
Adherence to Hydroxyurea Therapy for Pediatric Sickle Cell Anemia in Tanzania: Evidence from Bugando Medical Centre


Abstract
1. Background
1.1. Problem Statement
1.2. Rationale
1.3. Research Question
1.4. Broad Objective
1.5. Specific Objectives
- 1.
- To assess the level of adherence to hydroxyurea among children with sickle cell anemia attending the sickle cell clinic at Bugando Medical Centre.
- 2.
- To identify factors associated with adherence to hydroxyurea treatment among caregivers of children with sickle cell anemia attending the sickle cell clinic at Bugando Medical Centre.
1.6. Study Setting
1.7. Study Design
1.8. Study Population
1.9. Inclusion Criteria
1.10. Exclusion Criteria
1.11. Sampling Procedure
1.12. Ethical Considerations
1.13. Dissemination of Results
2. Results
2.1. Background Characteristics of the Study Participants
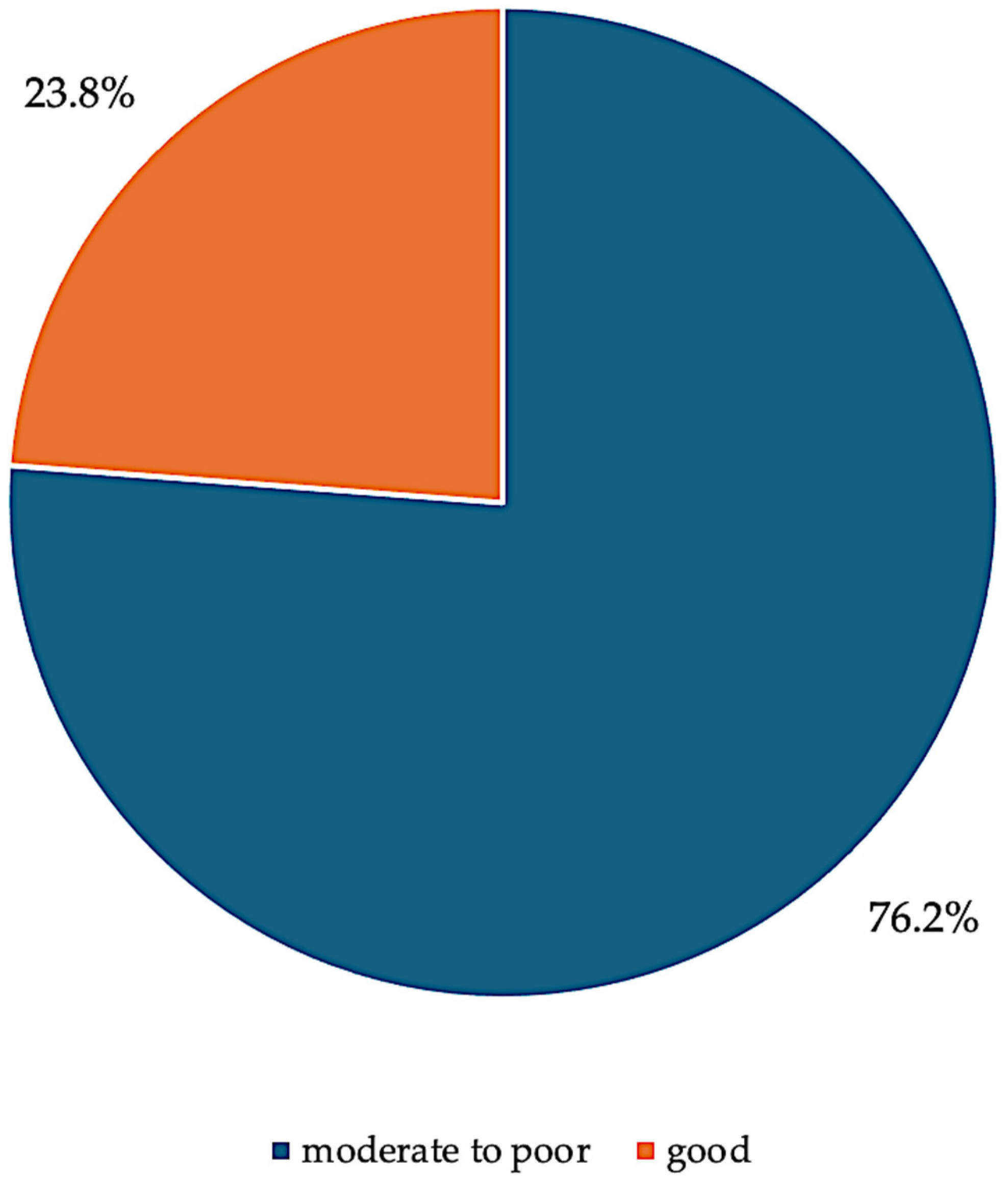
2.2. Adherence to Hydroxyurea Treatment Among Study Participants
2.3. Unadjusted Analysis on the Adherence to Hydroxyurea Treatment and the Associated Factors Among Study Participants
2.4. Adjusted Analysis on the Adherence to Hydroxyurea Treatment and the Associated Factors Among Study Participants
3. Discussion
3.1. Adherence to Hydroxyurea
3.2. Factors Associated with Adherence
3.3. Education of Caregivers
3.4. Knowledge of Hydroxyurea
3.5. Availability of Hydroxyurea
4. Conclusions
4.1. Study Limitations
4.2. Recommendations
4.3. Further Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Piel, F.B.; Hay, S.I.; Gupta, S.; Weatherall, D.J.; Williams, T.N. Global burden of sickle cell anaemia in children under five, 2010–2050: Modelling based on demographics, excess mortality, and interventions. PLoS Med. 2013, 10, e1001484. [Google Scholar] [CrossRef] [PubMed]
- Ambrose, E.E.; Makani, J.; Chami, N.; Masoza, T.; Kabyemera, R.; Peck, R.N.; Kamugisha, E.; Manjurano, A.; Kayange, N.; Smart, L.R. High birth prevalence of sickle cell disease in Northwestern Tanzania. Pediatr. Blood Cancer 2018, 65, e26735. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ambrose, E.E.; Smart, L.R.; Charles, M.; Hernandez, A.G.; Latham, T.; Hokororo, A.; Beyanga, M.; Howard, T.A.; Kamugisha, E.; McElhinney, K.E.; et al. Surveillance for sickle cell disease, United Republic of Tanzania. Bull. World Health Organ. 2020, 98, 859–868. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Grosse, S.D.; Odame, I.; Atrash, H.K.; Amendah, D.D.; Piel, F.B.; Williams, T.N. Sickle cell disease in Africa: A neglected cause of early childhood mortality. Am. J. Prev. Med. 2011, 41 (Suppl. S4), S398–S405. [Google Scholar] [CrossRef]
- Makani, J.; Cox, S.E.; Soka, D.; Komba, A.N.; Oruo, J.; Mwamtemi, H.; Magesa, P.; Rwezaula, S.; Meda, E.; Mgaya, J.; et al. Mortality in sickle cell anemia in Africa: A prospective cohort study in Tanzania. PLoS ONE 2011, 6, e14699. [Google Scholar] [CrossRef]
- Ware, R.E. How I use hydroxyurea to treat young patients with sickle cell anemia. Blood 2010, 115, 5300–5311. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- McGann, P.T.; Ware, R.E. Hydroxyurea therapy for sickle cell anemia. Expert. Opin. Drug Saf. 2015, 14, 1749–1758. [Google Scholar] [CrossRef]
- Power-Hays, A.; Ware, R.E. Effective use of hydroxyurea for sickle cell anemia in low-resource countries. Curr. Opin. Hematol. 2020, 27, 172–180. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ambrose, E.E.; Latham, T.S.; Songoro, P.; Charles, M.; Lane, A.C.; Stuber, S.E.; Makubi, A.N.; Ware, R.E.; Smart, L.R. Hydroxyurea with dose escalation for primary stroke risk reduction in children with sickle cell anaemia in Tanzania (SPHERE): An open-label, phase 2 trial. Lancet Haematol. 2023, 10, e261–e271. [Google Scholar] [CrossRef]
- Hodges, J.R.; Phillips, S.M.; Norell, S.; Nwosu, C.; Khan, H.; Luo, L.; Badawy, S.M.; King, A.; Tanabe, P.; Treadwell, M.; et al. Intentional and unintentional nonadherence to hydroxyurea among people with sickle cell disease: A qualitative study. Blood Adv. 2020, 4, 4463–4473. [Google Scholar] [CrossRef]
- Adewoyin, A.S.; Oghuvwu, O.S.; Awodu, O.A. Hydroxyurea therapy in adult Nigerian sickle cell disease: A monocentric survey on pattern of use, clinical effects and patient’s compliance. Afr. Health Sci. 2017, 17, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Okocha, E.C.; Gyamfi, J.; Ryan, N.; Babalola, O.; Etuk, E.A.; Chianumba, R.; Nwegbu, M.; Isa, H.; Madu, A.J.; Adegoke, S.; et al. Barriers to Therapeutic Use of Hydroxyurea for Sickle Cell Disease in Nigeria: A Cross-Sectional Survey. Front. Genet. 2022, 12, 765958. [Google Scholar] [CrossRef] [PubMed]
- Luoga, F.; Jonathan, A.; Chirande, L.; Balandya, E. Newborn Screening for Sickle Cell Disease in Tanzania: The Past, Present and Future. Tanzan. Med. J. 2020, 31, 79–82. [Google Scholar] [CrossRef]
- Makani, J.; Tluway, F.; Makubi, A.; Soka, D.; Nkya, S.; Sangeda, R.; Mgaya, J.; Rwezaula, S.; Kirkham, F.J.; Kindole, C.; et al. A ten year review of the sickle cell program in Muhimbili National Hospital, Tanzania. BMC Hematol. 2018, 18, 33. [Google Scholar] [CrossRef] [PubMed]
- Brousseau, D.C.; Owens, P.L.; Mosso, A.L.; Panepinto, J.A.; Steiner, C.A. Acute care utilization and rehospitalizations for sickle cell disease. JAMA 2010, 303, 1288–1294. [Google Scholar] [CrossRef]
- Walsh, K.E.; Cutrona, S.L.; Kavanagh, P.L.; Crosby, L.E.; Malone, C.; Lobner, K.; Bundy, D.G. Medication adherence among pediatric patients with sickle cell disease: A systematic review. Pediatrics 2014, 134, 1175–1183. [Google Scholar] [CrossRef]
- Cober, M.P.; Phelps, S.J. Penicillin prophylaxis in children with sickle cell disease. J. Pediatr. Pharmacol. Ther. 2010, 15, 152–159. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Charache, S.; Terrin, M.L.; Moore, R.D.; Dover, G.J.; Barton, F.B.; Eckert, S.V.; McMahon, R.P.; Bonds, D.R.; Investigators of the Multicenter Study of Hydroxyurea in Sickle Cell Anemia. Effect of hydroxyurea on the frequency of painful crises in sickle cell anemia. Investigators of the Multicenter Study of Hydroxyurea in Sickle Cell Anemia. N. Engl. J. Med. 1995, 332, 1317–1322. [Google Scholar] [CrossRef]
- Kripalani, S.; Yao, X.; Haynes, R.B. Interventions to enhance medication adherence in chronic medical conditions: A systematic review. Arch. Intern. Med. 2007, 167, 540–550. [Google Scholar] [CrossRef]
- Berkman, N.D.; Sheridan, S.L.; Donahue, K.E.; Halpern, D.J.; Crotty, K. Low health literacy and health outcomes: An updated systematic review. Ann. Intern. Med. 2011, 155, 97–107. [Google Scholar] [CrossRef]
- Gellad, W.F.; Grenard, J.L.; Marcum, Z.A. A systematic review of barriers to medication adherence in the elderly: Looking beyond cost and regimen complexity. Am. J. Geriatr. Pharmacother. 2011, 9, 11–23. [Google Scholar] [CrossRef]
- Zuvekas, S.H.; Taliaferro, G.S. Pathways to access: Health insurance, the health care delivery system, and racial/ethnic disparities, 1996–1999. Health Aff. 2003, 22, 139–153. [Google Scholar] [CrossRef] [PubMed]
- McGrady, M.E.; Hommel, K.A. Medication Adherence and Health Care Utilization in Pediatric Chronic Illness: A Systematic Review. Pediatrics 2013, 132, 730–740. [Google Scholar] [CrossRef]
- El-Rachidi, S.; LaRochelle, J.M.; Morgan, J.A. Pharmacists and Pediatric Medication Adherence: Bridging the Gap. Hosp. Pharm. 2017, 52, 124–131. [Google Scholar] [CrossRef]
- Bakshi, N.; Katoch, D.; Sinha, C.B.; Ross, D.; Quarmyne, M.-O.; Loewenstein, G.; Krishnamurti, L. Assessment of Patient and Caregiver Attitudes and Approaches to Decision-Making Regarding Bone Marrow Transplant for Sickle Cell Disease: A Qualitative Study. JAMA Netw. Open 2020, 3, e206742. [Google Scholar] [CrossRef] [PubMed]
- O’Leary, A.; Jemmott, J.B.; Jemmott, L.S.; Teitelman, A.; Heeren, G.A.; Ngwane, Z.; Icard, L.D.; Lewis, D.A. Associations Between Psychosocial Factors and Incidence of Sexually Transmitted Disease Among South African Adolescents. Sex. Transm. Dis. 2015, 42, 135–139. [Google Scholar] [CrossRef] [PubMed]
- Epstein, R.M.; Franks, P.; Fiscella, K.; Shields, C.G.; Meldrum, S.C.; Kravitz, R.L.; Duberstein, P.R. Measuring patient-centered communication in patient-physician consultations: Theoretical and practical issues. Soc. Sci. Med. 2005, 61, 1516–1528. [Google Scholar] [CrossRef]
- DeBaun, M.R. Hydroxyurea therapy contributes to infertility in adult men with sickle cell disease: A review. Expert Rev. Hematol. 2014, 7, 767–773. [Google Scholar] [CrossRef]
- Kalichman, S.C.; Grebler, T.; Amaral, C.M.; McNerey, M.; White, D.; Kalichman, M.O.; Cherry, C.; Eaton, L. Intentional non-adherence to medications among HIV positive alcohol drinkers: Prospective study of interactive toxicity beliefs. J. Gen. Intern. Med. 2013, 28, 399–405. [Google Scholar] [CrossRef]

{kind=link}
| Variables | n | % |
|---|---|---|
| Age caregiver (years) | ||
| Median (±SD) | 33 (29–40) | |
| Child age (years) | ||
| 1–10 | 118 | 68.6 |
| 11–17 | 54 | 31.4 |
| Median (±SD) | 8 (5–12) | |
| Education level | ||
| Illiterate to primary | 61 | 35.5 |
| Secondary | 66 | 38.4 |
| College/university | 45 | 26.1 |
| Occupation | ||
| Employed | 118 | 31.4 |
| Not employed | 54 | 68.6 |
| Knowledge of hydroxyurea | ||
| Good | 126 | 73.3 |
| Moderate | 31 | 18.0 |
| Poor | 15 | 8.7 |
| Number of family members using hydroxyurea | ||
| One | 143 | 85.1 |
| More than one | 25 | 14.9 |
| Way to obtain hydroxyurea | ||
| Health insurance | 141 | 82.0 |
| Cash/donation | 31 | 18.0 |
| Believe hydroxyurea reduces pain | ||
| Yes | 154 | 89.5 |
| No | 18 | 10.5 |
| Child has health insurance | ||
| Yes | 122 | 70.9 |
| No | 50 | 29.1 |
| Was hydroxyurea available when attending clinic? | ||
| Yes | 136 | 79.1 |
| No | 36 | 20.9 |
| Referred | ||
| Yes | 29 | 16.9 |
| No | 143 | 83.1 |
| Variables | cPR 95% CI | p-Values |
|---|---|---|
| Age categories of caregiver (years) | ||
| 21–34 | Ref | |
| 35–45 | 0.73 (0.37, 1.42) | 0.35 |
| 46–62 | 1.49 (0.77, 2.87) | 0.23 |
| Child age (years) | ||
| 1–10 | 3.29 (1.36, 7.95) | 0.01 |
| 11–17 | Ref | |
| Education level of caregiver | ||
| Illiterate to primary | Ref | |
| Secondary | 1.74 (0.84, 3.63) | 0.13 |
| College/university | 2.26 (1.08, 4.70) | 0.03 |
| Occupation of caregiver | ||
| Employed | 0.88 (0.50, 1.55) | 0.66 |
| Not employed | Ref | |
| Knowledge of hydroxyurea | ||
| Good | 1.96 (1.52, 7.40) | 0.02 |
| Moderate | 1.45 (0.33, 6.38) | 0.62 |
| Poor | Ref | |
| Number of family members using hydroxyurea | ||
| One | Ref | |
| More than one | 1.01 (0.47, 2.16) | 0.98 |
| Way to obtain hydroxyurea | ||
| Health insurance | 2.78 (0.91, 8.47) | 0.07 |
| Cash/donation | Ref | |
| Believe hydroxyurea reduces pain | ||
| Yes | 0.84 (0.38, 1.87) | 0.67 |
| No | Ref | |
| Child has health insurance | ||
| Yes | 1.69 (0.84, 3.41) | 0.14 |
| No | Ref | |
| Was hydroxyurea available when attending clinic? | ||
| Yes | 1.91 (0.80, 4.52) | 0.13 |
| No | Ref | |
| Referred | ||
| Yes | 0.39 (0.13, 1.18) | 0.09 |
| No | Ref |
| Variables | aPR 95% CI | p-Value |
|---|---|---|
| Age categories of caregiver (years) | ||
| 21–34 | Ref | |
| 35–45 | 0.70 (0.33, 1.50) | 0.36 |
| 46–62 | 2.08 (1.08, 3.97) | 0.03 |
| Child age (years) | ||
| 1–10 | 2.98 (1.18, 7.47) | 0.02 |
| 11–17 | Ref | |
| Education level of caregivers | ||
| Illiterate to primary | Ref | |
| Secondary | 1.41 (1.19, 2.87) | 0.04 |
| College/university | 1.92 (1.09, 4.63) | 0.01 |
| Occupation | ||
| Employed | 1.19 (0.65, 2.19) | 0.560 |
| Not employed | Ref | |
| Knowledge of hydroxyurea | ||
| Good | 1.55 (1.10, 4.78) | 0.04 |
| Moderate | 1.44 (1.04, 4.66) | 0.01 |
| Poor | Ref | |
| Number of family members using hydroxyurea | ||
| One | Ref | |
| More than one | 1.47 (0.67, 3.21) | 0.33 |
| Way to obtain hydroxyurea | ||
| Health insurance | 2.10 (0.58, 7.60) | 0.25 |
| Cash/donation | Ref | |
| Believe hydroxyurea reduces pain | ||
| Yes | 0.68 (0.27, 1.70) | 0.41 |
| No | Ref | |
| Child has health insurance | ||
| Yes | 0.96 (0.43, 2.12) | 0.91 |
| No | Ref | |
| Was hydroxyurea available when attending clinic? | ||
| Yes | 1.49 (1.03, 3.52) | 0.03 |
| No | Ref | |
| Referred | ||
| Yes | 0.41 (0.15, 1.14) | 0.09 |
| No | Ref |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Subira, M.I., Sr.; Ambrose, E.E.; Konje, E. Adherence to Hydroxyurea Therapy for Pediatric Sickle Cell Anemia in Tanzania: Evidence from Bugando Medical Centre. Int. J. Environ. Res. Public Health 2025, 22, 616. https://doi.org/10.3390/ijerph22040616
Subira MI Sr., Ambrose EE, Konje E. Adherence to Hydroxyurea Therapy for Pediatric Sickle Cell Anemia in Tanzania: Evidence from Bugando Medical Centre. International Journal of Environmental Research and Public Health. 2025; 22(4):616. https://doi.org/10.3390/ijerph22040616
Chicago/Turabian StyleSubira, Maria Inviolata, Sr., Emmanuela E. Ambrose, and Eveline Konje. 2025. "Adherence to Hydroxyurea Therapy for Pediatric Sickle Cell Anemia in Tanzania: Evidence from Bugando Medical Centre" International Journal of Environmental Research and Public Health 22, no. 4: 616. https://doi.org/10.3390/ijerph22040616
APA StyleSubira, M. I., Sr., Ambrose, E. E., & Konje, E. (2025). Adherence to Hydroxyurea Therapy for Pediatric Sickle Cell Anemia in Tanzania: Evidence from Bugando Medical Centre. International Journal of Environmental Research and Public Health, 22(4), 616. https://doi.org/10.3390/ijerph22040616