
Methods and Tools Used to Estimate the Shortages of Medical Staff in European Countries—Scoping Review



Abstract
1. Introduction
2. Materials and Methods
2.1. Defining Research Questions
- RQ1—What kinds of publications and research were carried out?
- RQ2—Which countries are included in the study?
- RQ3—Which professional groups are covered by the study?
- RQ4—What kinds of methods, tools, and procedures were used?
- RQ5—Which organizations/stakeholders are involved in predicting HWF shortages?
- RQ6—What results and conclusions were stated?
- RQ7—What are the research gaps for future studies?
2.2. Study Search
2.3. Selection of Publications
2.4. Data Extraction
2.5. Gathering and Reporting the Results
3. Results
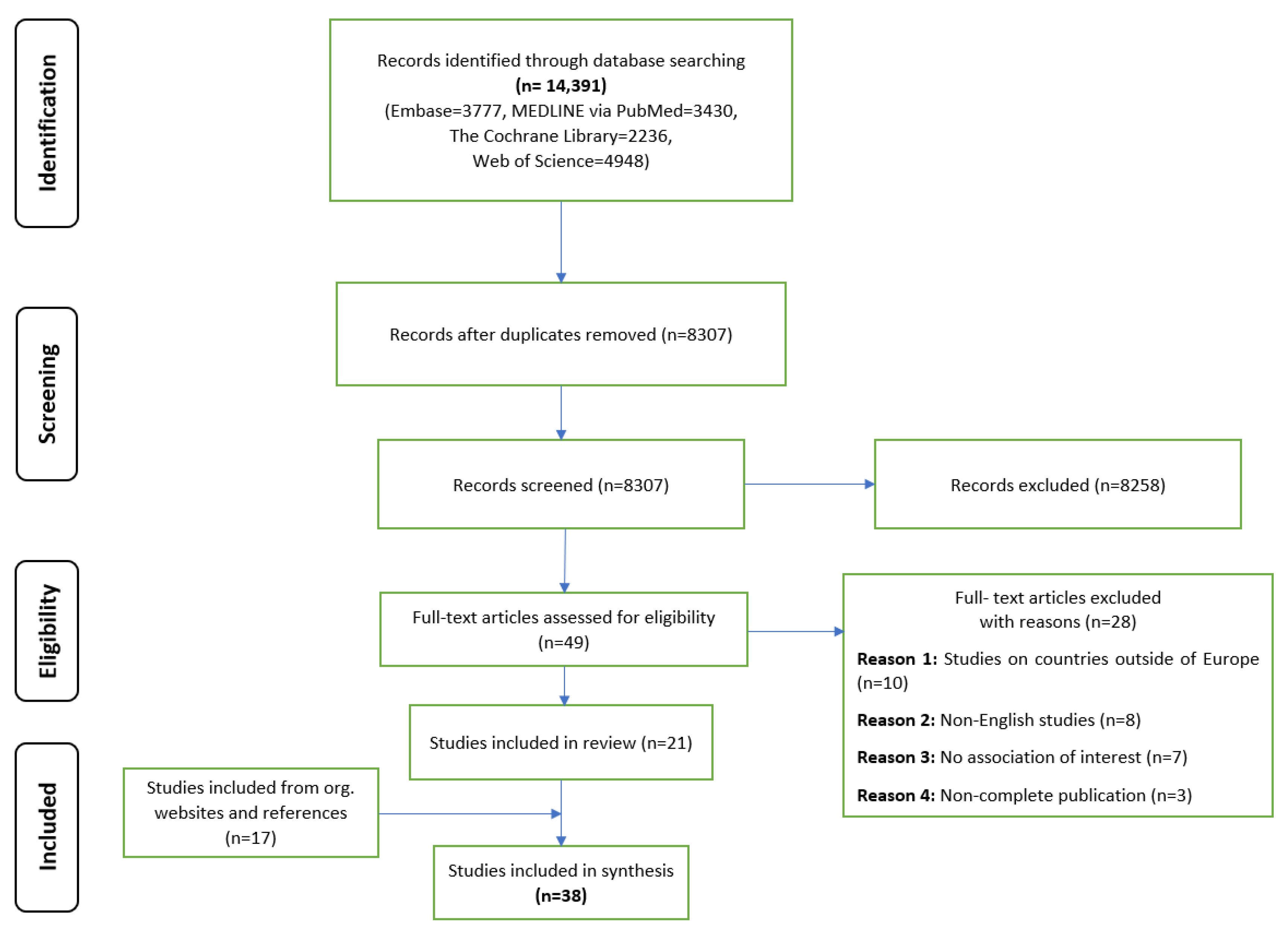
3.1. Search Results
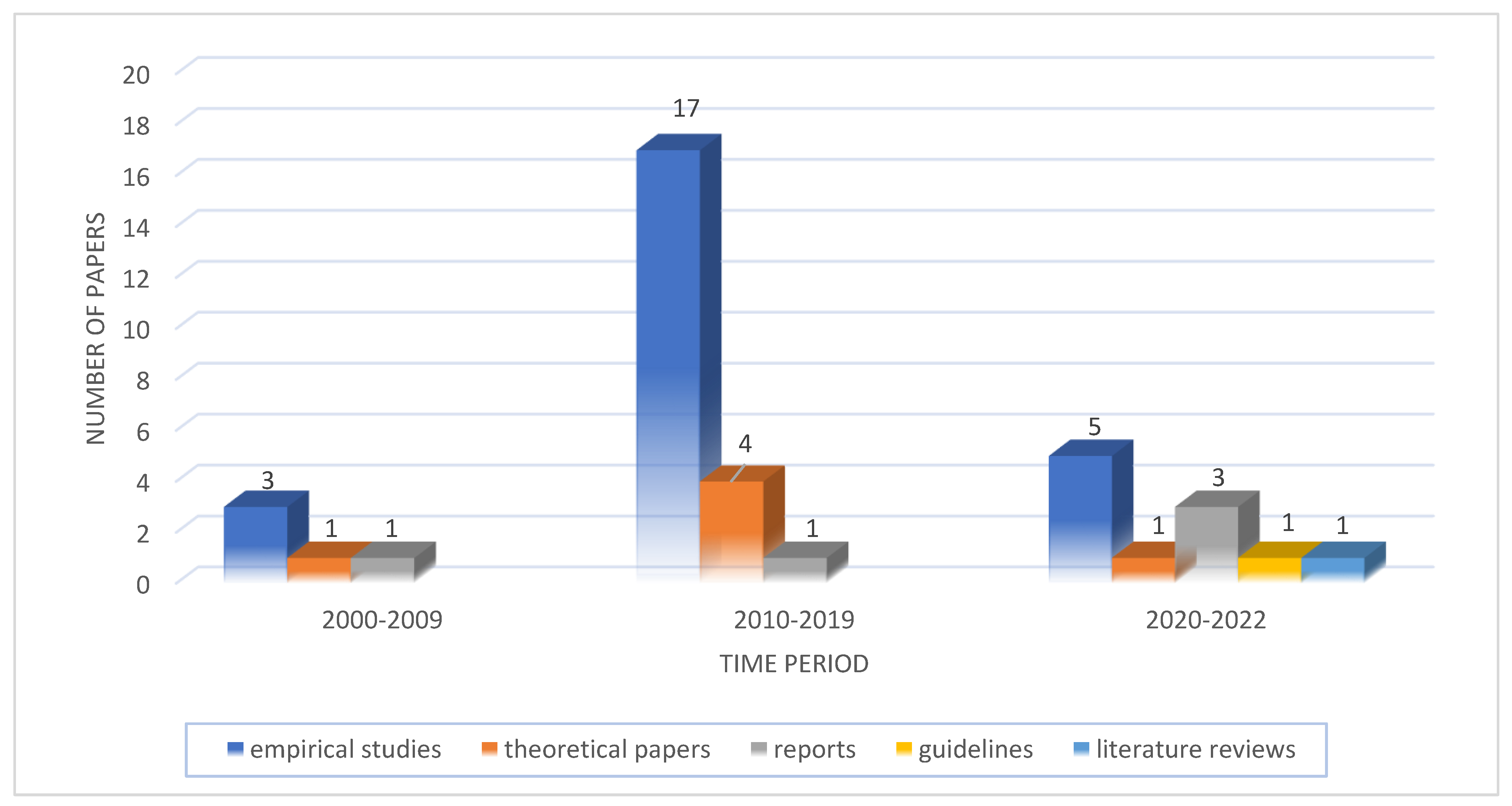
3.2. Characteristics of the Studies Included
3.3. Countries Covered in the Included Publications
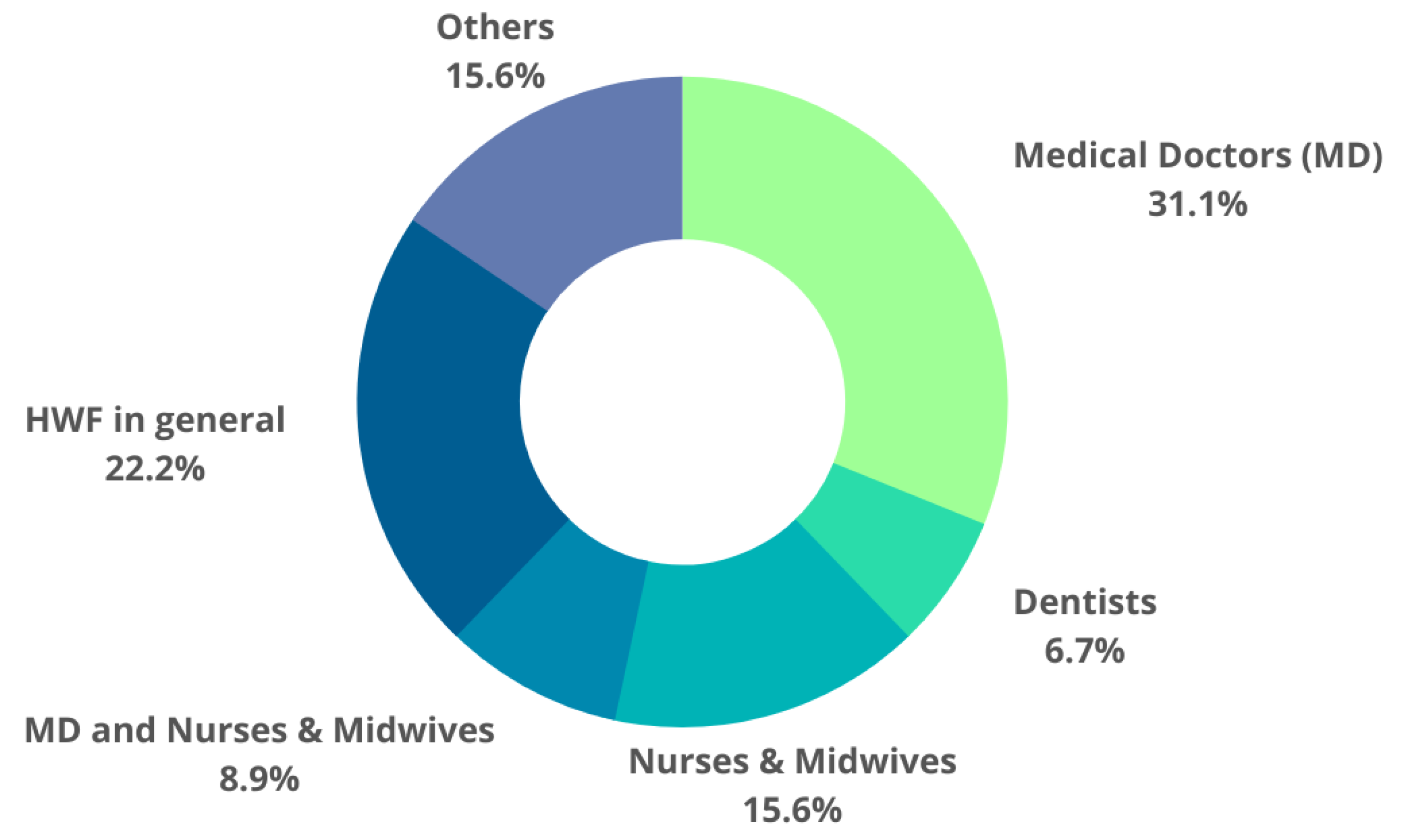
3.4. Professional Groups Covered by the Publications
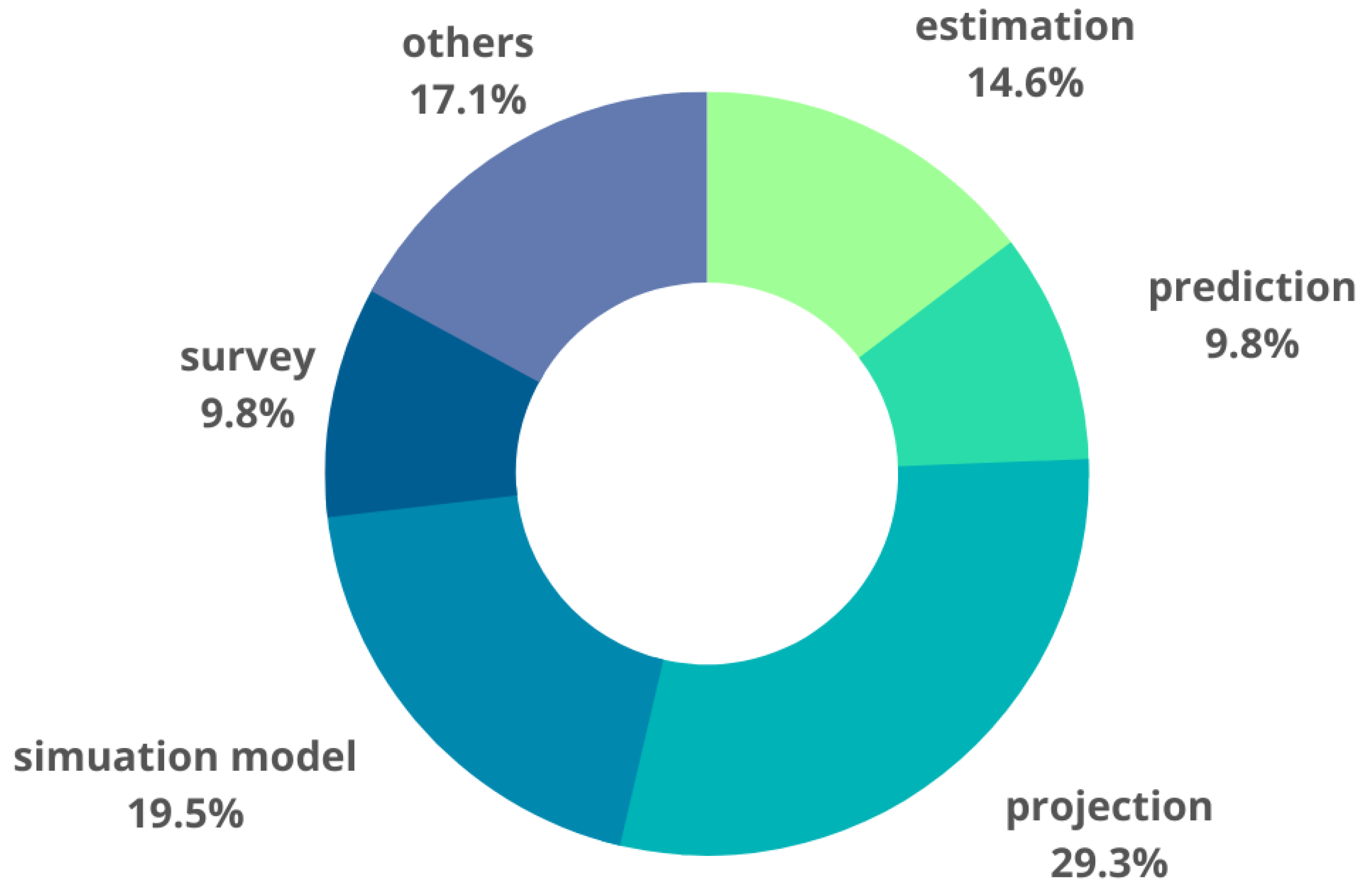
3.5. Methods, Tools, and Procedures Applied in the Identified Studies
3.6. Organizations/Stakeholders Involved in the Process of the Measurement of HWF Shortages
3.7. Results and Conclusions Achieved
3.8. Research Gaps for Future Studies
4. Discussion
4.1. Results Summary
4.2. Discussion
4.3. Limitations and Implications of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Regional Office for Europe. Health and Care Workforce in Europe: Time to Act; World Health Organization. Regional Office for Europe: Copenhagen, Denmark, 2022; ISBN 9789289058339. [Google Scholar]
- Tomblin Murphy, G.; Birch, S.; MacKenzie, A.; Bradish, S.; Elliott Rose, A. A Synthesis of Recent Analyses of Human Resources for Health Requirements and Labour Market Dynamics in High-Income OECD Countries. Hum. Resour. Health 2016, 14, 59. [Google Scholar] [CrossRef] [PubMed]
- Kuhlmann, E.; Batenburg, R.; Wismar, M.; Dussault, G.; Maier, C.B.; Glinos, I.A.; Azzopardi-Muscat, N.; Bond, C.; Burau, V.; Correia, T.; et al. A Call for Action to Establish a Research Agenda for Building a Future Health Workforce in Europe. Health Res. Policy Syst. 2018, 16, 52. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Strategy on Human Resources for Health: Workforce 2030; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- World Health Organization. Working for Health and Growth: Investing in the Health Workforce—Report of the High-Level Commission on Health Employment and Economic Growth; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- OECD/European Union. Health at a Glance: Europe 2020: State of Health in the EU Cycle; OECD Publishing: Paris, France, 2020. [Google Scholar]
- da Silva, K.R.; de Souza, F.G.; Roquete, F.F.; da Costa Faria, S.M.; Peixoto, B.C.F.; Vieira, A. Allocation of Resources for Health Care in COVID-19 Pandemic Times: Integrative Review. Rev. Bras. Enferm. 2020, 73, e20200244. [Google Scholar] [CrossRef] [PubMed]
- Bourgeault, I.L.; Maier, C.B.; Dieleman, M.; Ball, J.; MacKenzie, A.; Nancarrow, S.; Nigenda, G.; Sidat, M. The COVID-19 Pandemic Presents an Opportunity to Develop More Sustainable Health Workforces. Hum. Resour. Health 2020, 18, 83. [Google Scholar] [PubMed]
- Ono, T.; Lafortune, G.; Schoenstein, M. Health Workforce Planning in OECD Countries: A Review of 26 Projection Models from 18 Countries; OECD Publishing: Paris, France, 2013. [Google Scholar]
- Lopes, M.A.; Almeida, Á.S.; Almada-Lobo, B. Handling Healthcare Workforce Planning with Care: Where Do We Stand? Hum. Resour. Health 2015, 13, 38. [Google Scholar] [PubMed]
- Hall, T.L.; Mejía, A.; Albul, K.V. Health Manpower Planning: Principles, Methods, Issues; World Health Organization: Geneva, Switzerland, 1978; ISBN 924154130X. [Google Scholar]
- Subramanian, L. Effective Demand Forecasting in Health Supply Chains: Emerging Trend, Enablers, and Blockers. Logistics 2021, 5, 12. [Google Scholar] [CrossRef]
- Drennan, V.M.; Ross, F. Global Nurse Shortages-the Facts, the Impact and Action for Change. Br. Med. Bull. 2019, 130, 25–37. [Google Scholar] [CrossRef]
- Shembavnekar, N.; Buchan, J.; Bazeer, N.; Kelly, E.; Beech, J.; Charlesworth, A.; Mcconkey, R.; Fisher, R. NHS Workforce Projections 2022; The Health Foundation: London, UK, 2022. [Google Scholar]
- World Health Organization. Health Labour Market Analysis Guidebook; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Schneider, M. Health Workforce Shortage in EU27 in the Light of Accounting Systems; BASYS: Augsburg, Germany, 2021. [Google Scholar]
- Kovács, E.; Szegner, P.; Langner, L.; Sziklai, M.; Szócska, M.; Sermeus, W.; Van Hoegaerden, M.; Van Deun, E.; Snyers, B. Mapping of National Health Workforce Planning and Policies in the EU-28; EU Publications: Luxembourg, 2021. [Google Scholar]
- Arksey, H.; O’Malley, L. Scoping Studies: Towards a Methodological Framework. Int. J. Soc. Res. Methodol. Theory Pract. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Teare, G.; Taks, M. Extending the Scoping Review Framework: A Guide for Interdisciplinary Researchers. Int. J. Soc. Res. Methodol. 2020, 23, 311–315. [Google Scholar]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Open Science Framework. Open Science Framework Registries. Available online: https://osf.io/gkmv7 (accessed on 26 December 2022).
- Johnson, N.; Phillips, M. Rayyan for Systematic Reviews. J. Electron. Resour. Librariansh. 2018, 30, 46–48. [Google Scholar] [CrossRef]
- Kirch, D.G.; Henderson, M.K.; Dill, M.J. Physician Workforce Projections in an Era of Health Care Reform. Annu. Rev. Med. 2012, 63, 435–445. [Google Scholar] [PubMed]
- Morgan, P. Predicted Shortages of Physicians Might Even Disappear If We Fully Account for PAs and NPs. J. Am. Acad. PAs 2019, 32, 51–53. [Google Scholar] [CrossRef] [PubMed]
- Pando-Ezcurra, T.; Auccahuasi, W.; Saenz Arenas, E.R.; Rosario Pacahuala, E.A.; González Ponce de León, E.R.; Olaya Cotera, S.; Flores Castañeda, R.O.; Herrera, L. Method for the Analysis of Health Personnel Availability in a Pandemic Crisis Scenario through Monte Carlo Simulation. Appl. Sci. 2022, 12, 8299. [Google Scholar] [CrossRef]
- Van Greuningen, M.; Batenburg, R.S.; Van der Velden, L.F. Ten Years of Health Workforce Planning in the Netherlands: A Tentative Evaluation of GP Planning as an Example. Hum. Resour. Health 2012, 10, 21. [Google Scholar] [CrossRef]
- Pandit, J.J.; Tavare, A.N.; Millard, P. Why Are There Local Shortfalls in Anaesthesia Consultant Staffing?: A Case Study of Operational Workforce Planning. J. Health Organ. Manag. 2010, 24, 4–21. [Google Scholar] [CrossRef]
- Maier, T.; Afentakis, A. Forecasting Supply and Demand in Nursing Professions: Impacts of Occupational Flexibility and Employment Structure in Germany. Hum. Resour. Health 2013, 11, 24. [Google Scholar] [CrossRef]
- Tsiouli, K.; Karamesinis, K.; Antonarakis, G.S.; Christou, P. Prediction Model of Regional Orthodontic Workforce Needs, Using Greece as an Example. Eur. J. Paediatr. Dent. 2016, 17, 29–33. [Google Scholar]
- Lovkyte, L.; Reamy, J.; Padaiga, Z. Physicians Resources in Lithuania: Change Comes Slowly. Croat. Med. J. 2003, 44, 207–213. [Google Scholar]
- Stierli, R.; Rozsnyai, Z.; Felber, R.; Jörg, R.; Kraft, E.; Exadaktylos, A.K.; Streit, S. Primary Care Physician Workforce 2020 to 2025—A Cross-Sectional Study for the Canton of Bern. Swiss Med. Wkly. 2021, 151, w30024. [Google Scholar] [CrossRef]
- Barber, P.; López-Valcárcel, B.G. Forecasting the Need for Medical Specialists in Spain: Application of a System Dynamics Model. Hum. Resour. Health 2010, 8, 24. [Google Scholar] [CrossRef]
- Grech, V.; Cassar, M.; Distefano, S. Nurse Staffing Levels on the NPICU in the Island of Malta. J. Pediatr. Intensive Care 2012, 1, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Papp, M.; Korosi, L.; Sandor, J.; Nagy, C.; Juhasz, A.; Adany, R. Workforce Crisis in Primary Healthcare Worldwide: Hungarian Example in a Longitudinal Follow-up Study. BMJ Open 2019, 9, e024957. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.X.; Goryakin, Y.; Maeda, A.; Bruckner, T.; Scheffler, R. Global Health Workforce Labor Market Projections for 2030. Hum. Resour. Health 2017, 15, 11. [Google Scholar] [CrossRef] [PubMed]
- Scheffler, R.M.; Liu, J.X.; Kinfu, Y.; Dal Poz, M.R. Forecasting the Global Shortage of Physicians: An Economic- and Needs-Based Approach. Bull. World Health Organ. 2008, 86, 516–523. [Google Scholar] [CrossRef] [PubMed]
- Scheffler, R.M.; Campbell, J.; Cometto, G.; Maeda, A.; Liu, J.; Bruckner, T.A.; Arnold, D.R.; Evans, T. Forecasting Imbalances in the Global Health Labor Market and Devising Policy Responses. Hum. Resour. Health 2018, 16, 5. [Google Scholar] [CrossRef]
- Taylor, C.; McManus, I.C.; Davison, I. Would Changing the Selection Process for GP Trainees Stem the Workforce Crisis? A Cohort Study Using Multiple-Imputation and Simulation. BMC Med. Educ. 2018, 18, 81. [Google Scholar] [CrossRef]
- Lodi, A.; Tubertini, P.; Grilli, R.; Mazzocchetti, A.; Ruozi, C.; Senese, F. Needs Forecast and Fund Allocation of Medical Specialty Positions in Emilia-Romagna (Italy) by System Dynamics and Integer Programming. Health Syst. 2016, 5, 213–236. [Google Scholar]
- Gialama, F.; Saridi, M.; Prezerakos, P.; Pollalis, Y.; Contiades, X.; Souliotis, K. The Implementation Process of the Workload Indicators Staffing Need (WISN) Method by WHO in Determining Midwifery Staff Requirements in Greek Hospitals. Eur. J. Midwifery 2019, 3, 1. [Google Scholar] [CrossRef]
- Van Greuningen, M. Health Workforce Planning in the Netherlands; Tilburg University: Utrecht, The Netherlands, 2016. [Google Scholar]
- Gallagher, J.E.; Kleinman, E.R.; Harper, P.R. Modelling Workforce Skill-Mix: How Can Dental Professionals Meet the Needs and Demands of Older People in England? Br. Dent. J. 2010, 208, E6. [Google Scholar] [CrossRef]
- Starkiene, L.; Smigelskas, K.; Padaiga, Z.; Reamy, J. The Future Prospects of Lithuanian Family Physicians: A 10-Year Forecasting Study. BMC Fam. Pract. 2005, 6, 41. [Google Scholar] [CrossRef]
- Ravindran, S.; Munday, J.; Veitch, A.M.; Broughton, R.; Thomas-Gibson, S.; Penman, I.D.; McKinlay, A.; Fearnhead, N.S.; Coleman, M.; Logan, R. Bowel Cancer Screening Workforce Survey: Developing the Endoscopy Workforce for 2025 and Beyond. Frontline Gastroenterol. 2022, 13, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Teljeur, C.; Thomas, S.; O’Kelly, F.D.; O’Dowd, T. General Practitioner Workforce Planning: Assessment of Four Policy Directions. BMC Health Serv. Res. 2010, 10, 148. [Google Scholar] [CrossRef] [PubMed]
- Harkin, D.W.; Beard, J.D.; Shearman, C.P.; Wyatt, M.G.; Surg, R.C. Predicted Shortage of Vascular Surgeons in the United Kingdom: A Matter for Debate? Surgeon 2016, 14, 245–251. [Google Scholar] [CrossRef]
- Hegarty, H.; Knight, T.; Atkin, C.; Kelly, T.; Subbe, C.; Lasserson, D.; Holland, M. Nurse Staffing Levels within Acute Care: Results of a National Day of Care Survey. BMC Health Serv. Res. 2022, 22, 493. [Google Scholar] [CrossRef]
- Maresova, P.; Prochazka, M.; Barakovic, S.; Baraković Husić, J.; Kuca, K. A Shortage in the Number of Nurses-A Case Study from a Selected Region in the Czech Republic and International Context. Healthcare 2020, 8, 152. [Google Scholar] [CrossRef] [PubMed]
- Tsai, T.-C.; Eliasziw, M.; Chen, D.-F. Predicting the Demand of Physician Workforce: An International Model Based on “Crowd Behaviors”. BMC Health Serv. Res. 2012, 12, 79. [Google Scholar] [CrossRef] [PubMed]
- Boniol, M.; Kunjumen, T.; Nair, T.S.; Siyam, A.; Campbell, J.; Diallo, K. The Global Health Workforce Stock and Distribution in 2020 and 2030: A Threat to Equity and “universal” Health Coverage? BMJ Glob. Health 2022, 7, 009316. [Google Scholar] [CrossRef]
- Dussault, G.; Buchan, J.; Sermeus, W.; Padaiga, Z. Assessing Future Health Workforce Needs; World Health Organization: Copenhagen, Denmark, 2010. [Google Scholar]
- Mara, I. Health Professionals Wanted: Chain Mobility across European Countries; Research Report; The Vienna Institute for International Economic Studies (wiiw): Vienna, Austria, 2020. [Google Scholar]
- Roberfroid, D.; Stordeur, S.; Camberlin, C.; Van de Voorde, C.; Vrijens, F.; Leonard, C. Physician Workforce Supply in Belgium: Current Situation and Challenges; Belgian Health Care Knowledge Centre: Brussels, Belgium, 2008. [Google Scholar]
- World Health Organization. Models and Tools for Health Workforce Planning and Projections; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Kroezen, M.; Van Hoegaerden, M.; Batenburg, R. The Joint Action on Health Workforce Planning and Forecasting: Results of a European Programme to Improve Health Workforce Policies. Health Policy 2018, 122, 87–93. [Google Scholar] [CrossRef]
- Simoens, S.; Villeneuve, M.; Hurst, J. Tackling Nurse Shortages in OECD Countries; OECD: Paris, France, 2005. [Google Scholar]
- Malgieri, A.; Michelutti, P.; Van Hoegaerden, M. Handbook on Health Workforce Planning Methodologies across EU Countries; Ministry of Health of the Slovak Republic: Bratislava, Slovakia, 2015. [Google Scholar]
- MacKenzie, A.; Tomblin Murphy, G.; Audas, R. A Dynamic, Multi-Professional, Needs-Based Simulation Model to Inform Human Resources for Health Planning. Hum. Resour. Health 2019, 17, 42. [Google Scholar]
- Hurst, K.; Ford, J.; Keen, J.; Mottram, S.; Robinson, M. Selecting and Applying Methods for Estimating the Size and Mix of Nursing Teams: A Systematic Review of Literature Commissioned by Department of Health; Nuffield Institute for Health: Leeds, UK, 2002. [Google Scholar]
- Lakhan, S.E.; Laird, C. Addressing the Primary Care Physician Shortage in an Evolving Medical Workforce. Int. Arch. Med. 2009, 2, 14. [Google Scholar] [CrossRef] [PubMed]
- Birch, S.; Kephart, G.; Tomblin-Murphy, G.; O’Brien-Pallas, L.; Alder, R.; MacKenzie, A. Human Resources Planning and the Production of Health: A Needs-Based Analytical Framework. Can. Public Policy 2007, 33, S1–S16. [Google Scholar] [CrossRef]
- Birch, S.; Kephart, G.; Murphy, G.T.; O’Brien-Pallas, L.; Alder, R.; MacKenzie, A. Health Human Resources Planning and the Production of Health: Development of an Extended Analytical Framework for Needs-Based Health Human Resources Planning. J. Public Health Manag. Pract. 2009, 15, S56–S61. [Google Scholar] [PubMed]
- Goodman, D.C.; Fisher, E.S.; Bubolz, T.A.; Mohr, J.E.; Poage, J.F.; Wennberg, J.E. Benchmarking the US Physician Workforce: An Alternative to Needs-Based or Demand-Based Planning. JAMA 1996, 276, 1811–1817. [Google Scholar] [PubMed]
- Sloan, F.A. Access to Medical Care and the Local Supply of Physicians. Med. Care 1977, 15, 338–346. [Google Scholar] [PubMed]
- Lomas, J.; Stoddart, G.L.; Barer, M.L. Supply Projections as Planning: A Critical Review of Forecasting Net Physician Requirements in Canada. Soc. Sci. Med. 1985, 20, 411–424. [Google Scholar]
- Joyce, C.M.; McNeil, J.J.; Stoelwinder, J.U. Time for a New Approach to Medical Workforce Planning. Med. J. Aust. 2004, 180, 343–346. [Google Scholar] [CrossRef]
- Duckett, S.J. Health Workforce Design for the 21st Century. Aust. Health Rev. 2005, 29, 201–210. [Google Scholar]
- Asamani, J.A.; Christmals, C.D.; Reitsma, G.M. Advancing the Population Needs-Based Health Workforce Planning Methodology: A Simulation Tool for Country Application. Int. J. Environ. Res. Public Health 2021, 18, 2113. [Google Scholar] [CrossRef]
- Manzi, S.; Chalk, D.; Day, J.; Pearson, M.; Lang, I.; Stein, K.; Pitt, M. A Novel Modelling and Simulation Capacity Development Initiative for the National Health Service. BMJ Simul. Technol. Enhanc. Learn. 2018, 4, 97. [Google Scholar]
- Tomblin Murphy, G.; MacKenzie, A.; Guy-Walker, J.; Walker, C. Needs-Based Human Resources for Health Planning in Jamaica: Using Simulation Modelling to Inform Policy Options for Pharmacists in the Public Sector. Hum. Resour. Health 2014, 12, 67. [Google Scholar] [CrossRef] [PubMed]
- US Department of Health and Human Services. Supply and Demand Projections of the Nursing Workforce: 2014–2030; Health Resources and Services Administration: Rockville, MD, USA, 2017.
- Dreesch, N.; Dolea, C.; Dal Poz, M.R.; Goubarev, A.; Adams, O.; Aregawi, M.; Bergstrom, K.; Fogstad, H.; Sheratt, D.; Linkins, J. An Approach to Estimating Human Resource Requirements to Achieve the Millennium Development Goals. Health Policy Plan. 2005, 20, 267–276. [Google Scholar] [PubMed]
- International Labour Organization. Securing Decent Work for Nursing Personnel and Domestic Workers, Key Actors in the Care Economy. In Proceedings of the International Labour Conference, 110th Session, Geneva, Switzerland, 9 June 2022; p. 76. [Google Scholar]
- Jones, R.; Bhanbhro, S.M.; Grant, R.; Hood, R. The Definition and Deployment of Differential Core Professional Competencies and Characteristics in Multiprofessional Health and Social Care Teams. Health Soc. Care Community 2013, 21, 47–58. [Google Scholar]
- Klaasen, K.; Bowman, S.; Komenda, P. Advancing Interprofessional Collaborative Teams in the Winnipeg Health Region. Healthc. Q. 2016, 19, 65–69. [Google Scholar] [CrossRef]
- Curson, J.A.; Dell, M.E.; Wilson, R.A.; Bosworth, D.L.; Baldauf, B. Who Does Workforce Planning Well? Workforce Review Team Rapid Review Summary. Int. J. Health Care Qual. Assur. 2010, 23, 110–119. [Google Scholar] [CrossRef] [PubMed]
- Masnick, K.; McDonnell, G. A Model Linking Clinical Workforce Skill Mix Planning to Health and Health Care Dynamics. Hum. Resour. Health 2010, 8, 11. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Refs. | Author/s and Publication Year | Country | Study Design a | Type of Data b | Profession Group/s c | Methods/ Tools/Procedures Applied | Organizations/Stakeholders Involved in the Process of the Measurement of HWF Shortages |
|---|---|---|---|---|---|---|---|
| [26] | Van Greuningen et al., 2012 | The Netherlands | CS | N/CS | MD | Estimation; Projection | NIVEL; Advisory Committee on Medical Manpower Planning |
| [27] | Pandit et al., 2010 | UK | CS | CS | MD | Estimation; Prediction | NHS; workers at the Nuffield Department of Anaesthetics |
| [28] | Maier & Afentakis 2013 | Germany | CS | N | N | Projection | Federal Institute for Vocational Education and Training (BIBB), The Research Institute of the Federal Employment Agency (IAB) |
| [29] | Tsiouli et al., 2016 | Greece | CS | N | D | Prediction | Greek Association for Orthodontic Study and Research |
| [30] | Lovkyte et al., 2003 | Lithuania | CS | N | MD | Survey; Others | Lithuanian Health Information Centre |
| [31] | Stierli et al., 2021 | Switzerland | CS | R | MD | Survey; Estimation | Swiss Health Observatory (Obsan) |
| [32] | Barber & López-Valcárcel 2010 | Spain | CS | N | MD | Simulation Model | Ministry of Health |
| [33] | Grech et al., 2012 | Malta | LT | N | N | Estimation | Nurse Officers from the Maltese Neonatal Paediatric Intensive Care Unit |
| [34] | Papp et al., 2019 | Hungary | LT | N | MD | Survey; Others | National Public Health Institute, National Institute of Health Insurance Fund Management, Public Health Administration Service of Government Office of Capital City Budapest, MTA-DE Public Health Research Group of the Hungarian Academy of Sciences |
| [35] | Liu et al., 2017 | Multicountry—165 countries | CS | M | MD; N; O | Projection | World Bank; World Health Organization; members of the Global Health Workforce Alliance |
| [36] | Scheffler et al., 2008 | Multicountry—158 countries | CS | M | MD | Projection | World Health Organization |
| [37] | Scheffler et al., 2018 | Multicountry | CS | M | MD; N | Estimation; Projection | World Health Organization, OECD, World Bank |
| [38] | Taylor et al., 2018 | UK | LT | N | MD | Simulation Model; Others | General Medical Council’s |
| [39] | Lodi et al., 2015 | Italy | CS | R | MD | Projection; Simulation Model | Department of Electrical Energy and Information Engineering University of Bologna, Bologna, Italy; Regional Health and Social Agency of Emilia-Romagna, Bologna, Italy; Statistical service and geographical information of the Region Emilia-Romagna, Bologna, Italy |
| [40] | Gialama et al., 2019 | Greece | CS | N | N | Estimation; Others | Department of Social and Educational Policy, University of Peloponnese, Corinth; Department of Nursing, University of Peloponnese, Sparti; Department of Economics, University of Piraeus, Athens; Department of Public Administration, Panteion University, Athens; |
| [41] | Van Greuningen et al., 2016 | The Netherlands | CS | N | D; O | Projection; Others | NIVEL, Dutch Advisory Committee on Medical Manpower Planning |
| [42] | Gallagher et al., 2010 | UK | CS | N | D; O | Projection; Simulation Model | College and St Thomas’ Hospitals, Oral Health Services Research & Dental Public Health London; University of Southampton, Department of Mathematics Operational Research group, Southampton; Cardiff University, WIMCS Operational Research, School of Mathematics, Cardiff |
| [43] | Starkiene et al., 2005 | Lithuania | LT | N | MD | Projection; Simulation Model | Department of Preventive Medicine, Kaunas University of Medicine, Kaunas, Lithuania; Program in Health Services Administration, Xavier University, Ohio, USA |
| [44] | Ravindran et al., 2021 | UK | CS | N | MD; N; O | Survey; Projection | Joint Advisory Group on Gastrointestinal Endoscopy (JAG); the British Society of Gastroenterology (BSG); Association of Coloproctology of Great Britain and Ireland (ACPGBI) |
| [45] | Teljeur et al., 2010 | UK | CS | N | MD | Projection, Simulation Model | Department of Public Health and Primary Care, Trinity College Centre for Health Sciences |
| [46] | Harkin et al., 2016 | UK | CS | N | MD | Prediction | Researchers from the Vascular Surgery United Kingdom Workforce Survey (VSUKWS); National Health Service (NHS); |
| [47] | Hegarty et al., 2022 | UK | CS | N | N | Estimation | National Institute for Health Research, Society of Acute Medicine |
| [48] | Maresova et al., 2020 | Czech Republic | CS | N and R | N | Projection; Others | Healthcare Holding of the Hradec Kralove Region; the Hradec Kralove University Hospital; Hradec Kralove Labour Office |
| [49] | Tsai et al., 2012 | Multicountry—130 countries | CS | M | MD | Prediction; Others | The Health Department in Taiwan |
| [50] | Boniol et al., 2022 | Multicountry | CS | M | MD; N; P; D | Projection | Health Workforce department, World Health Organization |
| Method/Tool/Model. | Definition |
|---|---|
| Projection | A tool used to better understand future situations and changes (the dynamics of workforce supply and demand) based on a study of current trends and conditions. |
| Estimation | This process uses data to guess the parameter about the true state of nature. |
| Prediction | Expectation; this process uses data to guess a random value (variable) that is not part of the dataset. |
| Simulation model | The process of creating and analyzing a digital prototype of a physical model to predict its performance and various scenarios in the real world. |
| Survey | The collection of information from a sample of individuals via their responses to questions. |
| Other methods | |
| Delphi study | A process of consultations; aims to collect opinions from a group of experts. |
| Workload of Indicators Staffing Need (WISN) method | A method based on a health worker’s workload, with activity (time) standards applied to each workload component; it is able to calculate the optimal allocation and distribution of staff geographically and functionally between different types of health facilities or health services in a country as a whole. |
| An area-based composite indicator | A tool built from different indicators; enables the assessment of socioeconomic status (SES) and then allows preparing a comparison between the distribution of unfilled practices and SES. |
| Interview | A qualitative research method; relies on asking questions in order to collect data. |
| Multiple stepwise-linear regression | Selection of independent variables to use in a model based on an iterative process of adding or removing variables. |
| Multiple imputations | A general approach to the problem of missing data that is available in several commonly used statistical packages, which allows repeated imputations to assess the variability of estimated values. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parzonka, K.; Ndayishimiye, C.; Domagała, A. Methods and Tools Used to Estimate the Shortages of Medical Staff in European Countries—Scoping Review. Int. J. Environ. Res. Public Health 2023, 20, 2945. https://doi.org/10.3390/ijerph20042945
Parzonka K, Ndayishimiye C, Domagała A. Methods and Tools Used to Estimate the Shortages of Medical Staff in European Countries—Scoping Review. International Journal of Environmental Research and Public Health. 2023; 20(4):2945. https://doi.org/10.3390/ijerph20042945
Chicago/Turabian StyleParzonka, Kamila, Costase Ndayishimiye, and Alicja Domagała. 2023. "Methods and Tools Used to Estimate the Shortages of Medical Staff in European Countries—Scoping Review" International Journal of Environmental Research and Public Health 20, no. 4: 2945. https://doi.org/10.3390/ijerph20042945
APA StyleParzonka, K., Ndayishimiye, C., & Domagała, A. (2023). Methods and Tools Used to Estimate the Shortages of Medical Staff in European Countries—Scoping Review. International Journal of Environmental Research and Public Health, 20(4), 2945. https://doi.org/10.3390/ijerph20042945