
Sports Performance Tests for Amputee Football Players: A Scoping Review



Abstract
1. Introduction
2. Materials and Methods
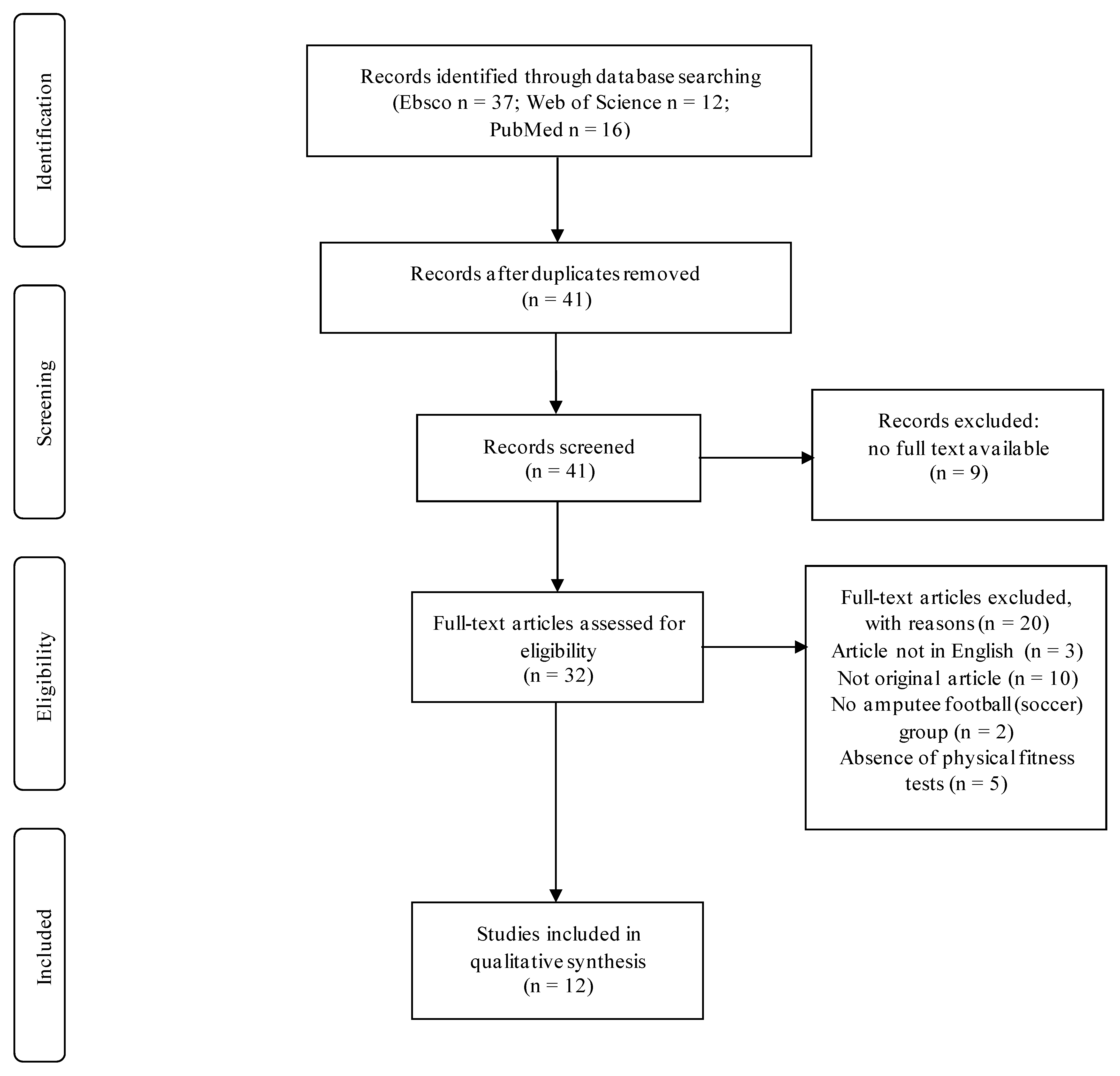
2.1. Search Strategy, Study Selection, and Data Extraction
2.2. Studies Description
2.3. Sports Performance Tests Description
2.4. Sports Performance Tests’ Quality Assessment
- validity, reliability and/or standardization information present and/or cited references that have confirmed validity, reliability and/or standardization and/or expert validity: “1”;
- cited references present but not available or in a language other than English or in unavailable books; no information on validity, reliability and/or standardization or insufficient standardization: “0”.
2.5. Studies’ Quality Assessment
3. Results
3.1. Qualitative Assessment of Sports Performance Tests
3.1.1. Reliability
3.1.2. Validity
3.1.3. Standardization
3.2. Qualitative Assessment of Articles
4. Discussion
Limitations and Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Frere, J. The History of “modern” Amputee Football. In Amputee Sports for Victims of Terrorism; Centre of Excellence—Defence Against Terrorism, Ed.; IOS Press: Ankara, Turkey, 2008; pp. 5–13. [Google Scholar]
- Yazicioglu, K.; Taskaynatan, M.; Guzelkucuk, U.; Tugcu, I. Effect of Playing Football (Soccer) on Balance, Strength, and Quality of Life in Unilateral Below-Knee Amputees. Am. J. Phys. Med. Rehabil. 2007, 86, 800–805. [Google Scholar] [CrossRef] [PubMed]
- Güçhan, Z.; Bayraklar, K.; Ergun, N.; Ercan, Y. Comparison of mobility and quality of life levels in sedentary amputees and amputee soccer players. J. Exerc. Ther. Rehabil. 2017, 4, 47–53. [Google Scholar]
- Ilkım, M.; Canpolat, B.; Akyol, B. The Effects of Eight-Week Regular Training in Amateur Amputee Football Team Athletes’ Body Composition. Turk. J. Sport Exerc. 2018, 20, 199–206. [Google Scholar] [CrossRef][Green Version]
- Monteiro, R.; Pfeifer, L.; Santos, A.; Sousa, N. Soccer practice and functional and social performance of men with lower limb amputations. J. Hum. Kinet. 2014, 43, 33–41. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Maehana, H.; Miyamoto, A.; Koshiyama, K.; Yanagiya, T.; Yoshimura, M. Profile of match performance and heart rate response in Japanese amputee soccer. J. Sports Med. Phys. Fit. 2018, 58, 816–824. [Google Scholar] [CrossRef] [PubMed]
- Nowak, A.M. Match performance in Polish amputee soccer Extra Ligue—A pilot study. Adv. Rehabil. 2020, 34, 16–25. [Google Scholar] [CrossRef]
- Chin, T.; Sawamura, S.; Fujita, H.; Nakajima, S.; Ojima, I.; Oyabu, H.; Nagakura, Y.; Otsuka, H.; Nakagawa, A. Physical fitness of lower limb amputees. Am. J. Phys. Med. Rehabil. 2002, 81, 321–325. [Google Scholar] [CrossRef]
- Özkan, A.; Kayıhan, G.; Köklü, Y.; Ergun, N.; Koz, M.; Ersöz, G.; Dellal, A. The Relationship Between Body Composition, Anaerobic Performance and Sprint Ability of Amputee Soccer Players. J. Hum. Kinet. 2012, 35, 141–146. [Google Scholar] [CrossRef][Green Version]
- Tatar, Y.; Gercek, N.; Ramazanoglu, N.; Gulmez, I.; Uzun, S.; Sanli, G.; Karagozoglu, C.; Cotuk, H.B. Load distribution on the foot and lofstrand crutches of amputee football players. Gait Posture 2018, 64, 169–173. [Google Scholar] [CrossRef]
- Hoff, J. Training and testing physical capacities for elite soccer players. J. Sports Sci. 2005, 23, 573–582. [Google Scholar] [CrossRef]
- Buckley, J.G.; O’Driscoll, D.; Bennett, S.J. Postural sway and active balance performance in highly active lower-limb amputees. Am. J. Phys. Med. Rehabil. 2002, 81, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Mikami, Y.; Fukuhara, K.; Kawae, T.; Sakamitsu, T.; Kamijo, Y.; Tajima, H.; Kimura, H.; Adachi, N. Exercise loading for cardiopulmonary assessment and evaluation of endurance in amputee football players. J. Phys. Ther. Sci. 2018, 30, 960–965. [Google Scholar] [CrossRef] [PubMed]
- Mine, T.; Cengiz, T.; Turgut, K.; Halil, T. Relationship between quickness and speed performance in amputee footballers. Sci. Mov. Health 2014, 14, 580–584. [Google Scholar]
- Miyamoto, A.; Maehana, H.; Yanagiya, T. The relationship between sprint speed and sprint motion in amputee soccer players. Eur. J. Adapt. Phys. Act. 2019, 12, 9. [Google Scholar] [CrossRef]
- Simim, M.A.M.; Silva, B.V.C.; Marocolo Jr, M.; Mendes, E.L.; de Mello, M.T.; da Mota, G.R.T. Anthropometric profile and physical performance characteristic of the Brazilian amputee football (soccer) team. Mot. Rev. Educ. Física 2013, 19, 641–648. [Google Scholar] [CrossRef][Green Version]
- Simim, M.A.; Bradley, P.S.; da Silva, B.V.; Mendes, E.L.; de Mello, M.T.; Marocolo, M.; da Mota, G.R. The quantification of game-induced muscle fatigue in amputee soccer players. J. Sports Med. Phys. Fit. 2017, 57, 766–772. [Google Scholar] [CrossRef]
- Simim, M.A.M.; da Mota, G.R.; Marocolo, M.; da Silva, B.V.C.; de Mello, M.T.; Bradley, P.S. The Demands of Amputee Soccer Impair Muscular Endurance and Power Indices but Not Match Physical Performance. Adapt. Phys. Act. Q. 2018, 35, 76–92. [Google Scholar] [CrossRef]
- Wieczorek, M.; Wiliński, W.; Struzik, A.; Rokita, A. Hand Grip Strength Vs. Sprint Effectiveness in Amputee Soccer Players. J. Hum. Kinet. 2015, 48, 133–139. [Google Scholar] [CrossRef]
- Zwierko, M.; Lesiakowski, P.; Zwierko, T. Postural Control during Progressively Increased Balance-Task Difficulty in Athletes with Unilateral Transfemoral Amputation: Effect of Ocular Mobility and Visuomotor Processing. Int. J. Environ. Res. Public Health 2020, 17, 6242. [Google Scholar] [CrossRef]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and Elaboration. PLoS Med. 2007, 4, e297. [Google Scholar] [CrossRef]
- Sorensen, A.A.; Wojahn, R.D.; Manske, M.C.; Calfee, R.P. Using the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement to Assess Reporting of Observational Trials in Hand Surgery. J. Hand Surg. 2013, 38, 1584–1589. [Google Scholar] [CrossRef] [PubMed]
- Deathe, A.B.; Miller, W.C. The L Test of Functional Mobility: Measurement Properties of a Modified Version of the Timed “Up & Go” Test Designed for People with Lower-Limb Amputations. Phys. Ther. 2005, 85, 626–635. [Google Scholar] [CrossRef] [PubMed]
- Negrete, R.J.; Hanney, W.J.; Pabian, P.; Kolber, M.J. Upper body push and pull strength ratio in recreationally active adults. Int. J. Sports Phys. Ther. 2013, 8, 138–144. [Google Scholar] [PubMed]
- Bangsbo, J.; Iaia, F.M.; Krustrup, P. The Yo-Yo Intermittent Recovery Test: A Useful Tool for Evaluation of Physical Performance in Intermittent Sports. Sports Med. 2008, 38, 37–51. [Google Scholar] [CrossRef]
- Giboin, L.-S.; Gruber, M.; Kramer, A. Additional Intra- or Inter-session Balance Tasks Do Not Interfere with the Learning of a Novel Balance Task. Front. Physiol. 2018, 9, 1319. [Google Scholar] [CrossRef]
- Tweedy, S.M.; Vanlandewijck, Y.C. International Paralympic Committee position stand—Background and scientific principles of classification in Paralympic sport. Br. J. Sports Med. 2009, 45, 259–269. [Google Scholar] [CrossRef]
- Tweedy, S.M.; Mann, D.; Vanlandewijck, Y.C. Research needs for the development of evidence-based systems of classification for physical, vision, and intellectual impairments. In Training and Coaching the Paralympic Athlete; Vanlandewijck, Y.C., Thompson, W.R., Eds.; Wiley Online Library: Hoboken, NJ, USA, 2016; pp. 122–149. [Google Scholar] [CrossRef]
- Marszałek, J.; Kosmol, A.; Morgulec-Adamowicz, N.; Mróz, A.; Gryko, K.; Molik, B. Test–retest reliability of the newly developed field-based tests focuses on short time efforts with maximal intensity for wheelchair basketball players. Adv. Rehabil. 2019, 33, 23–27. [Google Scholar] [CrossRef]


{kind=link}
| Authors | Type of Study | Purpose | SG / CG | Training Experience of SG |
|---|---|---|---|---|
| Buckley et al., 2002 | CC | To determine the balance performance of active lower limb amputees during quiet standing and under dynamic conditions. | n = 6 (AF) 25.7 ± 5.8 yrs. / n = 6 (AB) 24.7 ± 2.7 yrs. | ND |
| Yazicioglu et al., 2007 | CS-C | To investigate the effect of playing football on balance, muscle strength, locomotor capabilities, and health-related quality of life in subjects with unilateral below-knee amputation. | n = 12 AF, 28.3 ± 4.6 yrs. / n =12 (AMP) 29.8 ± 1.4 yrs. | ≥6 mths |
| Ozkan et al., 2012 | C | To investigate the relationship between body composition, anaerobic performance, and sprint performance of AF. | n = 15 (AF) 25.5 ± 5.8 yrs. | 3.3 ± 2.9 yrs. |
| Simim et al., 2013 | C | To describe anthropometric and physical characteristics of AF and to compare these results, taking into consideration the players’ tactical function, and to verify if there are differences between HR after maximum test and the employment of six equations for prediction of HRmax. | n = 12 (AF) 29.3 ± 8.6 yrs. | ≥5 yrs. |
| Mine et al., 2014 | C | To examine relationships between quickness and speed performance in AF. | n = 10 (AF) 25.8 ± 4.32 yrs. | ND |
| Wieczorek et al., 2015 | C | To find the relationship between handgrip strength and sprint time in AF. | n = 13 (AF) 26.1 ± 7.7 yrs. | 30.8 ± 14.3 mths |
| Guchan et al., 2017 | CC | To determine the effects of playing soccer on various components of physical performance such as body composition, muscular endurance, anaerobic power, flexibility, balance, and speed of individuals with transtibial amputation. | n = 12 (AF) 26.67 ± 7.76 yrs. / n = 12 (AMP, sedentary) 33 ± 6.7 yrs. | ≥1 yr. |
| Simim et al., 2017 | CC | To quantify the degree of game-induced muscular fatigue in AF. | n = 33 (AF) 31 ± 7 yrs. / n = 5 (AF, not playing all matches) | ≥4 yrs. |
| Simim et al., 2018 | C | To investigate the match demands of amputee football and its impact on muscular endurance and power. | n = 16 (AF) 32 ± 5 yrs. | ≥5 yrs. |
| Mikami et al., 2018 | CC | To examine the difference in measured CPX values among two-legged, one-legged, and two-armed exercises in AB, and to preliminarily evaluate the endurance of AF through CPX with two-armed exercise. | n = 20 (AB) 28.3 ± 5.6 yrs. / n = 8 (AF) 36.4 ± 5.7 yrs. | 0.4–5 yrs. |
| Miyamoto et al., 2019 | C | To analyze sprint motion in outfield positioned AF using crutches and to clarify the relationship between sprint speed and sprint motion. | n = 12 (AF) 42.3 ± 4.6 yrs. | 3.58 ± 2.48 yrs. |
| Zwierko et al., 2020 | CC | To examine postural control during single-leg stance test with progressively increased balance-task difficulty in soccer players with unilateral transfemoral amputation compared to AB soccer players. | n = 11 (AF) 27.45 ± 5.2 yrs. / n = 11 (AB football players) 21.91 ± 3.11 yrs. | 8.27 ± 3.63 yrs. |
| I | II | III | IV | ||||
|---|---|---|---|---|---|---|---|
| Authors | Methods | Test Descriptions | Outcomes | ||||
| Participants’ Preparation | Warm-Up | Procedures | Repetitions | Breaks | |||
| Buckley et al., 2002 | Static balance test (Kistler force platform) | sportswear; prosthesis | ND | comfortable position on the force platform surface with feet equidistant from a central dividing line, hands on the hips; a large visual target at eye level on a wall 5 m from the force platform; stand stationary, look straight at the visual target for 30 s | ND | ND | CP excursion range, sum of the square’s deviations from the mean CP location in the AP and ML directions |
| Dynamic balance test (modified dynamic stabilimeter) | approx. 5 min; standing on the stabilimeter | ML—standing on the board pivoted side-to-side in the frontal plane; AP—pivoted forwards and backwards in the sagittal plane; trials in a random order; place hands on hips, focus on a large visual target positioned at eye level on a wall 5 m in front of them | 3 trials of 20 s | step down from the stabilimeter | time spent in and out of balance; number of times the board contacted the ground; mean number of contacts per limb (prosthetic or intact, dominant, or non-dominant) or per direction (forwards or backwards) | ||
| Yazicioglu et al., 2007 | Berg Balance Scale | ND | ND | 14 tasks common in everyday life (sitting, standing, reaching, leaning over, turning, and looking over each shoulder, turning in a complete circle, and stepping) | ND | ND | each item is scored on a scale from 0 to 4, max. 56 points |
| One-leg static balance test (KAT 2000; Kinesthetic Ability Trainer; Breg, Vista, CA) | ND | 5 min. | standing on the intact limb; arms folded across the chest, the knee kept in approx. 10 degrees in flexion; unable to maintain a balance and touch the railing—test discontinued and restart performed in the first difficulty level according to subject’s body mass | once a day, for 3 days | 15 min. | distance from the central point to the reference position of each trial; balance index | |
| Dynamic balance test (KAT 2000; Kinesthetic Ability Trainer; Breg, Vista, CA) | prosthesis | standing on both legs; as above | |||||
| Isokinetic muscle strength test (Cybex dynamometer) | ND | ND | peak torques of nonamputee side knee in extension and flexion; perform maximal concentric-concentric motion at angular velocities of 60, 120, and 180 degrees/s | once | 20 s | Nm | |
| Özkan et al., 2012 | CMJ, SJ (force plate; Sport Expert TM, MPS-501 multi-purpose measuring system, Tumer Electronic LDT, Turkey; centimeter) | no crutches; no prosthesis | Test familiarization | jump as high as possible; SJ: starting position with knees flexed to 90°, hands fixed on the hips, and no allowance for preparatory counter movement; CMJ: performed from an upright standing position, hands fixed on the hips, and with a counter movement preparatory phase, with end position as SJ starting position | 3 CMJs; 3 SJs | 2 min. | jump height; total work produced in each jump (the Genuario and Dolgener formulas) |
| T10, T20, T30 (light gates with timing system; Prosport, Tumer Electronics, Ankara, Turkey) | crutches; no prosthesis | ND | indoor court; light gates placed at the start and at the finish of each sprint test | 2 times each distance | 1 min. | time | |
| Simim et al., 2013 | T20 (stopwatch) | crutches | 10 min, test familiarization | official field with natural grass; player initiated a movement | ND | at least 24 h of recovery between testing sessions; 5 min. between the two first tests on day one; 3 min. rest between each T-square trial | time; mean speed |
| T-square (stopwatch) | 3 times | time | |||||
| The YYIRT1; Polar F5 to HRmax; Six equations to predict HRmax | official field with natural grass; 20 m shuttle run test with increasing velocities, 10 s of active recovery between runs until exhaustion; test end if: participant fails twice to reach the front line within the time limit or is unable to complete another run at the imposed speed; HRmax record immediately after the test | ND | total distance; HRmax result compared with 6 equations used to predict HRmax | ||||
| Mine et al., 2014 | T30 (electronic timing system) | rubber-soled track shoes | ND | photocells set on 0, 5, 30 m; standardized starting position; players started the approx. 30 cm back from the starting line; quickness on 5 m, speed on 30 m | 3 times | 3 min. intervals | time |
| Wieczorek et al., 2015 | Handgrip test (SEHAN hydraulic hand dynamometer, Jamar) | ND | ND | sit with arms along the body, elbow joint in 90° flexion, forearm, wrist in a neutral position; grip the handle of the dynamometer | twice by each hand | ND | the highest value |
| T30 (Fusion Smart Speed System; Fusion Sport, Coopers Plains, QLD, Australia) | crutches | ND | 8 infrared working gates; 3 m distance between photocells and mirrors; splits recorded: 1, 5, 10, 15, 20, 25, 30 m; standing start; deciding themselves when to start; stretched crutches, no crossing the starting line | 2 times | ND | time; mean running velocity | |
| Güçhan et al., 2017 | Sit-ups isotonic | prosthesis; shoes | 5 min. | lie back with bent knees and sit up until the scapula is no longer in contact with the surface | ND | 2 min. between tests | repetitions; time |
| Isotonic PUT | trunk and head to the floor and push the body up | ||||||
| Back extensors isometric | lie on a table face down, with inguinal points and lower body on the end table, upper body over the table; cross arms in front of the shoulders, raise the trunk; assessor fixed participant’s leg | time sustaining in the position | |||||
| Trunk flexors | lie back with knees flexed; arms straight toward knees, raise head, neck, shoulders stay in the position | ||||||
| Vertical jump test | stand up, fix amputated limb next to the wall, extend arm above; the end of the longest finger was marked before and after a jump; jump vertically; repetition with intact limb near the wall; distance between two marked heights | 3 times for both sides | the best result; Lewis’ formula (anaerobic power) | ||||
| Modified Thomas test | sit on the end of a table and lie down, with hip joint fixed 28 cm away from the end of the table; flex the contralateral lower limb maximally with arms; tested both sides | ND | distance between the table and the tested knee | ||||
| Sit-and-reach test | no prosthesis; no shoes | sit on the floor, knees straight, feet resting vertically; reach forward with straight arms as far as possible; distance between the toes and the longest finger | 3 trials | the best result | |||
| Berg Balance Scale | prosthesis; shoes | 14 items | ND | each item scored 0–4 | |||
| L test | walk an “L” shaped path (7 × 3 m); starting position: sit on a chair without armrests; get up from a chair, walk with usual pace to the end and come back to the sitting position | time | |||||
| F8W test | stand in the middle between 2 cones and complete the 8-shaped path with preferred speed walk, come back to the same point; 1.22 × 1.52 m | time; steps | |||||
| Simim et al., 2017 | PUT | ND | tests familiarization; dynamic warm-up and stretching; 1–3 repetitions of each test | max. number of repetitions in 60 s; result divided by body mass | ND | 5 min. between tests | repetitions; relative measure |
| CMJ (accelerometer Myotest, Sion, Switzerland; centimeter) | use preliminary movement by rapidly flexing the knee, before launching the body vertically | 3 trials | as above; 30 s between jumps; 1 min. between throws | jump height; power | |||
| MBT (medicine ball 3 kg) | sit with your back against the wall; lower back stays in contact with the wall during the test; hold a medicine ball with both hands against a chest and throw it on command as far as possible | distance | |||||
| Simim et al., 2018 | PUT | ND | tests familiarization; dynamic warm-up and stretching; 3 repetitions of each test | max. number of repetitions in 60 s; result divided by body mass | ND | one day; pre-and post-match; 5 min. rest between tests | repetitions; relative measure |
| CMJ (accelerometer Myotest, Sion, Switzerland) | use preliminary movement by rapidly flexing the knee, before launching the body vertically | as above; 30 s between jumps; 1 min. rest between throws | jump height; power | ||||
| MBT (medicine ball 3 kg) | sit with your back against the wall; lower back stays in contact with the wall during the test; hold a medicine ball with both hands against a chest and throw it on command as far as possible | distance | |||||
| Mikami et al., 2018 | CPX exercise test (Strength Ergometer; Strength Ergo 8, Mitsubishi Electric Engineering Co., Ltd., Tokyo, Japan); Expired gas monitoring breath-by-breath (cardiorespiratory exercise monitoring system, AE-310s; Minato Medical Science Co., Tokyo, Japan); Fatigue (Modified Borg Scale) | ND | ND | a multistage, Ramp-wise upgrading continuous load; two-legged exercise: Ramp 25 M/min.; one-legged exercise: used leg on the dominant hand side; Ramp 15 W/min.; two-armed exercise: Ramp 15 W/min.; Modified Borg Scale after exercise | ND | ND | anaerobic threshold value of oxygen uptake/weight; peak value of oxygen uptake/weight; HR; VE; WR; c-RPE; p-RPE |
| Miyamoto et al., 2019 | T30 (electronic timing gates, TC Timing System, Brower Timing System, USA) | crutches; no prosthesis | ND | splits recorded: 10, 20, 30 m; sprint; running style by supporting both crutches together for 2 steps; the 30-m sprint test (10 m intervals); speed (between 10 to 20 m) | 2 trials | ND | time |
| Zwierko et al., 2020 | Static balance test with open eyes (Biodex Balance System Inc., Shirley, NY, USA) | barefoot | 3 trials of 20 s adaptation (in 12, 8, and 4 level of platform stability) | 12 dynamic stability levels (12 is the most stable, 1 is the most unstable); single-leg stance on rigid platform; single-leg stance with decreasing platform stability—levels 8 to 4; single-leg stance with platform stability—level 4; 20 s each balance task; during the tests, look straight ahead with arms folded along the chest | 3 trials | 10 s | OSI; API; MLI |
| I | II | III | IV | ||
|---|---|---|---|---|---|
| Physical Attribute Tested | Test Name (and Tools) | Authors | Sports Performance Tests Assessment | ||
| R | V | S | |||
| Balance | Static balance test (Kistler force platform) * | Buckley et al., 2002 | 0 | 1 | 0 |
| Dynamic balance test (modified dynamic stabilimeter) * | 0 | 1 | 1 | ||
| Static balance test (Biodex) | Zwierko et al., 2020 | 0 | 1 | 1 | |
| One-leg static balance test (KAT 2000) | Yazicioglu et al., 2007 | 0 | 1 | 0 | |
| Dynamic balance test (KAT 2000) * | 0 | 1 | 1 | ||
| Berg Balance Scale | Yazicioglu et al., 2007, Güçhan et al., 2017 | 1 | 1 | 0 | |
| Muscle strength | Isokinetic trunk strength test (Cybex dynamometer) | Yazicioglu et al., 2007 | 0 | 1 | 0 |
| Handgrip test (hydraulic hand dynamometer) | Wieczorek et al., 2015 | 1 | 1 | 0 | |
| PUT | Simim et al., 2017, 2018 | 0 | 1 | 0 | |
| Isotonic PUT | Güçhan et al., 2017 | 0 | 1 | 0 | |
| Isotonic sit-ups test | 0 | 1 | 0 | ||
| Isometric back extension test * | 0 | 1 | 0 | ||
| Isometric trunk flection test | 0 | 1 | 0 | ||
| Power | Vertical jump tests—CMJ, CMJs, SJ, SJs (force plate Sport Expert TM) | Özkan et al., 2012 | 0 | 1 | 1 |
| CMJ (accelerometer Myotest) | Simim et al., 2017, 2018 | 1 | 1 | 0 | |
| MBT (medicine ball 3 kg) | 0 | 1 | 0 | ||
| Vertical jump test (Lewis’ formula) * | Güçhan et al., 2017 | 0 | 1 | 1 | |
| Anaerobic performance (sprint and movement speed 1) | T10, T20, T30 | Özkan et al.2012 | 0 | 1 | 0 |
| T20 | Simim et al., 2013 | 0 | 1 | 0 | |
| T30 (5 m) | Mine et al., 2014 | 0 | 1 | 0 | |
| T30 (1, 5, 10, 15, 20, 25 m) | Wieczorek et al., 2015 | 0 | 1 | 0 | |
| T30 (10, 20 m) | Myiamoto et al., 2019 | 0 | 1 | 0 | |
| L test * | Güçhan et al., 2017 | 1 | 1 | 0 | |
| F8W test * | 0 | 1 | 0 | ||
| Aerobic capacity | YYIRT1 | Simim et al., 2013 | 1 | 1 | 0 |
| CPX two-armed exercise | Mikami et al., 2018 | 0 | 1 | 0 | |
| Flexibility | Modified Thomas test * | Güçhan et al., 2017 | 0 | 1 | 1 |
| Sit-and-reach test | 0 | 1 | 1 | ||
| Agility | T-square | Simim et al., 2013 | 0 | 1 | 1 |
| Introduction | Methods | Results | Discussion | Other Information | STROBE Points 1 | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Items | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | Total |
| Authors | |||||||||||||||||||||||
| Simim et al., 2018 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 0 | 17 |
| Guchan et al., 2017 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 15 |
| Simim et al., 2017 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 17 |
| Wieczorek et al., 2015 | 0 | 1 | 1 | 0 | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 5 |
| Simim e al. 2013 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 15 |
| Ozkan et al., 2012 | 0 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 9 |
| Yazicioglu et al., 2007 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 0 | 16 |
| Mikami et al., 2018 | 0 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 12 |
| Mine et al., 2014 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 5 |
| Buckley et al., 2002 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 15 |
| Miyamoto et al., 2019 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 15 |
| Zwierko et al., 2020 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 14 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nowak, A.M.; Marszalek, J.; Molik, B. Sports Performance Tests for Amputee Football Players: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 4386. https://doi.org/10.3390/ijerph19074386
Nowak AM, Marszalek J, Molik B. Sports Performance Tests for Amputee Football Players: A Scoping Review. International Journal of Environmental Research and Public Health. 2022; 19(7):4386. https://doi.org/10.3390/ijerph19074386
Chicago/Turabian StyleNowak, Agnieszka Magdalena, Jolanta Marszalek, and Bartosz Molik. 2022. "Sports Performance Tests for Amputee Football Players: A Scoping Review" International Journal of Environmental Research and Public Health 19, no. 7: 4386. https://doi.org/10.3390/ijerph19074386
APA StyleNowak, A. M., Marszalek, J., & Molik, B. (2022). Sports Performance Tests for Amputee Football Players: A Scoping Review. International Journal of Environmental Research and Public Health, 19(7), 4386. https://doi.org/10.3390/ijerph19074386