
The Beneficial Role of Involvement in Alcoholics Anonymous for Existential and Subjective Well-Being of Alcohol-Dependent Individuals? The Model Verification


Abstract
:1. Introduction
2. Review of Literature
2.1. Involvement in AA and Recovery from Alcohol Addiction
2.2. Improved Meaning of Life as a Potential Mechanism of Change Associated with AA Involvement
2.3. Improved Hope as a Potential Mechanism of Change Associated with AA Involvement
3. Material and Methods
3.1. Participants
3.2. Measures
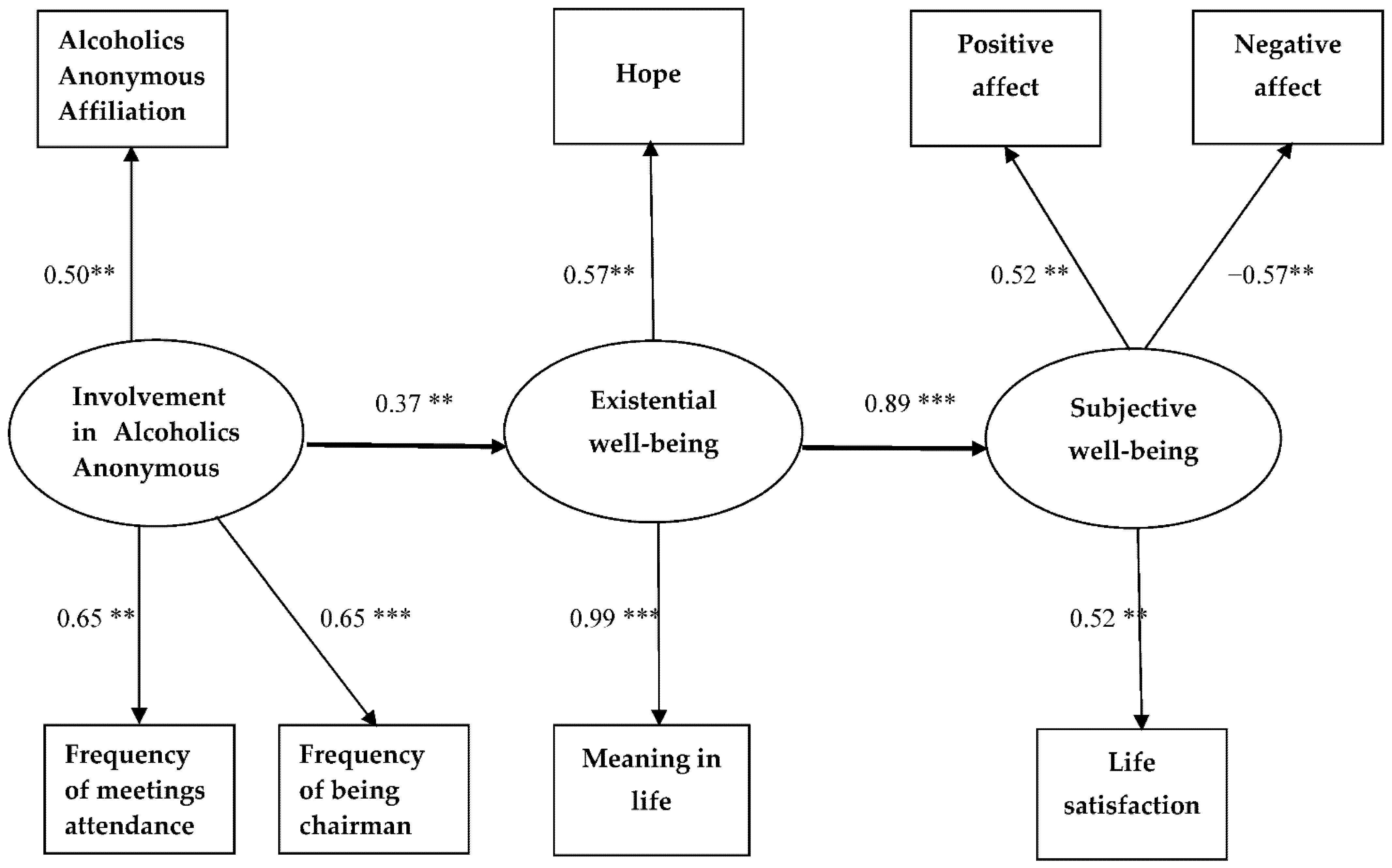
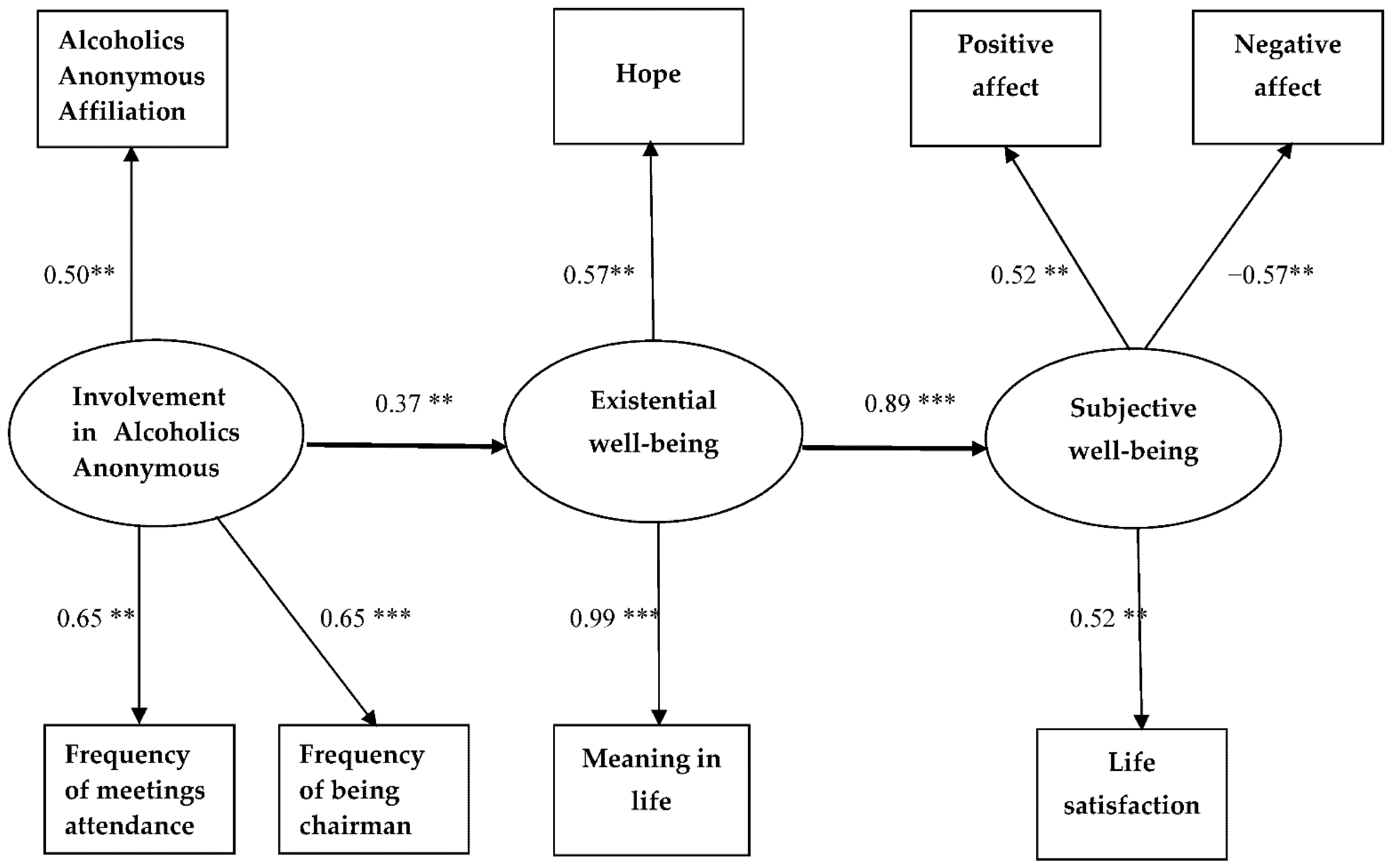
3.3. Conceptual Model
3.4. Statistical Analyses
4. Results
4.1. Descriptive Statistics
4.2. Model Verification
5. Discussion
6. Limitation and Future Research
7. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nowakowska, I.; Lewczuk, K.; Gola, M. Changes in the addiction prevalence in polish population between 1990-2019: Review of available data. J. Addict. Sci. 2020, 6, 17–31. [Google Scholar] [CrossRef]
- Available online: https://www.parpa.pl/index.php/33-analizy-badania-raporty (accessed on 13 August 2021).
- Twelve Steps and Twelve Traditions; Alcoholics Anonymous World Services Inc.: Akron, OH, USA, 1981.
- Alcoholics Anonymous. Alcoholics Anonymous: The Story of How Many Thousands of Men and Women Have Recovered from Alcoholism, 4th ed.; Alcoholics Anonymous World Services: New York, NY, USA, 2001. [Google Scholar]
- Tadeusz. History of AA in Poland; Fundacja Biura Służby Krajowej Anonimowych Alkoholików: Warszawa, Poland, 2012. [Google Scholar]
- Available online: https://www.parpa.pl/index.php/wspolnota-aa/163-wspolnota-anonimowych-alkoholikow (accessed on 13 August 2021).
- Kelly, J.F.; Yeterian, J.D. The role of mutual help groups in extending the framework of treatment. Alcohol Res. Health 2011, 33, 350–355. [Google Scholar]
- Kownacki, R.J.; Shadish, W.R. Does Alcoholics Anonymous work? The results from a meta-analysis of controlled experiments. Subst. Use Misuse 1999, 34, 1897–1916. [Google Scholar] [CrossRef] [PubMed]
- Kaskutas, L.A. Alcoholics anonymous effectiveness: Faith meets science. J. Addict. Dis. 2009, 28, 145–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Owen, P.L.; Slaymaker, V.; Tonigan, J.S.; McCrady, B.S.; Epstein, E.E.; Kaskutas, L.A.; Humphreys, K.; Miller, W.R. Participation in alcoholics anonymous: Intended and unintended change mechanisms. Alcohol. Clin. Exp. Res. 2003, 27, 524–532. [Google Scholar] [CrossRef]
- Cloud, R.N.; Ziegler, C.H.; Blondell, R.D. What is Alcoholics Anonymous affiliation? Subst. Use Misuse 2004, 39, 1117–1136. [Google Scholar] [CrossRef]
- Krentzman, A.R.; Robinson, E.A.; Perron, B.E.; Cranford, J.A. Predictors of membership in Alcoholics Anonymous in a sample of Successfully remitted alcoholics. J. Psychoact. Drugs 2011, 43, 20–26. [Google Scholar] [CrossRef] [Green Version]
- Humphreys, K.; Blodgett, J.C.; Wagner, T.H. Estimating the efficacy of Alcoholics Anonymous without self-selection bias: An instrumental variables re-analysis of randomized clinical trials. Alcohol. Clin. Exp. Res. 2014, 38, 2688–2694. [Google Scholar] [CrossRef] [Green Version]
- Witbrodt, J.; Kaskutas, L.; Bond, J.; Delucchi, K. Does sponsorship improve outcomes above Alcoholics Anonymous attendance? A latent class growth curve analysis. Addiction 2012, 107, 301–311. [Google Scholar] [CrossRef] [Green Version]
- Witbrodt, J.; Mertens, J.; Kaskutas, L.A.; Bond, J.; Chi, F.; Weisner, C. Do 12-step meeting attendance trajectories over 9 years predict abstinence? J. Subst. Abus. Treat. 2012, 43, 30–43. [Google Scholar] [CrossRef] [Green Version]
- Helm, P. Sobriety versus abstinence. How 12-stepper negotiate long-term recovery across groups. Addict. Res. Theory 2019, 27, 29–36. [Google Scholar] [CrossRef]
- Ellison, C.W. Spiritual well-being: Conceptualization and measurement. J. Psychol-Ogy Theol. 1983, 11, 330–340. [Google Scholar] [CrossRef]
- MacDonald, D.A. Spirituality: Description, measurement, and relation to the five factor model of personality. J. Personal. 2000, 68, 153–197. [Google Scholar] [CrossRef]
- Diener, E.; Ryan, K. Subjective well-being: A general overview. S. Afr. J. Psychol. 2009, 39, 391–406. [Google Scholar] [CrossRef]
- Seligman, M.E.P. Authentic Happiness: Using the New Positive Psychology to Realize Your Potential for Lasting Fulfillment; Free Press: New York, NY, USA, 2002. [Google Scholar]
- Frankl, V.E. Man’s Search for Meaning: An Introduction to Logotherapy, 4th ed.; Lasch, I., Translator; Beacon Press: Boston, MA, USA, 1992. [Google Scholar]
- Wnuk, M.; Marcinkowski, J.T. Do existential variables mediate between religious-spiritual facets of functionality and psychological wellbeing. J. Relig. Health 2014, 53, 56–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wnuk, M. The Indirect Relationship Between Spiritual Experiences and Subjective Wellbeing Through Hope? A Sample of Chilean Students. J. Relig. Health 2021. [Google Scholar] [CrossRef]
- Walitzer, K.S.; Dermen, K.H.; Barrick, C. Facilitating involvement in Alcoholics Anonymous during out-patient treatment: A randomized clinical trial. Addiction 2009, 104, 391–401. [Google Scholar] [CrossRef]
- Greenfield, B.L.; Tonigan, J.S. The general alcoholics anonymous tools of recovery: The adoption of 12-step practices and beliefs. Psychol. Addict. Behav. 2013, 27, 553–561. [Google Scholar] [CrossRef] [Green Version]
- Moos, R.H.; Moos, B.S. Participation in treatment and Alcoholics Anonymous: A 16-year follow-up of initially untreated individuals. J. Clin. Psychol. 2006, 62, 735–750. [Google Scholar] [CrossRef]
- Galanter, M.; Dermatis, H.; Santucci, C. Young People in Alcoholics Anonymous: The role of spiritual orientation and AA member affiliation. J. Addict. Dis. 2012, 31, 173–182. [Google Scholar] [CrossRef]
- McKellar, J.; Stewart, E.; Humphreys, K. Alcoholics anonymous involvement and positive alcohol-related outcomes: Cause, consequence, or just a correlate? A prospective 2-year study of 2319 alcohol-dependent men. J. Consult. Clin. Psychol. 2003, 71, 302–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zemore, S.E. A role for spiritual change in the benefits of 12-step involvement. Alcohol. Clin. Exp. Res. 2007, 31, 76s–79s. [Google Scholar] [CrossRef] [PubMed]
- Galanter, M.; Dermatis, H.; Stanievich, J.; Santucci, C. Physicians in long-term recovery who are members of alcoholics anonymous. Am. J. Addict. 2013, 22, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Zemore, S.E.; Mulia, N.; Jones-Webb, R.J.; Liu, H.; Schmidt, L. The 2008–2009 recession and alcohol outcomes: Differential exposure and vulnerability for Black and Latino populations. J. Stud. Alcohol Drugs 2013, 74, 9–20. [Google Scholar] [CrossRef]
- Galanter, M.; Dermatis, H.; Sampson, C. Narcotics anonymous: A comparison of military veterans and non-veterans. J. Addict. Dis. 2014, 33, 187–195. [Google Scholar] [CrossRef] [PubMed]
- Tonigan, J.S.; Rice, S.L. Is it beneficial to have an alcoholics anonymous sponsor? Psychol. Addict. Behav. J. Soc. Psychol. Addict. Behav. 2010, 24, 397–403. [Google Scholar] [CrossRef] [Green Version]
- Bond, J.; Kaskutas, L.A.; Weisner, C. The persistent influence of social networks and alcoholics anonymous on abstinence. J. Stud. Alcohol 2003, 64, 579–588. [Google Scholar] [CrossRef]
- Polcin, D.L.; Zemore, S. Psychiatric severity and spirituality, helping, and participation in alcoholics anonymous during recovery. Am. J. Drug Alcohol Abus. 2004, 30, 577–592. [Google Scholar] [CrossRef]
- Morgenstern, J.; Labouvie, E.; McCrady, B.S.; Kahler, C.W.; Frey, R.M. Affiliation with Alcoholics Anonymous after treatment: A study of its therapeutic effects and mechanisms of action. J. Consult. Clin. Psychol. 1997, 65, 768–777. [Google Scholar] [CrossRef]
- Kelly, J.F.; Stout, R.L.; Magill, M.; Tonigan, J.S.; Pagano, M.E. Mechanisms of behavior change in alcoholics anonymous: Does Alcoholics Anonymous lead to better alcohol use outcomes by reducing depression symptoms? Addiction 2010, 105, 626–636. [Google Scholar] [CrossRef] [Green Version]
- Blonigen, D.M.; Timko, C.; Finney, J.W.; Moos, B.S.; Moos, R.H. Alcoholics Anonymous attendance, decreases in impulsivity and drinking and psychosocial outcomes over 16 years: Moderated-mediation from a developmental perspective. Addiction 2011, 106, 2167–2177. [Google Scholar] [CrossRef] [Green Version]
- Kaskutas, L.A.; Bond, J.; Humphreys, K. Social networks as mediators of the effect of Alcoholics Anonymous. Addiction 2002, 97, 891–900. [Google Scholar] [CrossRef]
- Krentzman, A.R.; Cranford, J.A.; Robinson, E.A. Multiple dimensions of spirituality in recovery: A lagged mediational analysis of Alcoholics Anonymous’ principal theoretical mechanism of behavior change. Subst. Abus. 2013, 34, 20–32. [Google Scholar] [CrossRef] [PubMed]
- Krentzman, A.R.; Strobbe, S.; Harris, J.I.; Jester, J.M.; Robinson, E. Decreased drinking and alcoholics anonymous are associated with different dimensions of spirituality. Psychol. Relig. Spiritual. 2017, 9, S40–S48. [Google Scholar] [CrossRef]
- Montes, K.S.; Tonigan, J.S. Does Age Moderate the Effect of Spirituality/Religiousness in Accounting for Alcoholics Anonymous Benefit? Alcohol. Treat. Q. 2017, 35, 96–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baumsteiger, R.; Chenneville, T. Challenges to the conceptualization and measurement of religiosity and spirituality in mental health research. J. Relig. Health 2015, 54, 2344–2354. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, E.; White, W. Recovery spirituality. Religions 2015, 6, 58–81. [Google Scholar] [CrossRef] [Green Version]
- Csabonyi, M.; Phillips, L.J. Meaning in life and substance use. J. Humanist. Psychol. 2020, 60, 3–19. [Google Scholar] [CrossRef]
- Steger, M.F.; Fitch-Martin, A.R.; Donnelly, J.; Rickard, K.M. Meaning in life and health: Proactive health orientation links meaning in life to health variables among American undergraduates. J. Happiness Stud. Interdiscip. Forum Subj. Well-Being 2015, 16, 583–597. [Google Scholar] [CrossRef]
- Newcomb, M.D.; Harlow, L.L. Life events and substance use among adolescents: Mediating effects of perceived loss of control and meaninglessness in life. J. Personal. Soc. Psychol. 1986, 51, 564–577. [Google Scholar] [CrossRef]
- Nicholson, T.; Higgins, W.; Turner, P.; James, S.; Stickle, F.; Pruitt, T. The relation between meaning in life and the occurrence of drug abuse: A retrospective study. Psychol. Addict. Behav. 1994, 8, 24–28. [Google Scholar] [CrossRef]
- Crumbaugh, J.C. Cross-validation of Purpose-in-Life test based on Frankl’s concepts. J. Individ. Psychol. 1968, 24, 74–81. [Google Scholar] [PubMed]
- Crumbaugh, J.C.; Maholick, L.T. An Experimental Study in Existentialism: The Psychometric Approach to Frankl’s Concept of Noogenic Neurosis. J. Clin. Psychol. 1964, 20, 200–207. [Google Scholar] [CrossRef]
- Koushede, V.; Holstein, B.E. Sense of coherence and medicine use for headache among adolescents. J. Adolesc. Health Off. Publ. Soc. Adolesc. Med. 2009, 45, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Çevik, C.; Ciğerci, Y.; Kılıç, İ.; Uyar, S. Relationship between smartphone addiction and meaning and purpose of life in students of health sciences. Perspect. Psychiatr. Care 2020, 56, 705–711. [Google Scholar] [CrossRef]
- Ghaderi, R.M.; Askarizadeh, G.; Ahmadi, G.; Divsalar, K. The role of psychiatric symptoms, social supportand meaning in life in predicting internet addiction among university students: A causal model. Pract. Clin. Psychol. 2018, 6, 101–110. [Google Scholar]
- Zhang, M.X.; Yang, H.M.; Tong, K.K.; Wu, A. The prospective effect of purpose in life on gambling disorder and psychological flourishing among university students. J. Behav. Addict. 2020, 9, 756–765. [Google Scholar] [CrossRef]
- Kim, E.S.; Ryff, C.; Hassett, A.; Brummett, C.; Yeh, C.; Strecher, V. Sense of Purpose in life and likelihood of future illicit drug use or prescription medication misuse. Psychosom. Med. 2020, 82, 715–721. [Google Scholar] [CrossRef]
- Brassai, L.; Piko, B.F.; Steger, M.F. Meaning in life: Is it a protective factor for adolescents’ psychological health? Int. J. Behav. Med. 2011, 18, 44–51. [Google Scholar] [CrossRef]
- Montgomery, H.A.; Miller, W.R.; Tonigan, J.S. Does Alcoholics Anonymous involvement predict treatment outcome? J. Subst. Abus. Treat. 1995, 12, 241–246. [Google Scholar] [CrossRef]
- Tonigan, J.S. Benefits of Alcoholics Anonymous attendance: Replication of findings between clinical research sites in Project MATCH. Alcohol. Treat. Q. 2001, 19, 67–77. [Google Scholar] [CrossRef]
- Carroll, S. Spirituality and purpose in life in alcoholism recovery. J. Stud. Alcohol 1993, 54, 297–301. [Google Scholar] [CrossRef]
- Gomes, K.; Hart, K.E. Adherence to recovery practices prescribed by Alcoholics Anonymous: Benefits to sustained abstinence and subjective quality of life. Alcohol. Treat. Q. 2009, 27, 223–235. [Google Scholar] [CrossRef]
- Hart, K.E.; Singh, T. An Existential model of flourishing subsequent to treatment for addiction: The importance of living a meaningful and spiritual life. Illn. Crisis Loss 2009, 17, 125–147. [Google Scholar] [CrossRef]
- Oakes, K.E.; Allen, J.P.; Ciarrocchi, J.W. Spirituality, religious problem-solving, and sobriety in Alcoholics Anonymous. Alcohol. Treat. Q. 2000, 18, 37–50. [Google Scholar] [CrossRef]
- Beitra, D.; Howrey, H.L.; Seibert, S.; Ellis, A.E.; Mizrachi, J. Beyond abstinence: An examination of psychological well-being in members of Narcotics Anonymous. J. Happiness Stud. 2016, 17, 817–832. [Google Scholar] [CrossRef]
- Gutierrez, D. Spiritus contra spiritum: Addiction, hope, and the search for meaning. Spiritual. Clin. Pract. 2019, 6, 229–239. [Google Scholar] [CrossRef]
- Martin, R.A.; MacKinnon, S.; Johnson, J.; Rohsenow, D.J. Purpose in life predicts treatment outcome among adult cocaine abusers in treatment. J. Subst. Abus. Treat. 2011, 40, 183–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waisberg, J.L.; Porter, J.E. Purpose in life and outcome of treatment for alcohol dependence. Br. J. Clin. Psychol. 1994, 33, 49–63. [Google Scholar] [CrossRef]
- Jacobson, G.R.; Ritter, D.P.; Mueller, L. Purpose in life and personal values among adult alcoholics. J. Clin. Psychol. 1977, 33, 314–316. [Google Scholar] [CrossRef]
- Roos, C.R.; Kirouac, M.; Pearson, M.R.; Fink, B.C.; Witkiewitz, K. Examining temptation to drink from an existential perspective: Associations among temptation, purpose in life, and drinking outcomes. Psychol. Addict. Behav. 2015, 29, 716–724. [Google Scholar] [CrossRef] [PubMed]
- Herth, K. Development and refinement of an instrument to measure hope. Sch. Inq. Nurs. Pract. 1991, 5, 39–51. [Google Scholar]
- Nowotny, M.L. Assessment of hope in patients with cancer: Development of an instrument. Oncol. Nurs. Forum 1989, 16, 57–61. [Google Scholar]
- Snyder, C.R. Hope theory: Rainbows in the mind. Psychol. Inq. 2002, 13, 249–275. [Google Scholar] [CrossRef]
- Staats, S. Hope: Expected positive affect in an adult sample. J. Genet. Psychol. Res. Theory Hum. Dev. 1987, 148, 357–364. [Google Scholar] [CrossRef]
- Farran, C.J.; Wilken, C.; Popovich, J.M. Clinical assessment of hope. Issues Ment. Health Nurs. 1992, 13, 129–138. [Google Scholar] [CrossRef]
- Fredrickson, B.L. Positivity; Crown: New York, NY, USA, 2009. [Google Scholar]
- Lazarus, R.S. Stress and Emotion: A new Synthesis; Springer Publishing Co.: New York, NY, USA, 1999. [Google Scholar]
- Park, N.; Peterson, C.; Seligman, M.E.P. Strengths of character and well-being. J. Soc. Clin. Psychol. 2004, 23, 603–619. [Google Scholar] [CrossRef] [Green Version]
- Koehn, C.; O’Neill, L.; Sherry, J. Hope-focused interventions in substance abuse counselling. Int. J. Ment. Health Addict. 2012, 10, 441–452. [Google Scholar] [CrossRef]
- Jackson, R.; Wernicke, R.; Haaga, D.A.F. Hope as a predictor of entering substance abuse treatment. Addict. Behav. 2003, 28, 13–28. [Google Scholar] [CrossRef]
- Yalom, I.D. The Theory and Practice of Group Psychotherapy, 3rd ed.; Basic Books: New York, NY, USA, 1985. [Google Scholar]
- Gutierrez, D.; Dorais, S.; Goshorn, J.R. Recovery as life transformation: Examining the relationships between recovery, hope, and relapse. Subst. Use Misuse 2020, 55, 1949–1957. [Google Scholar] [CrossRef]
- Magura, S.; Knight, E.L.; Vogel, H.S.; Mahmood, D.; Laudet, A.B.; Rosenblum, A. Mediators of effectiveness in dual-focus self-help groups. Am. J. Drug Alcohol Abus. 2003, 29, 301–322. [Google Scholar] [CrossRef]
- Jason, L.A.; Stevens, E.; Light, J.M. The relationship of sense of community and trust to hope. J. Community Psychol. 2016, 44, 334–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathis, G.M.; Ferrari, J.R.; Groh, D.R.; Jason, L.A. Hope and substance abuse recovery: The impact of agency and pathways within an abstinent communal-living setting. J. Groups Addict. Recover. 2009, 4, 42–50. [Google Scholar] [CrossRef] [Green Version]
- May, E.M.; Hunter, B.A.; Ferrari, J.; Noel, N.; Jason, L.A. Hope and abstinence self-efficacy: Positive predictors of negative affect in substance abuse recovery. Community Ment. Health J. 2015, 51, 695–700. [Google Scholar] [CrossRef] [Green Version]
- Stevens, E.; Guerrero, M.; Green, A.; Jason, L.A. Relationship of hope, sense of community, and quality of life. J. Community Psychol. 2018, 46, 567–574. [Google Scholar] [CrossRef] [PubMed]
- Wnuk, M. Hope as an important factor for mental health in alcohol-dependent subjects attending Alcoholics Anonymous. J. Subst. Use 2017, 22, 182–186. [Google Scholar] [CrossRef]
- Wnuk, M.; Hędzelek, M. Hope as a positive factor for happiness among Sex and Love Addicts Anonymous. Pol. Sexol. 2008, 9, 51–56. [Google Scholar]
- Tonigan, J.S.; Connors, G.J.; Miller, W.R. Alcoholics Anonymous Involvement (AAI) scale: Reliability and norms. Psychol. Addict. Behav. 1996, 10, 75–80. [Google Scholar] [CrossRef]
- Herth, K.A. Development and implementation of a Hope Intervention Program. Oncol. Nurs. Forum 2001, 28, 1009–1016. [Google Scholar]
- Herth, K. Abbreviated instrument to measure hope: Development and psychometric evaluation. J. Adv. Nurs. 1992, 17, 1251–1259. [Google Scholar] [CrossRef] [PubMed]
- Cantril, H. Life satisfaction and chronic disease: Exploration of a theoretical model. Med. Care 1981, 29, 1136–1146. [Google Scholar]
- Czapinski, J. Psychology of Happiness: Research Review and Outline of the Onion Theory; Akademos: Warszawa-Poznan, Poland, 1992. [Google Scholar]
- Kivett, E.; Palmore, E. Change in Life Satisfaction: A Longitudinal Study of Persons Aged 46–70. J. Gerontol. 1977, 32, 311–316. [Google Scholar]
- Crawford, J.R.; Henry, J.D. The positive and negative affect schedule (PANAS): Construct validity, measurement properties and normative data in a large non-clinical sample. Br. J. Clin. Psychol. 2004, 43, 245–265. [Google Scholar] [CrossRef]
- Baumeister, R.F.; Vohs, K.D. The Pursuit of Meaningfulness in Life. In Handbook of Positive Psychology; Snyder, C.R., Lopez, S.J., Eds.; Oxford University Press: Oxford, UK, 2002; pp. 608–618. [Google Scholar]
- Hair, J.F., Jr.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis, 7th ed.; Pearson Prentice Hall: Upper Saddle River, NJ, USA, 2009. [Google Scholar]
- Brown, T.A. Confirmatory Factor Analysis for Applied Research; Guilford Press: New York, NY, USA, 2006. [Google Scholar]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Modeling 1999, 6, e82131. [Google Scholar] [CrossRef]
- Kline, R.B. Methodology in the Social Sciences. Principles and Practice of Structural Equation Modeling, 2nd ed.; Guilford Press: New York, NY, USA, 2005. [Google Scholar]
- Steiger, J.H. Structural model evaluation and modification: An interval estimation approach. Multivar. Behav. Res. 1990, 25, 173–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bollen, K.A.; Stine, R.A. Bootstrapping goodness-of-fit measures in structural equation models. Sociol. Methods Res. 1992, 21, 205–229. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Byrne, B.M. Burnout: Testing for the validity, replication, and invariance of causal structure across elementary, intermediate, and secondary teachers. Am. Educ. Res. J. 1994, 31, 645–673. [Google Scholar] [CrossRef]
- Kelly, J.F.; Magill, M.; Stout, R.L. How do people recover from alcohol dependence? A systematic review of the research on mechanisms of behavior change in Alcoholics Anonymous. Addict. Res. Theory 2009, 17, 236–259. [Google Scholar] [CrossRef]
- Laudet, A.B.; Cleland, C.M.; Magura, S.; Vogel, H.S.; Knight, E.L. Social Support Mediates the Effects of Dual-Focus Mutual Aid Groups on Abstinence from Substance Use. Am. J. Community Psychol. 2004, 34, 175–185. [Google Scholar] [CrossRef] [Green Version]
- Humphreys, K.; Mankowski, E.S.; Moos, R.H.; Finney, J.W. Do enhanced friendship networks and active coping mediate the effect of self-help groups on substance abuse? Ann. Behav. Med. 1999, 21, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Thompson, G. A meaning-centered therapy for addictions. Int. J. Ment. Health Addict. 2012, 10, 428–440. [Google Scholar] [CrossRef]
- Lyons, G.C.B.; Deane, F.P.; Kelly, P.J. Forgiveness and purpose in life as spiritual mechanisms of recovery from substance use disorders. Addict. Res. Theory 2010, 18, 528–543. [Google Scholar] [CrossRef]
- Schnell, T. The Sources of Meaning and Meaning in Life Questionnaire (SoMe): Relations to demographics and well-being. J. Posit. Psychol. 2009, 4, 483–499. [Google Scholar] [CrossRef]
- Sørensen, T.; la Cour, P.; Danbolt, L.J.; Stifoss-Hanssen, H.; Lien, L.; DeMarinis, V.; Pedersen, H.F.; Schnell, T. The sources of meaning and meaning in life questionnaire in the Norwegian context: Relations to mental health, quality of life, and self-efficacy. Int. J. Psychol. Relig. 2019, 29, 32–45. [Google Scholar] [CrossRef]
- Neff, J.A.; MacMaster, S.A. Spiritual mechanisms underlying substance abuse behavior change in faith-based substance abuse treatment. J. Soc. Work. Pract. Addict. 2005, 5, 33–54. [Google Scholar] [CrossRef]
- Bandura, A. Prentice-Hall Series in Social Learning Theory. Social Foundations of Thought and Action: A Social Cognitive Theory; National Institute of Mental Health: Bethesda, MD, USA; Prentice-Hall, Inc.: Hoboken, NJ, USA, 1986.
- McIntosh, D.N. Religion-as-schema, with implications for the relation between religion and coping. Int. J. Psychol. Relig. 1995, 5, 1–16. [Google Scholar] [CrossRef]
- Silberman, I. Religion as a meaning system: Implications for the new millennium. J. Soc. Issues 2005, 61, 641–663. [Google Scholar] [CrossRef]
- Emmons, R.A. The Psychology of Ultimate Concerns: Motivation and Spirituality in Personality; Guilford Press: New York, NY, USA, 1999. [Google Scholar]
- Pargament, K.I. The Psychology of Religion and Coping: Theory, Research, Practice; Guilford Press: New York, NY, USA, 1997. [Google Scholar]
- Steger, M.F.; Frazier, P.; Oishi, S.; Kaler, M. The meaning in life questionnaire: Assessing the presence of and search for meaning in life. J. Couns. Psychol. 2006, 53, 80–93. [Google Scholar] [CrossRef]

{kind=link}
| Classification | Percentage or Mean | |
|---|---|---|
| Gender | Men | 73.9% |
| Women | 26.1% | |
| Age | 46.1 years | |
| Education | Elementary education | 5.8 |
| Occupational education | 29% | |
| High school education | 46.4% | |
| University education | 18.8% |
| PANAS Positive | PANAS Negative | PIL | HHI | AAI | Quantity of Steps | Frequency of AA Attendance | Frequency of Being Chairman | Abstinence Duration | Duration of AA Participation | |
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | 21.47 | 21.37 | 108.14 | 38.54 | 3.77 | 6.96 | 100.31 | 7.97 | 76.04 | 102.76 |
| Standard deviation | 4.42 | 7.39 | 14.84 | 4.57 | 1.42 | 4.65 | 66.53 | 10.3 | 63.42 | 71.38 |
| Skewness | −0.46 | 0.76 | −0.88 | −0.01 | −0.53 | −0.07 | 1.05 | 1.83 | 0.88 | 0.73 |
| Kurtosis | 0.65 | 0.03 | 0.96 | −0.73 | 0.47 | −1.78 | 1.06 | 3.15 | −0.9 | 0.9 |
| Minimum | 7 | 5 | 66 | 29 | 0 | 0 | 5 | 0 | 1 | 1 |
| Maximum | 30 | 41 | 134 | 47 | 6 | 12 | 100 | 40 | 245 | 312 |
| Reliability | 0.90 | 0.78 | 0.79 | 0.80 | - | - | - |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | |
|---|---|---|---|---|---|---|---|
| 1. Life satisfaction | |||||||
| 2. Positive affect | 0.35 ** | ||||||
| 3. Negative affect | −0.24 * | −0.28 * | |||||
| 4. Meaning in life | 0.46 ** | 0.46 ** | −0.52 ** | ||||
| 5. Hope | 0.40 ** | 0.50 ** | −0.33 ** | 0.57 ** | |||
| 6. AA aliffiation | 0.23 | 0.23 * | −0.24 * | 0.36 ** | 0.26 * | ||
| 7. Frequency of AA attendance | 0.07 | 0.09 | −0.10 | 0.19 | 0.16 | 0.30 * | |
| 8. Frequency of being chairman | 0.16 | 0.01 | −0.03 | 0.20 | 0.20 | 0.20 * | 0.46 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wnuk, M. The Beneficial Role of Involvement in Alcoholics Anonymous for Existential and Subjective Well-Being of Alcohol-Dependent Individuals? The Model Verification. Int. J. Environ. Res. Public Health 2022, 19, 5173. https://doi.org/10.3390/ijerph19095173
Wnuk M. The Beneficial Role of Involvement in Alcoholics Anonymous for Existential and Subjective Well-Being of Alcohol-Dependent Individuals? The Model Verification. International Journal of Environmental Research and Public Health. 2022; 19(9):5173. https://doi.org/10.3390/ijerph19095173
Chicago/Turabian StyleWnuk, Marcin. 2022. "The Beneficial Role of Involvement in Alcoholics Anonymous for Existential and Subjective Well-Being of Alcohol-Dependent Individuals? The Model Verification" International Journal of Environmental Research and Public Health 19, no. 9: 5173. https://doi.org/10.3390/ijerph19095173
APA StyleWnuk, M. (2022). The Beneficial Role of Involvement in Alcoholics Anonymous for Existential and Subjective Well-Being of Alcohol-Dependent Individuals? The Model Verification. International Journal of Environmental Research and Public Health, 19(9), 5173. https://doi.org/10.3390/ijerph19095173