
The Prognostic Role of miR-31 in Head and Neck Squamous Cell Carcinoma: Systematic Review and Meta-Analysis with Trial Sequential Analysis

 ,
,  ,
,  ,
,  ,
,  , ,
, ,  , , ,
, , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol
2.2. Eligibility Criteria
2.3. Sources of Information, Research, and Selection
2.4. Data Collection Process, Data Characteristics
2.5. Risk of Bias in Individual Studies, Summary Measures, Summary of Results, Risk of Bias between Studies, Additional Measures
3. Results
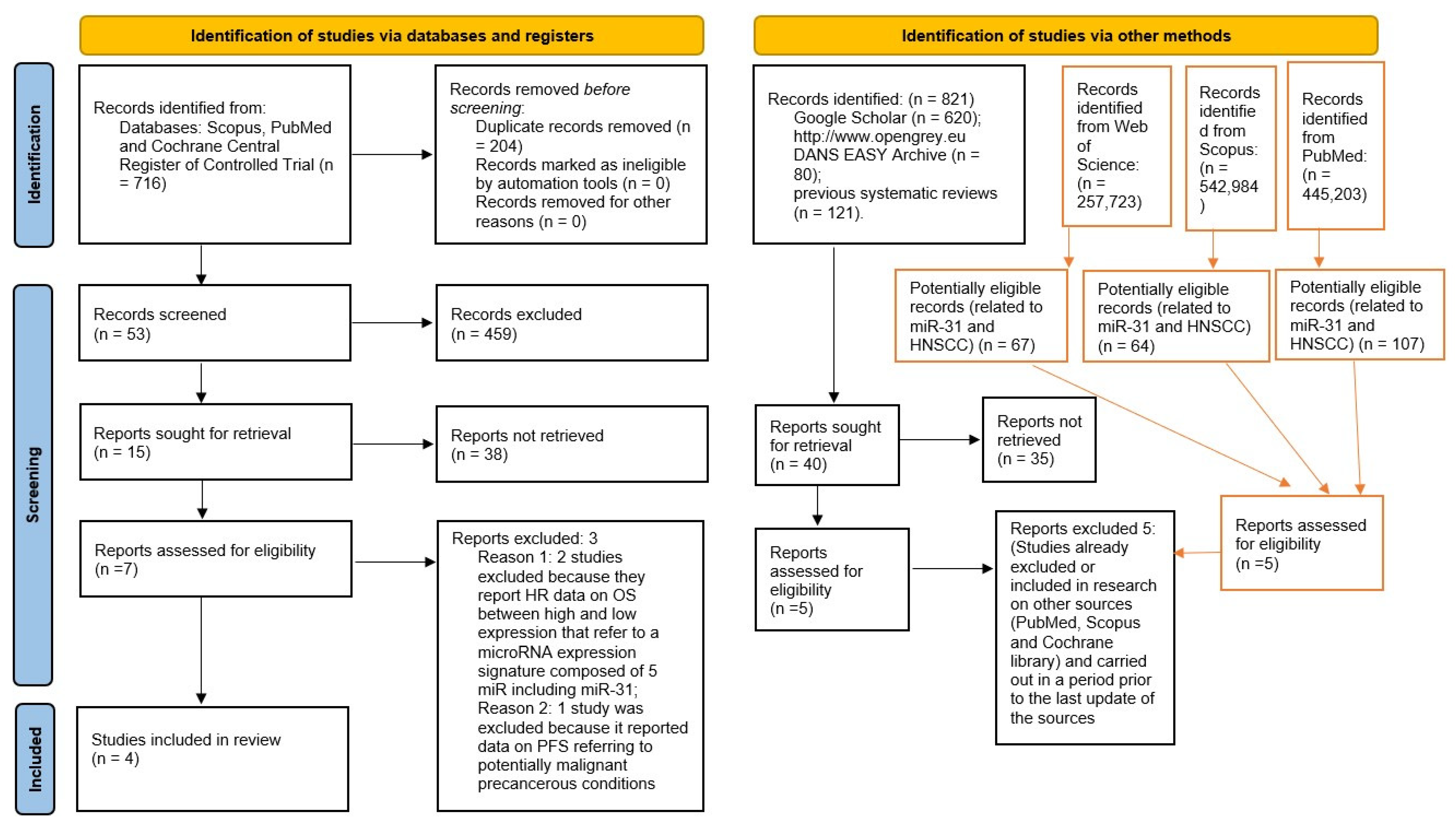
3.1. Selection of Studies
3.2. Data Characteristics
3.3. Risk of Bias in Studies
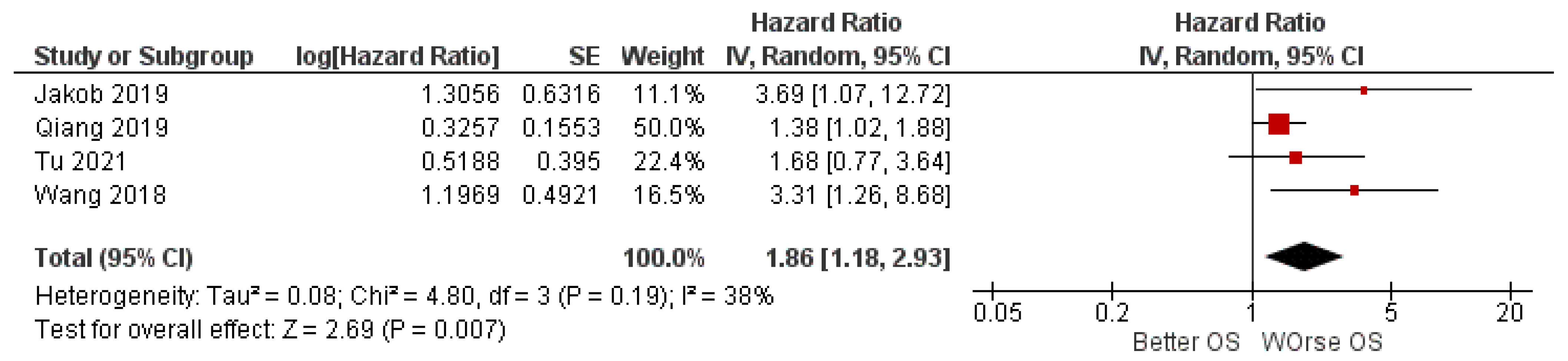
3.4. Meta-Analysis
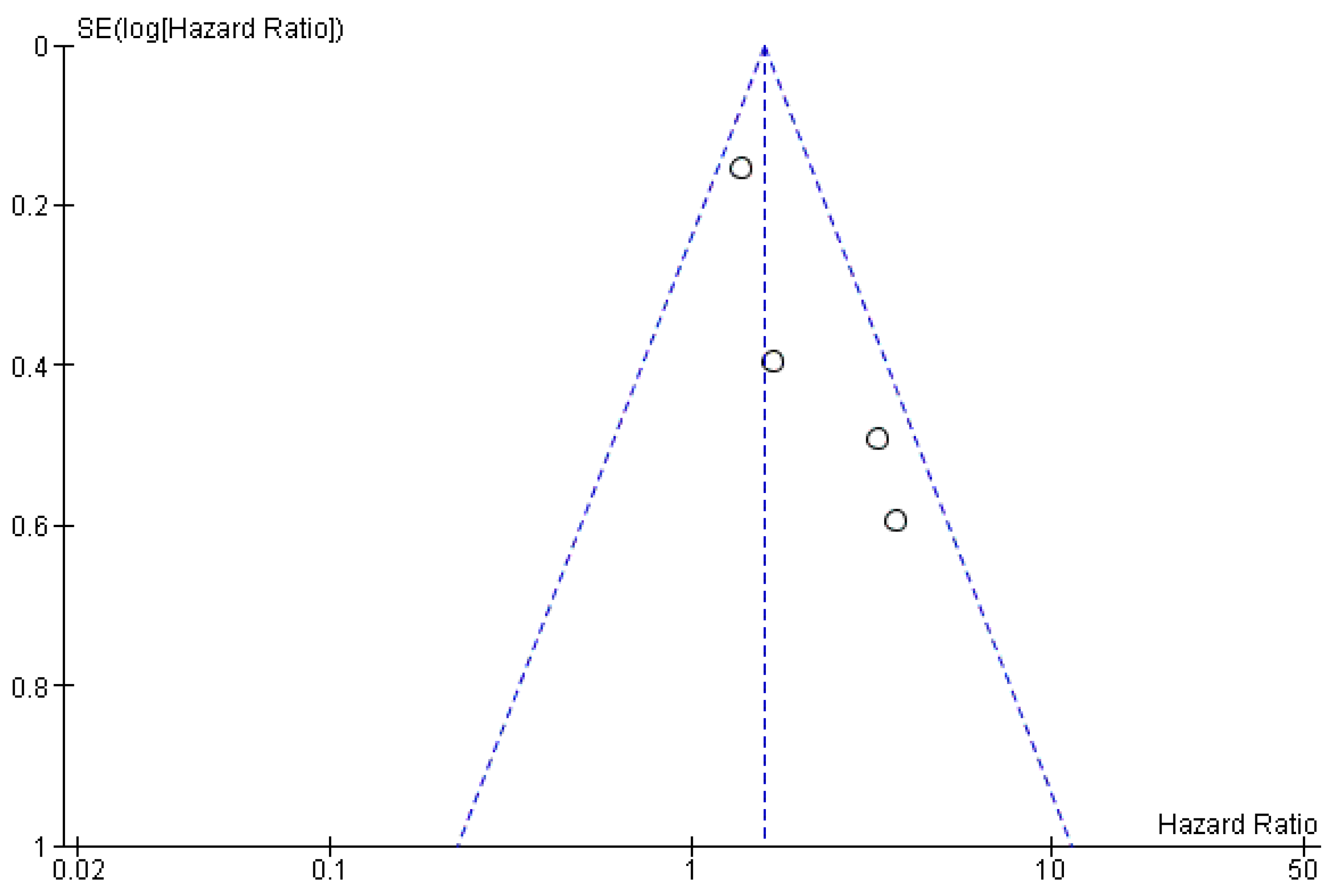
3.5. Risk of Bias across Study
3.6. Trial Sequential Analysis, Grade
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 2019, 144, 1941–1953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farhat, M.C.; Dyalram, D.; Ord, R.A.; Lubek, J.E. Oral squamous cell carcinoma in patients aged 45 and younger: Prognosis, survival, and quality of life. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2021, 133, 518–525. [Google Scholar] [CrossRef] [PubMed]
- Berglund, A.; Muenyi, C.; Siegel, E.M.; Ajidahun, A.; Eschrich, S.A.; Wong, D.; Hendrick, L.E.; Putney, R.M.; Kim, S.; Hayes, D.N.; et al. Characterization of epigenomic alterations in HPV16+ head and neck squamous cell carcinomas. Cancer Epidemiol. Biomark. Prev. 2022, 31, 858–869. [Google Scholar] [CrossRef] [PubMed]
- Muzio, L.L.; Ballini, A.; Cantore, S.; Bottalico, L.; Charitos, I.A.; Ambrosino, M.; Nocini, R.; Malcangi, A.; Dioguardi, M.; Cazzolla, A.P.; et al. Overview of Candida albicans and Human Papillomavirus (HPV) Infection Agents and their Biomolecular Mechanisms in Promoting Oral Cancer in Pediatric Patients. Biomed Res. Int. 2021, 2021, 7312611. [Google Scholar] [CrossRef]
- Wang, J.; Tian, Y.; Huang, H.; Huang, D.; Liu, Y.; Tian, Y.; Zhu, G.; Zhang, X.; Ferris, R.L. The prognosis of HPV-associated metastatic pharyngeal patients by primary and distant site. Oral Oncol. 2021, 125, 105675. [Google Scholar] [CrossRef]
- Martens, R.M.; Koopman, T.; Lavini, C.; Brug, T.V.; Zwezerijnen, G.J.C.; Marcus, J.T.; Vergeer, M.R.; Leemans, C.R.; Bree, R.; Graaf, P.; et al. Early Response Prediction of Multiparametric Functional MRI and (18) F-FDG-PET in Patients with Head and Neck Squamous Cell Carcinoma Treated with (Chemo) Radiation. Cancers 2022, 14, 216. [Google Scholar] [CrossRef]
- Shinohara, S.; Kikuchi, M.; Harada, H.; Hamaguchi, K.; Asato, R.; Tamaki, H.; Mizuta, M.; Hori, R.; Kojima, T.; Honda, K.; et al. Clinicopathological Characteristics and Survival Outcomes of Patients with Buccal Squamous Cell Carcinoma: Results of a Multi-Institutional Study. Medicina 2021, 57, 1361. [Google Scholar] [CrossRef]
- Yang, B.; Eliot, M.; McClean, M.D.; Waterboer, T.; Pawlita, M.; Butler, R.; Nelson, H.H.; Langevin, S.M.; Christensen, B.C.; Kelsey, K.T. DNA methylation-derived systemic inflammation indices and their association with oropharyngeal cancer risk and survival. Head Neck 2022, 44, 904–913. [Google Scholar] [CrossRef]
- Kara, G.; Calin, G.A.; Ozpolat, B. RNAi-based therapeutics and tumor targeted delivery in cancer. Adv. Drug Deliv. Rev. 2022, 182, 114113. [Google Scholar] [CrossRef]
- Bajbouj, K.; Al-Ali, A.; Ramakrishnan, R.K.; Saber-Ayad, M.; Hamid, Q. Histone Modification in NSCLC: Molecular Mechanisms and Therapeutic Targets. Int. J. Mol. Sci. 2021, 22, 11701. [Google Scholar] [CrossRef]
- Hasbullah, H.H.; Musa, M. Gene Therapy Targeting p53 and KRAS for Colorectal Cancer Treatment: A Myth or the Way Forward? Int. J. Mol. Sci. 2021, 22, 11941. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Cao, J.; Topatana, W.; Juengpanich, S.; Li, S.; Zhang, B.; Shen, J.; Cai, L.; Cai, X.; Chen, M. Targeting mutant p53 for cancer therapy: Direct and indirect strategies. J. Hematol. Oncol. 2021, 14, 157. [Google Scholar] [CrossRef] [PubMed]
- Kasikci, Y.; Gronemeyer, H. Complexity against current cancer research—Are we on the wrong track? Int. J. Cancer 2021, 150, 1569–1578. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.K.; Sun, X.J.; Gao, X.D.; Qian, Y.; Wang, L.; Zhao, W.L. Methylation alterations and advance of treatment in lymphoma. Front. Biosci. 2021, 26, 602–613. [Google Scholar] [CrossRef]
- Otmani, K.; Lewalle, P. Tumor Suppressor miRNA in Cancer Cells and the Tumor Microenvironment: Mechanism of Deregulation and Clinical Implications. Front. Oncol. 2021, 11, 708765. [Google Scholar] [CrossRef]
- Perri, P.; Ponzoni, M.; Corrias, M.V.; Ceccherini, I.; Candiani, S.; Bachetti, T. A Focus on Regulatory Networks Linking MicroRNAs, Transcription Factors and Target Genes in Neuroblastoma. Cancers 2021, 13, 5528. [Google Scholar] [CrossRef]
- Rozenberg, J.M.; Zvereva, S.; Dalina, A.; Blatov, I.; Zubarev, I.; Luppov, D.; Bessmertnyi, A.; Romanishin, A.; Alsoulaiman, L.; Kumeiko, V.; et al. The p53 family member p73 in the regulation of cell stress response. Biol. Direct 2021, 16, 23. [Google Scholar] [CrossRef]
- Sahin, I.; George, A.; Seyhan, A.A. Therapeutic Targeting of Alternative RNA Splicing in Gastrointestinal Malignancies and Other Cancers. Int. J. Mol. Sci. 2021, 22, 11790. [Google Scholar] [CrossRef]
- Jiang, M.; Liu, F.; Yang, A.-G.; Wang, W.; Zhang, R. The role of long non-coding RNAs in the pathogenesis of head and neck squamous cell carcinoma. Mol. Ther. Oncolytics 2021, 24, 127–138. [Google Scholar] [CrossRef] [PubMed]
- Shiiba, M.; Uzawa, K.; Tanzawa, H. MicroRNAs in Head and Neck Squamous Cell Carcinoma (HNSCC) and Oral Squamous Cell Carcinoma (OSCC). Cancers 2010, 2, 653–669. [Google Scholar] [CrossRef] [Green Version]
- Sannigrahi, M.K.; Sharma, R.; Panda, N.K.; Khullar, M. Role of non-coding RNAs in head and neck squamous cell carcinoma: A narrative review. Oral Dis. 2018, 24, 1417–1427. [Google Scholar] [CrossRef] [PubMed]
- Tu, H.F.; Lin, S.C.; Chang, K.W. MicroRNA aberrances in head and neck cancer: Pathogenetic and clinical significance. Curr. Opin. Otolaryngol. Head Neck Surg. 2013, 21, 104–111. [Google Scholar] [CrossRef]
- D’Souza, W.; Kumar, A. microRNAs in oral cancer: Moving from bench to bed as next generation medicine. Oral Oncol. 2020, 111, 104916. [Google Scholar] [CrossRef]
- Macfarlane, L.-A.; Murphy, P.R. MicroRNA: Biogenesis, Function and Role in Cancer. Curr. Genom. 2010, 11, 537–561. [Google Scholar] [CrossRef] [Green Version]
- Valastyan, S.; Weinberg, R.A. miR-31: A crucial overseer of tumor metastasis and other emerging roles. Cell Cycle 2010, 9, 2124–2129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, L.; Han, Y.; Zhang, H.; Fan, D. Prognostic markers in esophageal cancer: From basic research to clinical use. Expert Rev. Gastroenterol. Hepatol. 2015, 9, 887–889. [Google Scholar] [CrossRef] [Green Version]
- Nagy, Á.; Lánczky, A.; Menyhárt, O.; Győrffy, B. Validation of miRNA prognostic power in hepatocellular carcinoma using expression data of independent datasets. Sci. Rep. 2018, 8, 9227. [Google Scholar] [CrossRef]
- Balachandran, A.A.; Larcher, L.M.; Chen, S.; Veedu, R.N. Therapeutically Significant MicroRNAs in Primary and Metastatic Brain Malignancies. Cancers 2020, 12, 2534. [Google Scholar] [CrossRef] [PubMed]
- Qiang, H.; Zhan, X.; Wang, W.; Cheng, Z.; Ma, S.; Jiang, C. A Study on the Correlations of the miR-31 Expression with the Pathogenesis and Prognosis of Head and Neck Squamous Cell Carcinoma. Cancer Biother. Radiopharm. 2019, 34, 189–195. [Google Scholar] [CrossRef]
- Tu, H.-F.; Liu, C.-J.; Hung, W.-W.; Shieh, T.-M. Co-upregulation of miR-31 and its host gene lncRNA MIR31HG in oral squamous cell carcinoma. J. Dent. Sci. 2021, 17, 696–706. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef] [PubMed]
- Tierney, J.F.; Stewart, L.A.; Ghersi, D.; Burdett, S.; Sydes, M.R. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials 2007, 8, 16. [Google Scholar] [CrossRef] [Green Version]
- Jakob, M.; Mattes, L.M.; Küffer, S.; Unger, K.; Hess, J.; Bertlich, M.; Haubner, F.; Ihler, F.; Canis, M.; Weiss, B.G.; et al. MicroRNA expression patterns in oral squamous cell carcinoma: Hsa-mir-99b-3p and hsa-mir-100-5p as novel prognostic markers for oral cancer. Head Neck 2019, 41, 3499–3515. [Google Scholar] [CrossRef]
- Wang, L.-L.; Li, H.-X.; Yang, Y.-Y.; Su, Y.-L.; Lian, J.-S.; Li, T.; Xu, J.; Wang, X.-N.; Jin, N.; Liu, X.-F. MiR-31 is a potential biomarker for diagnosis of head and neck squamous cell carcinoma. Int. J. Clin. Exp. Pathol. 2018, 11, 4339–4345. [Google Scholar] [PubMed]
- Gao, G.; Gay, H.A.; Chernock, R.D.; Zhang, T.R.; Luo, J.; Thorstad, W.L.; Lewis Jr, J.S.; Wang, X. A microRNA expression signature for the prognosis of oropharyngeal squamous cell carcinoma. Cancer 2013, 119, 72–80. [Google Scholar] [CrossRef]
- Chen, L.; Wen, Y.; Zhang, J.; Sun, W.; Lui, V.W.Y.; Wei, Y.; Chen, F.; Wen, W. Prediction of radiotherapy response with a 5-microRNA signature-based nomogram in head and neck squamous cell carcinoma. Cancer Med. 2018, 7, 726–735. [Google Scholar] [CrossRef]
- Hung, K.F.; Liu, C.J.; Chiu, P.C.; Lin, J.S.; Chang, K.W.; Shih, W.Y.; Kao, S.Y.; Tu, H.F. MicroRNA-31 upregulation predicts increased risk of progression of oral potentially malignant disorder. Oral Oncol. 2016, 53, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Miladinovic, B.; Hozo, I.; Djulbegovic, B. Trial Sequential Boundaries for Cumulative Meta-Analyses. Stata J. 2013, 13, 77–91. [Google Scholar] [CrossRef] [Green Version]
- Al Rawi, N.; Elmabrouk, N.; Abu Kou, R.; Mkadmi, S.; Rizvi, Z.; Hamdoon, Z. The role of differentially expressed salivary microRNA in oral squamous cell carcinoma—A systematic review. Arch. Oral Biol. 2021, 125, 105108. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Identification Records through Databases and Registers | |||
|---|---|---|---|
| Databases | k-Words | Search Details | Number |
| PubMed | miR-31 AND HNSCC | Search: miR-31 AND HNSCC Sort by: Most Recent “miR-31”[All Fields] AND (“hnsccs”[All Fields] OR “squamous cell carcinoma of head and neck”[MeSH Terms] OR (“squamous”[All Fields] AND “cell”[All Fields] AND “carcinoma”[All Fields] AND “head”[All Fields] AND “neck”[All Fields]) OR “squamous cell carcinoma of head and neck”[All Fields] OR “hnscc”[All Fields]) Translations HNSCC: “hnsccs”[All Fields] OR “squamous cell carcinoma of head and neck”[MeSH Terms] OR (“squamous”[All Fields] AND “cell”[All Fields] AND “carcinoma”[All Fields] AND “head”[All Fields] AND “neck”[All Fields]) OR “squamous cell carcinoma of head and neck”[All Fields] OR “hnscc”[All Fields] | 34 |
| Microrna AND HNSCC AND prognosis | Search: Microrna AND HNSCC AND prognosis Sort by: Most Recent (“microrna s”[All Fields] OR “micrornas”[MeSH Terms] OR “micrornas”[All Fields] OR “microrna”[All Fields]) AND (“hnsccs”[All Fields] OR “squamous cell carcinoma of head and neck”[MeSH Terms] OR (“squamous”[All Fields] AND “cell”[All Fields] AND “carcinoma”[All Fields] AND “head”[All Fields] AND “neck”[All Fields]) OR “squamous cell carcinoma of head and neck”[All Fields] OR “hnscc”[All Fields]) AND (“prognosis”[MeSH Terms] OR “prognosis”[All Fields] OR “prognoses”[All Fields]) Translations Microrna: “microrna’s”[All Fields] OR “micrornas”[MeSH Terms] OR “micrornas”[All Fields] OR “microrna”[All Fields] HNSCC: “hnsccs”[All Fields] OR “squamous cell carcinoma of head and neck”[MeSH Terms] OR (“squamous”[All Fields] AND “cell”[All Fields] AND “carcinoma”[All Fields] AND “head”[All Fields] AND “neck”[All Fields]) OR “squamous cell carcinoma of head and neck”[All Fields] OR “hnscc”[All Fields] prognosis: “prognosis”[MeSH Terms] OR “prognosis”[All Fields] OR “prognoses”[All Fields] | 395 | |
| miR-31 AND OSCC | Search: miR-31 AND OSCC Sort by: Most Recent “miR-31”[All Fields] AND “OSCC”[All Fields] | 25 | |
| miR-31 AND laryngeal cancer | Search: miR-31 AND laryngeal cancer Sort by: Most Recent “miR-31”[All Fields] AND (“laryngeal neoplasms”[MeSH Terms] OR (“laryngeal”[All Fields] AND “neoplasms”[All Fields]) OR “laryngeal neoplasms”[All Fields] OR (“laryngeal”[All Fields] AND “cancer”[All Fields]) OR “laryngeal cancer”[All Fields]) Translations laryngeal cancer: “laryngeal neoplasms”[MeSH Terms] OR (“laryngeal”[All Fields] AND “neoplasms”[All Fields]) OR “laryngeal neoplasms”[All Fields] OR (“laryngeal”[All Fields] AND “cancer”[All Fields]) OR “laryngeal cancer”[All Fields] | 7 | |
| miR-31 AND oropharynx | Search: miR-31 AND oropharynx Sort by: Most Recent “miR-31”[All Fields] AND (“oropharynx”[MeSH Terms] OR “oropharynx”[All Fields] OR “oropharynxes”[All Fields]) Translations oropharynx: “oropharynx”[MeSH Terms] OR “oropharynx”[All Fields] OR “oropharynxes”[All Fields] | 1 | |
| Total PubMed | 462 | ||
| Duplicates removed (PubMed) EndNote | 432 | ||
| SCOPUS | miR-31 AND HNSCC | TITLE-ABS-KEY (mir-31 AND hnscc) | 13 |
| miR-31 AND OSCC | TITLE-ABS-KEY (mir-31 AND oscc) | 27 | |
| Microrna AND HNSCC AND prognosis | TITLE-ABS-KEY (microrna AND hnscc AND prognosis) | 211 | |
| Total SCOPUS | 251 | ||
| Duplicates removed (PubMed and SCOPUS) EndNote | 535 | ||
| Cochrane library | miR-31 AND HNSCC | miR-31 AND HNSCC in Title Abstract Keyword | 1 |
| Microrna AND HNSCC AND prognosis | Microrna AND HNSCC AND prognosis in Title Abstract Keyword | 2 | |
| Total Cochrane library | 3 | ||
| Total records | 716 | ||
| Number of records after duplicates removed (PubMed Scopus and Cochrane library) EndNote | 536 | ||
| Number of records after duplicates removed MANUAL | 512 | ||
| Other research sources, gray literature, and previous systematic reviews | |||
| Google Scholar | Mir 31 | allintitle: “mir 31” | 620 |
| http://www.opengrey.eu (accessed on 5 January 2022) DANS EASY Archive | Mir | 80 | |
| Previous systematic reviews | 121 | ||
| Update of the research completed on 3 March 2022 with the inclusion of records from Web of Science | |||
| Web of Science | Head and Neck Cancer | 81,593 | |
| Oral cancer | 104,022 | ||
| Oral carcinoma | 47,461 | ||
| Oral squamous cell carcinoma | 28,540 | ||
| Head and Neck Squamous Cell Carcinoma | 38,318 | ||
| Pharyngeal cancer | 3766 | ||
| miR-31 | 972 | ||
| Total Web Of Science | 257,723 | ||
| PubMed | Oral carcinoma OR Oral Cancer OR Head and Neck Cancer OR Oral squamous cell carcinoma OR Head and Neck Squamous Cell Carcinoma OR pharyngeal cancer | Search: Oral carcinoma OR Oral Cancer OR Head and Neck Cancer OR Oral squamous cell carcinoma OR Head and Neck Squamous Cell Carcinoma OR pharyngeal cancer ((“mouth”[MeSH Terms] OR “mouth”[All Fields] OR “oral”[All Fields]) AND (“carcinoma”[MeSH Terms] OR “carcinoma”[All Fields] OR “carcinomas”[All Fields] OR “carcinoma s”[All Fields])) OR (“mouth neoplasms”[MeSH Terms] OR (“mouth”[All Fields] AND “neoplasms”[All Fields]) OR “mouth neoplasms”[All Fields] OR (“oral”[All Fields] AND “cancer”[All Fields]) OR “oral cancer”[All Fields]) OR (“head and neck neoplasms”[MeSH Terms] OR (“head”[All Fields] AND “neck”[All Fields] AND “neoplasms”[All Fields]) OR “head and neck neoplasms”[All Fields] OR (“head”[All Fields] AND “neck”[All Fields] AND “cancer”[All Fields]) OR “head and neck cancer”[All Fields]) OR (“squamous cell carcinoma of head and neck”[MeSH Terms] OR (“squamous”[All Fields] AND “cell”[All Fields] AND “carcinoma”[All Fields] AND “head”[All Fields] AND “neck”[All Fields]) OR “squamous cell carcinoma of head and neck”[All Fields] OR (“oral”[All Fields] AND “squamous”[All Fields] AND “cell”[All Fields] AND “carcinoma”[All Fields]) OR “oral squamous cell carcinoma”[All Fields]) OR (“squamous cell carcinoma of head and neck”[MeSH Terms] OR (“squamous”[All Fields] AND “cell”[All Fields] AND “carcinoma”[All Fields] AND “head”[All Fields] AND “neck”[All Fields]) OR “squamous cell carcinoma of head and neck”[All Fields] OR (“head”[All Fields] AND “neck”[All Fields] AND “squamous”[All Fields] AND “cell”[All Fields] AND “carcinoma”[All Fields]) OR “head and neck squamous cell carcinoma”[All Fields]) OR (“pharyngeal neoplasms”[MeSH Terms] OR (“pharyngeal”[All Fields] AND “neoplasms”[All Fields]) OR “pharyngeal neoplasms”[All Fields] OR (“pharyngeal”[All Fields] AND “cancer”[All Fields]) OR “pharyngeal cancer”[All Fields]) Translations Oral: “mouth”[MeSH Terms] OR “mouth”[All Fields] OR “oral”[All Fields] carcinoma: “carcinoma”[MeSH Terms] OR “carcinoma”[All Fields] OR “carcinomas”[All Fields] OR “carcinoma’s”[All Fields] Oral Cancer: “mouth neoplasms”[MeSH Terms] OR (“mouth”[All Fields] AND “neoplasms”[All Fields]) OR “mouth neoplasms”[All Fields] OR (“oral”[All Fields] AND “cancer”[All Fields]) OR “oral cancer”[All Fields] Head and Neck Cancer: “head and neck neoplasms”[MeSH Terms] OR (“head”[All Fields] AND “neck”[All Fields] AND “neoplasms”[All Fields]) OR “head and neck neoplasms”[All Fields] OR (“head”[All Fields] AND “neck”[All Fields] AND “cancer”[All Fields]) OR “head and neck cancer”[All Fields] Oral squamous cell carcinoma: “squamous cell carcinoma of head and neck”[MeSH Terms] OR (“squamous”[All Fields] AND “cell”[All Fields] AND “carcinoma”[All Fields] AND “head”[All Fields] AND “neck”[All Fields]) OR “squamous cell carcinoma of head and neck”[All Fields] OR (“oral”[All Fields] AND “squamous”[All Fields] AND “cell”[All Fields] AND “carcinoma”[All Fields]) OR “oral squamous cell carcinoma”[All Fields] Head and Neck Squamous Cell Carcinoma: “squamous cell carcinoma of head and neck”[MeSH Terms] OR (“squamous”[All Fields] AND “cell”[All Fields] AND “carcinoma”[All Fields] AND “head”[All Fields] AND “neck”[All Fields]) OR “squamous cell carcinoma of head and neck”[All Fields] OR (“head”[All Fields] AND “neck”[All Fields] AND “squamous”[All Fields] AND “cell”[All Fields] AND “carcinoma”[All Fields]) OR “head and neck squamous cell carcinoma”[All Fields] pharyngeal cancer: “pharyngeal neoplasms”[MeSH Terms] OR (“pharyngeal”[All Fields] AND “neoplasms”[All Fields]) OR “pharyngeal neoplasms”[All Fields] OR (“pharyngeal”[All Fields] AND “cancer”[All Fields]) OR “pharyngeal cancer”[All Fields] | 445,203 |
| Scopus | TITLE-ABS-KEY (“Oral carcinoma” OR “Oral Cancer” OR “Head and Neck Cancer” OR “Oral squamous cell carcinoma” OR “Head and Neck Squamous Cell Carcinoma” OR “pharyngeal cancer”) | 97,781 | |
| Total of updated records | 542,984 | ||
| First Author, Data | Country | Study Design | Number of Patients | Follow-Up Max | Tumor Type\Tumor Site | Cut-off | miR | HR miR-31 Low and High Expression (OS, PFS, CSS, DFS, RFS) |
|---|---|---|---|---|---|---|---|---|
| Jakob (2019) [33] | Germany | RT | 36 | 60 months | OSCC | median | miR-21, miR-29, miR-31, miR-99a, miR-99b, miR-100, miR-143, miR-155. | OS:HR 3.69 (1.07–12.79) p = 0.028 RFS:HR 1.82(0.66–5.05) p = 2.4297 PFS: HR 2.31 (0.94–5.69) p = 0.05982 |
| Wang (2018) [34] | China | RT | 118 | 60 months | HNSCC | median | miR-31 | OS: HR 3.31 (1.42–5.36) * p = 0.015 DFS: HR 3.86 (1.53–6.05) p = 0.009 |
| Qiang (2019) [29] | China | RT | 46 | 60 months | 21 HSCC, 25 LSCC | median | miR-31 | OS: HR 1.38 (1.02–1.87) p = 0.036 |
| Tu (2021) [30] | Taiwan | RT | 40 | 160 months | OSCC | median | miR-31 | OS: HR 1.68 (0.7747–3.6433) p = 0.189 |
| Chen (2018) [36] 1 | China | RT | 509 (307 con R) | 80 months | HNSCC | median | miR-99a, miR-31 miR-410, miR-424, miR-495 | OS R: HR 3.65, (2.46–8.16) p < 0.0001; OS: HR 1.81 (1.45–2.57) p < 0.0001 |
| Gao (2013) [35] 2 | USA | RT | 150 | 50 months | OPSCC | median | miR-9, miR-223, miR-31, miR-18a, miR-155 | OS HR 3.22 p = 0.0022 |
| Hung (2016) [37] 3 | Taiwan | Prospective | 46 | 28 months | OPMD | median | miR-21, miR-31 | PFS:HR 8.43 (1.04–68.03) p = 0.047 |
| First Author, Data | Sample | Clinical Data | Marker Quantification | Prognostication | Statistics | Classical Prognostic Factors | Score |
|---|---|---|---|---|---|---|---|
| Wang (2018) [34] | 3 | 2 | 3 | 2 | 2 | 3 | 15 |
| Qiang (2019) [29] | 2 | 3 | 3 | 2 | 2 | 2 | 14 |
| Tu (2021) [30] | 1 | 3 | 3 | 2 | 2 | 2 | 13 |
| Jakob (2019) [33] | 1 | 3 | 3 | 3 | 3 | 3 | 16 |
| Certainty Assessment | No. of Patients | Effect | Certainty | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| No. of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | Relative (95% CI) | Absolute (95% CI) | ||
| 4 | observational studies | not serious | not serious | not serious | serious 1 | strong association | 240 | HR 1.58 (1.21 to 2.06) | 2 fewer per 1.000 (From 2 fewer to 1 fewer) | ⊕⊕◯◯ Low |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dioguardi, M.; Spirito, F.; Sovereto, D.; Alovisi, M.; Aiuto, R.; Garcovich, D.; Crincoli, V.; Laino, L.; Cazzolla, A.P.; Caloro, G.A.; et al. The Prognostic Role of miR-31 in Head and Neck Squamous Cell Carcinoma: Systematic Review and Meta-Analysis with Trial Sequential Analysis. Int. J. Environ. Res. Public Health 2022, 19, 5334. https://doi.org/10.3390/ijerph19095334
Dioguardi M, Spirito F, Sovereto D, Alovisi M, Aiuto R, Garcovich D, Crincoli V, Laino L, Cazzolla AP, Caloro GA, et al. The Prognostic Role of miR-31 in Head and Neck Squamous Cell Carcinoma: Systematic Review and Meta-Analysis with Trial Sequential Analysis. International Journal of Environmental Research and Public Health. 2022; 19(9):5334. https://doi.org/10.3390/ijerph19095334
Chicago/Turabian StyleDioguardi, Mario, Francesca Spirito, Diego Sovereto, Mario Alovisi, Riccardo Aiuto, Daniele Garcovich, Vito Crincoli, Luigi Laino, Angela Pia Cazzolla, Giorgia Apollonia Caloro, and et al. 2022. "The Prognostic Role of miR-31 in Head and Neck Squamous Cell Carcinoma: Systematic Review and Meta-Analysis with Trial Sequential Analysis" International Journal of Environmental Research and Public Health 19, no. 9: 5334. https://doi.org/10.3390/ijerph19095334
APA StyleDioguardi, M., Spirito, F., Sovereto, D., Alovisi, M., Aiuto, R., Garcovich, D., Crincoli, V., Laino, L., Cazzolla, A. P., Caloro, G. A., Di Cosola, M., Ballini, A., Lo Muzio, L., & Troiano, G. (2022). The Prognostic Role of miR-31 in Head and Neck Squamous Cell Carcinoma: Systematic Review and Meta-Analysis with Trial Sequential Analysis. International Journal of Environmental Research and Public Health, 19(9), 5334. https://doi.org/10.3390/ijerph19095334