
Initial Outcomes of the Safe and Sound Protocol on Patients with Adult Autism Spectrum Disorder: Exploratory Pilot Study

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Inclusion, Exclusion, and Discontinuance Criteria
2.3. Instrumentation and Testing Environment
2.4. Assessment & Measurements
- 1.
- SRS-2 Adult Self-Report and Family-Report Forms (main outcome):
- The SRS-2 Adult Self-Report and Family-Report Forms contain 65 items that identify ASD-related social impairments and quantify their severity [26]. The response options range from 0 to 3 for each item, with a higher score indicating greater severity. The SRS-2 is a valid measure of autistic symptomatology across cultures [27,28]; moreover, it has a conceptually derived three-factor structure that is consistent with the DSM-5 criteria for ASD. Its factors are social communication impairment, restricted interests, and repetitive behaviors.
- 2.
- Center for Epidemiological Studies Depression Scale (CES-D):
- The CES-D [29] is a 20-item measure that assesses symptoms associated with depression, including restless sleep, poor appetite, and feeling lonely. The response options range from 0 to 3 for each item. Total scores range from 0 to 60, with higher scores indicating more severe depressive symptoms. Moreover, the CES-D provides cutoff scores (e.g., ≥16) that aid in identifying individuals at risk for clinical depression with good sensitivity, specificity, and high internal consistency [30].
- 3.
- State-Trait Anxiety Inventory (STAI):
- The STAI is a commonly used and reliable measure of state anxiety (A-state) and trait anxiety (A-trait) [31]. Each subscale is comprised of 20 items. All the items are rated on a 4-point scale. The total score obtained from each subscale ranges from 20 to 80, with a high score indicating a high anxiety level.
- 4.
- WHO Quality of Life 26 (WHOQOL-BREF):
- The WHOQOL-BREF, which is an abbreviated 26-item version of the WHOQOL-100, was developed as a valid and reliable alternative assessment scale using data from the field-trial version of the WHOQOL-BREF-100 [32]. Individual items were rated on a 5-point scale, with each ranging from the highest to lowest score (5–1). Scores of 1 and 5 indicate the lowest negative and highest positive perceptions, respectively. The questionnaire score ranges from 26 to 130. The first question generally evaluates QOL, while the second question evaluates health condition satisfaction. The other 24 questions were grouped into 4 domains: psychological (6 items), social (3 items), environmental (8 items), and physical domains (7 items).
- 5.
- Adolescent/Adult Sensory Profile (A/ASP):
- The A/ASP is a valid and reliable tool for assessing behavioral responses to sensory occurrences similar to daily life experiences developed by Brown and Dunn [33]. This 60-item self-report questionnaire is divided into six different categories: auditory, visual, smell/taste, touch, movement, and activity level. The evaluation identifies the sensory profile and provides the following four quadrant scores: Low Registration (poor sensory registration), Sensation Seeking, Sensory Sensitivity, and Sensation Avoiding that correspond to the quadrant scores provided by the Sensory Profile (SP).
2.5. Data Analysis
3. Results
3.1. Scores of SRS-2 Adult Self-Report and Family-Report Forms after the Safe & Sound Protocol
3.2. Correlation between Score of SRS-2 Adult Self-Report and Family-Report Forms and Secondary Outcomes
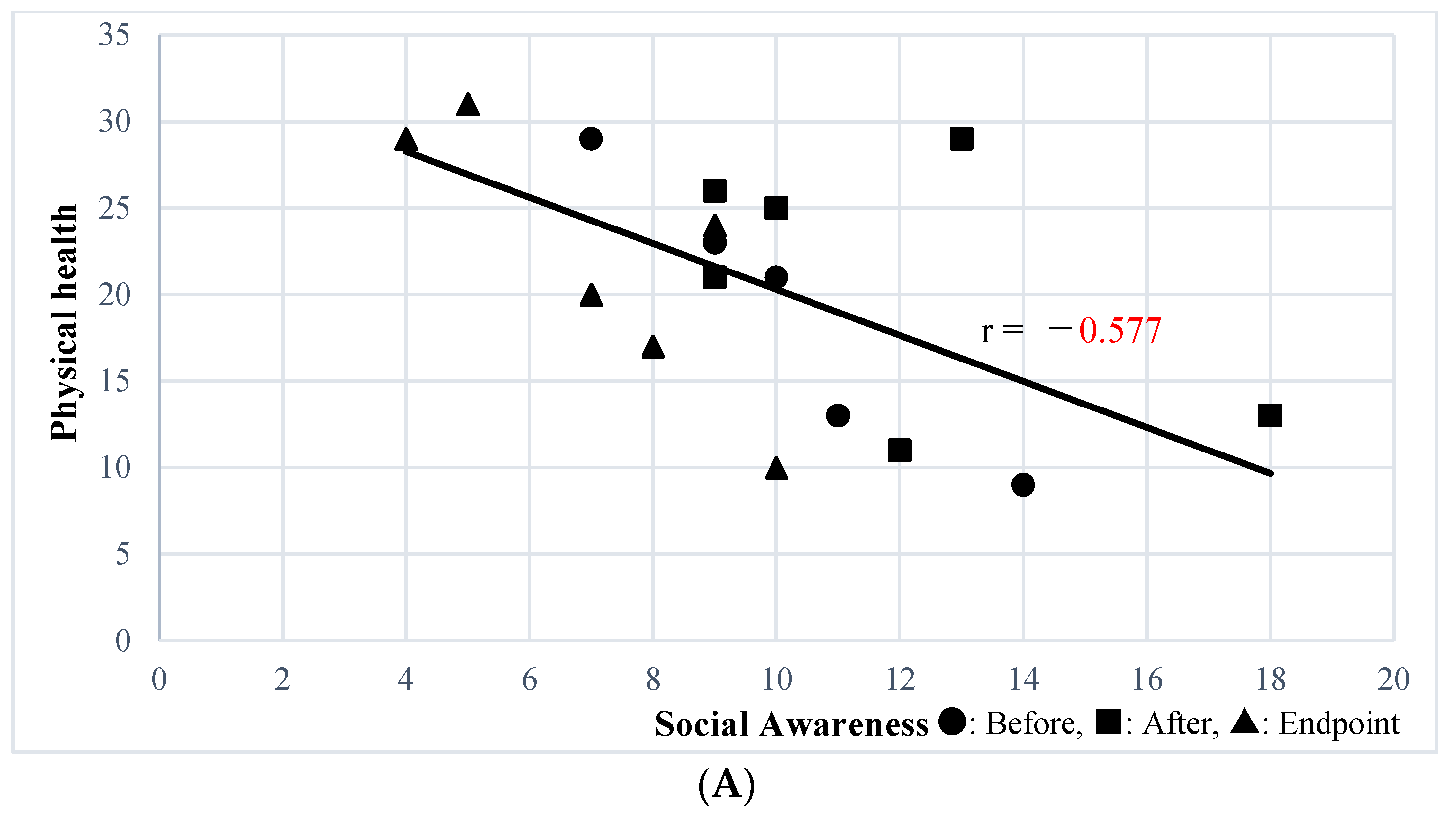
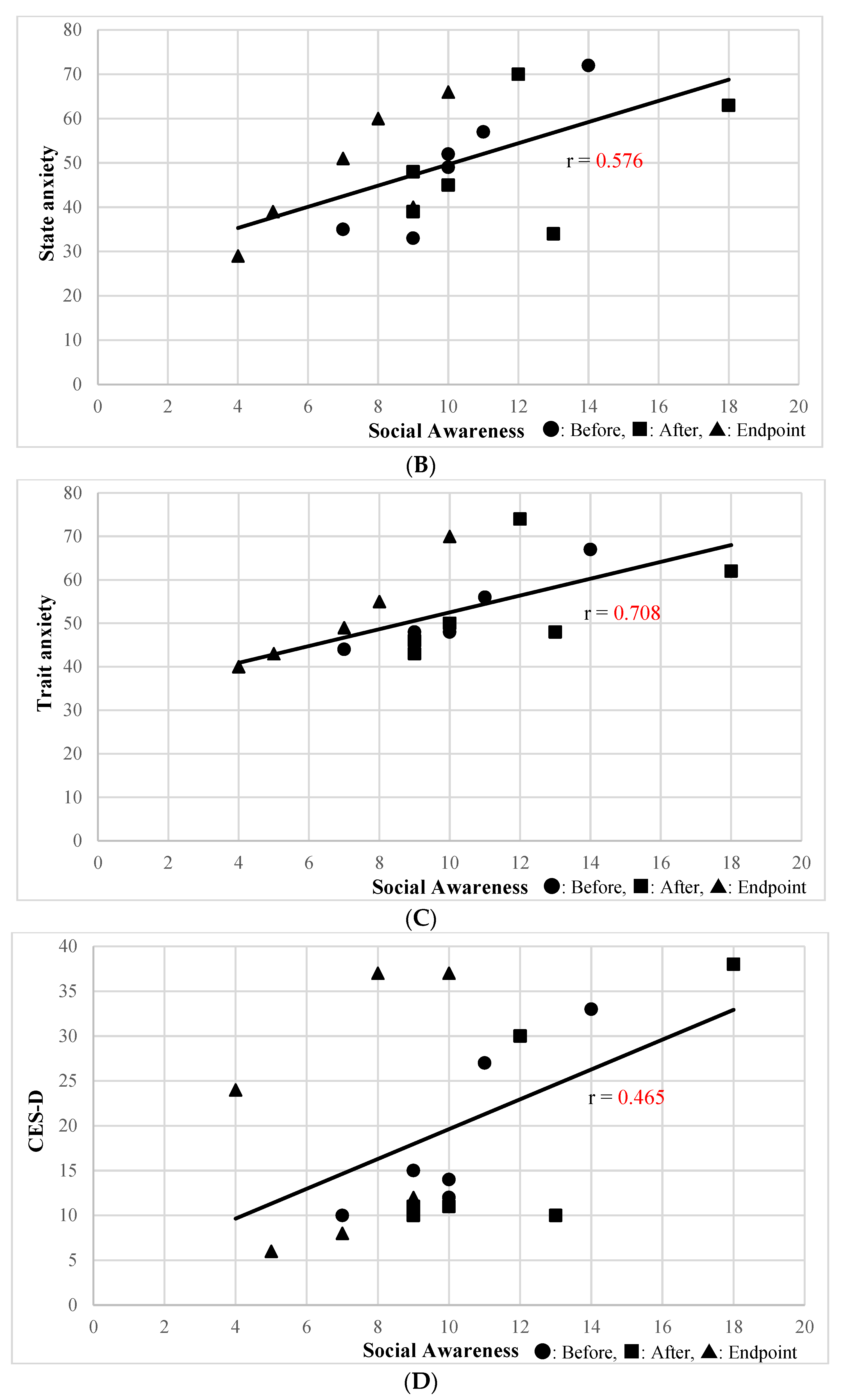
3.3. Correlation Analysis between Social Awareness Subscale of SRS-2 Adult Self-Report and Family-Report Forms and Secondary Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lyall, K.; Croen, L.; Daniels, J.; Fallin, M.D.; Ladd-acosta, C.; Lee, B.K.; Park, B.Y.; Snyder, N.W.; Schendel, D.; Volk, H.; et al. The Changing Epidemiology of Autism Spectrum Disorders. Annu. Rev. Public Health 2017, 38, 81–102. [Google Scholar] [CrossRef]
- Lewis, L.F. Identifying Autism Spectrum Disorder in Undiagnosed Adults. Nurse Pract. 2018, 43, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Wilson, C.E.; Roberts, G.; Gillan, N.; Ohlsen, C.; Robertson, D.; Zinkstok, J. The NICE Guideline on Recognition, Referral, Diagnosis and Management of Adults on the Autism Spectrum. Adv. Ment. Health Intellect. Disabil. 2013, 8, 3–14. [Google Scholar] [CrossRef]
- Vannucchi, G.; Masi, G.; Toni, C.; Dell’Osso, L.; Erfurth, A.; Perugi, G. Bipolar Disorder in Adults with Asperger׳s Syndrome: A Systematic Review. J. Affect. Disord. 2014, 168, 151–160. [Google Scholar] [CrossRef] [PubMed]
- Hollocks, M.J.; Lerh, J.W.; Magiati, I.; Meiser-Stedman, R.; Brugha, T.S. Anxiety and Depression in Adults with Autism Spectrum Disorder: A Systematic Review and Meta-Analysis. Psychol. Med. 2019, 49, 559–572. [Google Scholar] [CrossRef]
- Giuliani, F.; El Korh, P. Psychotherapy for Adults with Autistic Spectrum Disorders. Adv. Tech. Biol. Med. 2015, 4, 1. [Google Scholar] [CrossRef]
- Kose, L.K.; Fox, L.; Storch, E.A. Effectiveness of Cognitive Behavioral Therapy for Individuals with Autism Spectrum Disorders and Comorbid Obsessive-Compulsive Disorder: A Review of the Research. J. Dev. Phys. Disabil. 2018, 30, 69–87. [Google Scholar] [CrossRef] [PubMed]
- Agency for Healthcare Research and Quality Comparative Effectiveness of Therapies for Children with Autism Spectrum Disorder. 2014. Available online: https://effectivehealthcare.ahrq.gov/products/autism-update/clinician (accessed on 6 March 2023).
- Broadstock, M.; Doughty, C.; Eggleston, M. Systematic Review of the Effectiveness of Pharmacological Treatments for Adolescents and Adults with Autism Spectrum Disorder. Autism 2007, 11, 335–348. [Google Scholar] [CrossRef]
- Porges, S.W. The Polyvagal Theory: Neurophysiological Foundations of Emotions, Attachment, Communication, and Self-Regulation; W.W. Norton: New York, NY, USA, 2011; ISBN 0393707008. [Google Scholar]
- Porges, S.W. Orienting in a Defensive World: Mammalian Modifications of Our Evolutionary Heritage. Polyvagal Theory. Psychophysiology 1995, 32, 301–318. [Google Scholar] [CrossRef]
- Porges, S.W. The Polyvagal Theory: Phylogenetic Contributions to Social Behavior. Physiol. Behav. 2003, 79, 503–513. [Google Scholar] [CrossRef]
- Porges, S.W.; Bazhenova, O.V.; Bal, E.; Carlson, N.; Sorokin, Y.; Heilman, K.J.; Cook, E.H.; Lewis, G.F. Reducing Auditory Hypersensitivities in Autistic Spectrum Disorder: Preliminary Findings Evaluating the Listening Project Protocol. Front. Pediatr. 2014, 2, 80. [Google Scholar] [CrossRef]
- Porges, S.W.; Macellaio, M.; Stanfill, S.D.; McCue, K.; Lewis, G.F.; Harden, E.R.; Handelman, M.; Denver, J.; Bazhenova, O.V.; Heilman, K.J. Respiratory Sinus Arrhythmia and Auditory Processing in Autism: Modifiable Deficits of an Integrated Social Engagement System? Int. J. Psychophysiol. 2013, 88, 261–270. [Google Scholar] [CrossRef]
- Elwin, M.; Ek, L.; Schröder, A.; Kjellin, L. Autobiographical Accounts of Sensing in Asperger Syndrome and High-Functioning Autism. Arch. Psychiatr. Nurs. 2012, 26, 420–429. [Google Scholar] [CrossRef] [PubMed]
- Robertson, A.E.; Simmons, D.R. The Sensory Experiences of Adults with Autism Spectrum Disorder A Qualitative Analysis. Perception 2015, 44, 569–586. [Google Scholar] [CrossRef]
- Weitlauf, A.S.; Sathe, N.; McPheeters, M.L.; Warren, Z.E. Interventions Targeting Sensory Challenges in Autism Spectrum Disorder: A Systematic Review. Pediatrics 2017, 139, e20170347. [Google Scholar] [CrossRef]
- Sinha, Y.; Silove, N.; Wheeler, D.; Williams, K. Auditory Integration Training and Other Sound Therapies for Autism Spectrum Disorders: A Systematic Review. Arch. Dis. Child. 2006, 91, 1018–1022. [Google Scholar] [CrossRef]
- Anita, C.; Bundy, S.J.L. Sensory Integration: Theory and Practice, 3rd ed.; F.A. Davis Company: Philadelphia, PA, USA, 2019. [Google Scholar]
- Schoen, S.A.; Lane, S.J.; Mailloux, Z.; May-Benson, T.; Parham, L.D.; Smith Roley, S.; Schaaf, R.C. A Systematic Review of Ayres Sensory Integration Intervention for Children with Autism. Autism Res. 2019, 12, 6–19. [Google Scholar] [CrossRef]
- Petralia, R.S.; Mattson, M.P.; Yao, P.J. Communication Breakdown: The Impact of Ageing on Synapse Structure. Ageing Res. Rev. 2014, 14, 31. [Google Scholar] [CrossRef]
- Schoen, S.A.; Miller, L.J.; Sullivan, J. A Pilot Study of Integrated Listening Systems for Children with Sensory Processing Problems. J. Occup. Ther. Sch. Early Interv. 2015, 8, 256–276. [Google Scholar] [CrossRef]
- Gotham, K.; Risi, S.; Pickles, A.; Lord, C. The Autism Diagnostic Observation Schedule: Revised Algorithms for Improved Diagnostic Validity. J. Autism Dev. Disord. 2007, 37, 613–627. [Google Scholar] [CrossRef]
- Lord, C.; Risi, S.; Lambrecht, L.; Cook, E.H.; Leventhal, B.L.; DiLavore, P.C.; Pickles, A.; Rutter, M. The Autism Diagnostic Observation Schedule-Generic: A Standard Measure of Social and Communication Deficits Associated with the Spectrum of Autism. J. Autism Dev. Disord. 2000, 30, 205–223. [Google Scholar] [CrossRef]
- Porges, S.W.; Lewis, G.F. The Polyvagal Hypothesis: Common Mechanisms Mediating Autonomic Regulation, Vocalizations and Listening; Elsevier: Amsterdam, The Netherlands, 2010; Volume 19, ISBN 9780123745934. [Google Scholar]
- Constantino, J.; Gruber, C. Social Responsiveness Scale: SRS-2; Western Psychological Services: Torrance, CA, USA, 2012. [Google Scholar]
- Bölte, S.; Poustka, F.; Constantino, J.N. Assessing Autistic Traits: Cross-Cultural Validation of the Social Responsiveness Scale (SRS). Autism Res. 2008, 1, 354–363. [Google Scholar] [CrossRef] [PubMed]
- Wigham, S.; McConachie, H.; Tandos, J.; Le Couteur, A.S. The Reliability and Validity of the Social Responsiveness Scale in a UK General Child Population. Res. Dev. Disabil. 2012, 33, 944–950. [Google Scholar] [CrossRef]
- Radloff, L.S. The CES-D Scale. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Lewinsohn, P.M.; Seeley, J.R.; Roberts, R.E.; Allen, N.B. Center for Epidemiologic Studies Depression Scale (CES-D) as a Screening Instrument for Depression among Community-Residing Older Adults. Psychol. Aging 1997, 12, 277–287. [Google Scholar] [CrossRef]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R. STAI Manual for the State-Trait Anxiety Inventory (“Self-Evaluation Questionnaire”); Consulting Psychologists Press: Palo Alto, CA, USA, 1970. [Google Scholar]
- The WHOQOL Group. Development of the World Health Organization WHOQOL-BREF Quality of Life Assessment. Psychol. Med. 1998, 28, 551–558. [Google Scholar] [CrossRef]
- Brown, C.; Tollefson, N.; Dunn, W.; Cromwell, R.; Filion, D. The Adult Sensory Profile: Measuring Patterns of Sensory Processing. Am. J. Occup. Ther. 2001, 55, 75–82. [Google Scholar] [CrossRef]
- Thye, M.D.; Bednarz, H.M.; Herringshaw, A.J.; Sartin, E.B.; Kana, R.K. The Impact of Atypical Sensory Processing on Social Impairments in Autism Spectrum Disorder. Dev. Cogn. Neurosci. 2018, 29, 151–167. [Google Scholar] [CrossRef]
- Kojovic, N.; Ben Hadid, L.; Franchini, M.; Schaer, M. Sensory Processing Issues and Their Association with Social Difficulties in Children with Autism Spectrum Disorders. J. Clin. Med. 2019, 8, 1508. [Google Scholar] [CrossRef]
- Hilton, C.; Graver, K.; LaVesser, P. Relationship between Social Competence and Sensory Processing in Children with High Functioning Autism Spectrum Disorders. Res. Autism Spectr. Disord. 2007, 1, 164–173. [Google Scholar] [CrossRef]
- Crane, L.; Goddard, L.; Pring, L. Sensory Processing in Adults with Autism Spectrum Disorders. Autism 2009, 13, 215–228. [Google Scholar] [CrossRef]
- Seltzer, M.M.; Shattuck, P.; Abbeduto, L.; Greenberg, J.S. Trajectory of Development in Adolescents and Adults with Autism. Ment. Retard. Dev. Disabil. Res. Rev. 2004, 10, 234–247. [Google Scholar] [CrossRef]
- McGovern, C.W.; Sigman, M. Continuity and Change from Early Childhood to Adolescence in Autism. J. Child Psychol. Psychiatry Allied Discip. 2005, 46, 401–408. [Google Scholar] [CrossRef]
- Sereda, M.; Xia, J.; El Refaie, A.; Hall, D.A.; Hoare, D.J. Sound Therapy (Using Amplification Devices and/or Sound Generators) for Tinnitus. Cochrane Database Syst. Rev. 2018, 12, CD013094. [Google Scholar]



{kind=link}
{kind=link}
| No. | Sex | Age | Occupation | History of Psychiatric Disorder | SRS2 Family-Report Evaluator |
|---|---|---|---|---|---|
| 1 | Male | 21 | student | adjustment disorder | mother |
| 2 | Male | 24 | unemployed | adjustment disorder | mother |
| 3 | Female | 30 | unemployed | adjustment disorder | mother |
| 4 | Male | 23 | unemployed | adjustment disorder | mother |
| 5 | Female | 44 | housewife | None | husband |
| 6 | Female | 21 | student | None | mother |
| SRS-2 Self-Report | Mean Value ± SD | df | p Value | |||
|---|---|---|---|---|---|---|
| Before | After | Endpoint | Before and After | Before and Endpoint | ||
| Social Awareness | 12 ± 2.6 | 12.1 ± 5 | 13.6 ± 2.6 | 16 | 0.498 | 0.197 |
| Social Cognition | 19.1 ± 4.9 | 16.6 ± 7.3 | 19.5 ± 4.9 | 16 | 0.136 | 0.516 |
| Social Communication | 37.1 ± 9.4 | 36.1 ± 13.8 | 36.1 ± 8.4 | 16 | 1 | 0.753 |
| Social Motivation | 24.6 ± 4.7 | 23.8 ± 5.7 | 23.8 ± 4.9 | 16 | 0.236 | 0.496 |
| Restricted Interests and Repetitive Behavior | 18.8 ± 4.9 | 18.6 ± 8 | 19.1 ± 6.7 | 16 | 0.753 | 1 |
| Total Score | 111.8 ± 18.1 | 107.5 ± 36.7 | 112.3 ± 21.3 | 16 | 0.833 | 0.753 |
| SRS-2 Family Report | Mean Value ± SD | df | p Value | |||
| Before | After | Endpoint | Before and After | Before and Endpoint | ||
| Social Awareness | 10.1 ± 2.3 | 11.8 ± 3.4 | 7.1 ± 2.3 | 16 | 0.596 | 0.027 * |
| Social Cognition | 12 ± 4.2 | 14.8 ± 7 | 11.3 ± 5.6 | 16 | 0.131 | 0.414 |
| Social Communication | 22.1 ± 10.3 | 31.1 ± 14.1 | 21.8 ± 9.7 | 16 | 0.116 | 0.917 |
| Social Motivation | 14.1 ± 7 | 17.1 ± 5.7 | 15.6 ± 7.3 | 16 | 0.093 | 0.223 |
| Restricted Interests and Repetitive Behavior | 12.1 ± 6.8 | 15.1 ± 9.1 | 12.6 ± 7.2 | 16 | 0.144 | 0.414 |
| Total Score | 70.6 ± 22.5 | 90.1 ± 34.8 | 68.6 ± 24.6 | 16 | 0.116 | 0.786 |
| SRS-2 Self-Report | Adolescent/Adult Sensory Profile | |||
|---|---|---|---|---|
| Low Registration | Sensation Seeking | Sensory Sensitivity | Sensation Avoiding | |
| Social Awareness | 0.347 | −0.442 | 0.459 | 0.347 |
| Social Cognition | 0.587 ** | −0.421 | 0.295 | 0.313 |
| Social Communication | 0.348 | −0.396 | −0.115 | −0.0006 |
| Social Motivation | 0.589 * | −0.710 *** | 0.318 | 0.562 * |
| Restricted Interests and Repetitive Behavior | 0.696 ** | −0.219 | 0.401 | 0.313 |
| Total Score | 0.487 * | −0.572 * | 0.09 | 0.179 |
| SRS-2 Family-Report | Adolescent/Adult Sensory Profile | |||
| Low Registration | Sensation Seeking | Sensory Sensitivity | Sensation Avoiding | |
| Social Awareness | 0.519 * | −0.212 | 0.368 | 0.399 |
| Social Cognition | 0.764 *** | −0.133 | 0.651 ** | 0.620 ** |
| Social Communication | 0.211 | −0.191 | −0.048 | −0.07 |
| Social Motivation | −0.021 | −0.456 | −0.107 | −0.030 |
| Restricted Interests and Repetitive Behavior | 0.580 * | −0.223 | 0.442 | 0.350 |
| Total Score | 0.470 * | −0.107 | 0.220 | 0.157 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kawai, H.; Kishimoto, M.; Okahisa, Y.; Sakamoto, S.; Terada, S.; Takaki, M. Initial Outcomes of the Safe and Sound Protocol on Patients with Adult Autism Spectrum Disorder: Exploratory Pilot Study. Int. J. Environ. Res. Public Health 2023, 20, 4862. https://doi.org/10.3390/ijerph20064862
Kawai H, Kishimoto M, Okahisa Y, Sakamoto S, Terada S, Takaki M. Initial Outcomes of the Safe and Sound Protocol on Patients with Adult Autism Spectrum Disorder: Exploratory Pilot Study. International Journal of Environmental Research and Public Health. 2023; 20(6):4862. https://doi.org/10.3390/ijerph20064862
Chicago/Turabian StyleKawai, Hiroki, Makiko Kishimoto, Yuko Okahisa, Shinji Sakamoto, Seishi Terada, and Manabu Takaki. 2023. "Initial Outcomes of the Safe and Sound Protocol on Patients with Adult Autism Spectrum Disorder: Exploratory Pilot Study" International Journal of Environmental Research and Public Health 20, no. 6: 4862. https://doi.org/10.3390/ijerph20064862
APA StyleKawai, H., Kishimoto, M., Okahisa, Y., Sakamoto, S., Terada, S., & Takaki, M. (2023). Initial Outcomes of the Safe and Sound Protocol on Patients with Adult Autism Spectrum Disorder: Exploratory Pilot Study. International Journal of Environmental Research and Public Health, 20(6), 4862. https://doi.org/10.3390/ijerph20064862