
Assessment of Nutritional Status and Risk of Malnutrition Using Adapted Standard Tools in Patients with Mental Illness and in Need of Intensive Psychiatric Treatment

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
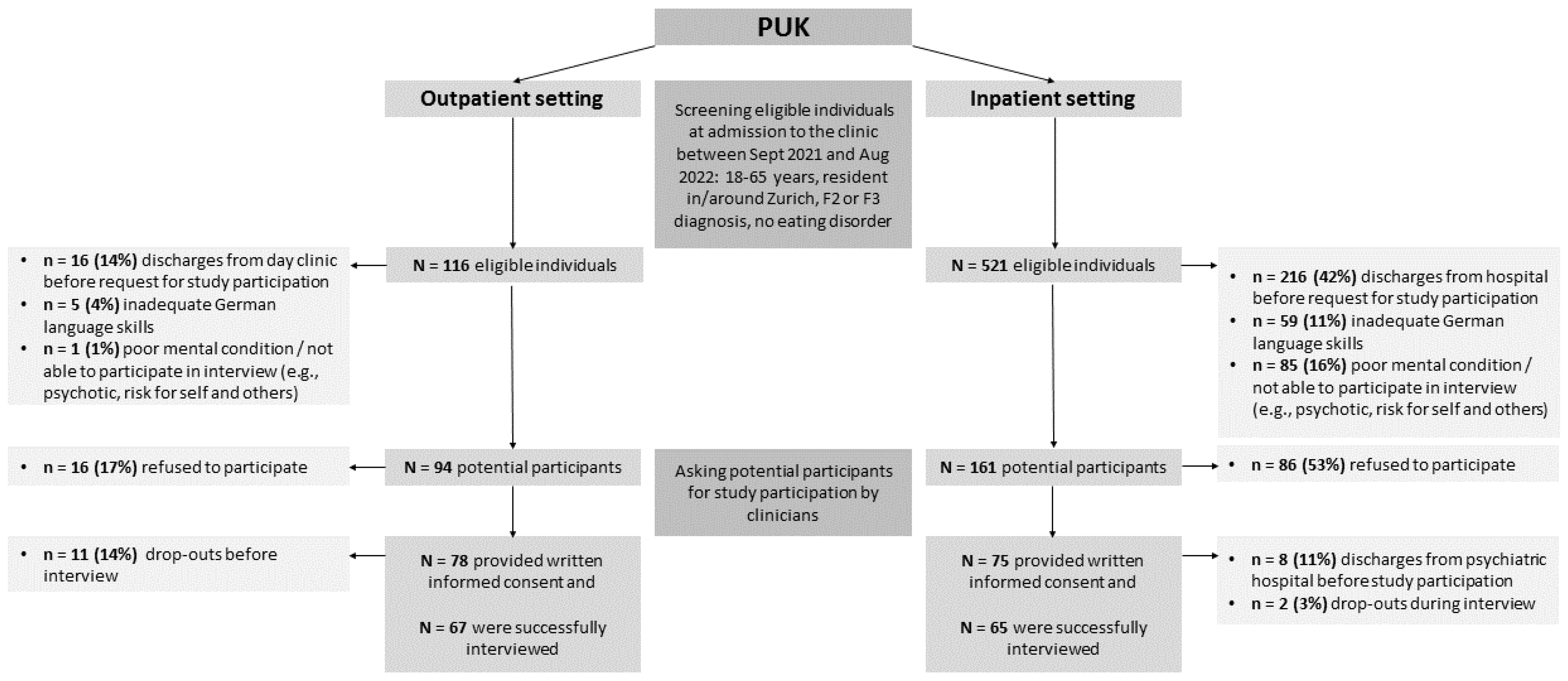
2.1. Participants and Procedure
2.2. Measures
2.2.1. Anthropometric Measures and Weight Changes
2.2.2. Nutrition Risk Screening
2.2.3. Mental Condition
2.2.4. Biochemical Parameters
2.2.5. Personal and Medical Data
2.2.6. Statistical Analyses
3. Results
3.1. Characteristics of the Participants
3.2. Nutritional Status and Risk of Malnutrition
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Thornicroft, G. Premature death among people with mental illness. BMJ 2013, 346, f2969. [Google Scholar] [CrossRef] [PubMed]
- Walker, E.R.; McGee, R.E.; Druss, B.G. Mortality in mental disorders and global disease burden implications: A systematic review and meta-analysis. JAMA Psychiatry 2015, 72, 334–341. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, D.; Hancock, K.J.; Kisely, S. The gap in life expectancy from preventable physical illness in psychiatric patients in Western Australia: Retrospective analysis of population based registers. BMJ 2013, 346, f2539. [Google Scholar] [CrossRef] [PubMed]
- Firth, J.; Stubbs, B.; Teasdale, S.B.; Ward, P.B.; Veronese, N.; Shivappa, N.; Hebert, J.R.; Berk, M.; Yung, A.R.; Sarris, J. Diet as a hot topic in psychiatry: A population-scale study of nutritional intake and inflammatory potential in severe mental illness. World Psychiatry 2018, 17, 365–367. [Google Scholar] [CrossRef]
- Teasdale, S.B.; Ward, P.B.; Samaras, K.; Firth, J.; Stubbs, B.; Tripodi, E.; Burrows, T.L. Dietary intake of people with severe mental illness: Systematic review and meta-analysis. Br. J. Psychiatry 2019, 214, 251–259. [Google Scholar] [CrossRef]
- Teasdale, S.B.; Samaras, K.; Wade, T.; Jarman, R.; Ward, P.B. A review of the nutritional challenges experienced by people living with severe mental illness: A role for dietitians in addressing physical health gaps. J. Hum. Nutr. Diet 2017, 30, 545–553. [Google Scholar] [CrossRef]
- Firth, J.; Siddiqi, N.; Koyanagi, A.; Siskind, D.; Rosenbaum, S.; Galletly, C.; Allan, S.; Caneo, C.; Carney, R.; Carvalho, A.F.; et al. The Lancet Psychiatry Commission: A blueprint for protecting physical health in people with mental illness. Lancet Psychiatry 2019, 6, 675–712. [Google Scholar] [CrossRef]
- Hancox, L.E.; Lee, P.S.; Armaghanian, N.; Hirani, V.; Wakefield, G. Nutrition risk screening methods for adults living with severe mental illness: A scoping review. Nutr. Diet 2021, 79, 349–363. [Google Scholar] [CrossRef]
- de van der Schueren, M.A.E.; Jager-Wittenaar, H. Malnutrition risk screening: New insights in a new era. Clin. Nutr. 2022, 41, 2163–2168. [Google Scholar] [CrossRef]
- Soeters, P.B.; Reijven, P.L.; van Bokhorst-de van der Schueren, M.A.; Schols, J.M.; Halfens, R.J.; Meijers, J.M.; van Gemert, W.G. A rational approach to nutritional assessment. Clin. Nutr. 2008, 27, 706–716. [Google Scholar] [CrossRef]
- Schuetz, P.; Seres, D.; Lobo, D.N.; Gomes, F.; Kaegi-Braun, N.; Stanga, Z. Management of disease-related malnutrition for patients being treated in hospital. Lancet 2021, 398, 1927–1938. [Google Scholar] [CrossRef] [PubMed]
- Barker, L.A.; Gout, B.S.; Crowe, T.C. Hospital malnutrition: Prevalence, identification and impact on patients and the healthcare system. Int. J. Environ. Res. Public Health 2011, 8, 514–527. [Google Scholar] [CrossRef] [PubMed]
- Kaegi-Braun, N.; Mueller, M.; Schuetz, P.; Mueller, B.; Kutz, A. Evaluation of Nutritional Support and In-Hospital Mortality in Patients With Malnutrition. JAMA Netw. Open 2021, 4, e2033433. [Google Scholar] [CrossRef]
- Guenter, P.; Abdelhadi, R.; Anthony, P.; Blackmer, A.; Malone, A.; Mirtallo, J.M.; Phillips, W.; Resnick, H.E. Malnutrition diagnoses and associated outcomes in hospitalized patients: United States, 2018. Nutr. Clin. Pr. 2021, 36, 957–969. [Google Scholar] [CrossRef] [PubMed]
- Schuetz, P.; Fehr, R.; Baechli, V.; Geiser, M.; Deiss, M.; Gomes, F.; Kutz, A.; Tribolet, P.; Bregenzer, T.; Braun, N.; et al. Individualised nutritional support in medical inpatients at nutritional risk: A randomised clinical trial. Lancet 2019, 393, 2312–2321. [Google Scholar] [CrossRef] [PubMed]
- Reber, E.; Gomes, F.; Vasiloglou, M.F.; Schuetz, P.; Stanga, Z. Nutritional Risk Screening and Assessment. J. Clin. Med. 2019, 8, 1065. [Google Scholar] [CrossRef]
- Mueller-Stierlin, A.S.; Cornet, S.; Peisser, A.; Jaeckle, S.; Lehle, J.; Moerkl, S.; Teasdale, S.B. Implications of Dietary Intake and Eating Behaviors for People with Serious Mental Illness: A Qualitative Study. Nutrients 2022, 14, 2616. [Google Scholar] [CrossRef]
- Abayomi, J.; Hackett, A. Assessment of malnutrition in mental health clients: Nurses' judgement vs. a nutrition risk tool. J. Adv. Nurs. 2004, 45, 430–437. [Google Scholar] [CrossRef]
- Kondrup, J.; Rasmussen, H.H.; Hamberg, O.; Stanga, Z. Nutritional risk screening (NRS 2002): A new method based on an analysis of controlled clinical trials. Clin. Nutr. 2003, 22, 321–336. [Google Scholar] [CrossRef]
- Kaiser, M.J.; Bauer, J.M.; Ramsch, C.; Uter, W.; Guigoz, Y.; Cederholm, T.; Thomas, D.R.; Anthony, P.; Charlton, K.E.; Maggio, M.; et al. Validation of the Mini Nutritional Assessment short-form (MNA-SF): A practical tool for identification of nutritional status. J. Nutr. Health Aging 2009, 13, 782–788. [Google Scholar] [CrossRef]
- Hotzy, F.; Risch, L.; Mötteli, S. Nutritional Needs in Mental Healthcare: Study Protocol of a Prospective Analytic Observational Study Assessing Nutritional Status, Eating Behavior and Barriers to Healthy Eating in Psychiatric Inpatients and Outpatients Compared to Healthy Adults. Front. Psychiatry 2022, 13, 906234. [Google Scholar] [CrossRef] [PubMed]
- Mötteli, S.; Schori, D.; Schmidt, H.; Seifritz, E.; Jäger, M. Utilization and Effectiveness of Home Treatment for People With Acute Severe Mental Illness: A Propensity-Score Matching Analysis of 19 Months of Observation. Front. Psychiatry 2018, 9, 495. [Google Scholar] [CrossRef] [PubMed]
- Zumstein, N.; Riese, F. Defining Severe and Persistent Mental Illness-A Pragmatic Utility Concept Analysis. Front. Psychiatry 2020, 11, 648. [Google Scholar] [CrossRef]
- LimeSurvey: An Open Source Survey Tool. Available online: http://www.limesurvey.org (accessed on 3 October 2022).
- Hall, R.C. Global assessment of functioning. A modified scale. Psychosomatics 1995, 36, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Rubenstein, L.Z.; Harker, J.O.; Salvà, A.; Guigoz, Y.; Vellas, B. Screening for undernutrition in geriatric practice: Developing the short-form mini-nutritional assessment (MNA-SF). J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M366–M372. [Google Scholar] [CrossRef]
- Prinz, U.; Nutzinger, D.O.; Schulz, H.; Petermann, F.; Braukhaus, C.; Andreas, S. Comparative psychometric analyses of the SCL-90-R and its short versions in patients with affective disorders. BMC Psychiatry 2013, 13, 104. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Löwe, B.; Kroenke, K.; Herzog, W.; Gräfe, K. Measuring depression outcome with a brief self-report instrument: Sensitivity to change of the Patient Health Questionnaire (PHQ-9). J. Affect. Disord. 2004, 81, 61–66. [Google Scholar] [CrossRef]
- Busner, J.; Targum, S.D. The clinical global impressions scale: Applying a research tool in clinical practice. Psychiatry 2007, 4, 28–37. [Google Scholar]
- Zimmermann, U.; Kraus, T.; Himmerich, H.; Schuld, A.; Pollmächer, T. Epidemiology, implications and mechanisms underlying drug-induced weight gain in psychiatric patients. J. Psychiatr. Res. 2003, 37, 193–220. [Google Scholar] [CrossRef]
- Benkert, O.; Hippius, H. Kompendium der Psychiatrischen Pharmakotherapie, 13th ed.; Springer: Berlin, Germany, 2021. [Google Scholar]
- Yusuf, S.; Hawken, S.; Ounpuu, S.; Dans, T.; Avezum, A.; Lanas, F.; McQueen, M.; Budaj, A.; Pais, P.; Varigos, J.; et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): Case-control study. Lancet 2004, 364, 937–952. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.; Joseph, L.; Pilote, L. Obesity and C-reactive protein in various populations: A systematic review and meta-analysis. Obes. Rev. 2013, 14, 232–244. [Google Scholar] [CrossRef] [PubMed]
- Teasdale, S.B.; Moerkl, S.; Moetteli, S.; Mueller-Stierlin, A. The Development of a Nutrition Screening Tool for Mental Health Settings Prone to Obesity and Cardiometabolic Complications: Study Protocol for the NutriMental Screener. Int. J. Environ. Res. Public Health 2021, 18, 11269. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Sociodemographic Variables | Inpatients (n = 65) | Outpatients (n = 67) | ||
|---|---|---|---|---|
| n | % | n | % | |
| Gender, female | 32 | 49 | 34 | 51 |
| Age > 40 years | 32 | 49 | 34 | 51 |
| Swiss nationality | 46 | 79 | 45 | 79 |
| Education | ||||
| Compulsory schooling | 14 | 22 | 9 | 13 |
| Vocational education | 22 | 34 | 30 | 45 |
| Matura (high school exit exam) | 7 | 11 | 6 | 9 |
| Higher vocational education | 8 | 12 | 8 | 12 |
| University | 14 | 21 | 14 | 21 |
| Source of income | ||||
| Salary | 21 | 32 | 32 | 47 |
| Disability pension | 18 | 28 | 5 | 8 |
| Social-welfare benefits | 12 | 18 | 15 | 22 |
| Support by family | 9 | 14 | 10 | 15 |
| Savings | 3 | 5 | 5 | 8 |
| Unknown | 2 | 3 | 0 | 0 |
| Housing situation | ||||
| Alone | 21 | 32 | 29 | 43 |
| Together with others | 37 | 57 | 38 | 57 |
| Residential care home | 6 | 9 | 0 | 0 |
| Homeless | 1 | 2 | 0 | 0 |
| Variables | Inpatients (n = 65) | Outpatients (n = 67) | ||||
|---|---|---|---|---|---|---|
| n or M | % or SD | n or M | % or SD | Chi-Square or t-Test | p | |
| Main psychiatric diagnosis (F3) | 40 | 62 | 58 | 87 | 10.81 | 0.001 |
| Age of first occurrence of psychiatric problems (years) | 22.7 | 12.3 | 28.0 | 15.3 | 2.17 | 0.032 |
| Involuntary admission (IA) | 14 | 23 | 0 | 0 | ||
| CGI at admission to hospital | 65.81 | <0.001 | ||||
| Moderately ill (4) | 4 | 7 | 9 | 15 | ||
| Significantly ill (5) | 15 | 25 | 49 | 83 | ||
| (Extremely) seriously ill (6–7) | 40 | 68 | 1 | 2 | ||
| GAF categories (interviews, in average 14 days after admission) | 3.64 | 0.162 | ||||
| Mild impairment (GAF 61–90) | 17 | 26 | 12 | 18 | ||
| Moderate impairment (GAF 41–60) | 31 | 48 | 43 | 64 | ||
| Pervasive impairment (GAF 01–40) | 17 | 26 | 12 | 18 | ||
| SCL-K-9 (higher scores = more psychiatric symptoms) | 1.8 | 0.8 | 2.0 | 0.9 | 1.31 | 0.192 |
| PHQ-D (higher scores = more depressive symptoms) | 13.4 | 6.3 | 16.3 | 5.1 | 2.83 | 0.005 |
| Prescribed medication | ||||||
| Number of medications | 3.7 | 2.0 | 2.1 | 1.2 | 5.39 | <0.001 |
| Sum score (higher scores = negative effect on weight gain) | 2.9 | 2.7 | 1.6 | 2.0 | 3.35 | <0.001 |
| BMI (kg/m2) | 25.3 | 5.0 | 27.9 | 5.3 | 2.92 | 0.004 |
| WHR (m) | 0.9 | 0.1 | 0.9 | 0.1 | 1.02 | 0.310 |
| Weight gain in last 3–6 months | ||||||
| Proportion (%) | 18 | 28 | 39 | 58 | 12.52 | <0.001 |
| kg | 1.9 | 4.8 | 3.7 | 4.7 | 2.16 | 0.033 |
| Weight loss in last 3–6 months | ||||||
| Proportion (%) | 28 | 43 | 20 | 30 | 2.49 | 0.114 |
| kg | 2.6 | 4.4 | 3.0 | 6.6 | 0.43 | 0.672 |
| Risk of malnutrition (combined adapted NRS and MNA-SF) | 21 | 32 | 23 | 34 | 0.06 | 0.806 |
| Subjective evaluation of nutritional status (1–10 = better) | 6.6 | 2.3 | 5.5 | 2.2 | 2.97 | 0.004 |
| Selected routine laboratory results (proportion within reference values) | ||||||
| Cholesterol (<5.2 mmol/L) | 35 | 58 | na | na | ||
| Triglyceride (<1.7 mmol/L) | 41 | 70 | na | na | ||
| C-reactive protein (<3 mg/L) | 41 | 67 | na | na | ||
| Folate acid (>7 nmol/L) | 52 | 93 | na | na | ||
| Vitamin B12 (150–700 pmol/L) | 51 | 90 | na | na | ||
| Nutrition-related diseases (e.g., diabetes, celiac disease, food allergies) | 12 | 19 | 24 | 36 | 5.01 | 0.025 |
| Gastrointestinal problems (e.g., swallowing, nausea, diarrhea) | 16 | 25 | 8 | 12 | 3.56 | 0.059 |
| Food intolerances | 21 | 32 | 34 | 51 | 4.62 | 0.032 |
| Risk of Malnutrition | |||
|---|---|---|---|
| Variables | B | SD | OR (95% CI) |
| Constant | −2.21 | 1.60 | 0.11 |
| Gender | 0.24 | 0.44 | 1.27 (0.53–3.02) |
| Age | 0.03 | 0.02 | 1.03 (0.99–1.07) |
| Education | −0.48 | 0.47 | 0.62 (0.25–1.55) |
| Diagnoses (F2 or F3) | 0.13 | 0.51 | 1.14 (0.42–3.09) |
| BMI | −0.07 | 0.05 | 0.94 (0.86–1.03) |
| Weight loss | 1.91 | 0.46 | 6.75 (2.76–16.52) ** |
| SCL-K-9 | 0.65 | 0.27 | 1.91 (1.13–3.21) * |
| −2LL | 132.24 | ||
| Omnibus test | χ2 = 35.80, df = 7, p < 0.001 | ||
| Nagelkerkers R2 | 33% | ||
| Classification accuracy | 74% | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Risch, L.; Hotzy, F.; Vetter, S.; Hiller, S.; Wallimann, K.; Seifritz, E.; Mötteli, S. Assessment of Nutritional Status and Risk of Malnutrition Using Adapted Standard Tools in Patients with Mental Illness and in Need of Intensive Psychiatric Treatment. Int. J. Environ. Res. Public Health 2023, 20, 109. https://doi.org/10.3390/ijerph20010109
Risch L, Hotzy F, Vetter S, Hiller S, Wallimann K, Seifritz E, Mötteli S. Assessment of Nutritional Status and Risk of Malnutrition Using Adapted Standard Tools in Patients with Mental Illness and in Need of Intensive Psychiatric Treatment. International Journal of Environmental Research and Public Health. 2023; 20(1):109. https://doi.org/10.3390/ijerph20010109
Chicago/Turabian StyleRisch, Ladina, Florian Hotzy, Stefan Vetter, Sascha Hiller, Kathrin Wallimann, Erich Seifritz, and Sonja Mötteli. 2023. "Assessment of Nutritional Status and Risk of Malnutrition Using Adapted Standard Tools in Patients with Mental Illness and in Need of Intensive Psychiatric Treatment" International Journal of Environmental Research and Public Health 20, no. 1: 109. https://doi.org/10.3390/ijerph20010109
APA StyleRisch, L., Hotzy, F., Vetter, S., Hiller, S., Wallimann, K., Seifritz, E., & Mötteli, S. (2023). Assessment of Nutritional Status and Risk of Malnutrition Using Adapted Standard Tools in Patients with Mental Illness and in Need of Intensive Psychiatric Treatment. International Journal of Environmental Research and Public Health, 20(1), 109. https://doi.org/10.3390/ijerph20010109