
Health-Related Quality of Life by Gulf War Illness Case Status

 , ,
, ,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Measures
2.2.1. Gulf War Illness
2.2.2. Health-Related Quality of Life (HRQOL)
2.2.3. Sleep Disturbance
2.2.4. Post-Traumatic Stress Disorder (PTSD)
2.2.5. Depressive Symptoms and Depression
2.2.6. Pain
2.2.7. Demographic and Military Characteristics
2.3. Analysis
3. Results
3.1. Sample Description
3.2. Correlations among HRQOL and Indices of Health
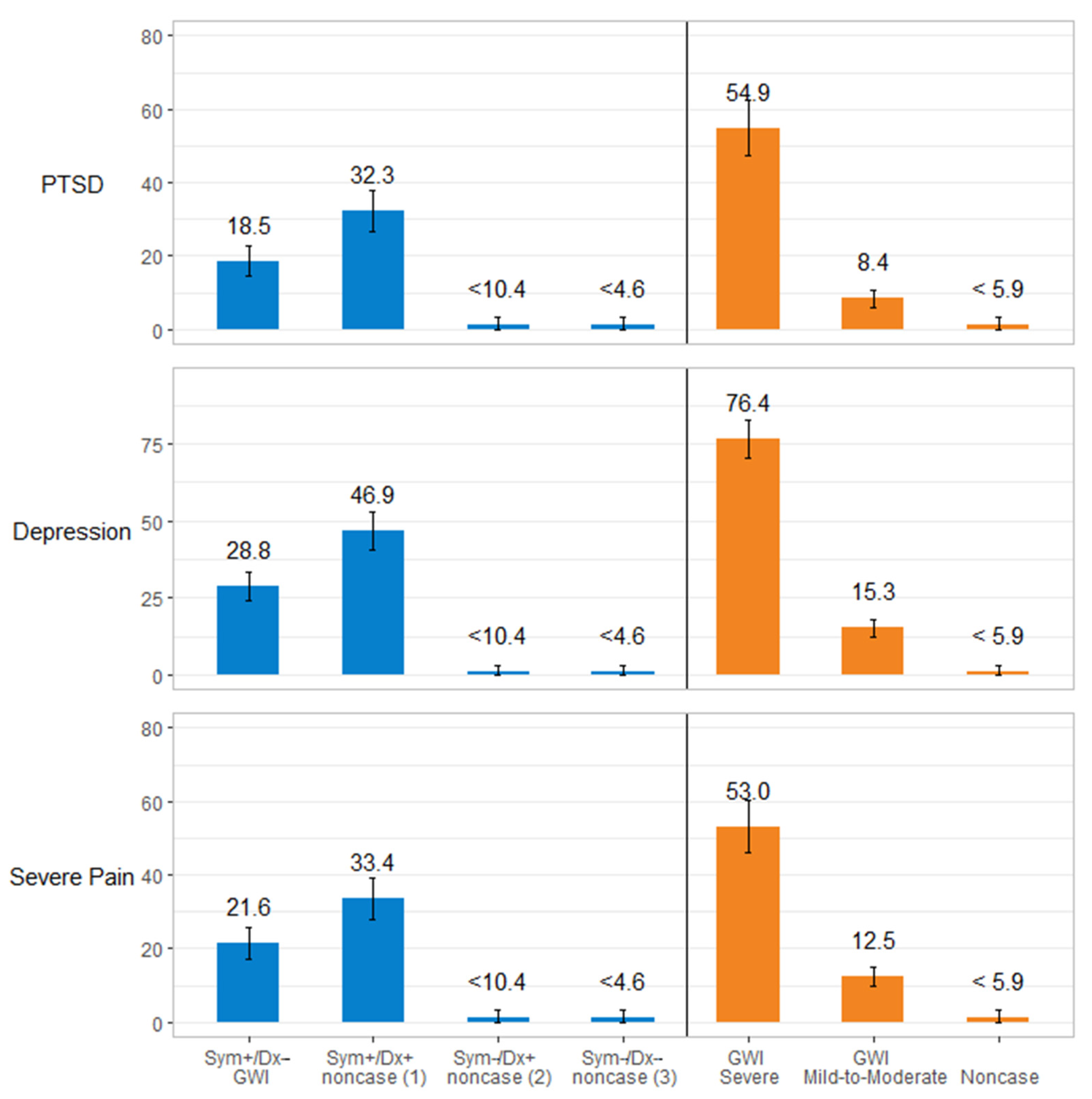
3.3. Association of Gulf War Illness Case Status with Health-Related Quality of Life, Sleep Disturbance, PTSD, Depression, and Pain Measures
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fukuda, K.; Nisenbaum, R.; Stewart, G.; Thompson, W.W.; Robin, L.; Washko, R.M.; Noah, D.L.; Barrett, D.H.; Randall, B.; Herwaldt, B.L.; et al. Chronic multisymptom illness affecting Air Force veterans of the Gulf War. JAMA 1998, 280, 981–988. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Chronic Multisymptom Illness in Gulf War Veterans: Case Definitions Reexamined; The National Academics Press: Washington, DC, USA, 2014. [Google Scholar]
- The Iowa Persian Gulf Study Group. Self-reported Illness and health status Among Gulf War Veterans: A population-based study. JAMA 1997, 277, 238–245. [Google Scholar] [CrossRef]
- Proctor, S.P.; Harley, R.; Wolfe, J.; Heeren, T.; White, R.F. Health-related quality of life in Persian Gulf War veterans. Mil. Med. 2001, 106, 510–519. [Google Scholar] [CrossRef]
- Toomey, R.; Kang, H.K.; Karlinsky, J.; Baker, D.G.; Vasterling, J.J.; Alpern, R.; Reda, D.J.; Henderson, W.G.; Murphy, F.M.; Eisen, S.A. Mental health of US Gulf War veterans 10 years after the war. Br. J. Psychiatry 2007, 190, 385–393. [Google Scholar] [CrossRef]
- Wright, B.K.; Kelsall, H.L.; Sim, M.R.; Clarke, D.M. Quality of Life in Gulf War Veterans: The Influence of Recency and Persistence of Psychiatric Morbidity. Appl. Res. Qual. Life 2019, 14, 23–38. [Google Scholar] [CrossRef]
- Barrett, D.H.; Doebbeling, C.C.; Schwartz, D.A.; Voelker, M.D.; Falter, K.H.; Woolson, R.F.; Doebbeling, B.N. Posttraumatic stress disorder and self-reported physical health status among U.S. Military personnel serving during the Gulf War period: A population-based study. Psychosomatics 2002, 43, 195–205. [Google Scholar] [CrossRef] [PubMed]
- McKenzie, D.P.; Ikin, J.F.; McFarlane, A.C.; Creamer, M.; Forbes, A.B.; Kelsall, H.L.; Glass, D.C.; Ittak, P.; Sim, M.R. Psychological health of Australian veterans of the 1991 Gulf War: An assessment using the SF-12, GHQ-12 and PCL-S. Psychol. Med. 2004, 34, 1419–1430. [Google Scholar] [CrossRef]
- Hotopf, M.; David, A.S.; Hull, L.; Nikalaou, V.; Unwin, C.; Wessely, S. Gulf war illness—Better, worse, or just the same? A cohort study. BMJ 2003, 327, 1370. [Google Scholar] [CrossRef] [PubMed]
- Voelker, M.D.; Saag, K.G.; Schwartz, D.A.; Chrischilles, E.; Clarke, W.R.; Woolson, R.F.; Doebbeling, B.N. Health-related Quality of Life in Gulf War Era Military Personnel. Am. J. Epidemiol. 2002, 155, 899–907. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.K.; Li, B.; Mahan, C.M.; Eisen, S.A.; Engel, C.C. Health of US veterans of 1991 Gulf War: A follow-up survey in 10 years. J. Occup. Environ. 2009, 51, 401–410. [Google Scholar] [CrossRef]
- Unwin, C.; Blatchley, N.; Coker, W.; Ferry, S.; Hotopf, M.; Hull, L.; Ismail, K.; Palmer, I.; David, A.; Wessely, S. Health of UK servicemen who served in Persian Gulf War. Lancet 1999, 353, 169–178. [Google Scholar] [CrossRef]
- Kelsall, H.L.; McKenzie, D.P.; Sim, M.R.; Leder, K.; Forbes, A.B.; Dwyer, T. Physical, psychological, and functional comorbidities of multisymptom illness in Australian male veterans of the 1991 Gulf War. Am. J. Epidemiol. 2009, 170, 1048–1056. [Google Scholar] [CrossRef] [PubMed]
- Testa, M.A.; Simonsson, D.C. Assessment of quality-of-life outcomes. N. Engl. J. Med. 1996, 334, 835–840. [Google Scholar] [CrossRef] [PubMed]
- Kazis, L.E. The Veterans SF-36 Health Status Questionnaire: Development and Application in the Veterans Health Administration. Med. Outcomes Trust. Monit. 2000, 5, 1–18. [Google Scholar]
- Kazis, L.E.; Miller, D.R.; Skinner, K.M.; Lee, A.; Ren, X.S.; Clark, J.A.; Rogers, W.H.; Spiro, A., III; Selim, A.; Linzer, M.; et al. Patient-Reported Measures of Health: The Veterans Health Study. J. Ambul. Care Manag. 2004, 27, 70–83. [Google Scholar] [CrossRef] [PubMed]
- Wilson, I.B.; Cleary, P.D. Linking clinical variables with health-related quality of life: A conceptual model of patient outcomes. JAMA 1995, 273, 59–65. [Google Scholar] [CrossRef]
- Ware, J.E.; Kosinksi, M.; Keller, S.D. A 12-item short-form health survey: Construction of scales and preliminary tests of reliability and validity. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36): I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.A.; Borowsky, S.J.; Nugent, S.; Murdoch, M.; Zhao, Y.; Nelson, D.B.; Petzel, R.; Nichol, K.L. Health-related quality of life, functional impairment, and healthcare utilization by veterans: Veterans’ Quality of Life Study. J. Am. Geriatr. Soc. 2005, 53, 108–113. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.A.; Nelson, D.B.; Nichol, K.L. Recent health-related quality of life, but not change, predicted mortality and healthcare utilization. J. Clin. Epidemiol. 2021, 140, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Blanchard, M.S.; Eisen, S.A.; Alpern, R.; Karlinsky, J.; Toomey, R.; Reda, D.J.; Murphy, F.M.; Jackson, L.W.; Kang, H.K. Chronic multisymptom illness complex in Gulf War I veterans 10 years later. Am. J. Epidemiol. 2006, 163, 66–75. [Google Scholar] [CrossRef] [PubMed]
- Wallin, M.T.; Wilken, J.; Alfaro, M.H.; Rogers, C.; Mahan, C.; Chapman, J.C.; Fratto, T.; Sullivan, C.; Kang, H.; Kane, R. Neuropsychologic assessment of a population-based sample of Gulf War veterans. Cogn. Behav. Neurol. 2009, 22, 155–166. [Google Scholar] [CrossRef] [PubMed]
- Jeffrey, M.; Collado, F.; Kibler, J.; DeLucia, C.; Messer, S.; Klimas, N.; Craddock, T.J.A. Post-traumatic stress impact on health outcomes in Gulf War Illness. BMC Psychol. 2021, 9, 57. [Google Scholar] [CrossRef] [PubMed]
- Steele, L.; Klimas, N.; Krengel, M.; Quinn, E.; Toomey, R.; Little, D.; Abreu, M.; Aenlle, K.; Killiany, R.; Koo, B.-B.; et al. Brain–Immune Interactions as the Basis of Gulf War Illness: Clinical Assessment and Deployment Profile of 1990–1991 Gulf War Veterans in the Gulf War Illness Consortium (GWIC) Multisite Case-Control Study. Brain Sci. 2021, 11, 1132. [Google Scholar] [CrossRef] [PubMed]
- Blanchard, M.S.; Molina-Vicenty, H.D.; Stein, P.K.; Li, X.; Karlinsky, J.; Alpern, R.; Reda, D.J.; Toomey, R. Medical Correlates of Chronic Multisymptom Illness in Gulf War Veterans. Am. J. Med. 2019, 132, 510–518. [Google Scholar] [CrossRef] [PubMed]
- Outcalt, S.D.; Kroenke, K.; Krebs, E.E.; Chumbler, N.R.; Wu, J.; Yu, Z.; Bair, M.J. Chronic pain and comorbid mental health conditions: Independent associations of posttraumatic stress disorder and depression with pain, disability, and quality of life. J. Behav. Med. 2015, 38, 535–543. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Choh, A.C.; Demerath, E.W.; Knutson, K.L.; Duren, D.L.; Sherwood, R.J.; Sun, S.S.; Chumlea, W.C.; Towne, B.; Siervogel, R.M.; et al. Sleep disturbance in relation to health-related quality of life in adults: The Fels longitudinal study. J. Nutr. Health Aging 2009, 6, 576–583. [Google Scholar] [CrossRef] [PubMed]
- Verster, J.C.; Pandi-Permual, S.R.; Streiner, D.L. Sleep and Quality of Life in Clinical Medicine; Springer: Berlin/Heidelberg, Germany, 2008. [Google Scholar]
- Matsui, K.; Yoshiike, T.; Nagao, K.; Utsumi, T.; Tsuru, A.; Otsuki, R.; Ayabe, N.; Hazumi, M.; Suzuki, M.; Saitoh, K.; et al. Association of subjective quality and quantity of sleep with suality of life among a general population. Int. J. Environ. Res. Public Health 2021, 18, 12835. [Google Scholar] [CrossRef] [PubMed]
- Forman-Hoffman, V.L.; Peloso, P.M.; Black, D.W.; Woolson, R.F.; Letuchy, E.M.; Doebbeling, B.N. Chronic widespread pain in veterans of the first Gulf War: Impact of deployment status and associated health effects. J. Pain 2007, 8, 954–961. [Google Scholar] [CrossRef]
- Bardel, A.; Wallander, M.-A.; Wallman, T.; Rosengren, A.; Johansson, S.; Eriksson, H.; Svardsudd, K. Age and sex related self-reported symptoms in a general population across 30 years: Patterns of reporting and secular trend. PLoS ONE 2019, 14, e0211532. [Google Scholar] [CrossRef] [PubMed]
- Gifford, E.J.; Vahey, J.; Hauser, E.R.; Sims, K.; Efird, J.T.; Dursa, E.K.; Steele, L.; Helmer, D.A.; Provenzale, D. Gulf War illness in the Gulf War Era Cohort and Biorepository: The Kansas and centers for disease control definitions. Life Sci. 2021, 278, 119454. [Google Scholar] [CrossRef] [PubMed]
- Kazis, L.E.; Miller, D.R.; Clark, J.; Skinner, K.; Lee, A.; Rogers, W.; Spiro, A.; Payne, S.; Fincke, G.; Selim, A.; et al. Health-Related Quality of Life in Patients Served by the Department of Veterans Affairs: Results from the Veterans Health Study. Arch. Intern. Med. 1998, 158, 626–632. [Google Scholar] [CrossRef] [PubMed]
- Khalil, L.; McNeil, R.B.; Sims, K.J.; Felder, K.A.; Hauser, E.R.; Goldstein, K.M.; Voils, C.I.; Klimas, N.G.; Brophy, M.T.; Thomas, C.M.; et al. The Gulf War Era Cohort and Biorepository: A longitudinal research resource of veterans of the 1990–1991 Gulf War Era. Am. J. Epidemiol. 2018, 187, 2279–2291. [Google Scholar] [CrossRef] [PubMed]
- Selim, A.J.; Rogers, W.; Fleishman, J.A.; Qian, S.X.; Fincke, B.G.; Rothendler, J.A.; Kazis, L.E. Updated U.S. population standard for the Veterans RAND 12-item Health Survey (VR-12). Qual. Life Res. 2009, 18, 43–52. [Google Scholar] [CrossRef]
- Jones, D.; Kazis, L.; Lee, A.; Rogers, W.; Skinner, K.; Cassar, L.; Wilson, N.; Hendricks, A. Health status assessments using the Veterans SF-36 and SF-12. Methods for evaluating outcomes in the Veterans Health Administration. J. Ambul. Care Manag. 2001, 24, 68–86. [Google Scholar] [CrossRef]
- Iqbal, S.U.; Rogers, W.; Selim, A.; Qian, S.; Austin, L.; Ren, X.S.; Rothendler, J.; Miller, D.; Kazis, L.E. The Veterans RAND 12 Item Health Survey (VR-12): What It Is and How It Is Used. 2015. Available online: https://www.bu.edu/sph/files/2015/01/veterans_rand_12_item_health_survey_vr-12_2007.pdf (accessed on 24 March 2022).
- PROMIS. Sleep Disturbance: A Brief Guide to the PROMIS(R) Sleep Disturbance Instruments. 2019. Available online: https://docplayer.net/47327671-Sleep-disturbance-a-brief-guide-to-the-promis-sleep-disturbance-instruments.html (accessed on 3 March 2020).
- Assessment Center Scoring Service. HealthMeasures Scoring Service Powered by Assessment Center. Available online: https://www.assessmentcenter.net/ac_scoringservice (accessed on 3 March 2020).
- Weathers, F.W.; Litz, B.T.; Herman, D.S.; Huska, J.A.; Keane, T.M. The PTSD checklist (PCL): Reliability, validity, and diagnostic utility. In Proceedings of the 9th Annual Conference of the International Society for Traumatic Stress Studies, San Antonio, TX, USA, 25 October 1993. [Google Scholar]
- The National Center for PTSD. Using the PTSD Checklist for DSM-IV (PCL). Available online: https://www.ptsd.va.gov/professional/assessment/documents/PCL_handoutDSM4.pdf (accessed on 5 March 2021).
- Barrett, D.H.; Gray, G.C.; Doebbeling, B.N.; Clauw, D.J.; Reeves, W.C. Prevalence of symptoms and symptom-based conditions among Gulf War veterans: Current status of research findings. Epidemiol. Rev. 2002, 24, 218–227. [Google Scholar] [CrossRef]
- Kroenke, K.; Strine, T.W.; Spitzer, R.L.; Williams, J.B.W.; Berry, J.T.; Mokdad, A.H. The PHQ-8 as a measure of current depression in the general population. J. Affect. Disord. 2009, 114, 163–173. [Google Scholar] [CrossRef]
- Serlin, R.C.; Mendoza, T.R.; Nakamura, Y.; Edwards, K.R.; Cleeland, C.S. When is cancer pain mild, moderate or severe? Grading pain severity by its interference with function. Pain Med. 1995, 61, 277–284. [Google Scholar] [CrossRef]
- Luncheon, C.; Zack, M. Health-related quality of life among US veterans and civilians by race and ethnicity. Prev. Chronic Dis. 2012, 9, E108. [Google Scholar] [CrossRef]
- Kazis, L.E.; Ren, X.S.; Lee, A.; Skinner, K.; Rogers, W.; Clark, J.; Miller, D.R. Health status in VA patients: Results from the Veterans Health Study. Am. J. Med. Qual. 1999, 14, 28–38. [Google Scholar] [CrossRef]
- Steele, L. Prevalence and patterns of Gulf War illness in Kansas veterans: Association of symptoms with characteristics of person, place, and time of military service. Am. J. Epidemiol. 2000, 152, 992–1002. [Google Scholar] [CrossRef] [PubMed]
- StataCorp. Stata Statistical Software: Release 16; StataCorp LLC: College Station, TX, USA, 2019. [Google Scholar]
- Alonso, J.; Ferrer, M.; Gandek, B.; Ware, J.E., Jr.; Aaronson, N.K.; Mosconi, P.; Rasmussen, N.K.; Bullinger, M.; Fukuhara, S.; Kaasa, S.; et al. Health-related quality of life associated with chronic conditions in eight countries: Results from the International Quality of Life Assessment (IQOLA) Project. Qual. Life Res. 2004, 13, 283–298. [Google Scholar] [CrossRef] [PubMed]
- Heyworth, I.T.; Hazell, M.L.; Linehan, M.F.; Frank, T.L. How do common chronic conditions affect health-related quality of life? Br. J. Gen. Pract. 2009, 59, e353–e358. [Google Scholar] [CrossRef] [PubMed]
- Dursa, E.K.; Cao, G.; Porter, B.; Culpepper, W.J.; Schneiderman, A.I. The health of Gulf War and Gulf era veterans over time: U.S. Department of Veterans Affairs’ Gulf War Longitudinal Study. J. Occup. Environ. 2021, 63, 889–894. [Google Scholar] [CrossRef] [PubMed]
- Burg, M.M.; Soufer, R. Post-traumatic Stress Disorder and Cardiovascular Disease. Curr. Cardiol. Rep. 2016, 18, 94. [Google Scholar] [CrossRef]
- Dyball, D.; Evans, S.; Boos, C.J.; Stevelink, S.A.; Fear, N.T. The association between PTSD and cardiovascular disease and its risk factors in male veterans of the Iraq/Afghanistan conflicts: A systematic review. Int. Rev. Psychiatry 2019, 31, 34–48. [Google Scholar] [CrossRef]
- Roberts, A.L.; Agnew-Blais, J.C.; Spiegelman, D.; Kubzansky, L.D.; Mason, S.M.; Galea, S.; Hu, F.B.; Rich-Edwards, J.W.; Koenen, K.C. Posttraumatic stress disorder and incidence of type 2 diabetes mellitus in a sample of women: A 22-year longitudinal study. JAMA Psychiatry 2015, 72, 203–210. [Google Scholar] [CrossRef]
- Graham, E.A.; Deschenes, S.S.; Khalil, M.N.; Danna, S.; Filion, K.B.; Schmitz, N. Measures of depression and risk of type 2 diabetes: A systematic review and meta-analysis. J. Affect. Disord. 2020, 265, 224–232. [Google Scholar] [CrossRef]
- Angst, F.; Benz, T.; Lehmann, S.; Wagner, S.; Simmen, B.R.; Sandor, P.S.; Gengenbacher, M.; Angst, J. Extended overview of the longitudinal pain-depression association: A comparison of six cohorts treated for specific chronic pain conditions. J. Affect. Disord. 2020, 273, 508–516. [Google Scholar] [CrossRef]
- Asmundson, G.J.; Wright, K.D.; Stein, M.B. Pain and PTSD symptoms in female veterans. Eur. J. Pain 2004, 8, 345–350. [Google Scholar] [CrossRef]
- Hunt, S.C.; Richardson, R.D.; Engel, C.C., Jr.; Atkins, D.C.; McFall, M. Gulf War veterans’ illnesses: A pilot study of the relationship of illness beliefs to symptom severity and functional health status. J. Occup. Environ. 2004, 46, 818–827. [Google Scholar] [CrossRef] [PubMed]
- Dickey, B.; Madhu, L.N.; Shetty, A.K. Gulf War Illness: Mechanisms Underlying Brain Dysfunction and Promising Therapeutic Strategies. Pharmacol. Ther. 2021, 220, 107716. [Google Scholar] [CrossRef] [PubMed]
- Nugent, S.M.; Freeman, M.; Ayers, C.K.; Winchell, K.A.; Press, A.M.; O’Neil, M.E.; Paynter, R.; Kansagara, D. A systematic review of therapeutic interventions and management strategies for Gulf War illness. Mil. Med. 2020, 186, e169–e178. [Google Scholar] [CrossRef] [PubMed]
- Alison Phillips, L.; McAndrew, L.M.; Laman-Maharg, B. Symptom attribution to a medically unexplained syndrome is associated with greater perceived severity and bothersomeness of symptoms in US military veterans. Psychol. Health 2021, 1–18. [Google Scholar] [CrossRef] [PubMed]
- RAND. Examining Possible Causes of Gulf War Illness; RAND National Defense Research Institute: Santa Monica, CA, USA, 2005. [Google Scholar]
- Institute of Medicine. Depleted Uranium, Pyridostigmine Bromide, Sarin, and Vaccines; National Academy Press: Washington, DC, USA, 2000; Volume 1. [Google Scholar]



{kind=link}
{kind=link}
| Characteristics | Total | Kansas | CDC | |||||
|---|---|---|---|---|---|---|---|---|
| GWI Sym+/Dx− | Noncase (1) Sym+/Dx+ | Noncase (2) Sym−/Dx+ | Noncase (3) Sym−/Dx− | GWI Severe | GWI Mild-to-Moderate | Noncase | ||
| (%) | (%) | (%) | (%) | (%) | (%) | (%) | (%) | |
| Female | 23.2 | 27.5 | 20.6 c | 21.7 | 20.1 c | 26.9 | 23.9 | 15.5 b |
| Age | ||||||||
| <50 years | 38.7 | 46.7 | 31.9 a | 24.5 a | 40.6 | 45.5 | 37.7 c | 32.6 b |
| 50–59 years | 36.9 | 40.6 | 35.7 | 25.5 b | 37.2 | 34.8 | 38.3 | 34.8 |
| 60+ years | 24.4 | 12.7 | 32.5 a | 50.0 a | 22.2 b | 19.7 | 23.9 | 32.6 b |
| Race/ethnicity | ||||||||
| White, non-Hispanic | 65.1 | 63.1 | 56.5 | 68.9 | 79.1 a | 45.5 | 70.2 a | 74.3 a |
| Black, non-Hispanic | 17.2 | 17.1 | 20.3 | 18.9 | 12.1 | 20.8 | 16.2 | 15.5 |
| Hispanic | 9.5 | 12.4 | 11.0 | 6.6 c | Sup.a | 18.6 | 7.1 a | 5.3 a |
| Other | 6.2 | 5.9 | 8.1 | Sup. | 5.0 | 11.7 | 4.7 a | 3.7 a |
| Income | ||||||||
| <$30,000 | 11.2 | 12.4 | 14.2 | Sup. | 6.3 b | 16.7 | 9.6 b | 9.1 c |
| $30,000-$59,999 | 23.1 | 22.8 | 31.0 c | 18.9 | 14.2 b | 29.9 | 22.7 c | 15.0 a |
| $60,000-$99,999 | 29.0 | 27.5 | 29.0 | 34.0 | 29.7 | 28.4 | 30.1 | 26.2 |
| $100,000+ | 29.7 | 31.5 | 17.7 a | 31.1 | 43.5 b | 16.7 | 31.1 a | 43.3 a |
| Education | ||||||||
| <Associate’s degree | 9.0 | 6.8 | 11.3 c | 14.2 c | 7.1 | 9.1 | 8.4 | 10.7 |
| Bachelor’s or Associate’s degree | 68.2 | 70.2 | 71.6 | 66.0 | 60.7 c | 75.8 | 67.1 b | 61.5 b |
| Master’s, Professional, or Doctorate’s degree | 20.7 | 20.7 | 13.9 c | 19.8 | 31.0 b | 12.1 | 22.3 a | 27.3 a |
| Military Component | ||||||||
| Active Duty only | 60.8 | 64.5 | 64.6 | 47.6 b | 54.6 c | 65.9 | 62.5 | 47.8 a |
| Active Duty and Reserves | 24.5 | 22.2 | 25.2 | 29.5 | 25.2 | 25.8 | 22.2 | 30.6 |
| Reserves only | 14.7 | 13.2 | 10.1 | 22.9 c | 20.2 c | 8.3 | 15.3 b | 21.5 a |
| Military Branch | ||||||||
| Army | 45.5 | 46.7 | 53.3 | 34.0 c | 37.2 c | 54.9 | 45.9 c | 31.0 a |
| Navy | 16.1 | 14.8 | 12.2 | 21.7 | 21.8 c | 11.7 | 15.5 | 24.6 a |
| Airforce | 11.0 | 11.0 | 9.3 | 15.1 | 11.7 | 7.2 | 12.0 c | 12.8 |
| Marines | 12.5 | 14.6 | 9.0 c | 12.3 | 14.2 | 11.7 | 12.2 | 15.0 |
| National Guard | 9.8 | 9.4 | 9.3 | 12.3 | 10.0 | 8.7 | 9.5 | 12.3 |
| Other | 5.0 | 3.5 | 7.0 c | Sup. | 5.0 | 5.7 | 5.0 | Sup. |
| VHA user | 44.6 | 47.6 | 61.7 a | 33.0 b | 20.1 a | 68.3 | 41.1 a | 24.2 a |
| Deployed to Gulf | 76.1 | 79.6 | 78.8 | 66.0 b | 70.3 b | 86.4 | 73.2 a | 71.7 a |
| N | 1116 | 426 | 345 | 106 | 239 | 264 | 665 | 187 |
| Total | Kansas | CDC | ||||||
|---|---|---|---|---|---|---|---|---|
| GWI Sym+/Dx− | Noncase (1) Sym+/Dx+ | Noncase (2) Sym−/Dx+ | Noncase (3) Sym−/Dx− | GWI Severe | GWI Mild-to-Moderate | Noncase | ||
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | |
| Health-Related Quality of Life | ||||||||
| Physical Component | 41.5 | 40.2 | 34.3 a | 46.9 a | 52.1 a | 30.0 | 43.5 a | 50.8 a |
| (12.3) | (11.3) | (11.3) | (10.5) | (6.5) | (10.1) | (10.7) | (8.0) | |
| Mental Component | 46.3 | 44.2 | 40.5 a | 56.0 a | 54.3 a | 34.6 | 48.1 a | 56.4 a |
| (12.7) | (12.5) | (12.8) | (7.2) | (7.5) | (11.1) | (11.1) | (6.5) | |
| Other Indices of Health | ||||||||
| Sleep Disturbance | 54.0 | 57.4 | 58.7 | 45.2 a | 45.0 a | 63.9 | 53.2 a | 43.1 a |
| (10.3) | (8.5) | (8.8) | (8.0) | (7.8) | (7.8) | (8.1) | (7.5) | |
| PTSD | 34.8 | 37.3 | 45.0 a | 20.7 a | 21.8 a | 55.3 | 30.8 a | 20.0 a |
| (17.3) | (15.9) | (18.2) | (4.7) | (6.7) | (15.1) | (12.6) | (6.1) | |
| Depression | 6.8 | 7.9 | 10.3 a | 1.9 a | 1.8 a | 14.1 | 5.5 a | 1.1 a |
| (6.2) | (5.8) | (6.3) | (2.2) | (2.4) | (5.4) | (4.5) | (2.1) | |
| Pain | 3.9 | 4.5 | 5.3 a | 2.0 a | 1.5 a | 6.6 | 3.5 a | 1.3 a |
| (2.8) | (2.6) | (2.7) | (2.2) | (1.7) | (2.3) | (2.4) | (1.9) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gifford, E.J.; Boyle, S.H.; Vahey, J.; Sims, K.J.; Efird, J.T.; Chesnut, B.; Stafford, C.; Upchurch, J.; Williams, C.D.; Helmer, D.A.; et al. Health-Related Quality of Life by Gulf War Illness Case Status. Int. J. Environ. Res. Public Health 2022, 19, 4425. https://doi.org/10.3390/ijerph19084425
Gifford EJ, Boyle SH, Vahey J, Sims KJ, Efird JT, Chesnut B, Stafford C, Upchurch J, Williams CD, Helmer DA, et al. Health-Related Quality of Life by Gulf War Illness Case Status. International Journal of Environmental Research and Public Health. 2022; 19(8):4425. https://doi.org/10.3390/ijerph19084425
Chicago/Turabian StyleGifford, Elizabeth J., Stephen H. Boyle, Jacqueline Vahey, Kellie J. Sims, Jimmy T. Efird, Blair Chesnut, Crystal Stafford, Julie Upchurch, Christina D. Williams, Drew A. Helmer, and et al. 2022. "Health-Related Quality of Life by Gulf War Illness Case Status" International Journal of Environmental Research and Public Health 19, no. 8: 4425. https://doi.org/10.3390/ijerph19084425
APA StyleGifford, E. J., Boyle, S. H., Vahey, J., Sims, K. J., Efird, J. T., Chesnut, B., Stafford, C., Upchurch, J., Williams, C. D., Helmer, D. A., & Hauser, E. R. (2022). Health-Related Quality of Life by Gulf War Illness Case Status. International Journal of Environmental Research and Public Health, 19(8), 4425. https://doi.org/10.3390/ijerph19084425