
Mindfulness-Based Intervention for Caregivers of Frail Older Chinese Adults: A Study Protocol

 , , , and
, , , and 
Abstract
:1. Introduction
1.1. Burden of Family Caregivers of Frail Elders in an Ageing Society
1.2. Intervention for Managing Caregiver Burden of Frail Older Adults
1.3. A Call for Model for Intergenerational Caregiving
1.4. Outcomes and Mediators of Intergenerational Caregiving
1.5. Research Questions and Hypotheses of the Study
2. Materials and Methods
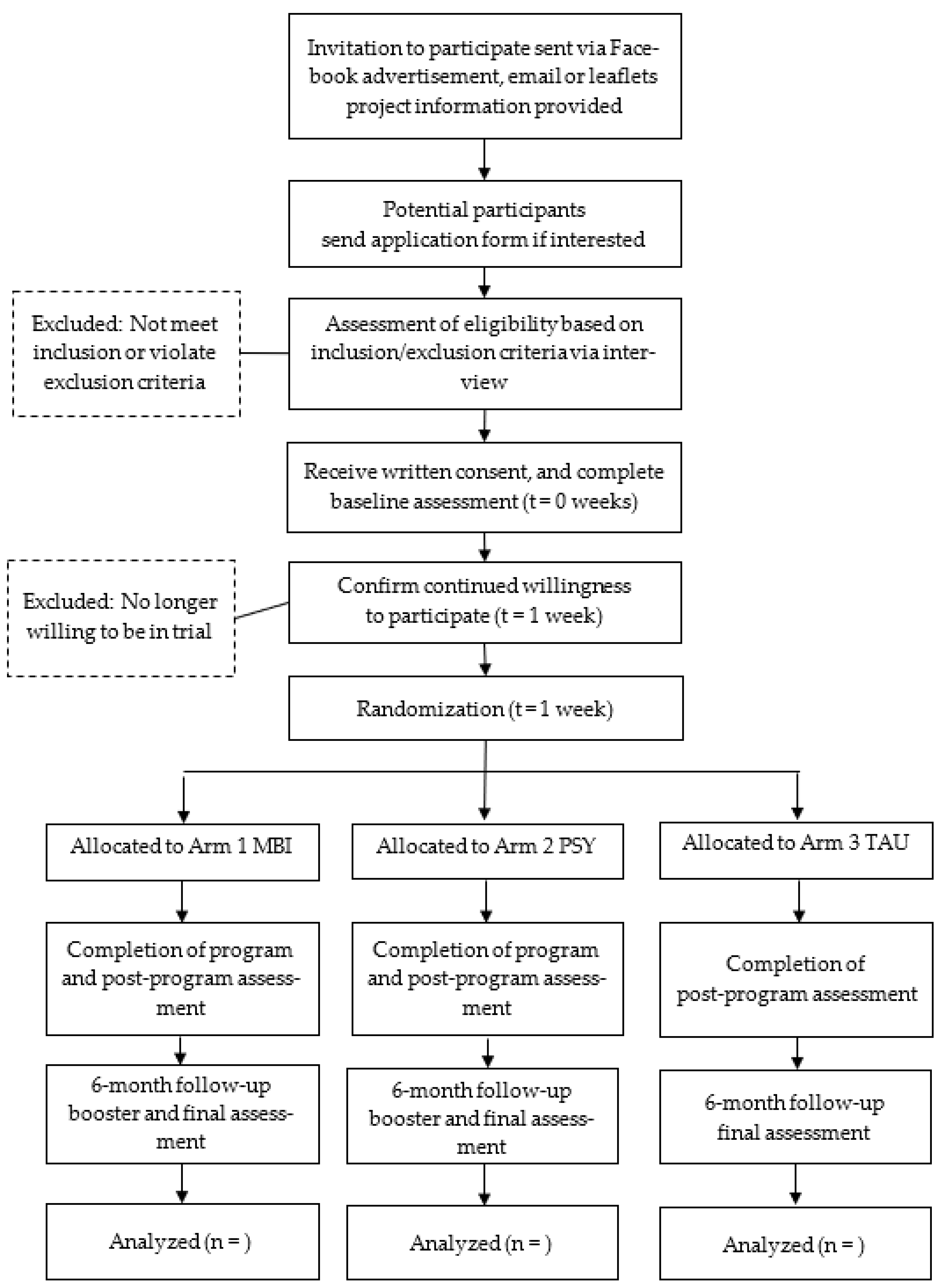
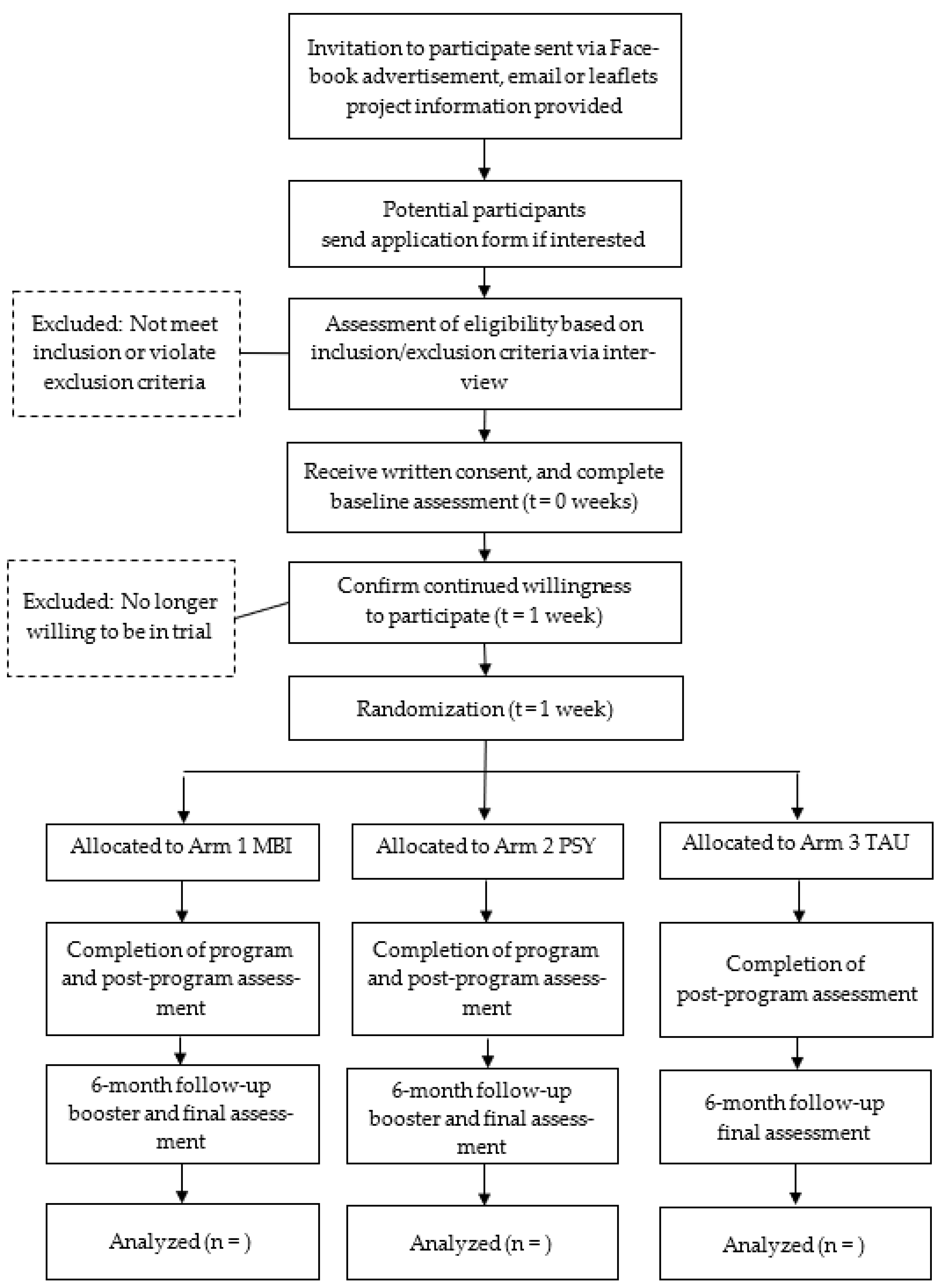
2.1. Study Design
2.1.1. Refinement of Design from a Pilot Study
2.1.2. Sample Size Estimation
2.1.3. Recruitment of Participants
2.1.4. Randomization
2.2. Proceudres and Intervention
2.3. Measures
2.3.1. Outcome Measures
2.3.2. Measures for Mediating Variables
2.3.3. Program Fidelity
2.4. Data Analyses
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rockwood, K.; Song, X.; Mitnitski, A. Changes in Relative Fitness and Frailty across the Adult Lifespan: Evidence from the Canadian National Population Health Survey. CMAJ 2011, 183, E487–E494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in Elderly People. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [Green Version]
- Kulmala, J.; Nykänen, I.; Mänty, M.; Hartikainen, S. Association between Frailty and Dementia: A Population-Based Study. Gerontology 2014, 60, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Census and Statistics Department. Census and Statistics Department Persons with Disabilities and Chronic Diseases in Hong Kong; Hong Kong Monthly Digest of Statistics: Hong Kong, China, 2015. [Google Scholar]
- Gaugler, J.E.; Reese, M.; Mittelman, M.S. The Effects of a Comprehensive Psychosocial Intervention on Secondary Stressors and Social Support for Adult Child Caregivers of Persons with Dementia. Innov. Aging 2018, 2, igy015. [Google Scholar] [CrossRef] [Green Version]
- Ho, S.C.; Chan, A.; Woo, J.; Chong, P.; Sham, A. Impact of Caregiving on Health and Quality of Life: A Comparative Population-Based Study of Caregivers for Elderly Persons and Noncaregivers. J. Gerontol. A Biol. Sci. Med. Sci. 2009, 64A, 873–879. [Google Scholar] [CrossRef]
- Mello, J.D.A.; Macq, J.; Van Durme, T.; Cès, S.; Spruytte, N.; Van Audenhove, C.; Declercq, A. The Determinants of Informal Caregivers’ Burden in the Care of Frail Older Persons: A Dynamic and Role-Related Perspective. Aging Ment. Health 2017, 21, 838–843. [Google Scholar] [CrossRef] [Green Version]
- Cooper, C.; Selwood, A.; Blanchard, M.; Walker, Z.; Blizard, R.; Livingston, G. The Determinants of Family Carers’ Abusive Behaviour to People with Dementia: Results of the CARD Study. J. Affect. Disord. 2010, 121, 136–142. [Google Scholar] [CrossRef]
- Carretero, S.; Garcés, J.; Ródenas, F.; Sanjosé, V. The Informal Caregiver’s Burden of Dependent People: Theory and Empirical Review. Arch. Gerontol. Geriatr. 2009, 49, 74–79. [Google Scholar] [CrossRef] [Green Version]
- Folkman, S.; Lazarus, R.S. An Analysis of Coping in a Middle-Aged Community Sample. J. Health Soc. Behav. 1980, 21, 219. [Google Scholar] [CrossRef]
- Di Mattei, V.E.; Prunas, A.; Novella, L.; Marcone, A.; Cappa, S.F.; Sarno, L. The Burden of Distress in Caregivers of Elderly Demented Patients and Its Relationship with Coping Strategies. Neurol. Sci. 2008, 29, 383–389. [Google Scholar] [CrossRef] [Green Version]
- Iavarone, A.; Ziello, A.R.; Pastore, F.; Fasanaro, A.M.; Poderico, C. Caregiver Burden and Coping Strategies in Caregivers of Patients with Alzheimer’s Disease. NDT 2014, 10, 1407. [Google Scholar] [CrossRef] [Green Version]
- Cooper, C.; Katona, C.; Orrell, M.; Livingston, G. Coping Strategies, Anxiety and Depression in Caregivers of People with Alzheimer’s Disease. Int. J. Geriat. Psychiatry 2008, 23, 929–936. [Google Scholar] [CrossRef]
- Snyder, C.M.; Fauth, E.; Wanzek, J.; Piercy, K.W.; Norton, M.C.; Corcoran, C.; Rabins, P.V.; Lyketsos, C.G.; Tschanz, J.T. Dementia Caregivers’ Coping Strategies and Their Relationship to Health and Well-Being: The Cache County Study. Aging Ment. Health 2015, 19, 390–399. [Google Scholar] [CrossRef] [Green Version]
- Zarit, S.H.; Todd, P.A.; Zarit, J.M. Subjective Burden of Husbands and Wives as Caregivers: A Longitudinal Study. Gerontologist 1986, 26, 260–266. [Google Scholar] [CrossRef]
- Zarit, S.H.; Zarit, J.M. Family caregiving. In Psychology and Geriatrics: Integrated Care for an Aging Population, 1st ed.; Bensadon, B.A., Ed.; Elsevier Science & Technology: Saint Louis, MO, USA, 2015; pp. 21–43. ISBN 978-0-12-420123-1. [Google Scholar]
- Elvish, R.; Lever, S.-J.; Johnstone, J.; Cawley, R.; Keady, J. Psychological Interventions for Carers of People with Dementia: A Systematic Review of Quantitative and Qualitative Evidence. Couns. Psychother. Res. 2013, 13, 106–125. [Google Scholar] [CrossRef]
- Selwood, A.; Johnston, K.; Katona, C.; Lyketsos, C.; Livingston, G. Systematic Review of the Effect of Psychological Interventions on Family Caregivers of People with Dementia. J. Affect. Disord. 2007, 101, 75–89. [Google Scholar] [CrossRef]
- Bohlmeijer, E.; Prenger, R.; Taal, E.; Cuijpers, P. The Effects of Mindfulness-Based Stress Reduction Therapy on Mental Health of Adults with a Chronic Medical Disease: A Meta-Analysis. J. Psychosom. Res. 2010, 68, 539–544. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Full Catastrophe Living: Using the Wisdom of Your Body and Mind to Face Stress, Pain, and Illness, revised ed.; Bantam Books: New York, NY, USA, 2013; p. 145. ISBN 978-0-345-53972-4. [Google Scholar]
- Segal, Z.V.; Williams, J.M.G.; Teasdale, J.D. Mindfulness-Based Cognitive Therapy for Depression, 2nd ed.; Guilford Press: New York, NY, USA, 2013; ISBN 978-1-4625-0750-4. [Google Scholar]
- Collins, R.N.; Kishita, N. The Effectiveness of Mindfulness- and Acceptance-Based Interventions for Informal Caregivers of People with Dementia: A Meta-Analysis. Gerontologist 2019, 59, e363–e379. [Google Scholar] [CrossRef] [Green Version]
- Brown, K.W.; Coogle, C.L.; Wegelin, J. A Pilot Randomized Controlled Trial of Mindfulness-Based Stress Reduction for Caregivers of Family Members with Dementia. Aging Ment. Health 2016, 20, 1157–1166. [Google Scholar] [CrossRef]
- Whitebird, R.R.; Kreitzer, M.; Crain, A.L.; Lewis, B.A.; Hanson, L.R.; Enstad, C.J. Mindfulness-Based Stress Reduction for Family Caregivers: A Randomized Controlled Trial. Gerontologist 2013, 53, 676–686. [Google Scholar] [CrossRef]
- Hou, R.J.; Wong, S.Y.-S.; Yip, B.H.-K.; Hung, A.T.F.; Lo, H.H.-M.; Chan, P.H.S.; Lo, C.S.L.; Kwok, T.C.-Y.; Tang, W.K.; Mak, W.W.S.; et al. The Effects of Mindfulness-Based Stress Reduction Program on the Mental Health of Family Caregivers: A Randomized Controlled Trial. Psychother. Psychosom. 2014, 83, 45–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oken, B.S.; Fonareva, I.; Haas, M.; Wahbeh, H.; Lane, J.B.; Zajdel, D.; Amen, A. Pilot Controlled Trial of Mindfulness Meditation and Education for Dementia Caregivers. J. Altern. Complement. Med. 2010, 16, 1031–1038. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping, 11th ed.; Springer: New York, NY, USA, 1984; ISBN 978-0-8261-4191-0. [Google Scholar]
- Skinner, E.A.; Edge, K.; Altman, J.; Sherwood, H. Searching for the Structure of Coping: A Review and Critique of Category Systems for Classifying Ways of Coping. Psychol. Bull. 2003, 129, 216–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, K.N.S.; Chan, C.S.; Ng, J.; Yip, C.-H. Action Type-Based Factorial Structure of Brief COPE among Hong Kong Chinese. J. Psychopathol. Behav. Assess. 2016, 38, 631–644. [Google Scholar] [CrossRef]
- Pinquart, M.; Sörensen, S. Helping Caregivers of Persons with Dementia: Which Interventions Work and How Large Are Their Effects? Int. Psychogeriatr. 2006, 18, 577–595. [Google Scholar] [CrossRef]
- Gilhooly, K.J.; Gilhooly, M.L.M.; Sullivan, M.P.; McIntyre, A.; Wilson, L.; Harding, E.; Woodbridge, R.; Crutch, S. A Meta-Review of Stress, Coping and Interventions in Dementia and Dementia Caregiving. BMC Geriatr. 2016, 16, 106. [Google Scholar] [CrossRef] [Green Version]
- Li, R.; Cooper, C.; Bradley, J.; Shulman, A.; Livingston, G. Coping Strategies and Psychological Morbidity in Family Careers of People with Dementia: A Systematic Review and Meta-Analysis. J. Affect. Disord. 2012, 139, 1–11. [Google Scholar] [CrossRef]
- Au, A.; Li, S.; Lee, K.; Leung, P.; Pan, P.-C.; Thompson, L.; Gallagher-Thompson, D. The Coping with Caregiving Group Program for Chinese Caregivers of Patients with Alzheimer’s Disease in Hong Kong. Patient. Educ. Couns. 2010, 78, 256–260. [Google Scholar] [CrossRef]
- Li, R.; Cooper, C.; Austin, A.; Livingston, G. Do Changes in Coping Style Explain the Effectiveness of Interventions for Psychological Morbidity in Family Carers of People with Dementia? A Systematic Review and Meta-Analysis. Int. Psychogeriatr. 2013, 25, 204–214. [Google Scholar] [CrossRef]
- Li, R.; Cooper, C.; Barber, J.; Rapaport, P.; Griffin, M.; Livingston, G. Coping Strategies as Mediators of the Effect of the START (Strategies for RelaTives) Intervention on Psychological Morbidity for Family Carers of People with Dementia in a Randomised Controlled Trial. J. Affect. Disord. 2014, 168, 298–305. [Google Scholar] [CrossRef]
- Tacón, A.M.; McComb, J.; Caldera, Y.; Randolph, P. Mindfulness Meditation, Anxiety Reduction, and Heart Disease: A Pilot Study. Fam. Community Health 2003, 26, 25–33. [Google Scholar] [CrossRef]
- Halland, E.; de Vibe, M.; Solhaug, I.; Friborg, O.; Rosenvinge, J.H.; Tyssen, R.; Sørlie, T.; Bjørndal, A. Mindfulness Training Improves Problem-Focused Coping in Psychology and Medical Students: Results from a Randomized Controlled Trial. Coll. Stud. J. 2015, 49, 387–398. [Google Scholar]
- Park, H.; Oh, S.; Noh, Y.; Kim, J.Y.; Kim, J.-H. Heart Rate Variability as a Marker of Distress and Recovery: The Effect of Brief Supportive Expressive Group Therapy with Mindfulness in Cancer Patients. Integr. Cancer Ther. 2018, 17, 825–831. [Google Scholar] [CrossRef] [Green Version]
- Gillions, A.; Cheang, R.; Duarte, R. The Effect of Mindfulness Practice on Aggression and Violence Levels in Adults: A Systematic Review. Aggress. Violent Behav. 2019, 48, 104–115. [Google Scholar] [CrossRef]
- Livingston, G.; Barber, J.; Rapaport, P.; Knapp, M.; Griffin, M.; Romeo, R.; King, D.; Livingston, D.; Lewis-Holmes, E.; Mummery, C.; et al. START (STrAtegies for RelaTives) Study: A Pragmatic Randomised Controlled Trial to Determine the Clinical Effectiveness and Cost-Effectiveness of a Manual-Based Coping Strategy Programme in Promoting the Mental Health of Carers of People with Dementia. Health Technol. Assess. 2014, 18, 1–242. [Google Scholar] [CrossRef] [Green Version]
- Peterman, A.H.; Fitchett, G.; Brady, M.J.; Hernandez, L.; Cella, D. Measuring Spiritual Well-Being in People with Cancer: The Functional Assessment of Chronic Illness Therapy—Spiritual Well-Being Scale (FACIT-Sp). Ann. Behav. Med. 2002, 24, 49–58. [Google Scholar] [CrossRef]
- Garland, S.N.; Carlson, L.E.; Cook, S.; Lansdell, L.; Speca, M. A Non-Randomized Comparison of Mindfulness-Based Stress Reduction and Healing Arts Programs for Facilitating Post-Traumatic Growth and Spirituality in Cancer Outpatients. Support. Care Cancer 2007, 15, 949–961. [Google Scholar] [CrossRef]
- Hayes, S.C.; Strosahl, K.; Wilson, K.G. Acceptance and Commitment Therapy: The Process and Practice of Mindful Change, 2nd ed.; Guilford Press: New York, NY, USA, 2012; ISBN 978-1-60918-962-4. [Google Scholar]
- Cheng, S.-T.; Au, A.; Losada, A.; Thompson, L.W.; Gallagher-Thompson, D. Psychological Interventions for Dementia Caregivers: What We Have Achieved, What We Have Learned. Curr. Psychiatry Rep. 2019, 21, 59. [Google Scholar] [CrossRef] [Green Version]
- Baron, G.; Perrodeau, E.; Boutron, I.; Ravaud, P. Reporting of Analyses from Randomized Controlled Trials with Multiple Arms: A Systematic Review. BMC Med. 2013, 11, 84. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates Inc.: Hillsdale, NJ, USA, 1988; ISBN 978-0-8058-0283-2. [Google Scholar]
- Lo, H.H.M.; Ng, S.M.; Chan, C.L.W. Evaluating Compassion–Mindfulness Therapy for Recurrent Anxiety and Depression: A Randomized Control Trial. Res. Soc. Work Pract. 2015, 25, 715–725. [Google Scholar] [CrossRef] [Green Version]
- Lo, H.H.M.; Chan, S.K.C.; Szeto, M.P.; Chan, C.Y.H.; Choi, C.W. A Feasibility Study of a Brief Mindfulness-Based Program for Parents of Preschool Children with Developmental Disabilities. Mindfulness 2017, 8, 1665–1673. [Google Scholar] [CrossRef]
- Lo, H.H.M.; Wong, S.W.L.; Wong, J.Y.H.; Yeung, J.W.K.; Snel, E.; Wong, S.Y.S. The Effects of Family-Based Mindfulness Intervention in ADHD Symptomology in Young Children and their Parents: A Randomized Control Trial. J. Atten. Disord. 2020, 24, 667–680. [Google Scholar] [CrossRef] [Green Version]
- Fritz, M.S.; MacKinnon, D.P. Required Sample Size to Detect the Mediated Effect. Psychol. Sci. 2007, 18, 233–239. [Google Scholar] [CrossRef] [Green Version]
- Rockwood, K. A Global Clinical Measure of Fitness and Frailty in Elderly People. CMAJ 2005, 173, 489–495. [Google Scholar] [CrossRef] [Green Version]
- Bédard, M.; Molloy, D.W.; Squire, L.; Dubois, S.; Lever, J.A.; O’Donnell, M. The Zarit Burden Interview: A new short version and screening version. Gerontologist 2001, 41, 652–657. [Google Scholar] [CrossRef] [Green Version]
- Hughes, C.P.; Berg, L.; Danziger, W.; Coben, L.A.; Martin, R.L. A New Clinical Scale for the Staging of Dementia. Br. J. Psychiatry 1982, 140, 566–572. [Google Scholar] [CrossRef]
- Crane, R.S.; Eames, C.; Kuyken, W.; Hastings, R.P.; Williams, J.M.G.; Bartley, T.; Evans, A.; Silverton, S.; Soulsby, J.G.; Surawy, C. Development and validation of the mindfulness-based interventions–teaching assessment criteria (MBI: TAC). Assessment 2013, 20, 681–688. [Google Scholar] [CrossRef]
- Radloff, L.S. The CES-D Scale: A Self-Report Depression Scale for Research in the General Population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Boey, K.W. Cross-Validation of a Short Form of the CES-D in Chinese Elderly. Int. J. Geriat. Psychiatry 1999, 14, 608–617. [Google Scholar] [CrossRef]
- Zarit, S.H.; Reever, K.E.; Bach-Peterson, J. Relatives of the Impaired Elderly: Correlates of Feelings of Burden. Gerontologist 1980, 20, 649–655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, B.; Yu, Y.; Liu, Z.; Lin, M.; Chen, Y.; Zhao, M.; Xiao, S. Factor Analyses of the Chinese Zarit Burden Interview among Caregivers of Patients with Schizophrenia in a Rural Chinese Community. BMJ Open 2017, 7, e015621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta. Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leung, C.M.; Wing, Y.K.; Kwong, P.K.; Shum, A.L.K. Validation of the Chinese-Cantonese Version of the Hospital Anxiety and Depression Scale and Comparison with the Hamilton Rating Scale of Depression. Acta Psychiatr. Scand. 1999, 100, 456–461. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.F.; Yang, S.H.; Koo, M. Psychometric Properties of the Chinese Version of Spiritual Index of Well-Being in Elderly Taiwanese. BMC Geriatr. 2017, 17, 3. [Google Scholar] [CrossRef] [Green Version]
- Smilkstein, G.; Ashworth, C.; Montano, D. Validity and Reliability of the Family APGAR as a Test of Family Function. J. Fam. Pract. 1982, 15, 303–311. [Google Scholar]
- Lo, H.H.M. Quality of life among adolescents in Hong Kong: General and gender-specific effects of self-efficacy and mindfulness. Appl. Res. Qual. Life 2021, 16, 2311–2334. [Google Scholar] [CrossRef]
- Straus, M.A.; Hamby, S.L.; Boney-McCoy, S.; Sugarman, D.B. The Revised Conflict Tactics Scales (CTS2): Development and Preliminary Psychometric Data. J. Fam. Issues 1996, 17, 283–316. [Google Scholar] [CrossRef]
- Yan, E.; Tang, C.S.-K. Prevalence and Psychological Impact of Chinese Elder Abuse. J. Interpers. Violence 2001, 16, 1158–1174. [Google Scholar] [CrossRef]
- Task Force of the European Society of Cardiology the North American Society of Pacing Electrophysiology. Heart Rate Variability: Standards of Measurement, Physiological Interpretation, and Clinical Use. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef] [Green Version]
- Carver, C.S. You Want to Measure Coping but Your Protocol’ Too Long: Consider the Brief Cope. Int. J. Behav. Med. 1997, 4, 92–100. [Google Scholar] [CrossRef]
- Leung, D.Y.P.; Chan, H.Y.L.; Chan, C.W.H.; Kwan, J.S.K.; Yau, S.Z.M.; Chiu, P.K.C.; Lo, R.S.K.; Lee, L.L.Y. Psychometric Properties of the Caregiver Inventory for Measuring Caregiving Self-Efficacy of Caregivers of Patients with Palliative Care Needs. Neuropsychiatry 2017, 7, 872–879. [Google Scholar] [CrossRef]
- Merluzzi, T.V.; Philip, E.J.; Vachon, D.O.; Heitzmann, C.A. Assessment of Self-Efficacy for Caregiving: The Critical Role of Self-Care in Caregiver Stress and Burden. Pall. Supp. Care 2011, 9, 15–24. [Google Scholar] [CrossRef]
- Gámez, W.; Chmielewski, M.; Kotov, R.; Ruggero, C.; Watson, D. Development of a Measure of Experiential Avoidance: The Multidimensional Experiential Avoidance Questionnaire. Psychol. Assess. 2011, 23, 692–713. [Google Scholar] [CrossRef]
- Lo, H.H.M.; Powell, C.L.Y.M.; Chan, S.H.W.; Tsang, E.Y.K.; Leung, S.S.M.; Leung, B.F.H. Developing and validating the Brief Experiential Avoidance Questionnaire in Hong Kong Chinese. 2022; in review. [Google Scholar]
- Schulz, K.; Altman, D.G.; Moher, D.; for the CONSORT Group. CONSORT 2010 statement: Updated Guidelines for Reporting Parallel Group Randomized Trials. Ann. Intern. Med. 2010, 152, 726–732. [Google Scholar] [CrossRef] [Green Version]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Press: New York, NY, USA, 2018; ISBN 978-1-4625-3467-8. [Google Scholar]

{kind=link}
| Mindfulness-Based Intervention (Arm 1) | Psychoeducation (Arm 2) |
|---|---|
Session 1 Stepping out from automatic pilot
| Session 1 Stress of caregivers
|
Session 2 Reaction vs. responding to older adults
| Session 2 Making a behavior plan
|
Session 3: Challenges in caregiving
| Session 3 Communicating with older adults
|
Session 4: Self-care and care of others
| Session 4 Self-care and care of others
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lo, H.H.M.; Au, A.; Cho, W.V.; Lau, E.N.S.; Wong, J.Y.H.; Wong, S.Y.S.; Yeung, J.W.K. Mindfulness-Based Intervention for Caregivers of Frail Older Chinese Adults: A Study Protocol. Int. J. Environ. Res. Public Health 2022, 19, 5447. https://doi.org/10.3390/ijerph19095447
Lo HHM, Au A, Cho WV, Lau ENS, Wong JYH, Wong SYS, Yeung JWK. Mindfulness-Based Intervention for Caregivers of Frail Older Chinese Adults: A Study Protocol. International Journal of Environmental Research and Public Health. 2022; 19(9):5447. https://doi.org/10.3390/ijerph19095447
Chicago/Turabian StyleLo, Herman H. M., Alma Au, W. V. Cho, Elsa N. S. Lau, Janet Y. H. Wong, Samuel Y. S. Wong, and Jerf W. K. Yeung. 2022. "Mindfulness-Based Intervention for Caregivers of Frail Older Chinese Adults: A Study Protocol" International Journal of Environmental Research and Public Health 19, no. 9: 5447. https://doi.org/10.3390/ijerph19095447
APA StyleLo, H. H. M., Au, A., Cho, W. V., Lau, E. N. S., Wong, J. Y. H., Wong, S. Y. S., & Yeung, J. W. K. (2022). Mindfulness-Based Intervention for Caregivers of Frail Older Chinese Adults: A Study Protocol. International Journal of Environmental Research and Public Health, 19(9), 5447. https://doi.org/10.3390/ijerph19095447