
Assessment of SDG 3 Research Priorities and COVID-19 Recovery Pathways: A Case Study from University of the Western Cape, South Africa


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Analytical Framework
2.2. Data Collection and Sampling
2.3. Detailed Exclusion Criteria
- Studies withdrawn before ethics approval: We excluded research projects that were submitted to the ethics committee but withdrawn by the investigators prior to receiving formal approval. This was done to ensure that only committed research initiatives were included in our analysis.
- Incomplete registration information: Studies lacking complete research titles or abstracts in the ethics database were excluded as these components were essential for accurate SDG 3 target classification using our coding framework [13].
- Non-health-related research: Studies from faculties outside our defined health-related scope (excluding Faculty of Community and Health Sciences, Faculty of Natural Sciences, and Faculty of Dentistry) were excluded to maintain focus on health research contributions to SDG 3.
- Duplicate registrations: Multiple registrations of the same research project were identified, and duplicate entries were excluded to prevent inflated research counts.
- Conditional approvals without completion: Studies that received conditional ethics approval but did not meet final requirements for full approval were excluded, ensuring that only fully approved research was analyzed.
- Protocol registrations without study approval: Preliminary protocol submissions that did not advance to full study registration were excluded to focus on research projects with institutional commitment.
2.4. Coding and Analysis Procedure
- Initial codebook development: We created a comprehensive coding guide containing definitions, keywords, and contextual indicators for each SDG 3 target.
- Pilot coding and reliability testing: Two researchers independently coded the same subset of 100 randomly selected titles (approximately 11% of the total sample) to establish inter-rater reliability using Cohen’s kappa coefficient (κ = 0.82, indicating substantial agreement).
- Codebook refinement: Based on discrepancies identified during reliability testing, we refined our coding guidelines through discussion and consensus before proceeding with the full dataset.
- Full dataset coding: Each research title was assigned to the most relevant SDG 3 target using our coding framework. For ambiguous titles that potentially related to multiple targets, we applied a hierarchical decision tree that prioritized the primary focus of the research.
- Abstract consultation: When titles alone provided insufficient information for classification, we consulted project abstracts from the ethics database to ensure accurate categorization.
- Consensus meetings: Regular meetings were held by the research team to discuss uncertain cases and ensure consistent application of the coding framework.
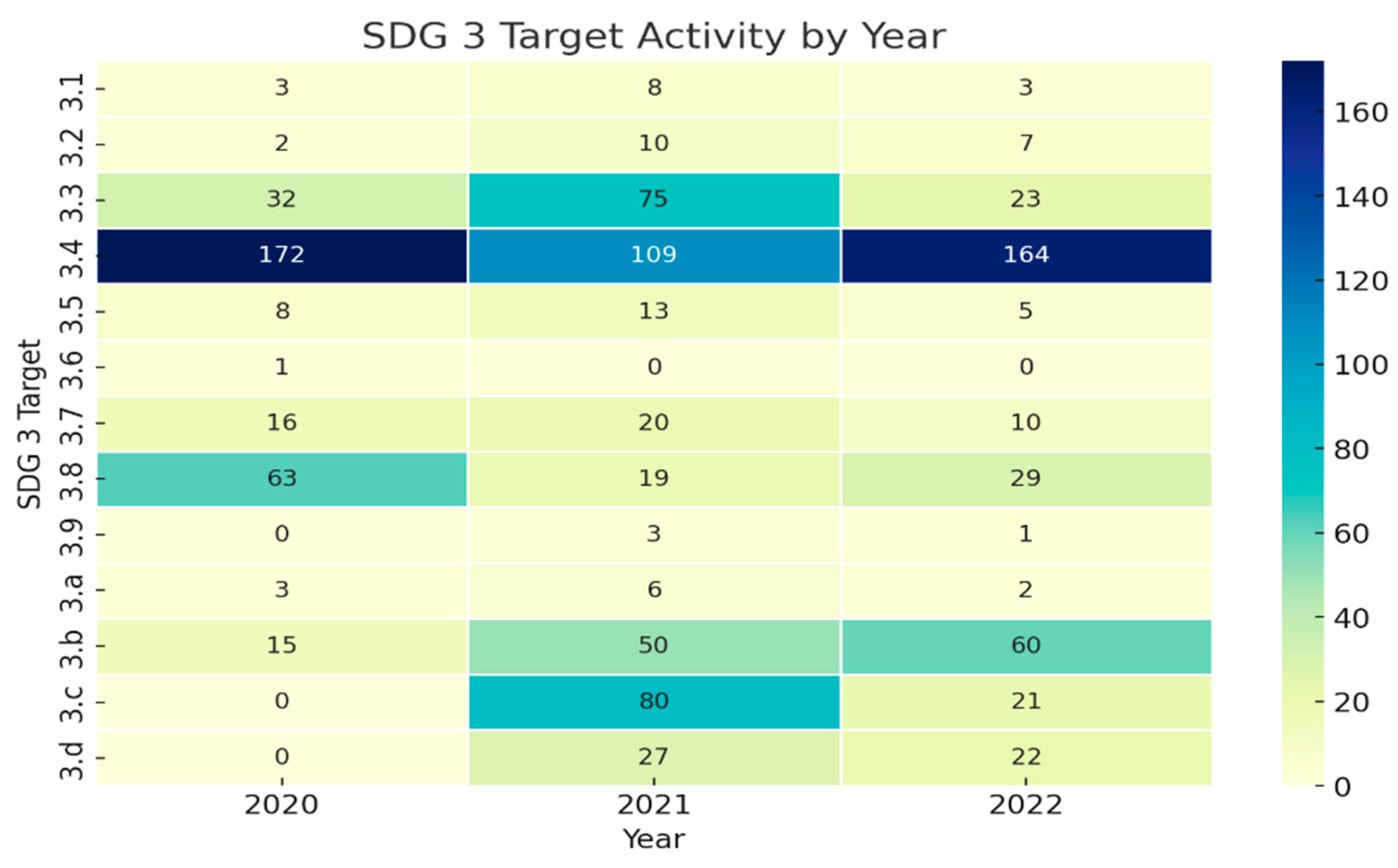
- Temporal analysis: After completing the initial coding, we analyzed changes in the distribution of research titles across SDG 3 targets over the three-year period to identify trends related to pandemic phases.
2.5. COVID-19 Context During Data Collection
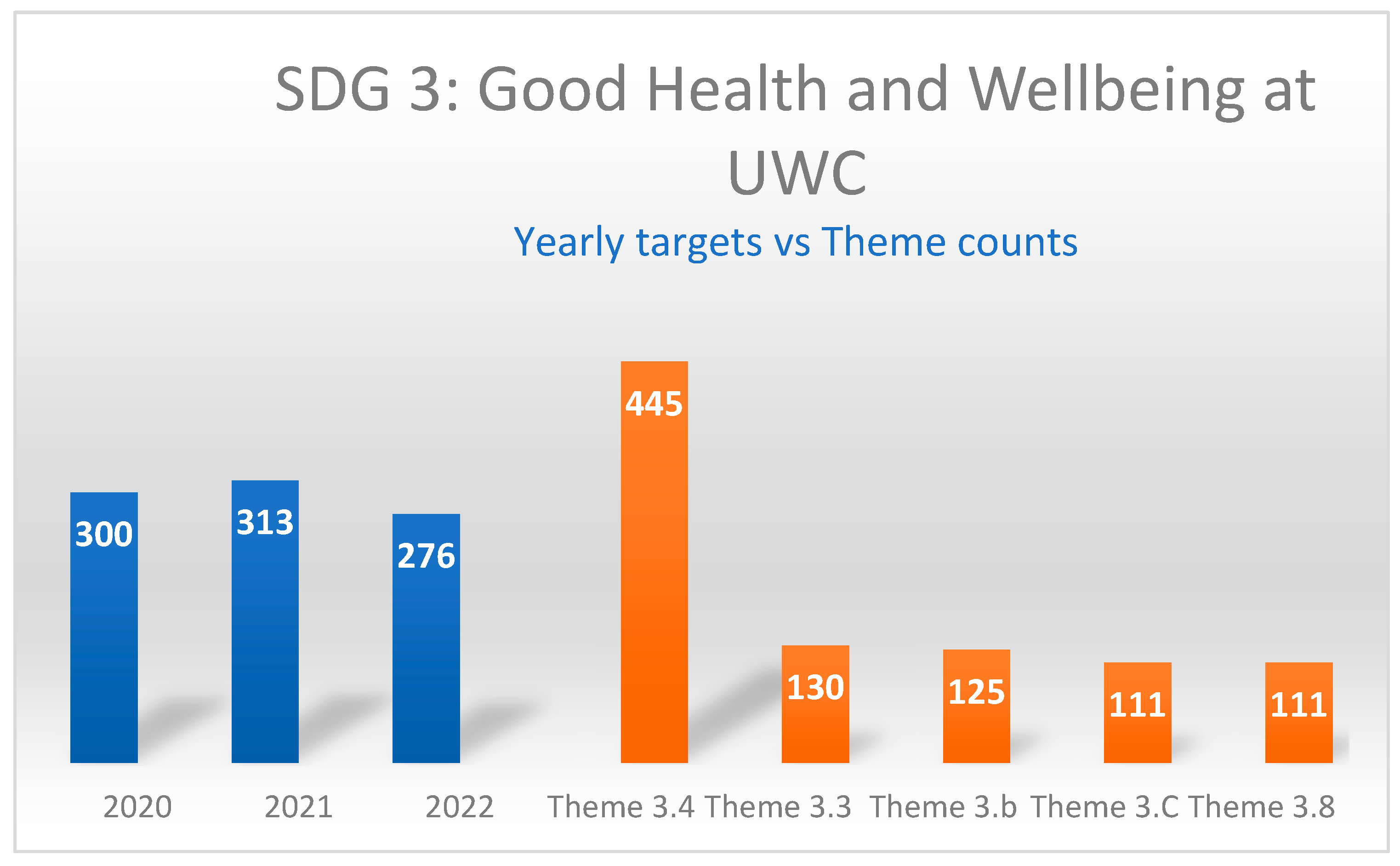
3. Results
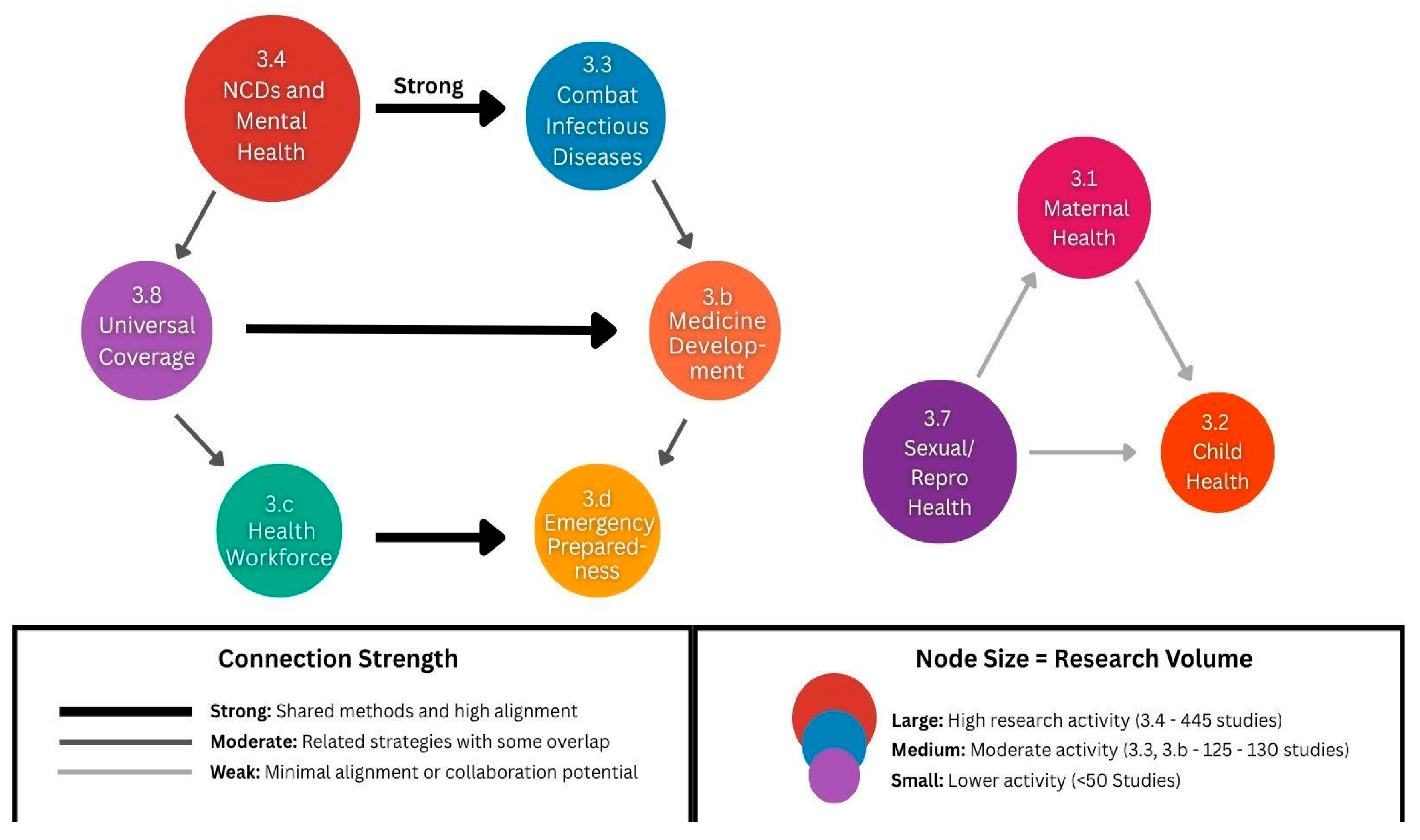
- Target 3.4 (NCDs and mental health): 445 titles (50.1% of total);
- Target 3.3 (infectious diseases): 130 titles (14.6% of total);
- Target 3.b (medicine and vaccine development): 125 titles (14.1% of total);
- Target 3.8 (universal health coverage): 111 titles (12.5% of total).
- Target 3.6 (road injuries and deaths): 1 title (0.1% of total);
- Target 3.9 (environmental health): 4 titles (0.5% of total);
- Target 3.a (tobacco control): 11 titles (1.2% of total);
- Target 3.1 (maternal mortality): 14 titles (1.6% of total).
3.1. Pandemic-Related Research Trends
3.2. Alignment with Regional Health Priorities
- Injury prevention: Despite injuries forming part of South Africa’s quadruple burden of disease, Target 3.6 (road injuries and deaths) received minimal research attention.
- Environmental health determinants: Target 3.9 (environmental health hazards) received limited research focus despite growing evidence linking environmental factors to health outcomes in disadvantaged communities.
- Maternal and child health: Targets 3.1 (maternal mortality) and 3.2 (child mortality) received relatively little research attention compared to their significance in the South African context.
4. Discussion
4.1. The Balancing Act: Crisis Response Meets Long-Term Development
4.2. Knowledge Translation Successes and Barriers
4.3. The Deeper Questions: From Knowledge Creation to Health System Impact
4.4. The University’s Evolving Role: Toward Integrated Knowledge Translation
4.5. Policy Impact Assessment and Transferability Framework
5. Recommendations
5.1. Policy Recommendations for Health Authorities
5.2. Limitations of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AIDS | Acquired Immunodeficiency Syndrome |
| COVID-19 | Coronavirus Disease 2019 |
| DVC | Deputy Vice-Chancellor |
| HIV | Human Immunodeficiency Virus |
| KTA | Knowledge-to-Action |
| NCD | Non-Communicable Disease |
| NDoH | National Department of Health |
| NHRSC | National Health Research Committee |
| POPIA | Protection of Personal Information Act |
| SA | South Africa |
| SDG | Sustainable Development Goal |
| TB | Tuberculosis |
| UWC | University of the Western Cape |
| WHO | World Health Organization |
| WHERETO | Where, Hook, Explore, Reflect, Evaluate, Tailor, Organize |
Appendix A. Keywords and Indicators for Each SDG 3 Target
- Target 3.1. Reduce maternal mortality
- Keywords: Maternal, pregnancy, childbirth, obstetric, prenatal, antenatal, and postpartum.
- Indicators: Maternal mortality ratio and skilled birth attendance.
- Target 3.2. End preventable deaths under 5 years of age
- Keywords: Child, infant, neonatal, pediatric, vaccination, and immunization
- Indicators: Under-5 mortality rate, neonatal mortality rate.
- Target 3.3. Fight infectious/communicable diseases
- Keywords: HIV, AIDS, tuberculosis, malaria, hepatitis, and sexually transmitted infections.
- Indicators: HIV incidence, TB incidence, and malaria incidence.
- Target 3.4. Reduce NCDs and promote mental health
- Keywords: Diabetes, hypertension, cancer, cardiovascular, mental health, depression, anxiety, and suicide.
- Indicators: NCD mortality rate and suicide mortality rate.
- Target 3.5. Prevent and treat substance abuse
- Keywords: Alcohol, drugs, substance abuse, addiction, and rehabilitation.
- Indicators: Treatment coverage for substance use disorders.
- Target 3.6. Reduce road injuries and deaths
- Keywords: Road traffic, motor vehicle, accidents, injuries, and trauma.
- Indicators: Road traffic mortality rate.
- Target 3.7. Universal access to sexual and reproductive healthcare
- Keywords: Family planning, contraception, reproductive health, and sexual health.
- Indicators: Contraceptive prevalence rate, unmet need for family planning.
- Target 3.8. Achieve Universal health coverage
- Keywords: Health insurance, healthcare access, health systems, and primary healthcare.
- Indicators: Coverage of essential health services and financial risk protection.
- Target 3.9. Reduce deaths from environmental health hazards
- Keywords: Air pollution, water contamination, chemical exposure, and environmental health.
- Indicators: Mortality rate from air pollution and unsafe water.
- Target 3.a. Implement tobacco control
- Keywords: Tobacco, smoking, cigarettes, and tobacco control.
- Indicators: Tobacco use prevalence.
- Target 3.b. Support medicine and vaccine development
- Keywords: Pharmaceuticals, vaccines, research and development, and essential medicines.
- Indicators: Access to affordable essential medicines.
- Target 3.c. Health worker density and distribution
- Keywords: Health workers, healthcare workforce, and medical personnel.
- Indicators: Health worker density and distribution.
- Target 3.d. Emergency preparedness
- Keywords: Emergency response, pandemic preparedness, health security, and outbreak response.
- Indicators: International health regulation capacity.
References
- World Health Organisation. Post COVID-19 Condition (Long COVID); WHO: Geneva, Switzerland, 2025; Available online: https://www.who.int/news-room/fact-sheets/detail/post-covid-19-condition-(long-covid) (accessed on 24 April 2025).
- Tilak, J.B.G. Policy Changes in Global Higher Education: What Lessons Do We Learn from the COVID-19 Pandemic? High. Educ. Policy 2022, 36, 593–616. [Google Scholar] [CrossRef] [PubMed]
- Welch, V.A.; Petticrew, M.; O’Neill, J.; Waters, E.; Armstrong, R.; Bhutta, Z.A.; Francis, D.; Koehlmoos, T.P.; Kristjansson, E.; Pantoja, T.; et al. Health equity: Evidence synthesis and knowledge translation methods. Syst. Rev. 2013, 2, 43. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3702469/ (accessed on 24 April 2025).
- Thompson, S.; Wilson, J.; Garcia, M. Knowledge systems and pandemic preparedness: University contributions to health system resilience. Acad. Med. 2024, 99, 156–163. [Google Scholar]
- Mensah, J. Sustainable Development: Meaning, history, principles, pillars and implications for human action: Literature review. Cogent Soc. Sci. 2019, 5, 1–21. [Google Scholar] [CrossRef]
- World Bank. World Development Report 2013: Jobs; World Bank: Washington, DC, USA, 2013. [Google Scholar]
- Ataguba, J.E.; Day, C.; McIntyre, D. Explaining the role of the social determinants of health on health inequality in South Africa. Glob. Health Action 2015, 8, 28865. [Google Scholar] [CrossRef]
- Massyn, N.; Barron, P.; Day, C.; Ndlovu, N.; Padarath, A. (Eds.) District Health Barometer 2019/2020; Health Systems Trust: Durban, South Africa, 2020. [Google Scholar]
- Naidoo, K.; Hoque, M.; Buckus, S.; Hoque, M.; Jagernath, K. Prevention-of-mother-to-child-transmission (PMTCT) program outcomes in South Africa in the pre-COVID and COVID eras. BMC Public Health 2023, 23, 1395. [Google Scholar] [CrossRef]
- University of the Western Cape. UWC Annual Report 2020; UWC: Cape Town, South Africa, 2020. [Google Scholar]
- Sipido, K.R.; Nagyova, I. Health research and knowledge translation for achieving the Sustainable Development Goals: Tackling the hurdles. Eur. J. Public Health 2020, 30 (Suppl. S1), i36–i40. Available online: https://academic.oup.com/eurpub/article/30/Supplement_1/i36/5813819 (accessed on 24 April 2025).
- Morgan, H. Conducting a Qualitative Document Analysis. Qual. Rep. 2022, 27, 64–77. [Google Scholar] [CrossRef]
- Wiggins, G.P.; McTighe, J. Understanding by Design; ASCD: Arlington, VA, USA, 2005. [Google Scholar]
- Bloom, B.S.; Engelhart, M.D.; Furst, E.J.; Hill, W.H.; Krathwohl, D.R. Taxonomy of Educational Objectives: The Classification of Educational Goals. Handbook I: Cognitive Domain; David McKay Company: New York, NY, USA, 1956. [Google Scholar]
- Graham, I.D.; Logan, J.; Harrison, M.B.; Straus, S.E.; Tetroe, J.; Caswell, W.; Robinson, N. Lost in knowledge translation: Time for a map? J. Contin. Educ. Health Prof. 2006, 26, 13–24. [Google Scholar] [CrossRef]
- National Health Research Committee. National Health Research Strategy: Research Priorities for South Africa 2021–2024; National Department of Health: Pretoria, South Africa, 2021. Available online: https://www.health.gov.za/wp-content/uploads/2022/05/National-Health-Research-Priorities-2021-2024.pdf (accessed on 24 April 2025).
- National Health Research Committee. National Health Research Summit Report: Research for Health Towards Uni-versal Health Coverage. National Department of Health. 2022. Available online: https://knowledgehub.health.gov.za/system/files/elibdownloads/2024-05/National%20Research%20for%20Health%20Summit%202022%20Report%20Final.pdf (accessed on 24 April 2025).
- Graham, I.D.; Tetroe, J. Some theoretical underpinnings of knowledge translation. Acad. Emerg. Med. 2007, 14, 936–941. [Google Scholar] [CrossRef] [PubMed]
- National Health Research Strategy: Research Priorities for South Africa 2021–2024; National Department of Health: Pretoria, South Africa, 2022. Available online: https://knowledgehub.health.gov.za/elibrary/health-research-priorities-revised-south-africa-2021-2024 (accessed on 24 April 2025).
- Straus, S.E.; Tetroe, J.; Graham, I.D. Knowledge Translation in Health Care: Moving from Evidence to Practice, 2nd ed.; Wiley-Blackwell: Oxford, UK, 2013. [Google Scholar]
- Mayosi, B.M.; Flisher, A.J.; Lalloo, U.G.; Sitas, F.; Tollman, S.M.; Bradshaw, D. The burden of non-communicable diseases in South Africa. Lancet 2009, 374, 934–947. [Google Scholar] [CrossRef] [PubMed]
- Pillay-van Wyk, V.; Msemburi, W.; Laubscher, R.; Dorrington, R.E.; Groenewald, P.; Glass, T.; Nojilana, B.; Joubert, J.D.; Matzopoulos, R.; Prinsloo, M.; et al. Mortality trends and differentials in South Africa from 1997 to 2012: Second National Burden of Disease Study. Lancet Glob. Health 2016, 4, e642–e653. [Google Scholar] [CrossRef]
- Fry, C.V.; Cai, X.; Zhang, Y.; Wagner, C.S. Consolidation in a crisis: Patterns of international collaboration in early COVID-19 research. PLoS ONE 2020, 15, e0236307. [Google Scholar] [CrossRef]
- Babarczy, B.; Scarlett, J.; Sharma, T.; Gaál, P.; Szécsényi-Nagy, B.; Kuchenmüller, T. National strategies for knowledge translation in health policy-making: A scoping review of grey literature. Health Res. Policy Syst. 2024, 22, 50. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, L.M.; Bishop, A.; Curran, J. Integrated knowledge translation with public health policy makers: A scoping review. Healthc. Policy 2019, 14, 55–77. [Google Scholar] [CrossRef]
- Flynn, R.; Cassidy, C.; Dobson, L.; Al-Rassi, J.; Langley, J.; Swindle, J.; Graham, I.D.; Scott, S.D. Knowledge translation strategies to support the sustainability of evidence-based interventions in healthcare: A scoping review. Implement. Sci. 2023, 18, 69. [Google Scholar] [CrossRef]
- Bennett, S.; Glandon, D.; Rasanathan, K. Governing multisectoral action for health in low-income and mid-dleincome countries: Unpacking the problem and rising to the challenge. BMJ Global Health 2018, 3, e000880. Available online: https://gh.bmj.com/content/3/Suppl_4/e000880 (accessed on 24 April 2025).
- Tancred, T.; Caffrey, M.; Falkenbach, M.; Raven, J. The pathway to health in all policies through intersectoral collaboration on the health workforce: A scoping review. Health Policy Plan. 2024, 39, i54–i74. [Google Scholar] [CrossRef]
- Royal Society of Canada Working Group. Royal Society of Canada working group on health research system recovery: Strengthening Canada’s health research system after the COVID-19 pandemic. FACETS 2024, 9, 1–28. [Google Scholar]
- Khatri, R.B.; Erku, D.; Endalamaw, A.; Wolka, E.; Nigatu, F.; Zewdie, A.; Assefa, Y.; Aryal, K.K. Multisectoral actions in primary health care: A realist synthesis of scoping review. PLoS ONE 2023, 18, e0289816. [Google Scholar] [CrossRef]
- Doubova, S.V.; Contreras Sánchez, S.E.; Ascencio-Montiel, I.J.; González-León, M.; Robledo-Aburto, Z.A. Strengthening Essential Health Services Recovery Policy after the COVID-19 Pandemic: Evidence from the Mexican Institute of Social Security. Arch. Med. Res. 2024, 55, 103011. [Google Scholar] [CrossRef] [PubMed]
- Amri, M.; Chatur, A.; O’Campo, P. Intersectoral and multisectoral approaches to health policy: An umbrella review protocol. Health Res. Policy Syst. 2022, 20, 2. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| WHERETO Component | Original Definition in Education | Adaptation for Research Analysis | KTA Framework Alignment | Research Application |
|---|---|---|---|---|
| W (Where/Why) | Where and why is a way of thinking purposefully about curriculum planning? | Where and why is a way of purposefully thinking about research conducted? | Knowledge Inquiry Phase: Systematic investigation and problem identification | Analyzing research gaps and institutional priorities that drive SDG 3 target selection |
| H (Hook/Hold) | To hook and hold is to make meaning of big ideas | Hook and hold the big ideas and themes in research | Knowledge Synthesis: Capturing compelling research themes that engage stakeholders | Identifying research clusters around major health challenges (NCDs and infectious diseases) |
| E (Explore/Enable) | Explore, experience, enable, and equip | Explore how research is being used to enable various stakeholders | Knowledge Adaptation: Tailoring research to local contexts and stakeholder needs | Assessing how research addresses specific community health priorities and policy needs |
| R (Reflect) | Reflect, rethink, and revise | Reflection on evidence to identify priorities and purposes | Barrier Assessment: Identifying obstacles to knowledge translation and research impact | Evaluating gaps between research focus and health system implementation requirements |
| E (Evaluate) | Evaluate work and progress | Evaluation of research projects and progress toward addressing indicators | Implementation Monitoring: Tracking research contributions to health outcomes | Measuring research alignment with SDG 3 targets and indicators over time |
| T (Tailor) | Tailor and personalize | Tailor to and personalize for the institutional and regional context | Local Knowledge Adaptation: Contextualizing evidence for specific settings | Adapting research priorities to South African health challenges and Western Cape needs |
| O (Organize) | Organize for optimal effectiveness | Organize findings to identify gaps and future research directions | Sustainability Planning: Ensuring continued knowledge translation and impact | Structuring research portfolios for sustained contribution to SDG 3 achievement |
| Target | Description | 2020 | 2021 | 2022 |
|---|---|---|---|---|
| 3.1 | Reduce maternal mortality | 3 | 8 | 3 |
| 3.2 | End preventable deaths under 5 years of age | 2 | 10 | 7 |
| 3.3 | Fight infectious/communicable diseases | 32 | 75 | 23 |
| 3.4 | Reduce NCDs and promote mental health | 172 | 109 | 164 |
| 3.5 | Prevent and treat substance abuse | 8 | 13 | 5 |
| 3.6 | Reduce road injuries and deaths | 1 | 0 | 0 |
| 3.7 | Universal access to sexual and reproductive healthcare | 16 | 20 | 10 |
| 3.8 | Achieve universal health coverage | 63 | 19 | 29 |
| 3.9 | Reduce deaths from environmental health hazards | 0 | 3 | 1 |
| 3.a | Implement tobacco control | 3 | 6 | 2 |
| 3.b | Support medicine and vaccine development | 15 | 50 | 60 |
| 3.c | Health worker density and distribution | 0 | 80 | 21 |
| 3.d | Emergency preparedness | 0 | 27 | 22 |
| Total | 300 | 313 | 276 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frantz, J.M.; Erasmus, P.; Magidigidi-Mathiso, L. Assessment of SDG 3 Research Priorities and COVID-19 Recovery Pathways: A Case Study from University of the Western Cape, South Africa. Int. J. Environ. Res. Public Health 2025, 22, 1057. https://doi.org/10.3390/ijerph22071057
Frantz JM, Erasmus P, Magidigidi-Mathiso L. Assessment of SDG 3 Research Priorities and COVID-19 Recovery Pathways: A Case Study from University of the Western Cape, South Africa. International Journal of Environmental Research and Public Health. 2025; 22(7):1057. https://doi.org/10.3390/ijerph22071057
Chicago/Turabian StyleFrantz, Josè M., Pearl Erasmus, and Lumka Magidigidi-Mathiso. 2025. "Assessment of SDG 3 Research Priorities and COVID-19 Recovery Pathways: A Case Study from University of the Western Cape, South Africa" International Journal of Environmental Research and Public Health 22, no. 7: 1057. https://doi.org/10.3390/ijerph22071057
APA StyleFrantz, J. M., Erasmus, P., & Magidigidi-Mathiso, L. (2025). Assessment of SDG 3 Research Priorities and COVID-19 Recovery Pathways: A Case Study from University of the Western Cape, South Africa. International Journal of Environmental Research and Public Health, 22(7), 1057. https://doi.org/10.3390/ijerph22071057