
A Positive Correlation between Steroid Injections and Cuff Tendon Tears: A Cohort Study Using a Clinical Database

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
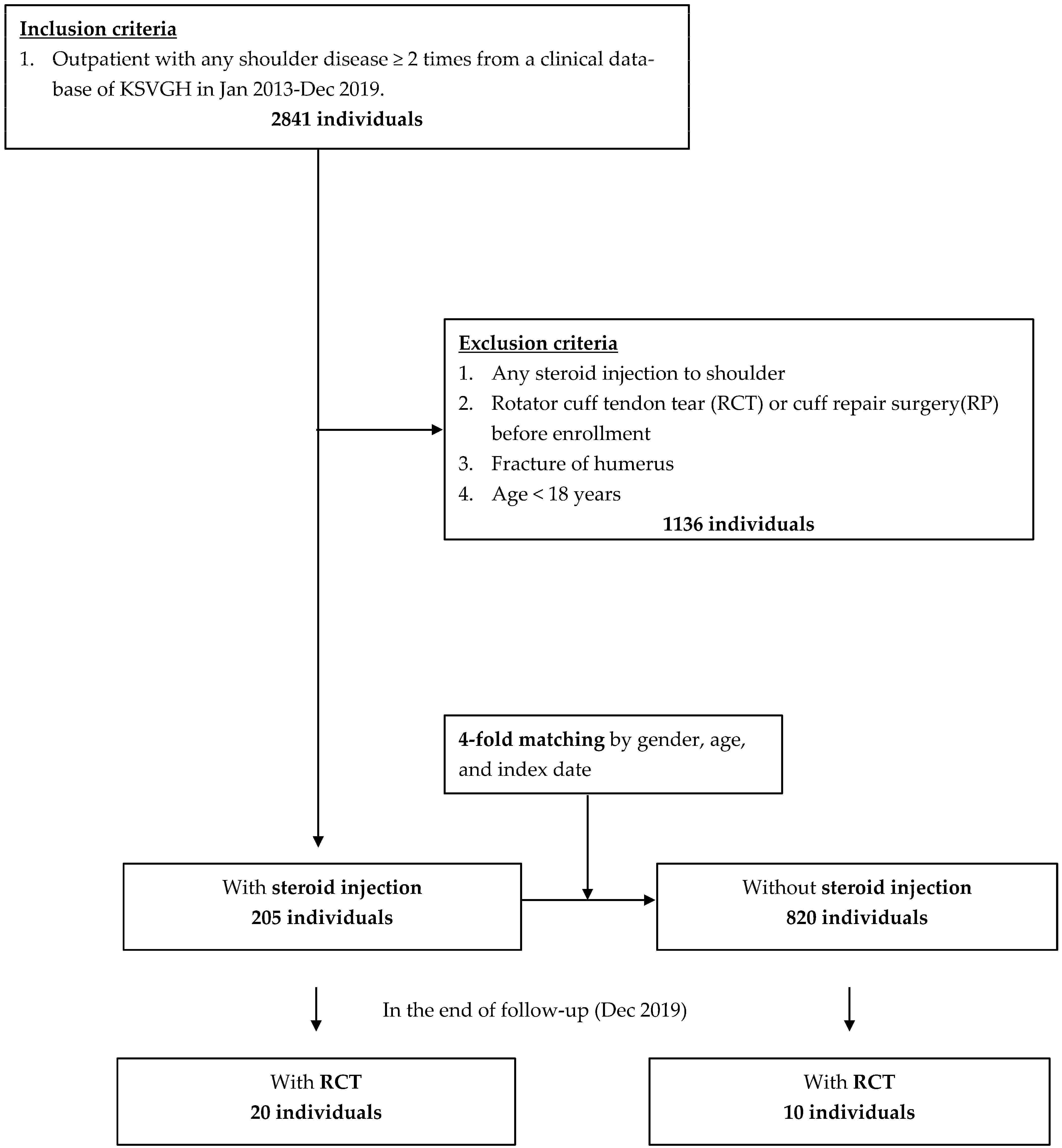
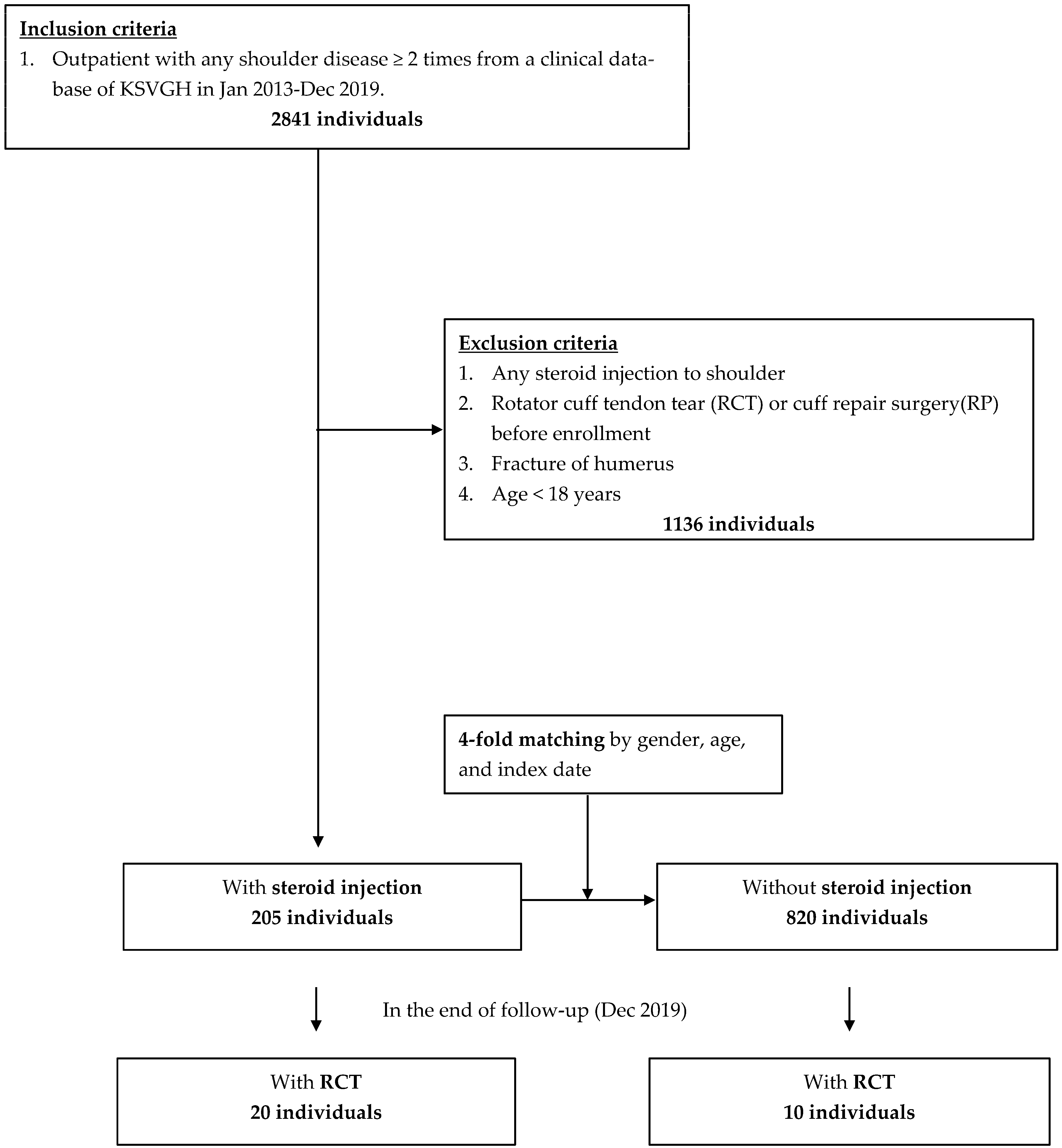
2.1. Inclusion and Exclusion Criteria
2.2. Intervention
2.3. Outcome
2.4. Comorbidities
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Buchbinder, R.; Green, S.; Youd, J.M. Corticosteroid injections for shoulder pain. Cochrane Database Syst. Rev. 2003, 2003, CD004016. [Google Scholar] [CrossRef]
- Buchbinder, R.; Green, S.; Youd, J.M.; Johnston, R.V.; Cumpston, M. Arthrographic distension for adhesive capsulitis (frozen shoulder). Cochrane Database Syst. Rev. 2008, 2008, CD007005. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.A.; Fitzgerald, P.M. Botulinum toxin for shoulder pain. Cochrane Database Syst. Rev. 2010, 2010, CD008271. [Google Scholar] [CrossRef]
- Page, M.; Green, S.E.; Kramer, S.; Johnston, R.V.; McBain, B.; Buchbinder, R. Electrotherapy modalities for adhesive capsulitis (frozen shoulder). Cochrane Database Syst. Rev. 2014, 2014, CD011324. [Google Scholar] [CrossRef] [PubMed]
- Page, M.; Green, S.E.; Kramer, S.; Johnston, R.V.; McBain, B.; Chau, M.; Buchbinder, R. Manual therapy and exercise for adhesive capsulitis (frozen shoulder). Cochrane Database Syst. Rev. 2014, 2014, CD011275. [Google Scholar] [CrossRef]
- Green, S.; Buchbinder, R.; Hetrick, S. Physiotherapy interventions for shoulder pain. Cochrane Database Syst. Rev. 2003, 2, Cd004258. [Google Scholar]
- Arroll, B.; Goodyear-Smith, F. Corticosteroid injections for painful shoulder: A meta-analysis. Br. J. Gen. Pract. 2005, 55, 224–228. [Google Scholar]
- Gialanella, B.; Prometti, P. Effects of Corticosteroids Injection in Rotator Cuff Tears. Pain Med. 2011, 12, 1559–1565. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.-T.; Yang, T.-F. Intra-substance steroid injection for full-thickness supraspinatus tendon rupture. BMC Musculoskelet. Disord. 2019, 20, 569. [Google Scholar] [CrossRef] [Green Version]
- Kim, I.B.; Jung, D.W. An Intra-articular Steroid Injection at 6 Weeks Postoperatively for Shoulder Stiffness after Arthro-scopic Rotator Cuff Repair Does Not Affect Repair Integrity. Am. J. Sports Med. 2018, 46, 2192–2202. [Google Scholar] [CrossRef]
- Kim, Y.-S.; Jin, H.-K.; Lee, H.-J.; Cho, H.-L.; Lee, W.-S.; Jang, H.-J. Is It Safe to Inject Corticosteroids into the Glenohumeral Joint after Arthroscopic Rotator Cuff Repair? Am. J. Sports Med. 2019, 47, 1694–1700. [Google Scholar] [CrossRef] [PubMed]
- Unverferth, L.J.; Olix, M.L. The effect of local steroid injections on tendon. J. Sports Med. 1973, 1, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Hugate, R.; Pennypacker, J.; Saunders, M.; Juliano, P. The effects of intratendinous and retrocalcaneal intrabursal injections of corticosteroid on the biomechanical properties of rabbit achilles tendons. J. Bone Jt. Surg. 2004, 86, 794–801. [Google Scholar] [CrossRef] [PubMed]
- Maman, E.; Yehuda, C.; Pritsch, T.; Morag, G.; Brosh, T.; Sharfman, Z.; Dolkart, O. Detrimental Effect of Repeated and Single Sub-acromial Corticosteroid Injections on the Intact and Injured Rotator Cuff: A Biomechanical and Imaging Study in Rats. Am. J. Sports Med. 2016, 44, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.K.; Ling, C.M. The response of human tendon to hydrocortisone injection. Singap. Med. J. 1975, 16, 259–262. [Google Scholar]
- Poulsen, R.C.; Watts, A.C.; Murphy, R.J.; Snelling, S.J.; Carr, A.J.; Hulley, P.A. Glucocorticoids induce senescence in primary human tenocytes by inhibition of sirtuin 1 and activation of the p53/p21 pathway: In vivo and in vitro evidence. Ann. Rheum. Dis. 2014, 73, 1405–1413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dean, B.J.; Franklin, S.L.; Murphy, R.J.; Javaid, M.K.; Carr, A.J. Glucocorticoids induce specific ion-channel-mediated toxicity in human rotator cuff tendon: A mechanism underpinning the ultimately deleterious effect of steroid injection in tendinopathy? Br. J. Sports Med. 2014, 48, 1620–1626. [Google Scholar] [CrossRef]
- Baumgarten, K.M.; Gerlach, D.; Galatz, L.M.; Teefey, S.A.; Middleton, W.D.; Ditsios, K.; Yamaguchi, K. Cigarette Smoking Increases the Risk for Rotator Cuff Tears. Clin. Orthop. Relat. Res. 2010, 468, 1534–1541. [Google Scholar] [CrossRef] [Green Version]
- Waldorff, E.I.; Lindner, J.; Kijek, T.G.; Downie, B.K.; Hughes, R.E.; Carpenter, J.E.; Miller, B.S. Bone density of the greater tuberosity is decreased in rotator cuff disease with and without full-thickness tears. J. Shoulder Elb. Surg. 2011, 20, 904–908. [Google Scholar] [CrossRef]
- Gumina, S.; Arceri, V.; Carbone, S.; Albino, P.; Passaretti, D.; Campagna, V.; Fagnani, C.; Postacchini, F. The association between arterial hypertension and rotator cuff tear: The influence on rotator cuff tear sizes. J. Shoulder Elb. Surg. 2013, 22, 229–232. [Google Scholar] [CrossRef]
- Huang, S.W.; Wu, C.W.; Lin, L.F.; Liou, T.H.; Lin, H.W. Gout Can Increase the Risk of Receiving Rotator Cuff Tear Repair Surgery. Am. J. Sports Med. 2017, 45, 2355–2363. [Google Scholar] [CrossRef] [PubMed]
- Sayampanathan, A.A.; Andrew, T.H.C. Systematic review on risk factors of rotator cuff tears. J. Orthop. Surg. 2017, 25, 2309499016684318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jancuska, J.; Matthews, J.; Miller, T.; Kluczynski, M.A.; Bisson, L.J. A Systematic Summary of Systematic Reviews on the Topic of the Rotator Cuff. Orthop. J. Sports Med. 2018, 6, 2325967118797891. [Google Scholar] [CrossRef] [Green Version]
- Bursac, Z.; Gauss, C.H.; Williams, D.K.; Hosmer, D.W. Purposeful selection of variables in logistic regression. Source Code Biol. Med. 2008, 3, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tillander, B.E.; Franzén, L.; Karlsson, M.H.; Norlin, R. Effect of steroid injections on the rotator cuff: An experimental study in rats. J. Shoulder Elb. Surg. 1999, 8, 271–274. [Google Scholar] [CrossRef]
- Akpinar, S.; Hersekli, M.A.; Demirors, H.; Tandogan, R.N.; Kayaselcuk, F. Effects of methylprednisolone and betamethasone in-jections on the rotator cuff: An experimental study in rats. Adv. Ther. 2002, 19, 194–201. [Google Scholar] [CrossRef]
- Dean, B.J.; Lostis, E.; Oakley, T.; Rombach, I.; Morrey, M.E.; Carr, A.J. The risks and benefits of glucocorticoid treatment for ten-dinopathy: A systematic review of the effects of local glucocorticoid on tendon. Semin. Arthritis Rheum. 2014, 43, 570–576. [Google Scholar] [CrossRef]
- Barnes, P.J. Corticosteroid effects on cell signalling. Eur. Respir. J. 2006, 27, 413–426. [Google Scholar] [CrossRef]
- Dinhane, K.G.I.; Godoy-Santos, A.; Fabro, A.T.; Moretto, M.R.; Deprá, I.; Yoshida, W.B. Short-term Changes after Corticosteroid Injections into the Normal Tendons of Rabbits: A Controlled Randomized Study. Am. J. Sports Med. 2019, 47, 721–728. [Google Scholar] [CrossRef]
- Lee, H.-J.; Kim, Y.-S.; Ok, J.-H.; Lee, Y.-K.; Ha, M.Y. Effect of a single subacromial prednisolone injection in acute rotator cuff tears in a rat model. Knee Surg. Sports Traumatol. Arthrosc. 2013, 23, 555–561. [Google Scholar] [CrossRef]
- Jiang, Y.; Zhao, J.; van Holsbeeck, M.T.; Flynn, M.J.; Ouyang, X.; Genant, H.K. Trabecular microstructure and surface changes in the greater tuberosity in rotator cuff tears. Skelet. Radiol. 2002, 31, 522–528. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, M.; Singh, B.; Nicolaou, N.; Ravikumar, K. Correlation between Rotator Cuff Tears and Repeated Subacromial Steroid Injections: A Case-Controlled Study. Ann. R. Coll. Surg. Engl. 2009, 91, 414–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Traven, S.A.; Brinton, D.; Simpson, K.N.; Adkins, Z.; Althoff, A.; Palsis, J.; Slone, H.S. Preoperative Shoulder Injections Are Associated with Increased Risk of Revision Rotator Cuff Repair. Arthrosc. J. Arthrosc. Relat. Surg. 2019, 35, 706–713. [Google Scholar] [CrossRef] [PubMed]
- Desai, V.S.; Camp, C.L.; Boddapati, V.; Dines, J.S.; Brockmeier, S.F.; Werner, B.C. Increasing Numbers of Shoulder Corticosteroid Injections within a Year Preoperatively May Be Associated with a Higher Rate of Subsequent Revision Rotator Cuff Surgery. Arthroscopy 2019, 35, 45–50. [Google Scholar] [CrossRef]
- Watson, M. Major ruptures of the rotator cuff. The results of surgical repair in 89 patients. J. Bone Jt. Surg. Br. 1985, 67, 618–624. [Google Scholar] [CrossRef] [Green Version]
- Ramírez, J.; Pomés, I.; Cabrera, S.; Pomés, J.; Sanmartí, R.; Cañete, J.D. Incidence of full-thickness rotator cuff tear after sub-acromial corticosteroid injection: A 12-week prospective study. Mod. Rheumatol. 2014, 24, 667–670. [Google Scholar] [CrossRef]
- Neer, C.S. Impingement lesions. Clin. Orthop. Relat. Res. 1983, 1983, 70–77. [Google Scholar] [CrossRef]
- Yamanaka, K. Pathological study of the supraspinatus tendon. Nihon Seikeigeka Gakkai Zasshi 1988, 62, 1121–1138. [Google Scholar]
- Lehman, C.; Cuomo, F.; Kummer, F.J.; Zuckerman, J.D. The incidence of full thickness rotator cuff tears in a large cadaveric population. Bull. Hosp. Jt. Dis. 1995, 54, 30–31. [Google Scholar]
- Ma, C.M.; Lin, L.H.; Chen, Y.H.; Chen, H.Y.; Chiang, J.H.; Chen, W.C. Liver Governs Tendon: A Theory from Traditional Chinese Medicine-Evidence from a Population-Based Matched Cohort Study in Taiwan for the Association of Chronic Liver Disease and Common Diseases in the Chiropractic Office. Evid.-Based Complement. Altern. Med. 2016, 2016, 7210705. [Google Scholar] [CrossRef]
- Yang, Y.; Kim, D. An Overview of the Molecular Mechanisms Contributing to Musculoskeletal Disorders in Chronic Liver Disease: Osteoporosis, Sarcopenia, and Osteoporotic Sarcopenia. Int. J. Mol. Sci. 2021, 22, 2604. [Google Scholar] [CrossRef] [PubMed]
- Cadet, E.R.; Hsu, J.W.; Levine, W.N.; Bigliani, L.U.; Ahmad, C.S. The relationship between greater tuberosity osteopenia and the chronicity of rotator cuff tears. J. Shoulder Elb. Surg. 2008, 17, 73–77. [Google Scholar] [CrossRef] [PubMed]
- Dougherty, K.A.; Dilisio, M.F.; Agrawal, D.K. Vitamin D and the immunomodulation of rotator cuff injury. J. Inflamm. Res. 2016, 9, 123–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
| Variable | Total | With RCT | Without RCT | p-Value |
|---|---|---|---|---|
| n = 1025 (%) | n = 30 (%) | n = 995 (%) | ||
| Steroid injection | 205 (20) | 20 (67) | 185 (19) | <0.001 |
| Sex-Male | 411 (40) | 12 (40) | 399 (40) | 0.991 |
| Age, years (Mean ± SD) | 59.4 ± 12.5 | 62.2 ± 11.3 | 59.3 ± 12.5 | 0.200 |
| Smoking | 94 (9) | 7 (23) | 87 (9) | 0.006 |
| Alcohol use | 64 (6) | 4 (13) | 60 (6) | 0.103 |
| Comorbidity | ||||
| Thyroid disorder | 39 (4) | 2 (7) | 37 (4) | 0.406 |
| Diabetes | 132 (13) | 7 (23) | 125 (13) | 0.083 |
| Gout | 42 (4) | 4 (13) | 38 (4) | 0.010 |
| Depression | 25 (2) | 1 (3) | 24 (2) | 0.747 |
| Hypertension | 249 (24) | 13 (43) | 236 (24) | 0.014 |
| Ischemic heart disease | 127 (12) | 5 (17) | 122 (12) | 0.471 |
| Chronic liver disease | 78 (8) | 7 (23) | 71 (7) | 0.001 |
| Chronic kidney disease | 62 (6) | 2 (7) | 60 (6) | 0.885 |
| Connective tissue disease | 34 (3) | 1 (3) | 33 (3) | 0.996 |
| Osteoporosis | 47 (5) | 3 (10) | 44 (4) | 0.150 |
| Variables | Hazard Ratio (95%CI) | p Value |
|---|---|---|
| Steroid injection | 8.50 (3.98–18.16) | <0.001 |
| Sex-Male | 0.92 (0.44–1.91) | 0.817 |
| Age ≥ 65 year | 1.70 (0.83–3.48) | 0.147 |
| Smoking | 3.00 (1.29–7.00) | 0.011 |
| Alcohol use | 2.27 (0.79–6.50) | 0.128 |
| Comorbidity | ||
| Thyroid disorder | 2.07 (0.49–8.69) | 0.322 |
| Diabetes | 1.94 (0.83–4.52) | 0.125 |
| Gout | 3.63 (1.27–10.41) | 0.016 |
| Depression | 1.42 (0.19–10.40) | 0.732 |
| Hypertension | 2.49 (1.21–5.13) | 0.013 |
| Ischemic heart disease | 1.53 (0.58–3.99) | 0.389 |
| Chronic liver disease | 3.79 (1.63–8.84) | 0.002 |
| Chronic kidney disease | 1.11 (0.27–4.68) | 0.883 |
| Connective tissue disease | 1.14 (0.16–8.36) | 0.899 |
| Osteoporosis | 2.30 (0.70–7.58) | 0.172 |
| Variables | Adjusted Hazard Ratio (95% CI) | p Value |
|---|---|---|
| Steroid injection | 7.44 (3.45–16.00) | <0.001 |
| Smoking | 2.40 (1.02–5.66) | 0.046 |
| Chronic liver disease | 3.25 (1.38–7.63) | 0.007 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, C.-Y.; Huang, S.-C.; Tzou, S.-J.; Yin, C.-H.; Chen, J.-S.; Chen, Y.-S.; Chang, S.-T. A Positive Correlation between Steroid Injections and Cuff Tendon Tears: A Cohort Study Using a Clinical Database. Int. J. Environ. Res. Public Health 2022, 19, 4520. https://doi.org/10.3390/ijerph19084520
Lin C-Y, Huang S-C, Tzou S-J, Yin C-H, Chen J-S, Chen Y-S, Chang S-T. A Positive Correlation between Steroid Injections and Cuff Tendon Tears: A Cohort Study Using a Clinical Database. International Journal of Environmental Research and Public Health. 2022; 19(8):4520. https://doi.org/10.3390/ijerph19084520
Chicago/Turabian StyleLin, Ching-Yueh, Shih-Chung Huang, Shiow-Jyu Tzou, Chun-Hao Yin, Jin-Shuen Chen, Yao-Shen Chen, and Shin-Tsu Chang. 2022. "A Positive Correlation between Steroid Injections and Cuff Tendon Tears: A Cohort Study Using a Clinical Database" International Journal of Environmental Research and Public Health 19, no. 8: 4520. https://doi.org/10.3390/ijerph19084520
APA StyleLin, C.-Y., Huang, S.-C., Tzou, S.-J., Yin, C.-H., Chen, J.-S., Chen, Y.-S., & Chang, S.-T. (2022). A Positive Correlation between Steroid Injections and Cuff Tendon Tears: A Cohort Study Using a Clinical Database. International Journal of Environmental Research and Public Health, 19(8), 4520. https://doi.org/10.3390/ijerph19084520