed mothers receiving In-Home Cognitive-Behavioral Therapy and concurrent home visiting. Behav. Modif. 2012, 36, 462–481. [Google Scholar] [CrossRef]
- Stacks, A.M.; Barron, C.C.; Wong, K. Infant mental health home visiting in the context of an infant—Toddler court team: Changes in parental responsiveness and reflective functioning. Infant Ment. Health J. 2019, 40, 523–540. [Google Scholar] [CrossRef]
- Stacks, A.M.; Jester, J.M.; Wong, K.; Huth-Bocks, A.; Brophy-Herb, H.; Lawler, J.; Riggs, J.; Ribaudo, J.; Muzik, M.; Rosenblum, K.L. Infant mental health home visiting: Intervention dosage and therapist experience interact to support improvements in maternal reflective functioning. Attach. Hum. Dev. 2022, 24, 53–75. [Google Scholar] [CrossRef]
- van Grieken, A.; Horrevorts, E.M.B.; Mieloo, C.L.; Bannink, R.; Bouwmeester-Landweer, M.B.R.; Groen, E.H.; Broeren, S.; Raat, H. A controlled trial in community pediatrics to empower parents who are at risk for parenting stress: The supportive parenting intervention. Int. J. Environ. Res. Public Health 2019, 16, 4508. [Google Scholar] [CrossRef]
- Giallo, R.; Rominov, H.; Fisher, C.; Jones, A.; Evans, K.; O’Brien, J.; Fogarty, A. A mixed-methods feasibility study of the Home Parenting Education and Support Program for families at risk of child maltreatment and recurrence in Australia. Child Abus. Negl. 2021, 122, 105356. [Google Scholar] [CrossRef]
- O’Donnell, R.; Savaglio, M.; Halfpenny, N.; Morris, H.; Miller, R.; Skouteris, H. A mixed-method evaluation of Cradle to Kinder: An Australian intensive home visitation program for families experiencing significant disadvantage. Child. Youth Serv. Rev. 2023, 150, 107016. [Google Scholar] [CrossRef]
- Bair-Merritt, M.H.; Jennings, J.M.; Chen, R.; Burrell, L.; McFarlane, E.; Fuddy, L.; Duggan, A.K. Reducing maternal intimate partner violence after the birth of a child: A randomized controlled trial of the Hawaii Healthy Start Home Visitation Program. Arch. Pediatr. Adolesc. Med. 2010, 164, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Barlow, J.; Davis, H.; McIntosh, E.; Jarrett, P.; Mockford, C.; Stewart-Brown, S. Role of home visiting in improving parenting and health in families at risk of abuse and neglect: Results of a multicentre randomised controlled trial and economic evaluation. Arch. Dis. Child 2007, 92, 229–233. [Google Scholar] [CrossRef]
- Bartu, A.; Sharp, J.; Ludlow, J.; Doherty, D.A. Postnatal home visiting for illicit drug-using mothers and their infants: A randomised controlled trial. Aust. New Zealand J. Obstet. Gynaecol. 2006, 46, 419–426. [Google Scholar] [CrossRef]
- Black, M.M.; Nair, P.; Kight, C.; Wachtel, R.; Roby, P.; Schuler, M. Parenting and early development among children of drug-abusing women: Effects of home intervention. Pediatrics 1994, 94, 440–448. [Google Scholar] [CrossRef] [PubMed]
- Butz, A.M.; Pulsifer, M.; Marano, N.; Belcher, H.; Lears, M.K.; Royall, R. Effectiveness of a home intervention for perceived child behavioral problems and parenting stress in children with in utero drug exposure. Arch. Pediatr. Adolesc. Med. 2001, 155, 1029–1037. [Google Scholar] [CrossRef]
- Catherine, N.L.A.; Boyle, M.; Zheng, Y.; McCandless, L.; Xie, H.; Lever, R.; Sheehan, D.; Gonzalez, A.; Jack, S.M.; Gafni, A.; et al. Nurse home visiting and prenatal substance use in a socioeconomically disadvantaged population in British Columbia: Analysis of prenatal secondary outcomes in an ongoing randomized controlled trial. CMAJ Open 2020, 8, E667–E675. [Google Scholar] [CrossRef]
- Duggan, A.; Fuddy, L.; Burrell, L.; Higman, S.M.; McFarlane, E.; Windham, A.; Sia, C. Randomized trial of a statewide home visiting program to prevent child abuse: Impact in reducing parental risk factors. Child Abus. Negl. 2004, 28, 623–643. [Google Scholar] [CrossRef]
- Fergusson, D.M.; Grant, H.; Horwood, L.J.; Ridder, E.M. Randomized trial of the Early Start program of home visitation. Pediatrics 2005, 116, e803–e809. [Google Scholar] [CrossRef]
- Fraser, J.A.; Armstrong, K.L.; Morris, J.P.; Dadds, M.R. Home visiting intervention for vulnerable families with newborns: Follow-up results of a randomized controlled trial. Child Abus. Negl. 2000, 24, 1399–1429. [Google Scholar] [CrossRef] [PubMed]
- Goldfeld, S.; Price, A.; Smith, C.; Bruce, T.; Bryson, H.; Mensah, F.; Orsini, F.; Gold, L.; Hiscock, H.; Bishop, L.; et al. Nurse home visiting for families experiencing adversity: A randomized trial. Pediatrics 2019, 143, e20181206. [Google Scholar] [CrossRef]
- Goldfeld, S.; Bryson, H.; Mensah, F.; Gold, L.; Orsini, F.; Perlen, S.; Price, A.; Hiscock, H.; Grobler, A.; Dakin, P.; et al. Nurse home visiting and maternal mental health: 3-year follow-up of a randomized trial. Pediatrics 2021, 147, e2020025361. [Google Scholar] [CrossRef]
- Kemp, L.; Harris, E.; McMahon, C.; Matthey, S.; Vimpani, G.; Anderson, T.; Schmied, V.; Aslam, H.; Zapart, S. Child and family outcomes of a long-term nurse home visitation programme: A randomised controlled trial. Arch. Dis. Child. 2011, 96, 533. [Google Scholar] [CrossRef]
- LeCroy, C.W.; Lopez, D. A Randomized Controlled Trial of Healthy Families: 6-Month and 1-Year Follow-Up. Prev. Sci. 2020, 21, 25–35. [Google Scholar] [CrossRef]
- Lowell, D.I.; Carter, A.S.; Godoy, L.; Paulicin, B.; Briggs-Gowan, M.J. A randomized controlled trial of Child FIRST: A comprehensive home-based intervention translating research into early childhood practice. Child Dev. 2011, 82, 193–208. [Google Scholar] [CrossRef] [PubMed]
- Mejdoubi, J.; van den Heijkant, S.C.C.M.; van Leerdam, F.J.M.; Heymans, M.W.; Hirasing, R.A.; Crijnen, A.A.M. Effect of nurse home visits vs. usual care on reducing intimate partner violence in young high-risk pregnant women: A randomized controlled trial. PLoS ONE 2013, 8, e78185. [Google Scholar] [CrossRef] [PubMed]
- Oxford, M.L.; Hash, J.B.; Lohr, M.J.; Fleming, C.B.; Dow-Smith, C.; Spieker, S.J. What works for whom? Mother’s psychological distress as a moderator of the effectiveness of a home visiting intervention. Infant Ment. Health J. 2023, 44, 301–318. [Google Scholar] [CrossRef]
- Rosenblum, K.L.; Muzik, M.; Jester, J.M.; Huth-Bocks, A.; Erickson, N.; Ludtke, M.; Weatherston, D.; Brophy-Herb, H.; Tableman, B.; Alfafara, E.; et al. Community-delivered infant–parent psychotherapy improves maternal sensitive caregiving: Evaluation of the Michigan model of infant mental health home visiting. Infant Ment. Health J. 2020, 41, 178–190. [Google Scholar] [CrossRef]
- Sharps, P.W.; Bullock, L.F.; Campbell, J.C.; Alhusen, J.L.; Ghazarian, S.R.; Bhandari, S.S.; Schminkey, D.L. Domestic violence enhanced perinatal home visits: The DOVE randomized clinical trial. J. Women’s Health 2016, 25, 1129–1138. [Google Scholar] [CrossRef]
- Tamaki, A. Effectiveness of home visits by mental health nurses for Japanese women with post-partum depression. Int. J. Ment. Health Nurs. 2008, 17, 419–427. [Google Scholar] [CrossRef]
- van Doesum, K.T.M.; Riksen-Walraven, J.M.; Hosman, C.M.H.; Hoefnagels, C. A randomized controlled trial of a home-visiting intervention aimed at preventing relationship problems in depressed mothers and their infants. Child Dev. 2008, 79, 547–561. [Google Scholar] [CrossRef] [PubMed]
- van Horne, B.S.; Nong, Y.H.; Cain, C.M.; Sampson, M.; Greeley, C.S.; Puryear, L. A promising new model of care for postpartum depression: A randomised controlled trial of a brief home visitation program conducted in Houston, Texas, USA. Health Soc. Care Community 2022, 30, e2203–e2213. [Google Scholar] [CrossRef] [PubMed]
- Mejdoubi, J.; van den Heijkant, S.C.C.M.; van Leerdam, F.J.M.; Crone, M.; Crijnen, A.A.M.; HiraSing, R.A. Effects of nurse home visitation on cigarette smoking, pregnancy outcomes and breastfeeding: A randomized controlled trial. Midwifery 2014, 30, 688–695. [Google Scholar] [CrossRef]
- Aslam, H.; Kemp, K. Home Visiting in South Western Sydney: An Integrative Literature Review, Description and Development of a Generic Model; Centre for Health Equity Training Research and Evaluation: Sydney, Australia, 2005. [Google Scholar]
- Adams, C.; Hooker, L.; Taft, A. A systematic review and qualitative meta-synthesis of the roles of home-visiting nurses working with women experiencing family violence. J. Adv. Nurs. 2023, 79, 1189–1210. [Google Scholar] [CrossRef]
- McGinnis, S.; Lee, E.; Kirkland, K.; Smith, C.; Miranda-Julian, C.; Greene, R. Engaging At-Risk Fathers in Home Visiting Services: Effects on Program Retention and Father Involvement. Child Adolesc. Soc. Work J. 2019, 36, 189–200. [Google Scholar] [CrossRef]
- Wynter, K.; Mansour, K.A.; Forbes, F.; Macdonald, J.A. Barriers and opportunities for health service access among fathers: A review of empirical evidence. Health Promot. J. Aust. 2024, 35, 891–910. [Google Scholar] [CrossRef]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.