
Analysis of Characteristics and Quality of Life of Elderly Women with Mild to Moderate Urinary Incontinence in Community Dwellings

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Measurement
2.2. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Trial Registration
References
- Sultan, A.H.; Monga, A.; Lee, J.; Emmanuel, A.; Norton, C.; Santoro, G.; Hull, T.; Berghmans, B.; Brody, S.; Haylen, B.T. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female anorectal dysfunction. Neurourol. Urodyn. 2017, 36, 10–34. [Google Scholar] [CrossRef] [Green Version]
- Cerruto, M.A.; D’Elia, C.; Aloisi, A.; Fabrello, M.; Artibani, W. Prevalence, incidence and obstetric factors’ impact on female urinary incontinence in Europe: A systematic review. Urol. Int. 2013, 90, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Lukacz, E.S.; Santiago-Lastra, Y.; Albo, M.E.; Brubaker, L. Urinary Incontinence in Women: A Review. JAMA 2017, 318, 1592–1604. [Google Scholar] [CrossRef] [PubMed]
- Anger, J.T.; Saigal, C.S.; Litwin, M.S. The prevalence of urinary incontinence among community dwelling adult women: Results from the National Health and Nutrition Examination Survey. J. Urol. 2006, 175, 601–604. [Google Scholar] [CrossRef]
- Hagen, S.; McClurg, D.; Bugge, C.; Hay-Smith, J.; Dean, S.G.; Elders, A.; Glazener, C.; Abdel-Fattah, M.; Agur, W.I.; Booth, J.; et al. Effectiveness and cost-effectiveness of basic versus biofeedback-mediated intensive pelvic floor muscle training for female stress or mixed urinary incontinence: Protocol for the OPAL randomised trial. BMJ Open 2019, 9, e024153. [Google Scholar] [CrossRef]
- De Tayrac, R.; Haylen, B.T.; Deffieux, X.; Hermieu, J.F.; Wagner, L.; Amarenco, G.; Labat, J.J.; Leroi, A.M.; Billecocq, S.; Letouzey, V.; et al. French translation of “An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction” published in Int Urogynecol J 2010;21(1):5-26. Prog. Urol. 2016, 26, 197–225. [Google Scholar] [CrossRef]
- Schüssler, B.; Alloussi, S. [Ingelman-Sundberg classification of stress incontinence]. Gynakol. Rundsch. 1983, 23, 166–174. [Google Scholar] [CrossRef]
- Gofrit, O.N.; Landau, E.H.; Shapiro, A.; Pode, D. The Stamey procedure for stress incontinence: Long-term results. Eur. Urol. 1998, 34, 339–343. [Google Scholar] [CrossRef]
- Haylen, B.T.; de Ridder, D.; Freeman, R.M.; Swift, S.E.; Berghmans, B.; Lee, J.; Monga, A.; Petri, E.; Rizk, D.E.; Sand, P.K.; et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Int. Urogynecol. J. 2010, 21, 5–26. [Google Scholar] [CrossRef]
- Almousa, S.; Bandin van Loon, A. The prevalence of urinary incontinence in nulliparous adolescent and middle-aged women and the associated risk factors: A systematic review. Maturitas 2018, 107, 78–83. [Google Scholar] [CrossRef]
- Blaganje, M.; Šćepanović, D.; Žgur, L.; Verdenik, I.; Pajk, F.; Lukanović, A. Non-ablative Er:YAG laser therapy effect on stress urinary incontinence related to quality of life and sexual function: A randomized controlled trial. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 224, 153–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weintraub, A.Y. A Validated Tool Would Greatly Enhance Future Research on the Impact of Surgery on Sexual Function. J. Women Health 2016, 25, 327–328. [Google Scholar] [CrossRef] [PubMed]
- Irwin, G.M. Urinary Incontinence. Prim. Care 2019, 46, 233–242. [Google Scholar] [CrossRef]
- Son, Y.J.; Kwon, B. Predictive risk factors for impaired quality of life in middle-aged women with urinary incontinence. Int. Neurourol. J. 2010, 14, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Guzelsoy, M.; Demirci, H.; Coban, S.; Belkiz Güngör, B.; Ustunyurt, E.; Isildak, S. Impact of urinary incontinence on quality of life among residents living in Turkey. Urol. J. 2014, 11, 1447–1451. [Google Scholar]
- Felce, D.; Perry, J. Quality of life: Its definition and measurement. Res. Dev. Disabil. 1995, 16, 51–74. [Google Scholar] [CrossRef]
- Verbeek, M.; Hayward, L. Pelvic Floor Dysfunction and Its Effect on Quality of Sexual Life. Sex. Med. Rev. 2019, 7, 559–564. [Google Scholar] [CrossRef] [PubMed]
- Gomes, T.A.; Faber, M.A.; Botta, B.; Brito, L.G.O.; Juliato, C.R.T. Severity of urinary incontinence is associated with prevalence of sexual dysfunction. Int. Urogynecol. J. 2020, 31, 1669–1674. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Gao, L.; Jia, Y.; Wang, S.; Wang, H.; Sun, X.; Wang, J. Construction of Progress Prediction Model of Urinary Incontinence in Elderly Women: Protocol for a Multi-Center, Prospective Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 734. [Google Scholar] [CrossRef]
- Lindau, S.T.; Schumm, L.P.; Laumann, E.O.; Levinson, W.; O’Muircheartaigh, C.A.; Waite, L.J. A study of sexuality and health among older adults in the United States. N. Engl. J. Med. 2007, 357, 762–774. [Google Scholar] [CrossRef] [Green Version]
- Pozza, A.; Veale, D.; Marazziti, D.; Delgadillo, J.; Albert, U.; Grassi, G.; Prestia, D.; Dèttore, D. Sexual dysfunction and satisfaction in obsessive compulsive disorder: Protocol for a systematic review and meta-analysis. Syst. Rev. 2020, 9, 8. [Google Scholar] [CrossRef] [PubMed]
- Diokno, A.C.; Newman, D.K.; Low, L.K.; Griebling, T.L.; Maddens, M.E.; Goode, P.S.; Raghunathan, T.E.; Subak, L.L.; Sampselle, C.M.; Boura, J.A.; et al. Effect of Group-Administered Behavioral Treatment on Urinary Incontinence in Older Women: A Randomized Clinical Trial. JAMA Intern. Med. 2018, 178, 1333–1341. [Google Scholar] [CrossRef] [PubMed]
- Hagen, S.; Elders, A.; Stratton, S.; Sergenson, N.; Bugge, C.; Dean, S.; Hay-Smith, J.; Kilonzo, M.; Dimitrova, M.; Abdel-Fattah, M.; et al. Effectiveness of pelvic floor muscle training with and without electromyographic biofeedback for urinary incontinence in women: Multicentre randomised controlled trial. BMJ 2020, 371, m3719. [Google Scholar] [CrossRef] [PubMed]
- De Andrade, R.L.; Bø, K.; Antonio, F.I.; Driusso, P.; Mateus-Vasconcelos, E.C.L.; Ramos, S.; Julio, M.P.; Ferreira, C.H.J. An education program about pelvic floor muscles improved women’s knowledge but not pelvic floor muscle function, urinary incontinence or sexual function: A randomised trial. J. Physiother. 2018, 64, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Zhang, S.W.; Wu, S.L.; Ma, L.; Deng, X.H. The Chinese version of ICIQ: A useful tool in clinical practice and research on urinary incontinence. Neurourol. Urodyn. 2008, 27, 522–524. [Google Scholar] [CrossRef]
- Kocak, I.; Okyay, P.; Dundar, M.; Erol, H.; Beser, E. Female urinary incontinence in the west of Turkey: Prevalence, risk factors and impact on quality of life. Eur. Urol. 2005, 48, 634–641. [Google Scholar] [CrossRef]
- Xu, C.; Chen, M.; Fu, J.; Meng, Y.; Qin, S.; Luo, Y. Urinary incontinence status and risk factors in women aged 50–70 years: A cross-sectional study in Hunan, China. Int. Urogynecol. J. 2021, 32, 95–102. [Google Scholar] [CrossRef]
- Homma, Y. Re: Validation of the overactive bladder symptom score J. G. Blaivas, G. Panagopoulos, J.P. Weiss and C. Somaroo J Urol 2007; 178: 543-547. J. Urol. 2008, 179, 791. [Google Scholar] [CrossRef]
- Bump, R.C.; Mattiasson, A.; Bø, K.; Brubaker, L.P.; DeLancey, J.O.; Klarskov, P.; Shull, B.L.; Smith, A.R. The standardization of terminology of female pelvic organ prolapse and pelvic floor dysfunction. Am. J. Obstet. Gynecol. 1996, 175, 10–17. [Google Scholar] [CrossRef]
- Siccardi, M.A.; Bordoni, B. Anatomy, Abdomen and Pelvis, Perineal Body. In StatPearls; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2022. [Google Scholar]
- Lauper, M.; Kuhn, A.; Gerber, R.; Luginbühl, H.; Radlinger, L. Pelvic floor stimulation: What are the good vibrations? Neurourol. Urodyn. 2009, 28, 405–410. [Google Scholar] [CrossRef]
- El-Haieg, D.O.; Madkour, N.M.; Basha, M.A.A.; Ahmad, R.A.; Sadek, S.M.; Al-Molla, R.M.; Tantwy, E.F.; Almassry, H.N.; Altaher, K.M.; Mahmoud, N.E.M.; et al. Magnetic resonance imaging and 3-dimensional transperineal ultrasound evaluation of pelvic floor dysfunction in symptomatic women: A prospective comparative study. Ultrasonography 2019, 38, 355–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Komesu, Y.M.; Schrader, R.M.; Ketai, L.H.; Rogers, R.G.; Dunivan, G.C. Epidemiology of mixed, stress, and urgency urinary incontinence in middle-aged/older women: The importance of incontinence history. Int. Urogynecol. J. 2016, 27, 763–772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xue, K.; Palmer, M.H.; Zhou, F. Prevalence and associated factors of urinary incontinence in women living in China: A literature review. BMC Urol. 2020, 20, 159. [Google Scholar] [CrossRef] [PubMed]
- Townsend, M.K.; Curhan, G.C.; Resnick, N.M.; Grodstein, F. BMI, waist circumference, and incident urinary incontinence in older women. Obesity 2008, 16, 881–886. [Google Scholar] [CrossRef]
- Guedes-Aguiar, E.O.; de Sá-Caputo, D.D.C.; Moreira-Marconi, E.; de Macêdo Uchôa, S.M.; de Barros, P.Z.; Valentin, E.K.; Bergmann, A.; Taiar, R.; Bernardo-Filho, M. Effect of whole-body vibration exercise in the pelvic floor muscles of healthy and unhealthy individuals: A narrative review. Transl. Androl. Urol. 2019, 8, 395–404. [Google Scholar] [CrossRef]
- Huang, Y.C.; Chang, K.V. Kegel Exercises. In StatPearls; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2021. [Google Scholar]
- Duralde, E.R.; Rowen, T.S. Urinary Incontinence and Associated Female Sexual Dysfunction. Sex. Med. Rev. 2017, 5, 470–485. [Google Scholar] [CrossRef]
- Åström, Y.; Asklund, I.; Lindam, A.; Sjöström, M. Quality of life in women with urinary incontinence seeking care using e-health. BMC Women Health 2021, 21, 337. [Google Scholar] [CrossRef]
- Bunyavejchevin, S. The impact of overactive bladder, stress and mixed urinary incontinence on quality of life in Thai postmenopausal women. J. Med. Assoc. Thail. Chotmaihet Thangphaet 2006, 89, 294–298. [Google Scholar]
- Coyne, K.S.; Zhou, Z.; Thompson, C.; Versi, E. The impact on health-related quality of life of stress, urge and mixed urinary incontinence. BJU Int. 2003, 92, 731–735. [Google Scholar] [CrossRef]
- Basak, T.; Kok, G.; Guvenc, G. Prevalence, risk factors and quality of life in Turkish women with urinary incontinence: A synthesis of the literature. Int. Nurs. Rev. 2013, 60, 448–460. [Google Scholar] [CrossRef]
- Chu, C.M.; Arya, L.A.; Andy, U.U. Impact of urinary incontinence on female sexual health in women during midlife. Women Midlife Health 2015, 1, 6. [Google Scholar] [CrossRef] [Green Version]
- Ratner, E.S.; Erekson, E.A.; Minkin, M.J.; Foran-Tuller, K.A. Sexual satisfaction in the elderly female population: A special focus on women with gynecologic pathology. Maturitas 2011, 70, 210–215. [Google Scholar] [CrossRef] [Green Version]
- Stadnicka, G.; Łepecka-Klusek, C.; Pilewska-Kozak, A.; Jakiel, G. Psychosocial problems of women with stress urinary incontinence. Ann. Agric. Environ. Med. 2015, 22, 499–503. [Google Scholar] [CrossRef]
- Karbage, S.A.; Santos, Z.M.; Frota, M.A.; de Moura, H.J.; Vasconcelos, C.T.; Neto, J.A.; Bezerra, L.R. Quality of life of Brazilian women with urinary incontinence and the impact on their sexual function. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 201, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Lin, X.D.; Lin, N.; Ke, Z.B.; Xu, N.; Jiang, P.; Li, H. Effects of overactive bladder syndrome on female sexual function. Medicine 2021, 100, e25761. [Google Scholar] [CrossRef] [PubMed]
- Sacomori, C.; Cardoso, F.L. Predictors of improvement in sexual function of women with urinary incontinence after treatment with pelvic floor exercises: A secondary analysis. J. Sex. Med. 2015, 12, 746–755. [Google Scholar] [CrossRef] [PubMed]
- Preda, A.; Moreira, S. [Stress Urinary Incontinence and Female Sexual Dysfunction: The Role of Pelvic Floor Rehabilitation]. Acta Med. Port. 2019, 32, 721–726. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Group A | Group B | |||||
|---|---|---|---|---|---|---|
| Total (n) | SUI (n = 717/77.43%) | UUI (n = 18/1.94%) | MUI (n = 191/20.63%) | |||
| Mild | Moderate | Mild | Moderate | Mild | Moderate | |
| 926 | 652 (90.9%) | 65 (9.1%) | 3 (16.7%) | 15 (83.3%) | 21 (11.0%) | 170 (89%) |
| Group A (SUI) (n = 717) | Group B (UUI/MUI) (n = 209) | Z/χ2 | p | |
|---|---|---|---|---|
| Age (years) | 64 (62–68) | 66 (62–69) | −2.686 | 0.007 * a |
| Educational level | −0.198 | 0.843 a | ||
| Primary education or less | 224 (31.3%) | 68 (32.6%) | ||
| Secondary education | 424 (59.1%) | 120 (57.4%) | ||
| Tertiary education or above | 69 (9.6%) | 21 (10%) | ||
| Lifetime dominant occupation | −0.545 | 0.586 a | ||
| Mental activity | 115 (16%) | 37 (17.7%) | ||
| Grade I mild 1 | 182 (25.4%) | 46 (22%) | ||
| Grade II moderate 2 | 362 (50.5%) | 103 (49.3%) | ||
| Grade III heavy 3 | 56 (7.8%) | 23 (11%) | ||
| Grade IV extreme heavy 4 | 3 (0.3) | 0 (0%) | ||
| Height (cm) | 158 (155–161) | 158 (155–160) | −0.527 | 0.598 a |
| Weight (kg) | 62 (56–68)) | 63 (58.25–70.0) | −1.984 | 0.047 * a |
| BMI (kg/m2) | 24.7 (22.6–26.7) | 25.4 (23.00–27.5) | −2.397 | 0.017 * a |
| Waist circumference (cm) | 90 (85–97) | 93 (86–100) | −2.087 | 0.037 * a |
| Hip circumference (cm) | 100 (95–105) | 101 (97.0–106.5) | −1.590 | 0.112 a |
| Waist-to-hip ratio (WHR) | 0.9 (0.87–0.95) | 0.91 (0.88–0.95) | −1.077 | 0.281 a |
| Delivery mode | 2.451 | 0.294 b | ||
| VD | 655 (91.4%) | 186 (89%) | ||
| CS | 57 (7.9%) | 19 (9.1%) | ||
| Both | 5 (0.7%) | 4 (1.9%) | ||
| Delivery with episiotomy | 227 (31.7%) | 58 (27.8%) | 1.264 | 0.531 b |
| Parity | 5.379 | 0.020 * b | ||
| 0–2 | 550 (76.7%) | 176 (84.2%) | ||
| ≥3 | 167 (23.3%) | 33 (15.8%) | ||
| Maximum fetal weight (kg) | 3.20 (3.00–3.50) | 3.25 (3.00–3.60) | −1.462 | 0.144 a |
| Leakage of urine during pregnancy | 42 (5.9%) | 12 (5.7%) | 0.309 | 0.857 b |
| Leakage of urine postpartum | 61 (8.5%) | 18 (8.6%) | 0.013 | 0.993 b |
| Family history of UI | 66 (9.2%) | 29 (13.9%) | 3.835 | 0.147 b |
| Beverage preference | 142 (19.8%) | 33 (15.8%) | 1.702 | 0.192 b |
| Volume of liquid intake (24 h, mL) | 1.828 | 0.401 b | ||
| <1000 | 216 (30.1%) | 57 (27.3%) | ||
| 1000–2000 | 374 (52.2%) | 120 (57.4%) | ||
| >2000 | 127 (17.7%) | 32 (15.3%) | ||
| Menopausal age | 50 (48–53) | 50 (48–52) | −1.100 | 0.271 a |
| Menopause mode | 1.867 | 0.172 b | ||
| Nature | 680 (94.8%) | 193 (92.3%) | ||
| Surgery | 37 (5.2%) | 16 (7.7%) | ||
| Postmenopausal years | 14 (11–20) | 16 (12–21) | −2.863 | 0.004 * a |
| Comorbidities | ||||
| Chronic cough | 95 (13.2%) | 53 (25.4%) | 17.671 | <0.001 * b |
| Asthma | 30 (4.2%) | 15 (7.2%) | 3.135 | 0.077 b |
| Diabetes mellitus | 93 (13.0%) | 27 (12.9%) | 0.000 | 0.984 b |
| Constipation | 207 (28.9%) | 69 (33.0%) | 1.328 | 0.249 b |
| Depression | 12 (1.7%) | 4 (1.9%) | 0.000 | 1.000 b |
| Group A (SUI) (n = 717) | Group B (UUI/MUI) (n = 209) | Total | χ2 | p | |
|---|---|---|---|---|---|
| POP | 0.123 | 0.726 b | |||
| YES | 464 (64.7%) | 138 (66.0%) | 602 (65.0%) | ||
| NO | 253 (35.3%) | 71 (34.0%) | 324 (35.0%) | ||
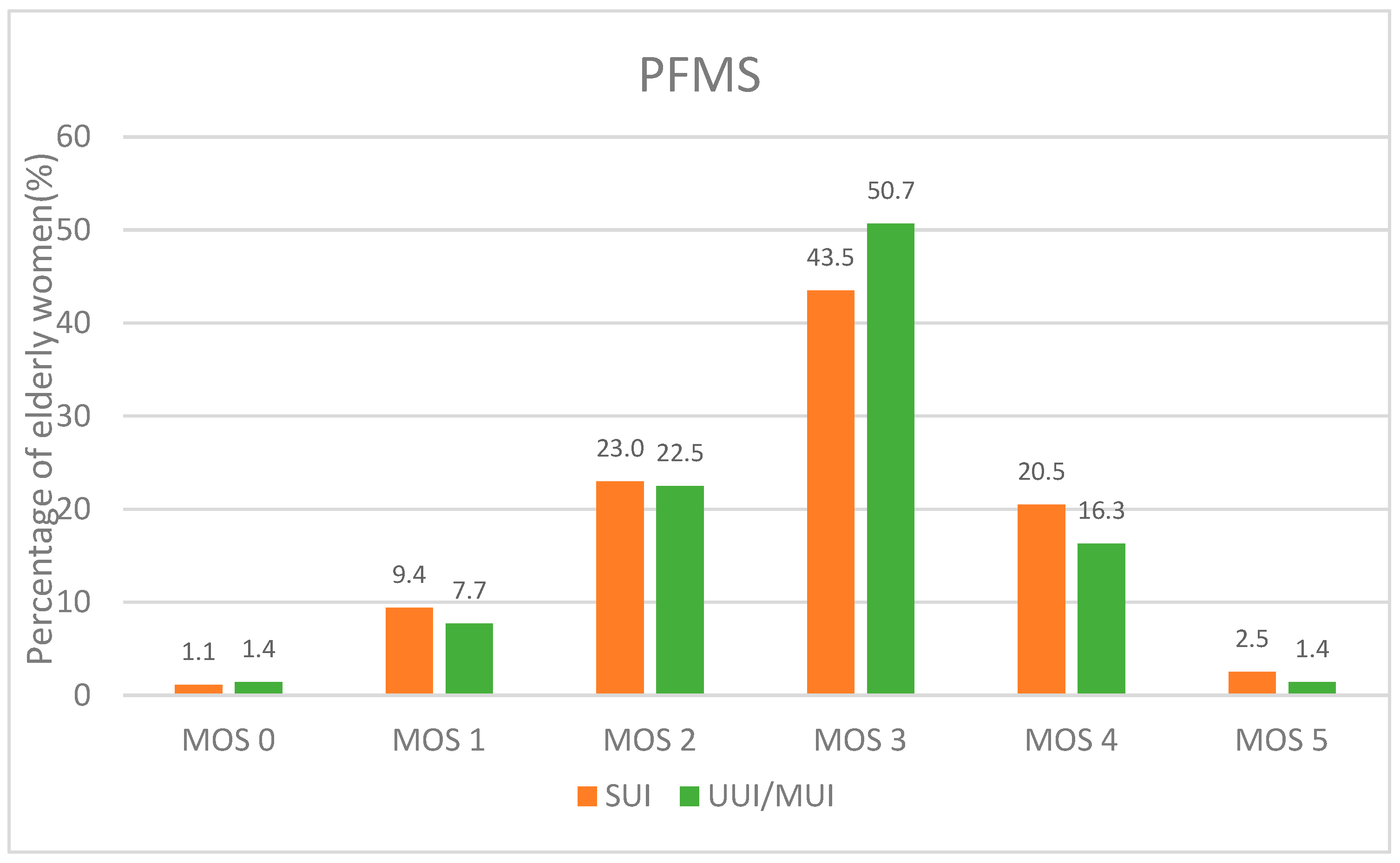
| PFMS | 2.675 | 0.102 b | |||
| Normal | 165 (23%) | 37 (17.7%) | 202 (21.8%) | ||
| Weakened | 552 (77%) | 172 (82.3%) | 724 (78.2%) |
| Group A (SUI) (n = 717) | Group B (UUI/MUI) (n = 209) | Total (n%) | Z/χ2 | p | |
|---|---|---|---|---|---|
| ICIQ-SF total score (0 to 21) | 5 (4–6) | 7 (5–10) | −8.618 | <0.001 * a | |
| Impact on QOL (0 to 10) | 2 (1–3) | 3 (1–5) | −5.425 | <0.001 * a | |
| (0) not at all | 112 (15.6%) | 17 (8.1%) | 129 (14.0%) | ||
| (1–3) mild | 470 (65.6%) | 112 (53.6%) | 582 (62.8%) | ||
| (4–6) moderate | 113 (15.8%) | 68 (32.5%) | 181 (19.5%) | ||
| (7–9) severe | 16 (2.2%) | 10 (4.8%) | 26 (2.8%) | ||
| (10) extensive | 6 (0.8%) | 2 (1.0%) | 8 (0.9%) |
| Group A (SUI) (n = 717) | Group B (UUI/MUI) (n = 209) | Total (n%) | Z/χ2 | p | |
|---|---|---|---|---|---|
| Active sex life | 4.105 | 0.043 * b | |||
| Yes | 231 (32.2%) | 52 (24.9%) | 283 (30.6%) | ||
| No | 486 (67.8%) | 157 (75.1%) | 643 (69.4%) | ||
| Degree of satisfaction with active sex life | −1.958 | 0.050 a | |||
| Very satisfied | 69/231 (29.9%) | 8/52 (15.4%) | 77/283 (27.2%) | ||
| Satisfied | 144/231 (62.3%) | 39/52 (75.0%) | 183/283 (64.7%) | ||
| Unsatisfied | 18/231 (7.8%) | 5/52 (9.6%) | 23/283 (8.1%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, D.; Wang, S.; Gao, L.; Jia, Y.; Wang, H.; Sun, X.; Wang, J. Analysis of Characteristics and Quality of Life of Elderly Women with Mild to Moderate Urinary Incontinence in Community Dwellings. Int. J. Environ. Res. Public Health 2022, 19, 5609. https://doi.org/10.3390/ijerph19095609
Zhang D, Wang S, Gao L, Jia Y, Wang H, Sun X, Wang J. Analysis of Characteristics and Quality of Life of Elderly Women with Mild to Moderate Urinary Incontinence in Community Dwellings. International Journal of Environmental Research and Public Health. 2022; 19(9):5609. https://doi.org/10.3390/ijerph19095609
Chicago/Turabian StyleZhang, Di, Shiyan Wang, Lei Gao, Yuanyuan Jia, Haibo Wang, Xiuli Sun, and Jianliu Wang. 2022. "Analysis of Characteristics and Quality of Life of Elderly Women with Mild to Moderate Urinary Incontinence in Community Dwellings" International Journal of Environmental Research and Public Health 19, no. 9: 5609. https://doi.org/10.3390/ijerph19095609
APA StyleZhang, D., Wang, S., Gao, L., Jia, Y., Wang, H., Sun, X., & Wang, J. (2022). Analysis of Characteristics and Quality of Life of Elderly Women with Mild to Moderate Urinary Incontinence in Community Dwellings. International Journal of Environmental Research and Public Health, 19(9), 5609. https://doi.org/10.3390/ijerph19095609