Development of an Ultraviolet-C Irradiation Room in a Public Portuguese Hospital for Safe Re-Utilization of Personal Protective Respirators

 ,
,  ,
,  ,
, 
 ,
,  ,
,  , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Respirators and Measurement Equipment
2.2. Antiviral and Antibacterial Assays
2.2.1. Virus
2.2.2. Bacteria
2.2.3. Culture Media, Buffers, and Culture Conditions
2.2.4. Antiviral Evaluation
2.2.5. Antibacterial Evaluation
2.2.6. Software
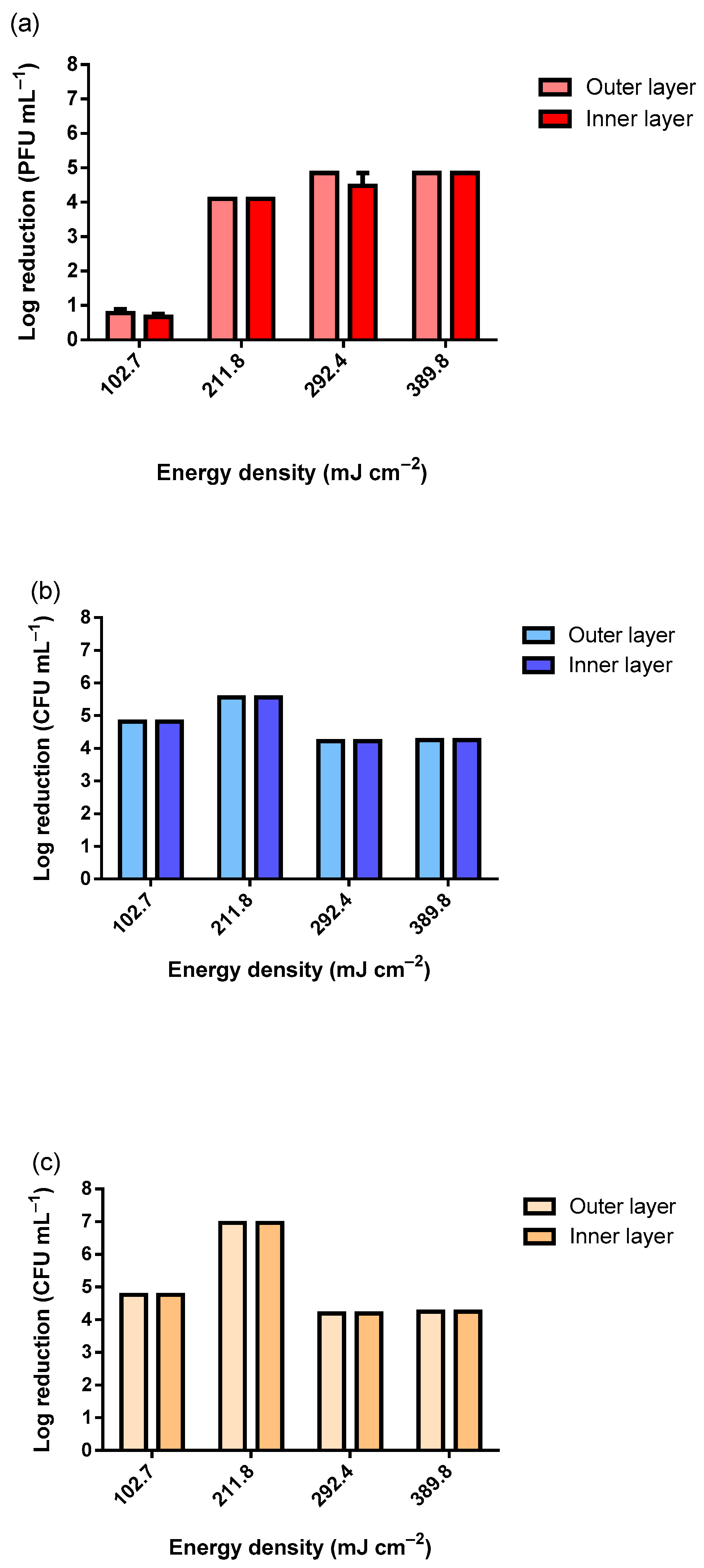
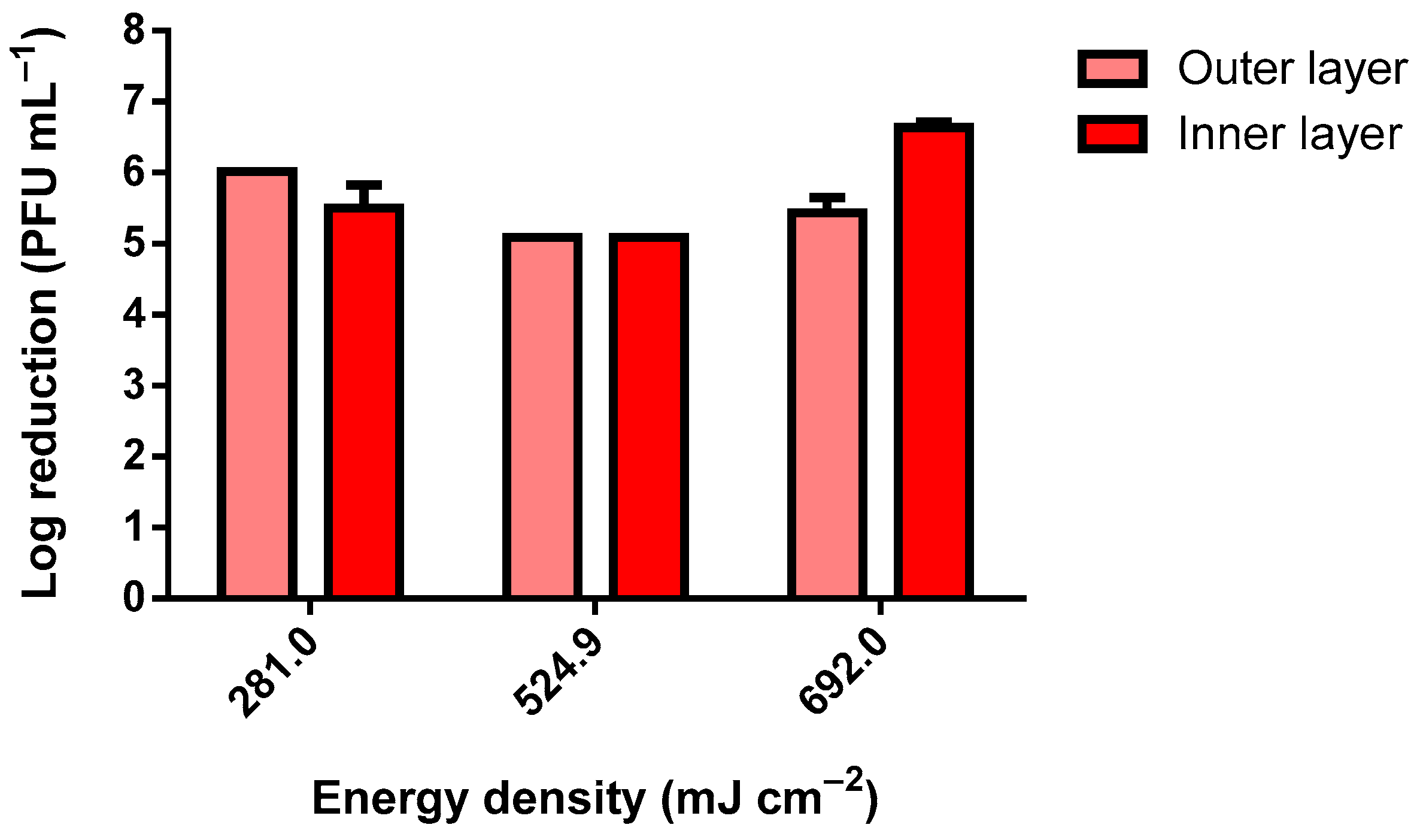
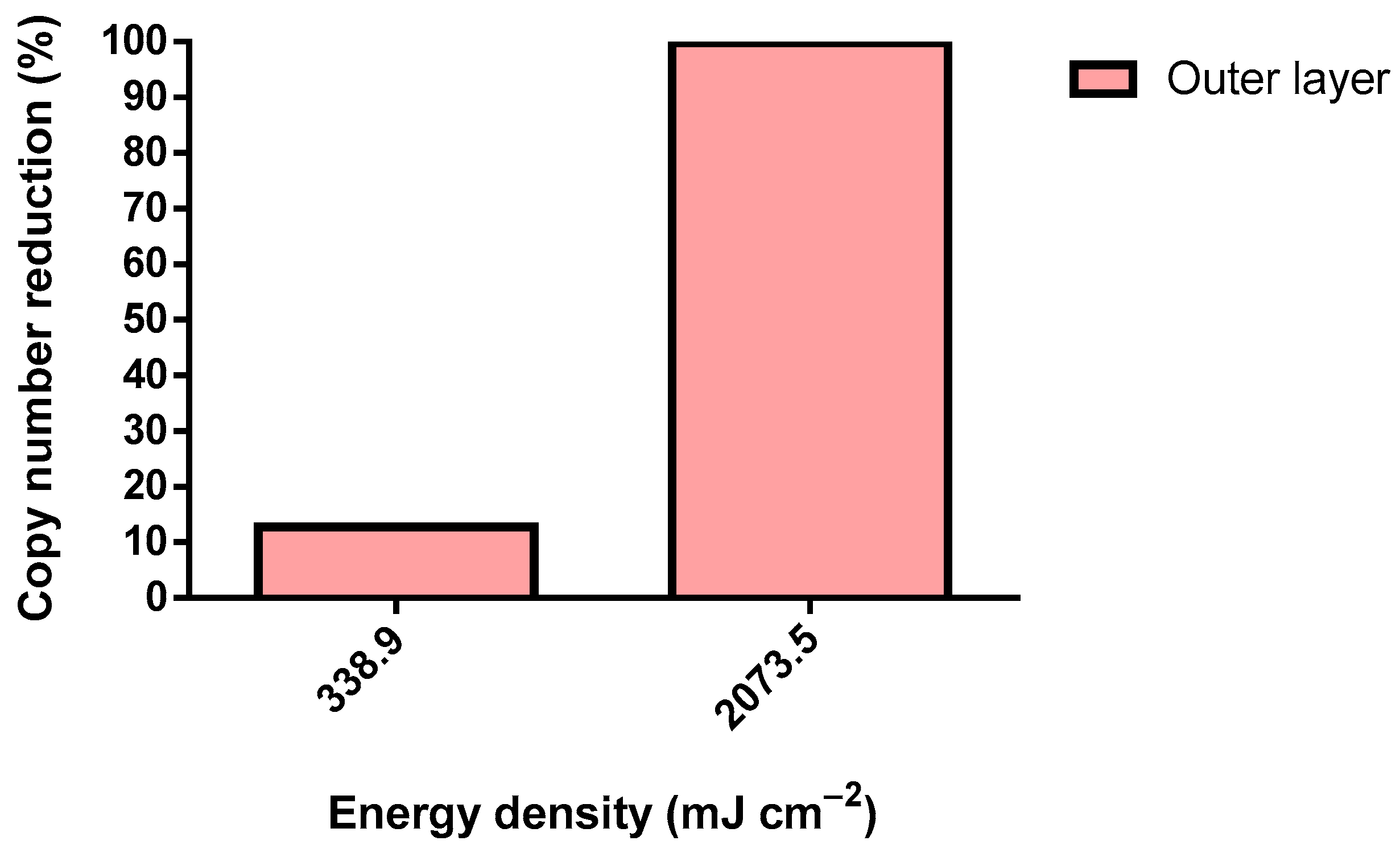
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| +ss | positive sense single stranded |
| AATCC | Textile Chemists and Colorists |
| ATCC | American Type Culture Collection |
| ATCC | American Type Culture Collection |
| CFU | colony-forming units |
| CP | coating proteins |
| Cq | quantification cycle |
| DNA | deoxyribonucleic acid |
| E | envelope proteins |
| ICU | intensive care unit |
| ISO | International Organization for Standardization (ISO) |
| M | membrane |
| N | nucleocapsid proteins |
| PBS | phosphate buffer saline |
| PFU | plaque forming units PFU |
| PP | polypropylene |
| PPE | personal protective equipment |
| RNA | ribonucleic acid |
| RT-qPCR | quantitative real-time polymerase chain reaction |
| S | spike proteins |
| SARS-CoV-2 | severe acute respiratory syndrome coronavirus 2 |
| TSA | tryptic soy agar |
| UV | ultra-violet |
References
- Kobayashi, L.M.; Marins, B.R.; dos Santos Costa, P.C.; Perazzo, H.; Castro, R. Extended use or reuse of N95 respirators during COVID-19 pandemic: An overview of national regulatory authority recommendations. Infect. Control Hosp. Epidemiol. 2020, 41, 1364–1366. [Google Scholar] [CrossRef] [PubMed]
- Heimbuch, B.K.; Wallace, W.H.; Kinney, K.; Lumley, A.E.; Wu, C.-Y.; Woo, M.-H.; Wander, J.D. A pandemic influenza preparedness study: Use of energetic methods to decontaminate filtering facepiece respirators contaminated with H1N1 aerosols and droplets. Am. J. Infect. Control 2011, 39, e1–e9. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.; Hemmatian, T.; Song, E.; Lee, K.; Seo, D.; Yi, J.; Kim, J. Disinfection treatments of disposable respirators influencing the bactericidal/bacteria removal efficiency, filtration performance, and structural integrity. Polymers 2021, 13, 45. [Google Scholar] [CrossRef] [PubMed]
- Lore, M.B.; Heimbuch, B.K.; Brown, T.L.; Wander, J.D.; Hinrichs, S.H. Effectiveness of three decontamination treatments against influenza virus applied to filtering facepiece respirators. Ann. Occup. Hyg. 2011, 56, 92–101. [Google Scholar] [CrossRef] [PubMed]
- Vo, E.; Rengasamy, S.; Shaffer, R. Development of a test system to evaluate procedures for decontamination of respirators containing viral droplets. Appl. Environ. Microbiol. 2009, 75, 7303–7309. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Chu, D.K.; Akl, E.A.; Duda, S.; Solo, K.; Yaacoub, S.; Schünemann, H.J.; El-harakeh, A.; Bognanni, A.; Lotfi, T.; Loeb, M.; et al. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: A systematic review and meta-analysis. Lancet 2020, 395, 1973–1987. [Google Scholar] [CrossRef]
- OWD. Our World in Data: Coronavirus (COVID-19) Vaccinations. Available online: https://ourworldindata.org/covid-vaccinations (accessed on 5 April 2022).
- WHO. Vaccine Efficacy, Effectiveness and Protection. Available online: https://www.who.int/news-room/feature-stories/detail/vaccine-efficacy-effectiveness-and-protection (accessed on 5 April 2022).
- Nicolau, T.; Filho, N.G.; Zille, A. Ultraviolet-C as a viable reprocessing method for disposable masks and filtering facepiece respirators. Polymers 2021, 13, 801. [Google Scholar] [CrossRef]
- Ranney, M.L.; Griffeth, V.; Jha, A.K. Critical supply shortages—The need for ventilators and personal protective equipment during the COVID-19 Pandemic. N. Engl. J. Med. 2020, 382, e41. [Google Scholar] [CrossRef]
- Mahanta, N.; Saxena, V.; Pandey, L.M.; Batra, P.; Dixit, U.S. Performance study of a sterilization box using a combination of heat and ultraviolet light irradiation for the prevention of COVID-19. Environ. Res. 2021, 198, 111309. [Google Scholar] [CrossRef]
- Benson, N.U.; Bassey, D.E.; Palanisami, T. COVID pollution: Impact of COVID-19 pandemic on global plastic waste footprint. Heliyon 2021, 7, e06343. [Google Scholar] [CrossRef]
- Kvale, K.; Prowe, A.E.F.; Chien, C.T.; Landolfi, A.; Oschlies, A. The global biological microplastic particle sink. Sci. Rep. 2020, 10, 16670. [Google Scholar] [CrossRef] [PubMed]
- Harussani, M.M.; Sapuan, S.M.; Khalina, A.; Rashid, U.; Tarique, J. Slow pyrolysis of disinfected COVID-19 non-woven polypropylene (PP) waste. In Proceedings of the International Symposium on Applied Sciences and Engineering ISASE 2021, Erzurum, Turkey, 9 March 2021; pp. 310–312. [Google Scholar]
- Nagy, Á.; Kuti, R. The environmental impact of plastic waste incineration. AARMS—Acad. Appl. Res. Mil. Public Manag. Sci. 2016, 15, 231–237. [Google Scholar] [CrossRef]
- Hinton, D.M. Emergency Use Authorization (EUA) for the Emergency Use of Stryker Instrument’s Sterizone VP4 Sterilizer; FDA: Silver Spring, MA, USA, 2020; pp. 1–8.
- Hinton, D.M. Emergency Use Authorization (EUA) for the Emergency Use of the Advanced Sterilization Products, Inc. (ASP) STERRAD 100S, NX, and 100NX Sterilization Systems1 (hereafter “ASP STERRAD Sterilization Systems”) for Use in Decontaminating Compatible N95 or N95-Equivalent Respirators; FDA: Silver Spring, MA, USA, 2020; pp. 1–8.
- Hinton, D.M. Emergency Use Authorization (EUA) for the Emergency Use of the Battelle CCDS Critical Care Decontamination System; FDA: Silver Spring, MA, USA, 2020; pp. 1–8.
- Hinton, D.M. Emergency Use Authorization (EUA) for the Emergency Use of the STERIS V-PRO 1 Plus, maX, and maX2 Low Temperature Sterilization Systems1 (Hereafter “STERIS Sterilization Systems”) for Use in Decontaminating Compatible N95 or N95-Equivalent Respirators; FDA: Silver Spring, MA, USA, 2020; pp. 1–8.
- Derraik, J.G.B.; Anderson, W.A.; Connelly, E.A.; Anderson, Y.C. Rapid review of SARS-CoV-1 and SARS-CoV-2 viability, susceptibility to treatment, and the disinfection and reuse of PPE, particularly filtering facepiece respirators. Int. J. Environ. Res. Public Health 2020, 17, 6117. [Google Scholar] [CrossRef] [PubMed]
- Sabino, C.P.; Ball, A.R.; Baptista, M.S.; Dai, T.; Hamblin, M.R.; Ribeiro, M.S.; Santos, A.L.; Sellera, F.P.; Tegos, G.P.; Wainwright, M. Light-based technologies for management of COVID-19 pandemic crisis. J. Photochem. Photobiol. B Biol. 2020, 212, 111999. [Google Scholar] [CrossRef] [PubMed]
- Kowalski, W. Ultraviolet Germicidal Irradiation Handbook, 1st ed.; Springer: Berlin, Germany, 2009. [Google Scholar]
- Livingston, E.; Desai, A.; Berkwits, M. Sourcing personal protective equipment during the COVID-19 pandemic. JAMA 2020, 323, 1912–1914. [Google Scholar] [CrossRef]
- Jeon, M.-J.; Ha, J.-W. Efficacy of UV-A, UV-B, and UV-C irradiation on inactivation of foodborne pathogens in different neutralizing buffer solutions. LWT 2018, 98, 591–597. [Google Scholar] [CrossRef]
- ISO 21348:2007; Space Environment (Natural and Artificial)—Process for Determining Solar Irradiances. ISO: Geneva, Switzerland, 2007; p. 12.
- Deng, L.-Z.; Mujumdar, A.S.; Pan, Z.; Vidyarthi, S.K.; Xu, J.; Zielinska, M.; Xiao, H.-W. Emerging chemical and physical disinfection technologies of fruits and vegetables: A comprehensive review. Crit. Rev. Food Sci. Nutr. 2020, 60, 2481–2508. [Google Scholar] [CrossRef]
- Singh, H.; Bhardwaj, S.K.; Khatri, M.; Kim, K.-H.; Bhardwaj, N. UVC radiation for food safety: An emerging technology for the microbial disinfection of food products. Chem. Eng. J. 2021, 417, 128084. [Google Scholar] [CrossRef]
- Chatzisymeon, E.; Droumpali, A.; Mantzavinos, D.; Venieri, D. Disinfection of water and wastewater by UV-A and UV-C irradiation: Application of real-time PCR method. Photochem. Photobiol. Sci. 2011, 10, 389–395. [Google Scholar] [CrossRef]
- Ubomba-Jaswa, E.; Navntoft, C.; Polo-López, M.I.; Fernandez-Ibáñez, P.; McGuigan, K.G. Solar disinfection of drinking water (SODIS): An investigation of the effect of UV-A dose on inactivation efficiency. Photochem. Photobiol. Sci. 2009, 8, 587–595. [Google Scholar] [CrossRef]
- Lakretz, A.; Ron, E.Z.; Mamane, H. Biofouling control in water by various UVC wavelengths and doses. Biofouling 2010, 26, 257–267. [Google Scholar] [CrossRef] [PubMed]
- Dias, D.F.C.; von Sperling, M. Solar radiation (PAR, UV-A, UV-B) penetration in a shallow maturation pond operating in a tropical climate. Water Sci. Technol. 2017, 76, 182–191. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.-K.; Kang, D.-H.; Schottel, J.L. UVC LED Irradiation Effectively Inactivates Aerosolized Viruses, Bacteria, and Fungi in a Chamber-Type Air Disinfection System. Appl. Environ. Microbiol. 2018, 84, e00944-18. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, S.; Zhao, X.; Manay, A.; Chen, Q. Effective ventilation and air disinfection system for reducing coronavirus disease 2019 (COVID-19) infection risk in office buildings. Sustain. Cities Soc. 2021, 75, 103408. [Google Scholar] [CrossRef]
- Linnes, J.C.; Rudnick, S.N.; Hunt, G.M.; McDevitt, J.J.; Nardell, E.A. Eggcrate UV: A whole ceiling upper-room ultraviolet germicidal irradiation system for air disinfection in occupied rooms. Indoor Air 2014, 24, 116–124. [Google Scholar] [CrossRef]
- Aljamali, N.M.; Abdullabass, H.K.; Jawad, A.M.; Alfatlawi, I.O.; Jawd, S.M. Review on types of automatic sterilization systems in Hospitals. Int. J. Ind. Biotechnol. Biomater. 2020, 6, 15–21. [Google Scholar]
- Guettari, M.; Gharbi, I.; Hamza, S. UVC disinfection robot. Environ. Sci. Pollut. Res. 2021, 28, 40394–40399. [Google Scholar] [CrossRef]
- Adams, R.L.P.; Knowler, J.T.; Leader, D.P. The Biochemistry of the Nucleic Acids; Springer Science & Business Media: Berlin, Germany, 1992. [Google Scholar]
- Gršković, B.; Zrnec, D.; Popović, M.; Petek, M.J.; Primorac, D.; Mršić, G. Effect of ultraviolet C radiation on biological samples. Croat. Med. J. 2013, 54, 263–271. [Google Scholar] [CrossRef]
- Meinhardt, M.; Krebs, R.; Anders, A.; Heinrich, U.; Tronnier, H. Wavelength-dependent penetration depths of ultraviolet radiation in human skin. J. Biomed. Opt. 2008, 13, 044030. [Google Scholar] [CrossRef]
- Kvam, E.; Benner, K. Mechanistic insights into UV-A mediated bacterial disinfection via endogenous photosensitizers. J. Photochem. Photobiol. B Biol. 2020, 209, 111899. [Google Scholar] [CrossRef]
- Fisher, E.M.; Shaffer, R.E. A method to determine the available UV-C dose for the decontamination of filtering facepiece respirators. J. Appl. Microbiol. 2011, 110, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Klemeš, J.J.; Fan, Y.V.; Jiang, P. The energy and environmental footprints of COVID-19 fighting measures—PPE, disinfection, supply chains. Energy 2020, 211, 118701. [Google Scholar] [CrossRef] [PubMed]
- Domingues, J.M.; Teixeira, M.O.; Teixeira, M.A.; Freitas, D.; Silva, S.F.d.; Tohidi, S.D.; Fernandes, R.D.V.; Padrão, J.; Zille, A.; Silva, C.; et al. Inhibition of Escherichia virus MS2, surrogate of SARS-CoV-2, via essential oils-loaded electrospun fibrous mats: Increasing the multifunctionality of antivirus protection masks. Pharmaceutics 2022, 14, 303. [Google Scholar] [CrossRef] [PubMed]
- Azeredo, J.; Sillankorva, S.; Pires, D.P. Pseudomonas bacteriophage isolation and production. In Pseudomonas Methods and Protocols; Filloux, A., Ramos, J.-L., Eds.; Humana Press: New York, NY, USA, 2014; pp. 23–32. [Google Scholar]
- Carvalho-Correia, E.; Calçada, C.; Branca, F.; Estévez-Gómez, N.; De Chiara, L.; Varela, N.; Gallego-García, P.; Posada, D.; Sousa, H.; Sousa, J.; et al. OmniSARS2: A highly sensitive and specific RT-qPCR-based COVID-19 diagnostic method designed to withstand SARS-CoV-2 lineage evolution. Biomedicines 2021, 9, 1314. [Google Scholar] [CrossRef]
- Lin, Y.-C.; Malott, R.J.; Ward, L.; Kiplagat, L.; Pabbaraju, K.; Gill, K.; Berenger, B.M.; Hu, J.; Fonseca, K.; Noyce, R.; et al. Detection and quantification of infectious Severe Acute Respiratory Coronavirus-2 in diverse clinical and environmental samples from infected patients: Evidence to support respiratory droplet, and direct and indirect contact as significant modes of transmission. Sci. Rep. 2021, 12, 5418. [Google Scholar] [CrossRef]
- Biasin, M.; Bianco, A.; Pareschi, G.; Cavalleri, A.; Cavatorta, C.; Fenizia, C.; Galli, P.; Lessio, L.; Lualdi, M.; Tombetti, E.; et al. UV-C irradiation is highly effective in inactivating SARS-CoV-2 replication. Sci. Rep. 2021, 11, 6260. [Google Scholar] [CrossRef]
- IUA. International Ultraviolet Association Inc. Available online: https://www.iuva.org/ (accessed on 5 April 2022).
- V’kovski, P.; Kratzel, A.; Steiner, S.; Stalder, H.; Thiel, V. Coronavirus biology and replication: Implications for SARS-CoV-2. Nat. Rev. Microbiol. 2021, 19, 155–170. [Google Scholar] [CrossRef]
- Schoeman, D.; Fielding, B.C. Coronavirus envelope protein: Current knowledge. Virol. J. 2019, 16, 69. [Google Scholar] [CrossRef]
- de Souza, P.M.; Fernández, A. Rheological properties and protein quality of UV-C processed liquid egg products. Food Hydrocoll. 2013, 31, 127–134. [Google Scholar] [CrossRef]
- Lo, C.-W.; Matsuura, R.; Iimura, K.; Wada, S.; Shinjo, A.; Benno, Y.; Nakagawa, M.; Takei, M.; Aida, Y. UVC disinfects SARS-CoV-2 by induction of viral genome damage without apparent effects on viral morphology and proteins. Sci. Rep. 2021, 11, 13804. [Google Scholar] [CrossRef]
- Kuzminov, A. Pyrimidine dimers. In Brenner’s Encyclopedia of Genetics; Kuzminov, A., Ed.; Elsevier Inc.: Amsterdam, The Netherlands, 2013. [Google Scholar]
- Merriam, V.; Gordon, M.P. Pyrimidine dimer formation in ultraviolet irradiated TMV-RNA. Photochem. Photobiol. 1967, 6, 309–319. [Google Scholar] [CrossRef] [PubMed]
- Muriaux, D.; Darlix, J.-L. Properties and functions of the nucleocapsid protein in virus assembly. RNA Biol. 2010, 7, 744–753. [Google Scholar] [CrossRef] [PubMed]
- Lindsley, W.G.; Martin, S.B., Jr.; Thewlis, R.E.; Sarkisian, K.; Nwoko, J.O.; Mead, K.R.; Noti, J.D. Effects of Ultraviolet Germicidal Irradiation (UVGI) on N95 Respirator Filtration Performance and Structural Integrity. J. Occup. Environ. Hyg. 2015, 12, 509–517. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Exposure Period | |||||||
|---|---|---|---|---|---|---|---|
| Lamp Power | Distance | 5 min | 6 min | 7 min | 8 min | 9 min | 10 min |
| UV-C Energy Density (mJ cm−2) | |||||||
| 30 W | 20 cm | 207.3 | 248.8 | 290.2 | 331.7 | 373.2 | 414.6 |
| 30 cm | 164.4 | 197.3 | 230.2 | 263.1 | 296.0 | 328.9 | |
| 40 cm | 132.3 | 158.8 | 185.3 | 211.7 | 238.2 | 264.7 | |
| 50 cm | 112.8 | 135.4 | 158.0 | 180.5 | 203.1 | 225.7 | |
| 55 W | 20 cm | 269.5 | 323.4 | 377.3 | 431.2 | 485.1 | 539.0 |
| 30 cm | 198.5 | 238.2 | 277.8 | 317.5 | 357.2 | 396.9 | |
| 40 cm | 162.7 | 195.2 | 227.8 | 260.3 | 292.9 | 325.4 | |
| 50 cm | 129.4 | 155.3 | 181.1 | 207.0 | 232.9 | 258.8 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Padrão, J.; Nicolau, T.; Felgueiras, H.P.; Calçada, C.; Veiga, M.I.; Osório, N.S.; Martins, M.S.; Dourado, N.; Taveira-Gomes, A.; Ferreira, F.; et al. Development of an Ultraviolet-C Irradiation Room in a Public Portuguese Hospital for Safe Re-Utilization of Personal Protective Respirators. Int. J. Environ. Res. Public Health 2022, 19, 4854. https://doi.org/10.3390/ijerph19084854
Padrão J, Nicolau T, Felgueiras HP, Calçada C, Veiga MI, Osório NS, Martins MS, Dourado N, Taveira-Gomes A, Ferreira F, et al. Development of an Ultraviolet-C Irradiation Room in a Public Portuguese Hospital for Safe Re-Utilization of Personal Protective Respirators. International Journal of Environmental Research and Public Health. 2022; 19(8):4854. https://doi.org/10.3390/ijerph19084854
Chicago/Turabian StylePadrão, Jorge, Talita Nicolau, Helena P. Felgueiras, Carla Calçada, Maria Isabel Veiga, Nuno S. Osório, Marcos S. Martins, Nuno Dourado, António Taveira-Gomes, Fernando Ferreira, and et al. 2022. "Development of an Ultraviolet-C Irradiation Room in a Public Portuguese Hospital for Safe Re-Utilization of Personal Protective Respirators" International Journal of Environmental Research and Public Health 19, no. 8: 4854. https://doi.org/10.3390/ijerph19084854
APA StylePadrão, J., Nicolau, T., Felgueiras, H. P., Calçada, C., Veiga, M. I., Osório, N. S., Martins, M. S., Dourado, N., Taveira-Gomes, A., Ferreira, F., & Zille, A. (2022). Development of an Ultraviolet-C Irradiation Room in a Public Portuguese Hospital for Safe Re-Utilization of Personal Protective Respirators. International Journal of Environmental Research and Public Health, 19(8), 4854. https://doi.org/10.3390/ijerph19084854