
Patient Reflections on Participation in a Randomised Controlled Multimodal Prehabilitation Trial Before Ventral Hernia Repair
 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants and Setting
2.3. Sampling Strategy
2.4. Data Collection
2.5. Data Analysis
2.6. Trustworthiness
3. Results
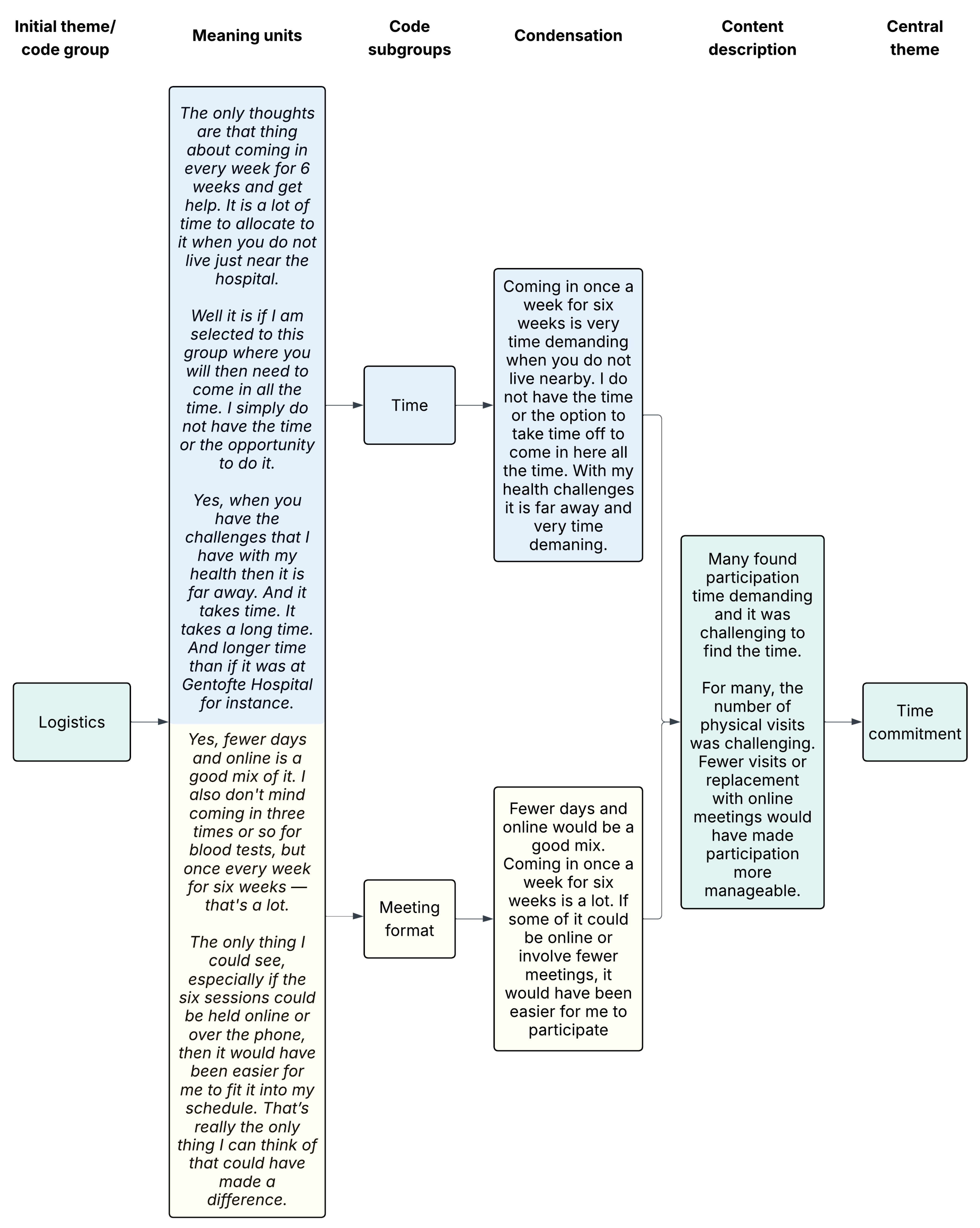
3.1. Time Commitment
“Logistics. The question is whether I can find the time for potentially weekly visits. But as long as there is some flexibility on this end, then I am also willing to make the time.”(P2 YES, 43-year-old man)
“You could say that what ultimately made me decline was simply time. I’m a mother of young children, and I have a full-time job with several responsibilities.”(P2 NO, 39-year-old woman)
3.2. Research Participation for the General Good
“Well, it was because someone has to! We can’t all say no to participating… Otherwise, there won’t be any progress. (…) Without sounding too self-righteous, it’s just basic civic responsibility.”(P6 YES, 68-year-old man)
3.3. Personal Benefits of RCT Participation
“My thought was that after speaking with the doctor, it made sense that I was recommended a robotic surgery, and the idea that the less we have here (pointing towards stomach), the better it probably is, right? So, I thought it was a good idea because I could take action myself before the surgery (…).”(P8 YES, 74-year-old man)
“So, combined with what I think I would gain from it, in relation to the things I am already doing, it was a decision on my part to opt out.”(P3 NO, 48-year-old man)
3.4. Ambivalence of Own Health and Lifestyle
“It is not necessarily a slim body. For me, it is a body that works where the musculoskeletal system does not hurt. And that you can do things without too much discomfort. In other words, having a decent everyday life—do some gardening, exercising, taking a bike ride without having to lie down afterwards and groan…”(P5 NO, 60-year-old woman)
“Well, of course, you can feel that you’re carrying a few extra kilos, but uh… Sometimes. But otherwise I’d say I feel fine. I mean, the only issue with those extra kilos is that you get more out of breath, also because you don’t move around as much as you used to. But otherwise, I’d say I feel fine.”(P4 YES, 58-year-old man)
“I know that I’m too heavy, and I know I should lose weight, because I know I can’t keep up with my kids anymore, but I don’t have pain (…) I don’t mind being big. So I actually feel healthy enough, even though I know, according to my BMI and all that, I know I’m not.”(P1 NO, 34-year-old woman)
3.5. Complications After Surgery
“I don’t know anything about that. I did not even know that it affected anything at all. Because I wasn’t told anything like that at all when I had my prostate surgery back then, so… (…) The doctor said that I should… What is it called… Well… That it would be a good idea to cut down on tobacco and alcohol a few weeks before surgery. And also after so you… I mean both… So there would be a better healing process.”(P6 NO, 61-year-old man)
“No, I’m not afraid. I have to take things as they come. If it… Well, life isn’t without risks in general … So, what’s the word… I expect it will turn out fine. If it doesn’t, that sucks. But on the other hand, there’s probably a way forward. There’s no need to expect the worst—you might as well take a positive approach.”(P11 YES, 83-year-old man)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| COREQ | Consolidated criteria for reporting qualitative research |
| P-NO | Participants who declined to participate in the prehabilitation RCT |
| P-YES | Participants who agreed to participate in the prehabilitation RCT |
| RCT | Randomised controlled trial |
| SNAP | Smoking, nutrition (both obesity and malnutrition), alcohol, and physical inactivity |
References
- Grønkjær, M.; Eliasen, M.; Skov-Ettrup, L.S.; Tolstrup, J.S.; Christiansen, A.H.; Mikkelsen, S.S.; Becker, U.; Flensborg-Madsen, T. Preoperative smoking status and postoperative complications: A systematic review and meta-analysis. Ann. Surg. 2014, 259, 52–71. [Google Scholar] [CrossRef] [PubMed]
- Eliasen, M.; Grønkjær, M.; Skov-Ettrup, L.S.; Mikkelsen, S.S.; Becker, U.; Tolstrup, J.S.; Flensborg-Madsen, T. Preoperative alcohol consumption and postoperative complications: A systematic review and meta-analysis. Ann. Surg. 2013, 258, 930–942. [Google Scholar] [CrossRef]
- Weimann, A.; Braga, M.; Carli, F.; Higashiguchi, T.; Hübner, M.; Klek, S.; Laviano, A.; Ljungqvist, O.; Lobo, D.N.; Martindale, R.G.; et al. ESPEN practical guideline: Clinical nutrition in surgery. Clin. Nutr. 2021, 40, 4745–4761. [Google Scholar] [CrossRef]
- Park, H.; de Virgilio, C.; Kim, D.Y.; Shover, A.L.; Moazzez, A. Effects of smoking and different BMI cutoff points on surgical site infection after elective open ventral hernia repair. Hernia 2021, 25, 337–343. [Google Scholar] [CrossRef]
- Bohlin, K.S.; Ankardal, M.; Stjerndahl, J.-H.; Lindkvist, H.; Milsom, I. Influence of the modifiable life-style factors body mass index and smoking on the outcome of hysterectomy. Acta Obstet. Gynecol. Scand. 2016, 95, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Snowden, C.P.; Prentis, J.; Jacques, B.; Anderson, H.; Manas, D.; Jones, D.; Trenell, M. Cardiorespiratory fitness predicts mortality and hospital length of stay after major elective surgery in older people. Ann. Surg. 2013, 257, 999–1004. [Google Scholar] [CrossRef]
- Onerup, A.; Angenete, E.; Bonfre, P.; Börjesson, M.; Haglind, E.; Wessman, C.; Nilsson, H. Self-assessed preoperative level of habitual physical activity predicted postoperative complications after colorectal cancer surgery: A prospective observational cohort study. Eur. J. Surg. Oncol. 2019, 45, 2045–2051. [Google Scholar] [CrossRef] [PubMed]
- McIsaac, D.I.; Gill, M.; Boland, L.; Hutton, B.; Branje, K.; Shaw, J.; Grudzinski, A.L.; Barone, N.; Gillis, C.; Akhtar, S.; et al. Prehabilitation in adult patients undergoing surgery: An umbrella review of systematic reviews. Br. J. Anaesth. 2022, 128, 244–257. [Google Scholar] [CrossRef]
- Thomsen, T.; Villebro, N.; Møller, A.M. Interventions for preoperative smoking cessation. Cochrane Database Syst. Rev. 2014, 2014, CD002294. [Google Scholar] [CrossRef]
- Egholm, J.W.; Pedersen, B.; Møller, A.M.; Adami, J.; Juhl, C.B.; Tønnesen, H. Perioperative alcohol cessation intervention for postoperative complications. Cochrane Database Syst. Rev. 2018, 2018, CD008343. [Google Scholar] [CrossRef]
- Sowerbutts, A.M.; Burden, S.; Sremanakova, J.; French, C.; Knight, S.R.; Harrison, E.M. Pre-operative nutrition support in patients undergoing gastrointestinal surgery. Cochrane Database Syst. Rev. 2024, 2024, CD008879. [Google Scholar] [CrossRef]
- Steffens, D.; Solomon, M.; Young, J.; Beckenkamp, P.R.; Bartyn, J.; Koh, C.; Hancock, M. A review of patient recruitment in randomised controlled trials of preoperative exercise. Clin. Trials 2024, 21, 371–380. [Google Scholar] [CrossRef]
- Molenaar, C.J.L.; Minnella, E.M.; Coca-Martinez, M.; Ten Cate, D.W.G.; Regis, M.; Awasthi, R.; Martínez-Palli, G.; López-Baamonde, M.; Sebio-Garcia, R.; Feo, C.V.; et al. Effect of multimodal prehabilitation on reducing postoperative complications and enhancing functional capacity following colorectal cancer surgery: The PREHAB randomized clinical trial. JAMA Surg. 2023, 158, 572–581. [Google Scholar] [CrossRef] [PubMed]
- Lydom, L.N.; Lauridsen, S.V.; Liljendahl, M.S.; Schmedes, A.V.; Joensen, U.N.; Tønnesen, H. Perioperative intensive smoking cessation intervention among smokers who underwent transurethral resection of bladder tumor (TURBT) in two different settings: A randomized controlled trial. Cancers 2025, 17, 713. [Google Scholar] [CrossRef] [PubMed]
- Treweek, S.; Pitkethly, M.; Cook, J.; Fraser, C.; Mitchell, E.; Sullivan, F.; Jackson, C.; Taskila, T.K.; Gardner, H. Strategies to improve recruitment to randomised trials. Cochrane Database Syst. Rev. 2018, 2018, MR000013. [Google Scholar] [CrossRef] [PubMed]
- Estabrooks, P.A.; Bolyard, M.L.; Casucci, T.; Christensen, J.T.; Gibson, B.; Golden, C.A.; Hill, J.L.; Horvath, L.; Lee, S.; Maxfield, E.M.; et al. Identifying recruitment strategies to improve the reach of evidence-based health promotion, disease prevention, and disease self-management interventions: A scoping review. Front. Public Health 2025, 13, 1515042. [Google Scholar] [CrossRef]
- Polen-De, C.; Langstraat, C.; Asiedu, G.B.; Jatoi, A.; Kumar, A. Advanced ovarian cancer patients identify opportunities for prehabilitation: A qualitative study. Gynecol. Oncol. Rep. 2021, 36, 100731. [Google Scholar] [CrossRef]
- Barnes, K.; Hladkowicz, E.; Dorrance, K.; Bryson, G.L.; Forster, A.J.; Gagné, S.; Huang, A.; Lalu, M.M.; Lavallée, L.T.; Saunders, C.; et al. Barriers and facilitators to participation in exercise prehabilitation before cancer surgery for older adults with frailty: A qualitative study. BMC Geriatr. 2023, 23, 356. [Google Scholar] [CrossRef]
- Paulo, C.M.; Ali, A.A.; Schmeusser, B.N.; Midenberg, E.; Helman, T.A.; Diller, M.L.; Pisters, M.F.; Ogan, K.; Master, V.A. Barriers and facilitators to physical activity prehabilitation in patients with kidney cancer. Eur. J. Oncol. Nurs. 2023, 65, 102333. [Google Scholar] [CrossRef]
- Karlsson, E.; Dahl, O.; Rydwik, E.; Nygren-Bonnier, M.; Bergenmar, M. Older patients’ attitudes towards, and perceptions of, preoperative physical activity and exercise prior to colorectal cancer surgery—A gap between awareness and action. Support. Care Cancer 2020, 28, 3945–3953. [Google Scholar] [CrossRef]
- Kerstiens, S.; Gleason, L.J.; Huisingh-Scheetz, M.; Landi, A.J.; Rubin, D.; Ferguson, M.K.; Quinn, M.T.; Holl, J.L.; Madariaga, M.L.L. Barriers and facilitators to smartwatch-based prehabilitation participation among frail surgery patients: A qualitative study. BMC Geriatr. 2024, 24, 129. [Google Scholar] [CrossRef]
- Tønnesen, H.; Lauridsen, S.V. Patient insight—Perioperative smoking and alcohol cessation intervention. Clin. Health Promot. 2017, 7, 18–21. [Google Scholar] [CrossRef]
- Voorn, M.J.J.; Bastiaansen, E.M.W.; Schröder, C.D.; van Kampen-van den Boogaart, V.E.M.; Bootsma, G.P.; Bongers, B.C.; Janssen-Heijnen, M.L.G. A qualitative stakeholder analysis of beliefs, facilitators, and barriers for a feasible prehabilitation program before lung cancer surgery. J. Cancer Res. Clin. Oncol. 2023, 149, 15713–15726. [Google Scholar] [CrossRef]
- van der Velde, M.; van der Leeden, M.; Geleijn, E.; Veenhof, C.; Valkenet, K. What moves patients to participate in prehabilitation before major surgery? A mixed methods systematic review. Int. J. Behav. Nutr. Phys. Act. 2023, 20, 75. [Google Scholar] [CrossRef] [PubMed]
- Tsay, S.L.; Ko, W.S.; Lin, K.P. The lifestyle change experiences of cancer survivors. J. Nurs. Res. 2016, 25, 328–335. [Google Scholar] [CrossRef] [PubMed]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef]
- Danish Ethical Committee Ethical Approval for Research Projects in Denmark. Available online: https://www.regionh.dk/til-fagfolk/forskning-og-innovation/de-regionale-videnskabsetiske-komiteer/sider/hvilke-projekter-skal-jeg-anmelde.aspx (accessed on 5 May 2025).
- Malterud, K. Systematic text condensation: A strategy for qualitative analysis. Scand. J. Public Health 2012, 40, 795–805. [Google Scholar] [CrossRef]
- Jensen, S.A.-M.S.; Lauridsen, S.V.; Fonnes, S.; Rosenberg, J.; Tønnesen, H. Effect of tailored, intensive prehabilitation for risky lifestyles before ventral hernia repair on postoperative outcomes, health, and costs—Study protocol for a randomised controlled trial (STRONG-Hernia). PLoS ONE 2025, 20, e0324002. [Google Scholar] [CrossRef]
- Creswell, J.W. Qualitative Inquiry and Research Design: Choosing Among Five Traditions, 2nd ed.; SAGE: Thousand Oaks, CA, USA, 2007. [Google Scholar]
- Malterud, K.; Siersma, V.D.; Guassora, A.D. Sample size in qualitative interview studies: Guided by information power. Qual. Health Res. 2016, 26, 1753–1760. [Google Scholar] [CrossRef]
- Palinkas, L.A.; Horwitz, S.M.; Green, C.A.; Wisdom, J.P.; Duan, N.; Hoagwood, K. Purposeful sampling for qualitative data collection and analysis in mixed method implementation research. Adm. Policy Ment. Health 2015, 42, 533–544. [Google Scholar] [CrossRef]
- Guba, E.G. Criteria for assessing the trustworthiness of naturalistic inquiries. ECTJ 1981, 29, 75–91. [Google Scholar] [CrossRef]
- Shenton, A.K. Strategies for ensuring trustworthiness in qualitative research projects. Educ. Inf. 2004, 22, 63–75. [Google Scholar] [CrossRef]
- Houghton, C.; Dowling, M.; Meskell, P.; Hunter, A.; Gardner, H.; Conway, A.; Treweek, S.; Sutcliffe, K.; Noyes, J.; Devane, D.; et al. Factors that impact on recruitment to randomised trials in health care: A qualitative evidence synthesis. Cochrane Database Syst. Rev. 2020, 2020, MR000045. [Google Scholar] [CrossRef]
- Henchcliffe, B.E.; Holihan, J.L.; Flores-Gonzalez, J.R.; Mitchell, T.O.; Ko, T.C.; Kao, L.S.; Liang, M.K. Barriers to participation in preoperative risk-reduction programs prior to ventral hernia repair: An assessment of underserved patients at a safety-net hospital. JAMA Surg. 2016, 151, 488–490. [Google Scholar] [CrossRef]
- Lerdal, A.; Moe, B.; Digre, E.; Harding, T.; Kristensen, F.; Grov, E.K.; Bakken, L.N.; Eklund, M.L.; Ruud, I.; Rossi, J.S. Stages of change—Continuous measure (URICA-E2): Psychometrics of a norwegian version. J. Adv. Nurs. 2009, 65, 193–202. [Google Scholar] [CrossRef]
- Phrochaska, J.O.; Chiou, S.-T.; Schroeder, T.V.; Larsen, M.L.; Høst, A.; Gentilello, L.M.; Damsgaard, E.M.S.; Spies, C.D.; Berger, H.; Groene, O.; et al. Engage in the Process of Change: Facts and Methods, 1st ed.; World Health Organization: Copenhagen, Denmark, 2012. [Google Scholar]

{kind=link}
| All participants | |
|---|---|
| Six meetings before surgery would be held at the hospital, i.e., on a weekly basis Participants receive education and motivational and pharmaceutical support (optional, free) Blood and urine samples are collected at some of the meetings | |
| Specific interventions according to the risky lifestyle | |
| Smokers: | Personalised nicotine replacement therapy in accordance with participant preferences and nicotine dependency |
| Risky drinkers: | Optional:
|
| Obese or at risk of malnutrition: | Personalised nutritional plan, Nupo™ meal replacements (optional) |
| Physically inactive: | Personalised physical exercise plan |
| Characteristics | RCT Decliners (n = 10) | RCT Accepters (n = 12) | |
|---|---|---|---|
| Sex, n (%) | |||
| Men | 7 (70) | 8 (67) | |
| Women | 3 (30) | 4 (33) | |
| Age, median [range] | 61 [34–84] | 69 [40–87] | |
| Working, n (%) | |||
| Yes | 5 (50) | 6 (50) | |
| No | 5 (50) | 6 (50) | |
| Risky lifestyles, n (%) | |||
| Daily smoker | 3 (30) | 4 (33) | |
| BMI > 30 kg/m2 | 6 (60) | 6 (50) | |
| Malnutrition (NRS ≥ 3) | 0 (0) | 1 (8) | |
| Alcohol intake > 14 units/week | 1 (10) | 3 (25) | |
| Physically active < 30 min/day | 2 (20) | 3 (25) | |
| Number of risky lifestyles, n (%) | |||
| 1 risky lifestyle | 8 (80) | 8 (67) | |
| 2 risky lifestyles | 2 (20) | 3 (25) | |
| ≥3 risky lifestyles | 0 (0) | 1 (8) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jensen, S.A.-M.S.; Fonnes, S.; Rosenberg, J.; Tønnesen, H.; Lauridsen, S.V. Patient Reflections on Participation in a Randomised Controlled Multimodal Prehabilitation Trial Before Ventral Hernia Repair. Int. J. Environ. Res. Public Health 2025, 22, 1039. https://doi.org/10.3390/ijerph22071039
Jensen SA-MS, Fonnes S, Rosenberg J, Tønnesen H, Lauridsen SV. Patient Reflections on Participation in a Randomised Controlled Multimodal Prehabilitation Trial Before Ventral Hernia Repair. International Journal of Environmental Research and Public Health. 2025; 22(7):1039. https://doi.org/10.3390/ijerph22071039
Chicago/Turabian StyleJensen, Sofie Anne-Marie Skovbo, Siv Fonnes, Jacob Rosenberg, Hanne Tønnesen, and Susanne Vahr Lauridsen. 2025. "Patient Reflections on Participation in a Randomised Controlled Multimodal Prehabilitation Trial Before Ventral Hernia Repair" International Journal of Environmental Research and Public Health 22, no. 7: 1039. https://doi.org/10.3390/ijerph22071039
APA StyleJensen, S. A.-M. S., Fonnes, S., Rosenberg, J., Tønnesen, H., & Lauridsen, S. V. (2025). Patient Reflections on Participation in a Randomised Controlled Multimodal Prehabilitation Trial Before Ventral Hernia Repair. International Journal of Environmental Research and Public Health, 22(7), 1039. https://doi.org/10.3390/ijerph22071039