
The Primary Nursing Care Model and Inpatients’ Nursing-Sensitive Outcomes: A Systematic Review and Narrative Synthesis of Quantitative Studies

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Process
2.3. Data Extraction
2.4. Outcomes
2.5. Quality Assessment of Studies
2.6. Data Synthesis and Analysis
3. Results
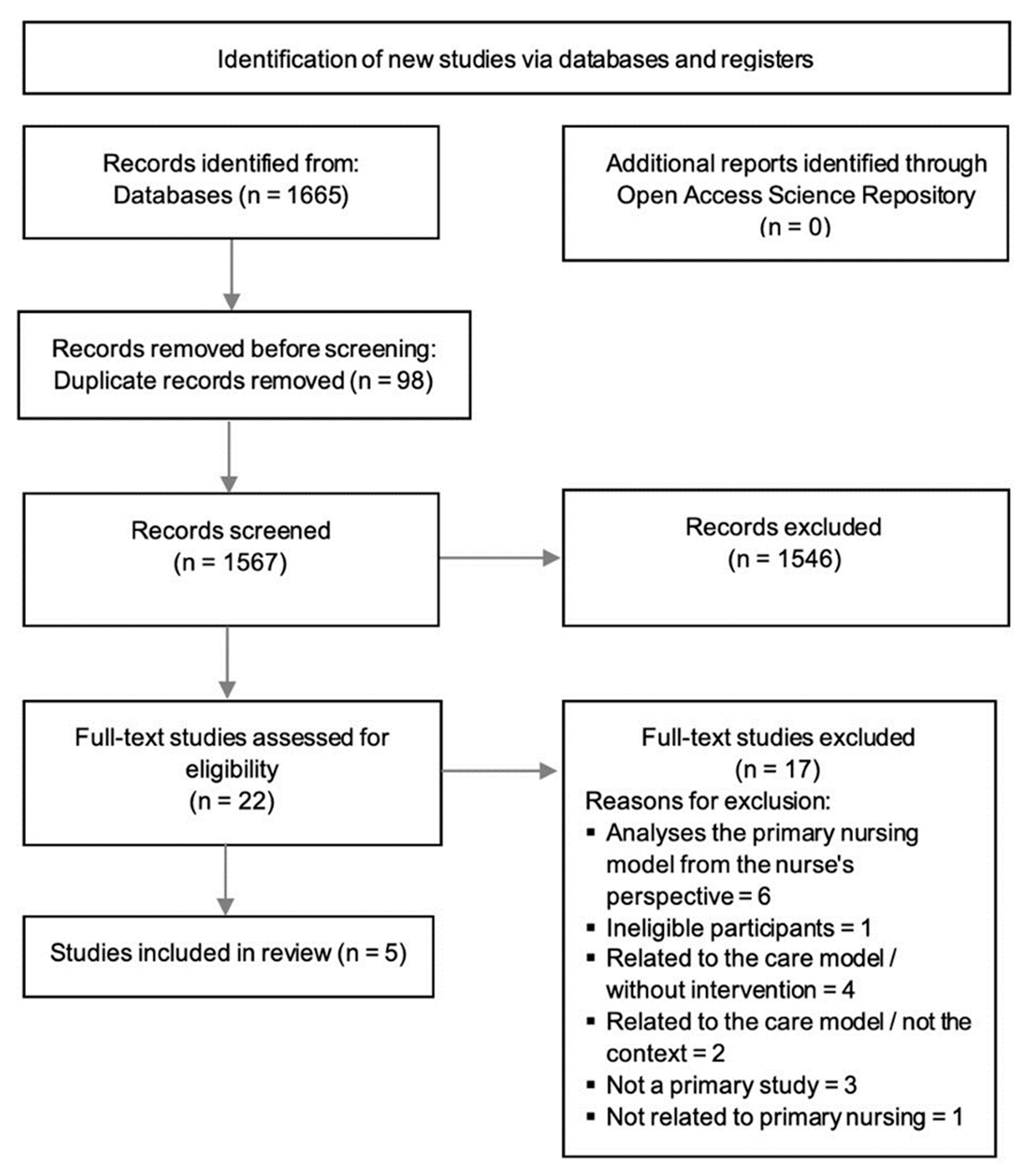
3.1. Study Selection
3.2. Study Characteristics
3.3. Quality Assessment of Studies
3.4. The Use of the Primary Nursing Care Model in Inpatients’ Outcomes
3.5. Primary Nursing Care Model and Inpatients’ Nursing-Sensitive Outcomes
3.6. Primary Nursing Care Model and Inpatients’ Experience
3.7. Other Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Database- | Search Strategy |
|---|---|
| Web of Science Core Collection Date of search: June 2021 and updated in October 2022 | # 1 ALL = chronic disease; # 2 ALL = chronic illness; # 3 ALL = long term conditions; # 4 ALL = chronic conditions; # 5 ALL = Inpatients; # 6 ALL = Acute care; # 7 ALL = wards; # 8 #7 OR #6 OR #5 OR #4 OR #3 OR #2 OR #1; # 9 ALL = primary nursing; # 10 ALL = primary nursing model of care; # 11 ALL = primary nursing care model; # 12 #11 OR #10 OR #9; # 13 ALL = patient outcomes; # 14 ALL = nursing sensitive outcomes; # 15 ALL = patient satisfaction; # 16 ALL = patient experience; # 17 ALL = medication errors in nursing; # 18 ALL = falls in hospitalized patients; # 19 ALL = pressure ulcers in hospital; # 20 ALL = urinary tract infections catheter-related; # 21 ALL = Patient-selfcare; # 22 ALL = Patient self management; # 23 ALL = patient safety; # 24 ALL = symptom management; # 25 ALL = discharge planning; # 26 #25 OR #24 OR #23 OR #22 OR #21 OR #20 OR #19 OR #18 OR #17 OR #16 OR #15 OR #14 OR #13; # 27 #26 AND #12 AND #8 Refined by: WEB OF SCIENCE CATEGORIES: (NURSING) AND LANGUAGES: (ENGLISH OR SPANISH OR PORTUGUESE) AND DOCUMENT TYPES: (ARTICLE). (Results = 1188) |
| CINAHL (EBSCO host platform) Date of search: June 2021 and updated in October 2022 | S1 (MH “Chronic Disease”) S2 chronic disease or chronic illness or long term conditions or chronic conditions S3 (MH “Inpatients”) S4 inpatients or hospitalization or ‘hospitalized patients’ or acute or ward or hospital or unit S5 S1 OR S2 OR S3 OR S4 S6 “primary nursing” S7 “primary nursing care model” S8 “primary nursing model” S9 “primary nursing care” S10 “primary nursing care delivery mode” S11 S6 OR S7 OR S8 OR S9 OR S10 S12 patient outcomes or quality of care or health outcomes or patient satisfaction or patient experience S13 “nursing sensitive outcomes” S14 S12 OR S13 S15 S5 AND S11 AND S14 S16 (MH “Medication Errors”) S17 “medication errors in nursing” S18 (MH “Accidental Falls”) S19 “falls in hospitals” S20 (MH “Pressure Ulcer”) S21 “pressure ulcers in hospitals” S22 “urinary tract infections, catheter-related” S23 (MH “Urinary Tract Infections, Catheter-Related”) S24 patient self-care or self management S25 (MH “Patient Safety”) S26 patient safety or patient outcomes or quality of care or safety S27 symptom management or symptom control S28 (MH “Discharge Planning”) S29 discharge planning or discharge process S30 S16 OR S17 OR S18 OR S19 OR S20 OR S21 OR S22 OR S23 OR S24 OR S25 OR S26 OR S27 OR S28 OR S29 S31 S15 AND S30 S32 S15 AND S30 Limiters—Publication Date 2000 01 01–2022 12 31; Age Groups: All Adult; Languages: English or Spanish or Portuguese (Results = 68) |
| MEDLINE with Full Text (EBSCOhost platform) Date of search: June 2021 and updated in October 2022 | S1 (MH “Chronic Disease”) S2 chronic disease or chronic illness or long term conditions or chronic conditions S3 (MH “Inpatients”) S4 inpatients or hospitalization or ‘hospitalized patients’ or acute or ward or hospital or unit S5 S1 OR S2 OR S3 OR S4 S6 primary nursing S7 primary nursing care model S8 primary nursing care delivery model S9 primary nursing model S10 S6 OR S7 OR S8 OR S9 S11 (MH “Patient Outcome Assessment”) S12 patient outcomes or quality of care or health outcomes or patient satisfaction or patient experience S13 “nursing sensitive outcomes” S14 (MH “Medication Errors”) S15 “medication errors in nursing” S16 (MH “Accidental Falls”) S17 “falls in hospitalized patients” S18 (MH “Pressure Ulcer”) S19 “pressure ulcers in hospitals” S20 (MH “Urinary Tract Infections”) S21 “urinary tract infections, catheter-related” S22 Patient- selfcare or self management S23 (MH “Patient Safety”) S24 patient safety S25 symptom management or symptom control S26 discharge planning or discharge process or discharge management S27 S13 OR S14 OR S15 OR S16 OR S17 OR S18 OR S19 OR S20 OR S21 OR S22 OR S23 OR S24 OR S25 OR S26 S28 S5 AND S10 AND S27 Limiters—Publication Date 2000 01 01–2022 12 31; Age Groups: All Adult; Languages: English or Spanish or Portuguese (Results = 110) |
| Nursing & Allied Health Collection (EBSCOhost platform) Date of search: June 2021 and updated in October 2022 | S1 chronic disease or chronic illness or long term conditions or chronic conditions S2 inpatients or hospitalization or ‘hospitalized patients’ or acute or ward or hospital or unit S3 S1 OR S2 S4 primary nursing S5 primary nursing care model S6 primary nursing care delivery model S7 primary nursing model S8 S4 OR S5 OR S6 OR S7 S9 patient outcomes or quality of care or health outcomes or patient satisfaction or patient experience S10 nursing sensitive outcomes S11 medication errors in nursing S12 falls in hospitalized patients S13 pressure ulcers in hospitals S14 urinary tract infections, catheter-related S15 Patient-selfcare or self management S16 patient safety S17 symptom management or symptom control S18 discharge planning or discharge process or discharge management S19 S9 OR S10 OR S11 OR S12 OR S13 OR S14 OR S15 OR S16 OR S17 OR S18 S20 S3 AND S8 AND S19 S27 Limiters—Publication Date 2000 01 01–2022 12 31; Languages: English or Spanish or Portuguese (Results = 20) |
| Cochrane Central Register of Controlled Trials (EBSCOhost platform) Date of search:June 2021 and updated in October 2022 | S1 chronic disease or chronic illness or long term conditions or chronic conditions S2 inpatients or hospitalization or ‘hospitalized patients’ or acute or ward or hospital or unit S3 S1 OR S2 S4 primary nursing S5 primary nursing model S6 S4 OR S5 S7 patient outcomes or quality of care or health outcomes or patient satisfaction or patient experience S8 medication errors in nursing S9 falls in hospitalized patients S10 pressure ulcers in hospitals S11 urinary tract infections, catheter-related S12 Patient- selfcare or self management S13 patient safety S14 symptom management or symptom control S15 discharge planning or discharge process S16 S7 OR S8 OR S9 OR S10 OR S11 OR S12 OR S14 OR S15 S17 S3 AND S6 AND S16 Limiters—Publication Date 2000 01 01–2022 12 31 Languages: English or Spanish or Portuguese; (Results = 14) |
| Scielo Citation Index (Web of Scicence) Date of search: June 2021 and updated in October 2022 | # 1 TS = chronic disease; # 2 TS = chronic illness; # 3 TS = long term conditions; # 4 TS = chronic conditions; # 5 TS = Inpatients; # 6 TS = Acute care; # 7 TS = wards; # 8 #7 OR #6 OR #5 OR #4 OR #3 OR #2 OR #1; # 9 TS = primary nursing; # 10 TS = primary nursing model of care; # 11 TS = primary nursing care delivery model; # 12 #11 OR #10 OR #9; # TS = patient outcomes; # 14 TS = Nursing sensitive outcomes; # 15 TS = patient satisfaction; # 16 TS = patient experience; # 17 TS = Patient reported outcomes; # 18 TS = medication errors; # 19 TS = falls; # 20 TS = pressure ulcers; # 21 TS = urinary tract infections; # 22 TS = Patient- selfcare; # 23 TS = patient safety; # 24 TS = symptom management; # 25 TS = discharge planning; # 26 #25 OR #24 OR #23 OR #22 OR #21 OR #20 OR #19 OR #18 OR #17 OR #16 OR #15 OR #14 OR #13; # 27 #26 AND #12 AND #8; # 28 #26 AND #12 AND #8 Refined by: document types: (research article) (Results = 46) |
References
- Copanitsanou, P.; Fotos, N.; Brokalaki, H. Effects of Work Environment on Patient and Nurse Outcomes. Br. J. Nursing 2017, 26, 172–176. [Google Scholar] [CrossRef] [PubMed]
- Aiken, L.H.; Sloane, D.M.; Ball, J.; Bruyneel, L.; Rafferty, A.M.; Griffiths, P. Patient Satisfaction with Hospital Care and Nurses in England: An Observational Study. BMJ Open 2018, 8, 19189. [Google Scholar] [CrossRef] [PubMed]
- Hoffart, N.; Woods, C.Q. Elements of a Nursing Professional Practice Model. J. Prof. Nurs. 1996, 12, 354–364. [Google Scholar] [CrossRef] [PubMed]
- Slatyer, S.; Coventry, L.L.; Twigg, D.; Davis, S. Professional Practice Models for Nursing: A Review of the Literature and Synthesis of Key Components. J. Nurs. Manag. 2016, 24, 139–150. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.; Zhao, Y.; While, A. Job Satisfaction among Hospital Nurses: A Literature Review. Int. J. Nurs. Stud. 2019, 94, 21–31. [Google Scholar] [CrossRef]
- Parreira, P.; Santos-Costa, P.; Neri, M.; Marques, A.; Queirós, P.; Salgueiro-Oliveira, A. Work Methods for Nursing Care Delivery. Int. J. Environ. Res. Public Health 2021, 18, 2088. [Google Scholar] [CrossRef]
- Pontin, D. Primary Nursing: A Mode of Care or a Philosophy of Nursing? J. Adv. Nurs. 1999, 29, 584–591. [Google Scholar] [CrossRef]
- Wessel, S.L.; Manthey, M. Primary Nursing: Person-Centered Care Delivery System Design; Creative Healthcare Management: Minneapolis, MN, USA, 2015. [Google Scholar]
- Cocchieri, A.; Cesare, M.; Anderson, G.; Zega, M.; Damiani, G.; D’agostino, F. Effectiveness of the Primary Nursing Model on Nursing Documentation Accuracy: A Quasi-Experimental Study. J. Clin. Nurs. 2022, 1–11. [Google Scholar] [CrossRef]
- Cocchieri, A.; Magon, G.; Cavalletti, M.; Cristofori, E.; Zega, M. Exploring Hospital Compliance with the Primary Nursing Care Model: Validating an Inventory Using the Delphi Method. BMC Nurs. 2021, 20, 188. [Google Scholar] [CrossRef]
- Kuipers, S.J.; Cramm, J.M.; Nieboer, A.P. The Importance of Patient-Centered Care and Co-Creation of Care for Satisfaction with Care and Physical and Social Well-Being of Patients with Multi-Morbidity in the Primary Care Setting 11 Medical and Health Sciences 1117 Public Health and Health Service. BMC Health Serv. Res. 2019, 19, 13. [Google Scholar] [CrossRef]
- Mokkink, L.B.; Terwee, C.B.; Patrick, D.L.; Alonso, J.; Stratford, P.W.; Knol, D.L.; Bouter, L.M.; de Vet, H.C.W. The COSMIN Study Reached International Consensus on Taxonomy, Terminology, and Definitions of Measurement Properties for Health-Related Patient-Reported Outcomes. J. Clin. Epidemiol. 2010, 63, 737–745. [Google Scholar] [CrossRef] [PubMed]
- Blanco-López, R.M.; Fole-Santalla, M.D.; Rio-Enríquez, M.; Quiroga-Mariño, M.J.; Barcón-Pajón, M.; Casariego-Vales, E. Effectiveness of a Nursing Training Intervention in Complex Chronic Patients. Enfermería Clínica (Engl. Ed.) 2020, 30, 302–308. [Google Scholar] [CrossRef]
- Drenkard, K. The Business Case for Magnet®. J. Nurs. Adm. 2010, 40, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Oldland, E.; Botti, M.; Hutchinson, A.M.; Redley, B. A Framework of Nurses’ Responsibilities for Quality Healthcare—Exploration of Content Validity. Collegian 2019, 27, 150–163. [Google Scholar] [CrossRef]
- Dubois, C.A.; D’amour, D.; Brault, I.; Dallaire, C.; Déry, J.; Duhoux, A.; Lavoie-Tremblay, M.; Mathieu, L.; Karemere, H.; Zufferey, A. Which Priority Indicators to Use to Evaluate Nursing Care Performance? A Discussion Paper. J. Adv. Nurs. 2017, 73, 3154–3167. [Google Scholar] [CrossRef] [PubMed]
- Dubois, C.A.; D’Amour, D.; Pomey, M.P.; Girard, F.; Brault, I. Conceptualizing Performance of Nursing Care as a Prerequisite for Better Measurement: A Systematic and Interpretive Review. BMC Nurs. 2013, 12, 7. [Google Scholar] [CrossRef]
- Mattila, E.; Pitkänen, A.; Alanen, S.; Leino, K.; Luojus, K.; Rantanen, A.; Aalto, P. The Effects of the Primary Nursing Care Model: A Systematic Review. J. Nurs. Care 2014, 3, 6. [Google Scholar] [CrossRef]
- Butler, M.; Schultz, T.J.; Halligan, P.; Sheridan, A.; Kinsman, L.; Rotter, T.; Beaumier, J.; Kelly, R.G.; Drennan, J. Hospital Nurse-Staffing Models and Patient-and Staff-Related Outcomes (Review). Cochrane Database Syst. Rev. 2019. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Irvine, D.; Sidani, S.; Hall, L.M. Linking Outcomes to Nurses’ Roles in Health Care. Nurs. Econ. 1998, 16, 58–64. [Google Scholar]
- Doran, D. (Ed.) Nursing Outcomes The State of the Science, 2nd ed.; Jones & Bartlett Learning: Guelph, ON, Canada, 2011. [Google Scholar]
- Tuinman, A.; de Greef, M.H.G.; Finnema, E.J.; Roodbol, P.F. A Systematic Review of the Association between Nursing Staff and Nursing-Sensitive Outcomes in Long-Term Institutional Care. J. Adv. Nurs. 2021, 77, 3303–3316. [Google Scholar] [CrossRef] [PubMed]
- Oner, B.; Zengul, F.D.; Oner, N.; Ivankova, N.V.; Karadag, A.; Patrician, P.A. Nursing-Sensitive Indicators for Nursing Care: A Systematic Review (1997–2017). Nurs. Open 2021, 8, 1005–1022. [Google Scholar] [CrossRef] [PubMed]
- Armijo-Olivo, S.; Stiles, C.R.; Hagen, N.A.; Biondo, P.D.; Cummings, G.G. Assessment of Study Quality for Systematic Reviews: A Comparison of the Cochrane Collaboration Risk of Bias Tool and the Effective Public Health Practice Project Quality Assessment Tool: Methodological Research. J. Eval. Clin. Pract. 2012, 18, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Thomas, B.H.; Ciliska, D.; Dobbins, M.; Micucci, S. A Process for Systematically Reviewing the Literature: Providing the Research Evidence for Public Health Nursing Interventions. Worldviews Evid. Based Nurs. 2004, 1, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Deeks, J.J.; Higgins, J.P.; Altman, D.G. Cochrane Statistical Methods Group. Analysing Data and Undertaking Meta-Analyses. Cochrane Handb. Syst. Rev. Interv. 2019, 241–284. [Google Scholar]
- Grant, M.J.; Booth, A. A Typology of Reviews: An Analysis of 14 Review Types and Associated Methodologies. Health Inf. Libr. J. 2009, 26, 91–108. [Google Scholar] [CrossRef]
- Dal Molin, A.; Gatta, C.; Boggio Gilot, C.; Ferrua, R.; Cena, T.; Manthey, M.; Croso, A. The Impact of Primary Nursing Care Pattern: Results from a before–after Study. J. Clin. Nurs. 2018, 27, 1094–1102. [Google Scholar] [CrossRef]
- Naef, R.; Ernst, J.; Petry, H. Adaption, Benefit and Quality of Care Associated with Primary Nursing in an Acute Inpatient Setting: A Cross-Sectional Descriptive Study. J. Adv. Nurs. 2019, 75, 2133–2143. [Google Scholar] [CrossRef]
- Moura, E.C.C.; Lima, M.B.; Peres, A.M.; Lopez, V.; Batista, M.E.M.; das Braga, F.C.S.A.G. Relationship between the Implementation of Primary Nursing Model and the Reduction of Missed Nursing Care. J. Nurs. Manag. 2020, 28, 2103–2112. [Google Scholar] [CrossRef]
- Tonkikh, O.; Zisberg, A.; Shadmi, E. Association between Continuity of Nursing Care and Older Adults’ Hospitalization Outcomes: A Retrospective Observational Study. J. Nurs. Manag. 2020, 28, 1062–1069. [Google Scholar] [CrossRef]
- Chen, Q.; Gottlieb, L.; Liu, D.; Tang, S.; Bai, Y. The Nurse Outcomes and Patient Outcomes Following the High-Quality Care Project. Int. Nurs. Rev. 2020, 67, 362–371. [Google Scholar] [CrossRef] [PubMed]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159. [Google Scholar] [CrossRef] [PubMed]
- Recio-Saucedo, A.; Dall’Ora, C.; Maruotti, A.; Ball, J.; Briggs, J.; Meredith, P.; Redfern, O.C.; Kovacs, C.; Prytherch, D.; Smith, G.B.; et al. What Impact Does Nursing Care Left Undone Have on Patient Outcomes? Review of the Literature. J. Clin. Nurs. 2018, 27, 2248–2259. [Google Scholar] [CrossRef] [PubMed]
- Otter, C.E.M.; Hoogerduijn, J.G.; Keers, J.C.; Hagedoorn, E.I.; de Man-van Ginkel, J.M.; Schuurmans, M.J. Older Patients’ Motives of Whether or Not to Perform Self-Management during a Hospital Stay and Influencing Factors ✰. Geriatr. Nurs. 2019, 40, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Kalánková, D.; Kirwan, M.; Bartoníčková, D.; Cubelo, F.; Žiaková, K.; Kurucová, R. Missed, Rationed or Unfinished Nursing Care: A Scoping Review of Patient Outcomes. J. Nurs. Manag. 2020, 28, 1783–1797. [Google Scholar] [CrossRef]
- Assaye, A.M.; Wiechula, R.; Schultz, T.J.; Feo, R. Missed Nursing Care, Nurse Staffing Levels, and Patient Safety Outcomes in Low-Income Country Acute Care Settings: An Observational Study. Int. J. Nurs. Pract. 2021, 28, e13031. [Google Scholar] [CrossRef]
- Andersson, Å.; Frank, C.; Willman, A.M.L.; Sandman, P.O.; Hansebo, G. Factors Contributing to Serious Adverse Events in Nursing Homes. J. Clin. Nurs. 2018, 27, e354–e362. [Google Scholar] [CrossRef]
- Desborough, J.; Bagheri, N.; Banfield, M.; Mills, J.; Phillips, C.; Korda, R. The Impact of General Practice Nursing Care on Patient Satisfaction and Enablement in Australia: A Mixed Methods Study. Int. J. Nurs. Stud. 2016, 64, 108–119. [Google Scholar] [CrossRef]
- Sugg, H.V.R.; Russell, A.M.; Morgan, L.M.; Iles-Smith, H.; Richards, D.A.; Morley, N.; Burnett, S.; Cockcroft, E.J.; Thompson Coon, J.; Cruickshank, S.; et al. Fundamental Nursing Care in Patients with the SARS-CoV-2 Virus: Results from the ‘COVID-NURSE’ Mixed Methods Survey into Nurses’ Experiences of Missed Care and Barriers to Care. BMC Nurs. 2021, 20, 215. [Google Scholar] [CrossRef]
- Topaz, M.; Lisby, M.; Morrison, C.R.C.; Levtzion-Korach, O.; Hockey, P.M.; Salzberg, C.A.; Efrati, N.; Lipsitz, S.; Bates, D.W.; Rozenblum, R. Nurses’ Perspectives on Patient Satisfaction and Expectations: An International Cross-Sectional Multicenter Study With Implications for Evidence-Based Practice. Worldviews Evid. Based Nurs. 2016, 13, 185–196. [Google Scholar] [CrossRef]
- Swiger, P.A.; Loan, L.A.; Raju, D.; Breckenridge-Sproat, S.T.; Miltner, R.S.; Patrician, P.A. Relationships between Army Nursing Practice Environments and Patient Outcomes. Res. Nurs. Health 2018, 41, 131–144. [Google Scholar] [CrossRef] [PubMed]
- Aranburu-Imatz, A.; de la López-Carrasco, J.C.; Moreno-Luque, A.; Jiménez-Pastor, J.M.; del Valverde-León, M.R.; Rodríguez-Cortés, F.J.; Arévalo-Buitrago, P.; López-Soto, P.J.; Morales-Cané, I. Nurse-Led Interventions in Chronic Obstructive Pulmonary Disease Patients: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 9101. [Google Scholar] [CrossRef] [PubMed]

| Title/Author(s)/Publication Year | Research Design | Settings and Participants (Sample and Characteristics) | Outcome Measurement | Main Findings |
|---|---|---|---|---|
| “The impact of Primary Nursing care pattern: results from a before–after study.” (Dal Molin et al., 2018) [29] | Quasi-experimental (before–after study). | 400-bed community hospital, Italy. t0 (before PN) = from May to November 2013); t1 (after PN) = from December 2013 to May 2014); 2857 inpatients (t0) before PN. Average age 70.4 years 3169 inpatients (t1) after PN. Average age 68 years. Adults more than 18 years old in units where PN was implemented. 369 nurses working in units where PN was implemented and that attended to the specific training sessions (82.4% female). | Patients’ outcomes: (1) Data collection tool to measure the effect of PN in patient-related outcomes: pressure ulcer; patient fall; urinary tract infection; venous catheter-related infection. (2) Newcastle Satisfaction with Nursing Scales: to measure patient satisfaction with care, the reliability of the Italian version (Cronbach’s alpha = 0.94) Nurses’ outcomes: (3) Nursing Competence Scale: 73 items and includes 7 groups of competencies (helping role, teaching-coaching, diagnostic functions, managing situations, therapeutic interventions, ensuring quality and word role); this scale exhibited good reliability (Cronbach’s alpha from 0.79 to 0.91); (4) Diagnostic Thinking Inventory: 41 items, this instrument evaluates flexibility in thinking (21 items) and the structure of memory (20 items); the overall reliability was 0.84 for internal consistency, 0.73 for flexibility and 0.75 for structure items. For the organization: (5) Empowering Leadership Questionnaire: was used to analyze head nurse leadership in 5 factors (learning by example, participative decision-making, coaching, informing and showing concern/interacting with the team); (6) Team Climate Inventory: 38 items that evaluate 4 factors (participate safety, support to innovation, vision of group and task orientation). | • The incidence of adverse events such as pressure ulcer (t0 = 136 to t1 = 126), patient falls (t0 = 67 to t1 = 59), urinary tract infections (t0 = 153 to t1 = 133) and venous catheter infection (peripheral t0 = 61 to t1 = 30, central t0 = 12 in 215 to t1 = 3 in 295) decreased after the implementation of PN. • The nurses reported an increase in their competencies such as: helping role (t0 = 18.11 and t1 = 19.85, p = 0.0001); diagnostic functions (t0 = 18.88 and t1 = 20.11, p = 0.0007); managing situations (t0 = 27.60 and t1 = 28.60, p = 0.0210); ensuring quality (t0 = 16.03 and t1 = 16.93, p = 0.0057); teaching-coaching the patient (t0 = 14.60 and t1 = 15.55, p = 0.0002); teaching-coaching the family (t0 = 5.60 to t1 = 5.98, p = 0.0015); teaching-coaching the student (t0 = 4.72 to t1 = 5.14, p = 0335); teaching-coaching evaluation of the education program (t0 = 8.29 and t1 = 8.90, p = 0.0004). • With the application of Diagnostic Thinking Inventory, the results were an increase of thinking flexibility (from 92.39 to 96.34, p < 0.00001) and structure of memory (from 86.49 to 92.16, p < 0.00001). |
| “Adaption, benefit and quality of care associated with primary nursing in an acute inpatient setting: A cross-sectional descriptive study” (Naef et al., 2019) [30] | Descriptive cross-sectional study. | 900-bed University hospital In Switzerland, 2017 study. Acute care inpatients. N = 369 inpatients Median age = 59 years Female = 52.0% Median hospital stay = 6 days N = 381 nurses N = 360 registered nurses N = 13 practical nurses (Swiss certification) N = 8 nurse assistants Female = 48.2% Full-time work = 246 Registered nurses = 60.8% Bachelor’s degree/Master of Advanced Studies = 33.6% Postgraduate degree = 5.6% Worked as primary nurses = 87.8% registered nurses | (1) Primary Nursing Scale (PNS)—a nine-item questionnaire (nurses’ perception of the extent to which primary nursing was adopted and was beneficial in ensuring coordinated, person-centered care in an acute care setting). A Likert scale 1–6, was used and high scores indicated high level of primary nursing adoption and benefit; (2) A structured extraction sheet to uptake primary nursing in the patient care process, as evidenced in the patient record, with four indicators dichotomized (yes, no): (a) a primary nurse had been assigned to the patient; (b) nursing admission assessment and care planning had been completed within 48 h by the primary nurse; (c) follow-up assessment and care planning had been conducted at least once a week by the primary nurse; (d) discharge planning had been initiated by the primary nurse; (3) The Oncology Patients’ Perceptions of Quality of Nursing Care Scale (OPPQNCS). The 18-item OPPQNCS measures patients’ perceptions of the quality of nursing care in four types of person-centered nursing interventions: responsiveness; individualization, coordination, and proficiency (Likert scale 1–6 was used, high scores indicate higher quality of person-centered care). | • 96.5% of patients reported high overall quality of nursing care (median score of 5.4), the attributes of patient centered nursing interventions responsiveness, proficiency and individuality of care scored high (>90.0%). The attribute coordination of care was perceived to be lower (median = 4.7); • 72.1% of patients had a primary nurse assigned to them; • 81.1% of cases had admission assessments and care planning completed within 48 h; • In 26.1% of cases, the assigned primary nurse fully completed the admission assessment and care planning; • 86.5% of patients had discharge planning activities documented in the records; • In 50.5% of patients with a stay of 7 days or longer weekly follow-up assessments and care planning by a designated primary nurse occurred; • 63.3% of nurses agreed or strongly agreed that primary nursing was adopted on their unit; • 80.5% of nurses agreed or strongly agreed that primary nursing is beneficial for the delivery of person centered care; • Nurses’ demographic and professional characteristics did not influence nurses’ perceptions of the extent of adoption or benefit of primary nursing; • There was a statistically significant positive correlation between adoption and benefits scores (Spearman’s correlation: rs 0.449, p < 0.000). |
| “Relationship between the implementation of primary nursing model and the reduction of missed nursing care.” (Moura et al., 2020) [31] | Predictive correlational study. | University Hospital in the northeast region of Brazil, 201 beds. Four inpatient units. 4 and 7 months following the implementation of primary nursing model Final sample 96 participants (37 nurses and 57 nursing technicians). Average age of 34.9 years and 88.5% female. 40.6% had nursing specialties. 96.9% worked full time in the unit. 58.3% worked 6-h shifts, 36 h per week. Average years of experience = 8.3. Average years of experience in this unit = 1.8. 94.8% did not intend to leave their role at the unit. | MISSCARE instrument: the 56-item consisted in two parts: (A) missed care with 28-items and (B) reasons, also with 28-items. The responses had a 5-point Likert-type scale. The B part was distributed in 5 dimensions: communication (10-items), material resources (4-items), labor resources (8-items), ethical dimension (3-itemsn) and management/leadership style (3-items). | • Missed nursing care was reduced 78.5% with primary nursing. • In the fourth month of implementation of MISSCARE, 6 items obtained high levels (>40%), such as: Item 1—Ambulation three times per day or as ordered, Item 2—Turning patient every 2-h, Item 4—Setting up meals for patients who feed themselves, Item 19—Response to call light is initiated within 5 min., Item 22—Attend interdisciplinary care conferences whenever held and Item 27—Sitting the patient off the bed. Main reasons for missed care found in this study: labor resources (89.6%) and communication dimension (77.1%). |
| “The nurse outcomes and patient outcomes following the High-Quality Care Project” (Chen et al., 2020) [33] “Association between continuity of nursing care and older adults’ hospitalization outcomes: A retrospective observational study” (Tonkikh et al., 2020) [32] | Analytical cross-sectional study. Two studies on the High-Quality Care Project that implemented primary nursing: before (2009) and after (2016). | 40 units of 10 tertiary hospitals in China 2006 study: 354 patients Male = 56.8% Mean age = 54.4 years Median hospital stay = 6 days 580 nurses Female = 98.8% Non-permanent employment contracts = 65.3% Advanced diploma = 56.2% Baccalaureate = 38.4% Master or above = 0.7% 2016 study: 550 patients Male = 59.1% Mean age = 56 years Median hospital stay = 5 days 796 nurses Female = 94.3% Non-permanent employment contracts = 73.8% Advanced diploma = 25.4% Baccalaureate = 72.0% Master or above = 2.4% | Nurse outcomes: (1) Nurse Work Index—Practice: Environment Scale (NWI-PES)—31 items divided into five subscales. A 4-point Likert scale where a higher score means a better nurse work environment; (2) Maslach Burnout Inventory (MBI)—22 items divided into three subscales. A 6-point Likert scale, a score on the Emotional Exhaustion subscale ≥27 indicate a high level of burnout; (3) An overall job satisfaction item and eight individual items of different aspects of job satisfaction (each item was scored from 0 “Very dissatisfied” to 3 “Very satisfied”); intention to leave job (measured with a dichotomous item (yes, no)). Patient outcomes: (4) Quality of patient care through an item in the nurses’ questionnaire (rating from 0 “poor” to 3 “excellent”) and patient safety by asking nurses to estimate the frequency of nursing-sensitive events, namely medication administration errors, pressure ulcers, falls, urinary tract infections and venous catheter-related infections (the rating ranged from 0 to 30, the higher the rating the higher the frequency of adverse events); (5) Consumer Assessment of Healthcare Providers and Systems (CAHPS). Scores 0 to 10 given by the patient. The scores 8 and 10 are the best rating. | • The length of patient stay in 2016 was shorter than in 2009; • The rating quality of patient care ‘excellent’ had increased by 1.718 times in 2016 compared with 2009, OR= 1.718 (p = 0.005), controlling the covariates on the nurse level (nurses’ characteristics); • Nurses in 2016 reported fewer patient adverse events then 2009 β = −0.894 (p < 0.001), controlling the covariates on the nurse level (nurses’ characteristics); • For patients, the rating of hospital in 2016 with a score of “9” or “10”, had increased compared with patients in 2009. OR= 1.705 (p = 0.01), controlling the covariate on the patient level (length of hospital stay). |
| Retrospective observational study. | Two tertiary hospitals (internal medicine units) in Israel between 2009 and 2011 609 patients aged ≥ 70 years Mean age = 79 years Median hospital stay = 5.7 days 37.8% experienced cognitive decline 22.3% experienced physical functioning decline between admission and discharge 40.6%) reported high satisfaction with the hospital care experience. | (1) 10-item Short Portable Mental Status Questionnaire (SPMSQ), score 0 to 10 with higher scores indicating better cognitive status; (2) 11-item modified Barthel index, total score ranges from 0 to 100 (decline in physical functioning was defined as at least a 2-point decline on the modified Barthel index from the at-admission to at-discharge assessments); (3) Modified version of the Perceived Hospital Environment Quality Index at discharge with 12 of the original items, 5-point Likert-type scale, score 1 “totally disagree” to 5 “totally agree” (average score of 4 or above was considered high satisfaction); (4) Continuity of Care Index (CoC) and Sequential Continuity Index (SECON) to measure continuity in the assignment of nurses to patients: the continuity score was dichotomized into higher and lower than 75.0% and the cut-off was 25.0% (two-thirds of the sample fall within the 25.0% of the highest feasible continuity score). | • On average, patients met the same nurse 1.5 times during hospitalization. • On average, seven different nurses were assigned to care for each patient during the hospitalization; • Mean for continuity score was low for both CoC (0.09) and SECON (0.24); • 21.0% of patients hospitalized for 2 to 7 days were not assigned to the same nurse on any of the consecutive days (SECON = 0); • 81.6% of those patients were assigned to a new nurse each morning and evening shift (CoC = 0); • 31.5% achieved 25.0% of the highest feasible in-hospital CoC; • 41.2% achieved 25.0% of the highest feasible SECON; • Patients achieving 25.0% of the highest feasible in-hospital continuity were similar to patients with lower continuity levels in terms of illness severity, comorbidities, baseline cognitive and physical status and length of stay; • 25.0% of the maximum CoC was associated with lower odds of cognitive decline (OR = 0.64, 95% CI) and higher odds of high satisfaction with the hospital care experience (OR = 1.52, 95% CI); • 25.0% of the maximum SECON was associated only with higher odds of high satisfaction with the hospital care experience (OR = 1.43, 95%CI); • No significant associations were found between the CoC and SECON and decline in physical functioning. |
| A (Selection Bias) | B (Study Design) | C (Confounder) | D (Blinding) | E (Data Collection Method) | F (Withdrawals/Dropouts) | Global Rating | |
|---|---|---|---|---|---|---|---|
| (Dal Molin et al., 2018) [29] | 2 | 1 | 3 | 2 | 1 | NA | 2 |
| (Moura et al., 2020) [31] | 3 | 3 | 1 | 1 | 1 | NA | 3 |
| (Naef, Ernst, and Petry, 2019) [30] | 2 | 3 | 1 | 1 | 1 | NA | 2 |
| (Chen, 2020) [33] | 1 | 2 | 1 | 1 | 1 | NA | 1 |
| (Tonkikh, Zisberg, and Shadmi, 2020) [32] | 2 | 2 | 1 | 1 | 1 | NA | 1 |
| 1—Strong; 2—Moderate; 3—Weak; NA—Non-applicable. | |||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gonçalves, I.; Mendes, D.A.; Caldeira, S.; Jesus, É.; Nunes, E. The Primary Nursing Care Model and Inpatients’ Nursing-Sensitive Outcomes: A Systematic Review and Narrative Synthesis of Quantitative Studies. Int. J. Environ. Res. Public Health 2023, 20, 2391. https://doi.org/10.3390/ijerph20032391
Gonçalves I, Mendes DA, Caldeira S, Jesus É, Nunes E. The Primary Nursing Care Model and Inpatients’ Nursing-Sensitive Outcomes: A Systematic Review and Narrative Synthesis of Quantitative Studies. International Journal of Environmental Research and Public Health. 2023; 20(3):2391. https://doi.org/10.3390/ijerph20032391
Chicago/Turabian StyleGonçalves, Isabel, Diana Arvelos Mendes, Sílvia Caldeira, Élvio Jesus, and Elisabete Nunes. 2023. "The Primary Nursing Care Model and Inpatients’ Nursing-Sensitive Outcomes: A Systematic Review and Narrative Synthesis of Quantitative Studies" International Journal of Environmental Research and Public Health 20, no. 3: 2391. https://doi.org/10.3390/ijerph20032391
APA StyleGonçalves, I., Mendes, D. A., Caldeira, S., Jesus, É., & Nunes, E. (2023). The Primary Nursing Care Model and Inpatients’ Nursing-Sensitive Outcomes: A Systematic Review and Narrative Synthesis of Quantitative Studies. International Journal of Environmental Research and Public Health, 20(3), 2391. https://doi.org/10.3390/ijerph20032391