
An Augmented Reality (AR) App Enhances the Pulmonary Function and Potency/Feasibility of Perioperative Rehabilitation in Patients Undergoing Orthopedic Surgery


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Intervention
2.3. Participants
2.4. Ethical Statement
2.5. Outcome Assessment
2.6. Data Analysis
3. Results
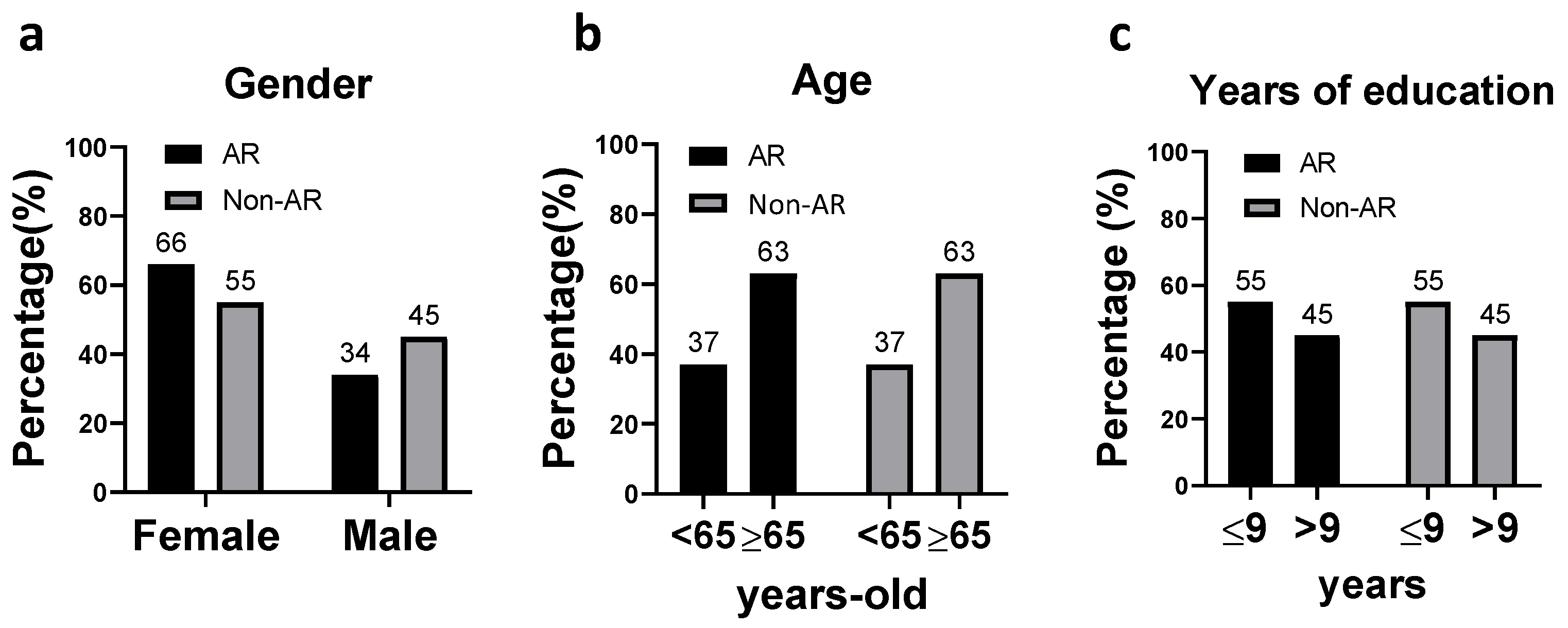
3.1. Demographic Characteristics
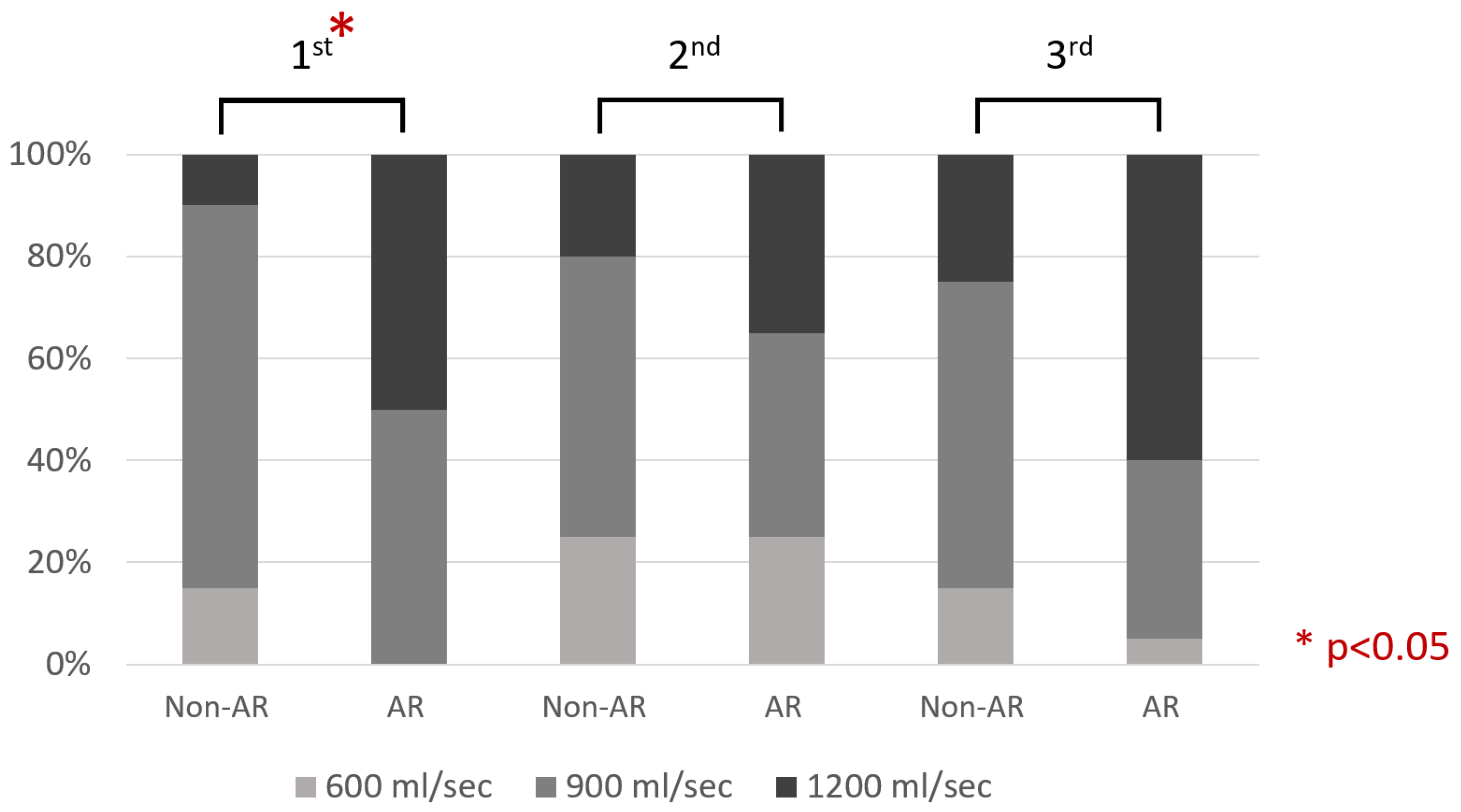
3.2. Objective Outcome
3.3. Subjective Assessment
3.4. Descriptive Feedback
4. Discussion
Limitation of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- National Development Council. Available online: https://www.ndc.gov.tw/Content_List.aspx?n=D527207EEEF59B9B (accessed on 1 June 2021).
- Talmo, C.T.; Robbins, C.E.; Bono, J.V. Total joint replacement in the elderly patient. Clin. Geriatr. Med. 2010, 26, 517–529. [Google Scholar] [CrossRef] [PubMed]
- Lin, F.-H.; Chen, H.-C.; Lin, C.; Chiu, Y.-L.; Lee, H.-S.; Chang, H.; Huang, G.-S.; Chang, H.-L.; Yeh, S.-J.; Su, W.; et al. The increase in total knee replacement surgery in Taiwan: A 15-year retrospective study. Medicine 2018, 97, e11749. [Google Scholar] [CrossRef] [PubMed]
- Leme, L.E.G.; Sitta, M.d.C.; Toledo, M.; Henriques, S.d.S. Orthopedic Surgery among the Elderly: Clinical Characteristics. Rev. Bras. Ortop. 2011, 46, 238–246. [Google Scholar] [CrossRef]
- Greenstein, A.S.; Gorczyca, J.T. Orthopedic Surgery and the Geriatric Patient. Clin. Geriatr. Med. 2019, 35, 65–92. [Google Scholar] [CrossRef] [PubMed]
- Pioli, G.; Bendini, C.; Pignedoli, P.; Giusti, A.; Marsh, D. Orthogeriatric co-management—Managing frailty as well as fragility. Injury 2018, 49, 1398–1402. [Google Scholar] [CrossRef]
- Healy, W.L.; Della Valle, C.J.; Iorio, R.; Berend, K.R.; Cushner, F.D.; Dalury, D.F.; Lonner, J.H. Complications of total knee arthroplasty: Standardized list and definitions of the Knee Society. Clin. Orthop. Relat. Res. 2013, 471, 215–220. [Google Scholar] [CrossRef]
- Gupta, S.; Fernandes, R.J.; Rao, J.S.; Dhanpal, R. Perioperative risk factors for pulmonary complications after non-cardiac surgery. J. Anaesthesiol. Clin. Pharmacol. 2020, 36, 88–93. [Google Scholar] [CrossRef]
- Arozullah, A.M.; Khuri, S.F.; Henderson, W.G.; Daley, J.; Participants in the National Veterans Affairs Surgical Quality Improvement Program. Development and validation of a multifactorial risk index for predicting postoperative pneumonia after major noncardiac surgery. Ann. Intern. Med. 2001, 135, 847–857. [Google Scholar] [CrossRef]
- Kelkar, K.V. Post-operative pulmonary complications after non-cardiothoracic surgery. Indian J. Anaesth. 2015, 59, 599–605. [Google Scholar] [CrossRef]
- Song, K.; Rong, Z.; Yang, X.; Yao, Y.; Shen, Y.; Shi, D.; Xu, Z.; Chen, D.; Zheng, M.; Jiang, Q. Early Pulmonary Com-plications following Total Knee Arthroplasty under General Anesthesia: A Prospective Cohort Study Using CT Scan. BioMed Res. Int. 2016, 2016, 4062043. [Google Scholar] [CrossRef]
- Canet, J.; Gallart, L.; Gomar, C.; Paluzie, G.; Vallès, J.; Castillo, J.; Sabaté, S.; Mazo, V.; Briones, Z.; Sanchis, J.; et al. Prediction of postoperative pulmonary complications in a population-based surgical cohort. Anesthesiology 2010, 113, 1338–1350. [Google Scholar] [CrossRef] [PubMed]
- Kitahata, Y.; Hirono, S.; Kawai, M.; Okada, K.I.; Miyazawa, M.; Shimizu, A.; Kobayashi, R.; Ueno, M.; Hayami, S.; Shimokawa, T.; et al. Intensive perioperative rehabilitation improves surgical outcomes after pancreati-coduodenectomy. Langenbeck’s Arch. Surg. 2018, 403, 711–718. [Google Scholar] [CrossRef] [PubMed]
- Qaseem, A.; Snow, V.; Fitterman, N.; Hornbake, E.R.; Lawrence, V.A.; Smetana, G.W.; Weiss, K.; Owens, D.K.; Aronson, M.; Barry, P.; et al. Risk assessment for and strategies to reduce perioperative pulmonary complications for patients undergoing noncardiothoracic surgery: A guideline from the American College of Physicians. Ann. Intern. Med. 2006, 144, 575–580. [Google Scholar] [CrossRef] [PubMed]
- Carli, F.; Scheede-Bergdahl, C. Prehabilitation to enhance perioperative care. Anesthesiol. Clin. 2015, 33, 17–33. [Google Scholar] [CrossRef]
- Bickerton, W.L.; Humphreys, G.W.; Riddoch, M.J. The use of memorised verbal scripts in the rehabilitation of action disorganisation syndrome. Neuropsychol. Rehabil. 2006, 16, 155–177. [Google Scholar] [CrossRef]
- Pereira, M.F.; Prahm, C.; Kolbenschlag, J.; Oliveira, E.; Rodrigues, N.F. Application of AR and VR in hand rehabilitation: A systematic review. J. Biomed. Inform. 2020, 111, 103584. [Google Scholar] [CrossRef]
- Alamri, A.; Cha, J.; Saddik, A.E. AR-REHAB: An Augmented Reality Framework for Poststroke-Patient Rehabilitation. IEEE Trans. Instrum. Meas. 2010, 59, 2554–2563. [Google Scholar] [CrossRef]
- Cerritelli, F.; Chiera, M.; Abbro, M.; Megale, V.; Esteves, J.; Gallace, A.; Manzotti, A. The Challenges and Perspectives of the Integration Between Virtual and Augmented Reality and Manual Therapies. Front. Neurol. 2021, 12, 700211. [Google Scholar] [CrossRef]
- Azuma, R.T. A survey of augmented reality. Presence Teleoperators Virtual Environ. 1997, 6, 355–385. [Google Scholar] [CrossRef]
- Dey, A.; Billinghurst, M.; Lindeman, R.W.; Swan, J.E., 2nd. A Systematic Review of 10 Years of Augmented Reality Usability Studies: 2005 to 2014. Front. Robot. AI 2018, 5, 37. [Google Scholar] [CrossRef]
- Johnson, D.; Deterding, S.; Kuhn, K.-A.; Staneva, A.; Stoyanov, S.; Hides, L. Gamification for health and wellbeing: A systematic review of the literature. Internet Interv. 2016, 6, 89–106. [Google Scholar] [CrossRef] [PubMed]
- Meijer, H.A.; Graafland, M.; Goslings, J.C.; Schijven, M.P. Systematic Review on the Effects of Serious Games and Wearable Technology Used in Rehabilitation of Patients With Traumatic Bone and Soft Tissue Injuries. Arch. Phys. Med. Rehabil. 2018, 99, 1890–1899. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.-T.; Chen, K.-H.; Ban, S.-L.; Tung, K.Y.; Chen, L.-R. Evaluation of leap motion control for hand rehabilitation in burn patients: An experience in the dust explosion disaster in Formosa Fun Coast. Burns 2019, 45, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, E.; Zucchella, C.; Bottiroli, S.; Federico, A.; Giugno, R.; Sandrini, G.; Chiamulera, C.; Tamburin, S. Telemedicine and Virtual Reality for Cognitive Rehabilitation: A Roadmap for the COVID-19 Pandemic. Front. Neurol. 2020, 11, 926. [Google Scholar] [CrossRef] [PubMed]
- Portalés, C.; Lerma, J.L.; Navarro, S. Augmented reality and photogrammetry: A synergy to visualize physical and virtual city environments. Isprs J. Photogramm. Remote Sens. 2010, 65, 134–142. [Google Scholar] [CrossRef]
- Phan, H.L.; Le, T.H.; Lim, J.M.; Hwang, C.H.; Koo, K.-i. Effectiveness of Augmented Reality in Stroke Rehabilitation: A Meta-Analysis. Appl. Sci. 2022, 12, 1848. [Google Scholar] [CrossRef]
- Gil, M.J.V.; Gonzalez-Medina, G.; Lucena-Anton, D.; Perez-Cabezas, V.; Ruiz-Molinero, M.D.C.; Martín-Valero, R. Augmented Reality in Physical Therapy: Systematic Review and Meta-analysis. JMIR Serious Games 2021, 9, e30985. [Google Scholar] [CrossRef]
- Held, J.P.O.; Yu, K.; Pyles, C.; Veerbeek, J.M.; Bork, F.; Heining, S.M.; Navab, N.; Luft, A.R. Augmented Reality-Based Rehabilitation of Gait Impairments: Case Report. JMIR Mhealth Uhealth 2020, 8, e17804. [Google Scholar] [CrossRef]
- Penn, I.-W.; Chuang, E.; Chuang, T.-Y.; Yang, C.-Y. Effects of Virtual-Reality-Augmented Cardiopulmonary Rehabilitation Programs for Patients with Cardiovascular Diseases: A Systemic Review. Neuropsychiatry 2018, 8, 1630–1636. [Google Scholar] [CrossRef]
- Commodari, E.; Guarnera, M. Attention and aging. Aging Clin. Exp. Res. 2008, 20, 578–584. [Google Scholar] [CrossRef]
- Bank, P.J.M.; Cidota, M.A.; Ouwehand, P.E.W.; Lukosch, S.G. Patient-Tailored Augmented Reality Games for Assessing Upper Extremity Motor Impairments in Parkinson’s Disease and Stroke. J. Med. Syst. 2018, 42, 246. [Google Scholar] [CrossRef] [PubMed]
- Di Giacomo, D.; Guerra, F.; Perilli, E.; Ranieri, J. Technophobia as emerging risk factor in aging: Investigation on computer anxiety dimension. Health Psychol. Res. 2020, 8, 8207. [Google Scholar] [CrossRef] [PubMed]
- Koutsiana, E.; Ladakis, I.; Fotopoulos, D.; Chytas, A.; Kilintzis, V.; Chouvarda, I. Serious Gaming Technology in Upper Extremity Rehabilitation: Scoping Review. JMIR Serious Games 2020, 8, e19071. [Google Scholar] [CrossRef] [PubMed]
- Seals, A.; Olaosebikan, M.; Otiono, J.; Shaer, O.; Nov, O. Effects of Self-focused Augmented Reality on Health Perceptions During the COVID-19 Pandemic: A Web-Based Between-Subject Experiment. J. Med. Internet Res. 2021, 23, e26963. [Google Scholar] [CrossRef]
- Gajarawala, S.N.; Pelkowski, J.N. Telehealth Benefits and Barriers. J. Nurse Pract. 2021, 17, 218–221. [Google Scholar] [CrossRef]
- Mehra, V.M.; Gaalema, D.E.; Pakosh, M.; Grace, S.L. Systematic review of cardiac rehabilitation guidelines: Quality and scope. Eur. J. Prev. Cardiol. 2020, 27, 912–928. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Domain | Item | Statement of Item | Agreement Scale |
|---|---|---|---|
| Feasibility | Familiarity | Are you familiar with the rehabilitation program? | 5: strongly agree 4: agree 3: neutral 2: disagree 1: strongly disagree |
| Confidence | Are you confident with the rehabilitation program? | (same as above) | |
| Anxiety | Are you anxious about not being able to finish the rehabilitation program? | (same as above) | |
| Potency | Cooperation | Are you willing to cooperate with the healthcare providers to finish the rehabilitation program? | (same as above) |
| Educative effect | Do you agree that the rehabilitation program is educative? | (same as above) | |
| Accuracy | Do you agree that the rehabilitation program can precisely convey information? | (same as above) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, P.-H.; Wang, Y.-J.; Chen, Y.-W.; Hsu, P.-T.; Yang, Y.-Y. An Augmented Reality (AR) App Enhances the Pulmonary Function and Potency/Feasibility of Perioperative Rehabilitation in Patients Undergoing Orthopedic Surgery. Int. J. Environ. Res. Public Health 2023, 20, 648. https://doi.org/10.3390/ijerph20010648
Wang P-H, Wang Y-J, Chen Y-W, Hsu P-T, Yang Y-Y. An Augmented Reality (AR) App Enhances the Pulmonary Function and Potency/Feasibility of Perioperative Rehabilitation in Patients Undergoing Orthopedic Surgery. International Journal of Environmental Research and Public Health. 2023; 20(1):648. https://doi.org/10.3390/ijerph20010648
Chicago/Turabian StyleWang, Pin-Hsuan, Yi-Jen Wang, Yu-Wei Chen, Po-Ting Hsu, and Ying-Ying Yang. 2023. "An Augmented Reality (AR) App Enhances the Pulmonary Function and Potency/Feasibility of Perioperative Rehabilitation in Patients Undergoing Orthopedic Surgery" International Journal of Environmental Research and Public Health 20, no. 1: 648. https://doi.org/10.3390/ijerph20010648
APA StyleWang, P.-H., Wang, Y.-J., Chen, Y.-W., Hsu, P.-T., & Yang, Y.-Y. (2023). An Augmented Reality (AR) App Enhances the Pulmonary Function and Potency/Feasibility of Perioperative Rehabilitation in Patients Undergoing Orthopedic Surgery. International Journal of Environmental Research and Public Health, 20(1), 648. https://doi.org/10.3390/ijerph20010648