
Telecardiology in Rural Practice: Global Trends

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
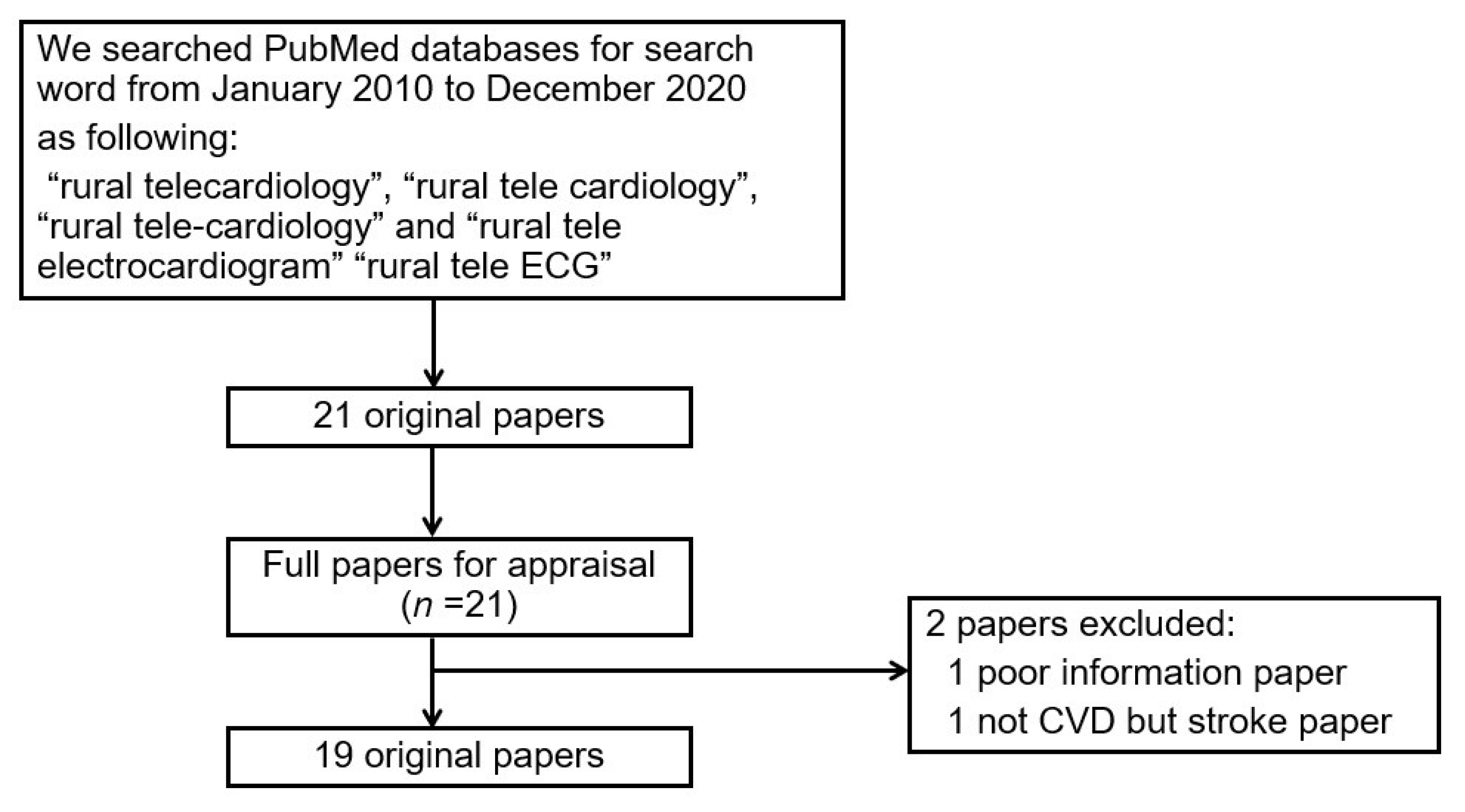
2. Materials and Methods
2.1. Study Sites and Participants
2.2. Classification of Telecardiology
3. Results
4. Discussion
4.1. A New Summary
4.2. Tele-Consultation
4.3. Telemedical System
4.4. Monitoring System
4.5. Prehospital Triage
4.6. Tele-Training
4.7. Additional Views
4.8. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thomas, A.G. Reducing the Growing Burden of Cardiovascular Disease in the Developing World. Health Aff. 2007, 26, 13–24. [Google Scholar] [CrossRef] [Green Version]
- Antiperovitch, P.; Zareba, W.; Steinberg, J.S.; Bacharova, L.; Tereshchenko, L.G.; Farre, J.; Nikus, K.; Ikeda, T.; Baranchuk, A. Proposed In-Training Electrocardiogram Interpretation Competencies for Undergraduate and Postgraduate Trainees. J. Hosp. Med. 2018, 13, 185–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seligman, B.; Vedanthan, R.; Fuster, V. Acute coronary syndromes in low- and middle-income countries: Moving forward. Int. J. Cardiol. 2016, 217, S10–S12. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Li, X.; Wang, Q.; Hu, S.; Wang, Y.; Masoudi, F.A.; Spertus, J.A.; Krumholz, H.M.; Jiang, L.; China PEACE Collaborative Group. ST-segment elevation myocardial infarction in China from 2001 to 2011 (the China PEACE-Retrospective Acute Myocardial Infarction Study): A retrospective analysis of hospital data. Lancet 2015, 385, 441–451. [Google Scholar] [CrossRef] [Green Version]
- Kakou-Guikahue, M.; N’Guetta, R.; Anzouan-Kacou, J.B.; Kramoh, E.; N’Dori, R.; Ba, S.A.; Diao, M.; Sarr, M.; Kane, A.; Kane, A.; et al. Optimizing the management of acute coronary syndromes in sub-Saharan Africa: A statement from the AFRICARDIO 2015 Consensus Team. Arch. Cardiovasc. Dis. 2016, 109, 376–383. [Google Scholar] [CrossRef]
- Vollenbroek-Hutten, M.; Jansen-Kosterink, S.; Tabak, M.; Feletti, L.C.; Zia, G.; N’dja, A.; Hermens, H.; SPRINTT Consortium. Possibilities of ICT-supported services in the clinical management of older adults. Aging Clin. Exp. Res. 2017, 29, 49–57. [Google Scholar] [CrossRef] [Green Version]
- Molinari, G.; Molinari, M.; Di Biase, M.; Brunetti, N.D. Telecardiology and its settings of application: An update. J. Telemed. Telecare 2018, 24, 373–381. [Google Scholar] [CrossRef]
- Teraura, H.; Iguchi, S.; Maeda, T.; Koike, S.; Matsumoto, M.; Haruyama, S.; Kotani, K. The use of information and communication technology in Japanese rural clinics. J. Rural Med. 2021, 16, 298–300. [Google Scholar] [CrossRef]
- Welsford, M.; Nikolaou, N.I.; Beygui, F.; Bossaert, L.; Ghaemmaghami, C.; Nonogi, H.; O’Connor, R.E.; Pichel, D.R.; Scott, T.; Walters, D.L.; et al. Acute Coronary Syndrome Chapter Collaborators. Part 5: Acute Coronary Syndromes: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Circulation 2015, 132 (Suppl. 1), S146–S176. [Google Scholar] [CrossRef]
- Kotani, K.; Watanabe, J.; Miura, K.; Gugliucci, A. Paraoxonase 1 and Non-Alcoholic Fatty Liver Disease: A Meta-Analysis. Molecules 2021, 26, 2323. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Verhoeven, F.; Tanja-Dijkstra, K.; Nijland, N.; Eysenbach, G.; van Gemert-Pijnen, L. Asynchronous and synchronous teleconsultation for diabetes care: A systematic literature review. J. Diabetes Sci. Technol. 2010, 4, 666–684. [Google Scholar] [CrossRef] [Green Version]
- Crepaldi, C.; Giuliani, A.; Milan, M.S.; Marchionna, N.; Piasentin, P.; Ronco, C. Remote Patient Management in Peritoneal Dialysis: Impact on Clinician’s Practice and Behavior. Contrib. Nephrol. 2019, 197, 44–53. [Google Scholar] [CrossRef]
- Brunetti, N.D.; Dellegrottaglie, G.; Lopriore, C.; Di Giuseppe, G.; De Gennaro, L.; Lanzone, S.; Di Biase, M. Prehospital telemedicine electrocardiogram triage for a regional public emergency medical service: Is it worth it? A preliminary cost analysis. Clin. Cardiol. 2014, 37, 140–145. [Google Scholar] [CrossRef]
- Chipps, J.; Brysiewicz, P.; Mars, M. A systematic review of the effectiveness of videoconference-based tele-education for medical and nursing education. Worldviews Evid. Based Nurs. 2012, 9, 78–87. [Google Scholar] [CrossRef]
- Hsieh, J.C.; Hsu, M.W. A cloud computing based 12-lead ECG telemedicine service. BMC Med. Inform. Decis. Mak. 2012, 12, 77. [Google Scholar] [CrossRef] [Green Version]
- Otto, C.A.; Shemenski, R.; Drudi, L. Real-time tele-echocardiography: Diagnosis and management of a pericardial effusion secondary to pericarditis at an Antarctic research station. Telemed. J. E Health 2012, 18, 521–524. [Google Scholar] [CrossRef]
- Brunetti, N.D.; Di Pietro, G.; Aquilino, A.; Bruno, A.I.; Dellegrottaglie, G.; Di Giuseppe, G.; Lopriore, C.; De Gennaro, L.; Lanzone, S.; Caldarola, P.; et al. Pre-hospital electrocardiogram triage with tele-cardiology support is associated with shorter time-to-balloon and higher rates of timely reperfusion even in rural areas: Data from the Bari- Barletta/Andria/Trani public emergency medical service 118 registry on primary angioplasty in ST-elevation myocardial infarction. Eur. Heart J. Acute Cardiovasc. Care 2014, 3, 204–213. [Google Scholar] [CrossRef] [PubMed]
- Singh, M.; Agarwal, A.; Sinha, V.; Kumar, R.M.; Jaiswal, N.; Jindal, I.; Pant, P.; Kumar, M. Application of Handheld Tele-ECG for Health Care Delivery in Rural India. Int. J. Telemed. Appl. 2014, 2014, 981806. [Google Scholar] [CrossRef]
- Noubiap, J.J.; Jingi, A.M.; Kengne, A.P. Local innovation for improving primary care cardiology in resource-limited African settings: An insight on the Cardio Pad project in Cameroon. Cardiovasc. Diagn. Ther. 2014, 4, 397–400. [Google Scholar] [CrossRef]
- Büscher, C.; Elsner, J.; Schneiders, M.T.; Thelen, S.; Brodziak, T.; Seidenberg, P.; Schilberg, D.; Tobias, M.; Jeschke, S. The Telemedical Rescue Assistance System “TemRas”—Development, first results, and impact. Biomed. Tech. 2014, 59, 113–123. [Google Scholar] [CrossRef]
- Chandra, B.S.; Sastry, C.S.; Jana, S. Reliable resource-constrained telecardiology via compressive detection of anomalous ECG signals. Comput. Biol. Med. 2015, 66, 144–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lapão, L.V.; Correia, A. Improving Access to Pediatric Cardiology in Cape Verde via a Collaborative International Telemedicine Service. Stud. Health Technol. Inform. 2015, 209, 51–57. [Google Scholar]
- De la Torre-Díez, I.; Lopez-Coronado, M.; Garcia-Zapirain, S.B.; Mendez-Zorrilla, A. Secure Cloud-Based Solutions for Different eHealth Services in Spanish Rural Health Centers. J. Med. Int. Res. 2015, 17, e157. [Google Scholar] [CrossRef] [PubMed]
- Muehlberg, F.; Neumann, D.; von Knobelsdorff-Brenkenhoff, F.; Traber, J.; Alwardt, N.; Schulz-Menger, J. A multicenter cardiovascular MR network for tele-training and beyond: Setup and initial experiences. J. Am. Coll. Radiol. 2015, 8, 876–883. [Google Scholar] [CrossRef] [PubMed]
- Riley, W.T.; Keberlein, P.; Sorenson, G.; Mohler, S.; Tye, B.; Ramirez, A.S.; Carroll, M. Program evaluation of remote heart failure monitoring: Healthcare utilization analysis in a rural regional medical center. Telemed. J. E Health 2015, 21, 157–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagayoshi, Y.; Oshima, S.; Ogawa, H. Clinical Impact of Telemedicine Network System at Rural Hospitals Without On-Site Cardiac Surgery Backup. Telemed. J. E Health 2016, 22, 960–964. [Google Scholar] [CrossRef]
- Shetty, R.; Samant, J.; Nayak, K.; Maiya, M.; Reddy, S. Feasibility of Telecardiology Solution to Connect Rural Health Clinics to a Teaching Hospital. Indian J. Community Med. 2017, 42, 170–173. [Google Scholar] [CrossRef]
- De la Torre-Díez, I.; Garcia-Zapirain, B.; López-Coronado, M.; Rodrigues, J.J.P.C. Proposing Telecardiology Services on Cloud for Different Medical Institutions: A Model of Reference. Telemed. J. E Health 2017, 23, 654–661. [Google Scholar] [CrossRef]
- Pyles, L.; Hemmati, P.; Pan, J.; Yu, X.; Liu, K.; Wang, J.; Tsakistos, A.; Zheleva, B.; Shao, W.; Ni, Q. Initial Field Test of a Cloud-Based Cardiac Auscultation System to Determine Murmur Etiology in Rural China. Pediatr. Cardiol. 2017, 38, 656–662. [Google Scholar] [CrossRef]
- Chauhan, V.; Negi, P.C.; Raina, S.; Raina, S.; Bhatnagar, M.; Guleri, R.; Kanwar, V.; Pandey, K.S. Smartphone-based tele-electrocardiography support for primary care physicians reduces the pain-to-treatment time in acute coronary syndrome. J. Telemed. Telecare 2018, 24, 540–546. [Google Scholar] [CrossRef]
- Pineda-López, F.; Martínez-Fernández, A.; Rojo-Álvarez, J.L.; García-Alberola, A.; Blanco-Velasco, M. A Flexible 12-Lead/Holter Device with Compression Capabilities for Low-Bandwidth Mobile-ECG Telemedicine Applications. Sensors 2018, 18, 3773. [Google Scholar] [CrossRef] [Green Version]
- Ganapathy, K.; Alagappan, D.; Rajakumar, H.; Dhanapal, B.; Rama, S.G.; Nukala, L.; Premanand, S.; Veerla, K.M.; Kumar, S.; Thaploo, V. Tele-Emergency Services in the Himalayas. Telemed. J. E Health 2019, 25, 380–390. [Google Scholar] [CrossRef]
- Ohligs, M.; Stocklassa, S.; Rossaint, R.; Czaplik, M.; Follmann, A. Employment of Telemedicine in Nursing Homes: Clinical Requirement Analysis, System Development and First Test Results. Clin. Interv. Aging 2020, 15, 1427–1437. [Google Scholar] [CrossRef]
- Walsh, J.A.; Warren, K.S. Selective primary health care: An interim strategy for disease control in developing countries. N. Engl. J. Med. 1979, 301, 967–974. [Google Scholar] [CrossRef]
- Kuwayama, T.; Hamabata, K.; Kamesaki, T.; Koike, S.; Kotani, K. Research on Home Care Nursing in Japan Using Geographic Information Systems: A Literature Review. Jpn. Clin. Med. 2018, 9, 1179670718814539. [Google Scholar] [CrossRef]
- Lazarus, G.; Kirchner, H.L.; Siswanto, B.B. Prehospital tele-electrocardiographic triage improves the management of acute coronary syndrome in rural populations: A systematic review and meta-analysis. J. Telemed. Telecare 2020, 30, 1357633X20960627. [Google Scholar] [CrossRef]
- Dowie, R.; Mistry, H.; Young, T.A.; Weatherburn, G.C.; Gardiner, H.M.; Rigby, M.; Rowlinson, G.V.; Franklin, R.C. Telemedicine in pediatric and perinatal cardiology: Economic evaluation of a service in English hospitals. Int. J. Technol. Assess. Health Care 2007, 23, 116–125. [Google Scholar] [CrossRef]
- Yang, Y.; Islam, S.U.; Noor, A.; Khan, S.; Afsar, W.; Nazir, S. Influential Usage of Big Data and Artificial Intelligence in Healthcare. Comput. Math. Methods Med. 2021, 2021, 5812499. [Google Scholar] [CrossRef]

{kind=link}
| No. | Author (Reference) | Year | Country (Continent) | Equipment | Main Findings | Classified Field | Usage Method and Used Population | Clinical Outcome |
|---|---|---|---|---|---|---|---|---|
| 1 | Hsieh et al. [16] | 2012 | Taiwan (Asia) | A new cloud and pervasive computing-based 12-lead ECG telemedical service | The inclusion of new cloud service in ECG telemedical service, an ECG tele-diagnosis via cellphone, and cloud-based 12-lead ECG e-learning; upgrades previously developed applications, facilitates the collaboration of hospitals, and enhances the efficacy of telemedical system. | Telemedical system | Network among ambulance, clinic, and hospital by cloud system | Diagnosis on ECG |
| 2 | Otto et al. [17] | 2012 | USA (North America) | Telehealth consultation at the level of a rural community hospital | Real-time tele-ultrasound consultation can serve as an important diagnostic resource in remote environments. | Tele-consultation | Rural doctor to urban specialist by tele-ultrasound consultation | Diagnosis on echocardiology |
| 3 | Brunetti et al. [18] | 2014 | Italy (Europe) | A registry of prehospital triage of patients with ST-segment elevation myocardial infarction | Time to treatment in patients who received prehospital triage with the tele-cardiology ECG is significantly shorter, and rates of patients timely treated are higher. | Prehospital triage | Ambulance to catheterization laboratory for primary PCI by tele-medicine service | Treatment of ACS |
| 4 | Singh et al. [19] | 2014 | India (Asia) | Clinical validation of handheld (portable) tele-ECG as a screening tool | The tele-ECG method shows similar results with conventional ECG, with 99% correlation. Tele-ECG is a portable, cost-effective, and convenient tool for monitoring heart diseases. | Monitoring system | Patient to remote centers by portable tele-ECG | Diagnosis on ECG |
| 5 | Noubiap et al. [20] | 2014 | South Africa (Africa) | Telemedical strategies for using a Cardionet system in developed locally | A tele-cardiology device provides several advantages in terms of cost, ease of use, autonomy, and reduced technology requirements. Test results are transferred wirelessly via mobile phone connection to specialist physicians who can interpret them and provide assistance with case management. | Telemedical system | Network among cardiologist, remote hospital, and remote center by Cardionet system (Cloudnet system) | Diagnosis on ECG |
| 6 | Büscher et al. [21] | 2014 | Germany (Europe) | Telemedical rescue assistance system in German emergency medical services | Telemedical rescue assistance system can transmit audio and video data as well as vital signs and 12-lead ECG from the emergency site to a teleconsultation center for patients with ACS. | Prehospital triage | Ambulance to teleconsultation center by telemedical rescue assistance system | Treatment of ACS |
| 7 | Chandra et al. [22] | 2015 | India (Asia) | Two-tier framework enabling reliable resource-constrained telecardiology with limited power and bandwidth in rural communities | High reliability is maintained even at substantial power and bandwidth savings in a monitoring system in India. | Monitoring system | ECG signal transmission from user end to diagnostic center (mainly technical system, population not specified) | Improvement of technical system |
| 8 | Lapão et al. [23] | 2015 | Portugal (Europe) | International tele-consultation services in supporting the evacuation procedures from Africa to Europe | This study provides evidence (e.g., case study, interview, cost reduction) of the importance of telemedicine for coping with both geographical constraints and shortage of physicians. | Tele-consultation | Rural doctor to urban specialist by international telemedicine service | Diagnosis of heart disease |
| 9 | De la Torre-Diez et al. [24] | 2015 | Spain (Europe) | Cloud system called eHealth Services in Spanish rural health centers | This telemedical system provides all information on the cloud in patients at a local area for health care staff and they could transparently check any data. | Telemedical system | Network among rural health centers by electronic health records (cloud) | Diagnosis of heart disease |
| 10 | Muehlberg et al. [25] | 2015 | Germany (Europe) | Tele-training trial for cardiovascular magnetic resonance | Network teaching reduced off-site training to only five weeks and provided an efficient teaching platform with a minimum of off-site time for trainees in rurally located institutions. | Tele-training | Fellows teach trainees by module-based network | Diagnosis on magnetic resonance |
| 11 | Riley et al. [26] | 2015 | USA (North America) | Remote monitoring for heart failure patients in a single center | Heart-failure patients with remote monitoring mobile devices showed substantial and statistically significant reductions in health care utilization compared with those who declined to participate. | Monitoring system | Monitor for heart-failure patients by broadband-enabled remote monitoring devices | Diagnosis of Heart failure |
| 12 | Nagayoshi et al. [27] | 2016 | Japan (Asia) | Benefit and utility of a Digital Imaging and Communications in Medicine tele-consultation network at a rural hospital | Ten cases (20.8%) of 48 tele-consultations that had been conducted were transferred to a high-volume center. The tele-consultation network enabled open communication between distant hospitals. | Tele-consultation | Rural low-volume hospitals to high-volume centers by broadband network | Network on DICOM |
| 13 | Shetty et al. [28] | 2017 | India (Asia) | Feasibility of tele-consultation to link rural clinics to a teaching hospital | ECGs were transmitted to the hospital with 99.7% success on first attempt. The staff at the hospital were able to provide timely interpretation of ECGs and advice to patients. | Tele-consultation | Rural clinics to city hospital by tele-ECG system | Diagnosis on ECG |
| 14 | De la Torre-Diez et al. [29] | 2017 | Spain (Europe) | Cloud-based telemedical system solution in a hospital, a health center in a city, and health centers in a rural area | ICT software simulated different scenarios to provide an adapted solution in the form of a telemedical service. | Telemedical system | Rural hospital to city health center by mobile-ECG telemedicine application | Diagnosis of heart disease |
| 15 | Pyles et al. [30] | 2017 | China (Asia) | A system to allow rural physicians to obtain assistance in the diagnosis and management of children with heart disease | The project tested the hypothesis that acceptable screening of heart murmurs could be accomplished using a digital stethoscope and internet cloud transmittal to deliver phonocardiograms to an experienced observer. The overall test accuracy was 91% with 78.5% sensitivity and 92.6% specificity. | Tele-training | From remote clinic to regional cardiology center by HeartLink tele-auscultation system (tablet and computer) | Diagnosis of heart disease in children |
| 16 | Cauhan et al. [31] | 2018 | India (Asia) | Whether to reduce the time taken for diagnosis of acute coronary syndrome using 24 h tele-ECG-consultation support | The hospital-to-aspirin time of the tele-consultations group was significantly reduced compared with the control group. This is an effective, low-cost, and replicable strategy. | Tele-consultation | Primary care physicians to specialist physician by tele-ECG system | Treatment of ACS |
| 17 | Pineda-Lopz et al. [32] | 2018 | Spain (Europe) | 12-lead ECG recording and monitoring system using mobile phones | The 32-bit mobile microcontroller ECG system can be especially useful in rural areas in developing countries. | Monitoring system | Monitor for patient’s 12-lead/Holter data by cellphone and webserver | Diagnosis of heart disease |
| 18 | Ganapathy et al. [33] | 2019 | India (Asia) | 24 h tele-emergency consultation services at an altitude over 3000 m | 753 teleconsults were given in the first 35 months, and several cases were transferred to larger centers or required helicopter transfer. | Tele-consultation | Regional hospital to community health center by tele-emergency services | Diagnosis of heart disease |
| 19 | Ohligs et al. [34] | 2020 | Germany (Europe) | A holistic tele-consultation system for nursing home residents | This telemedical system applied video telephony, electrocardiography, and assessment of vitals for general practitioners | Tele-consultation | Nurses in nursing homes to general practitioner by exclusive telemedical system | Diagnosis of heart disease |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamano, T.; Kotani, K.; Kitano, N.; Morimoto, J.; Emori, H.; Takahata, M.; Fujita, S.; Wada, T.; Ota, S.; Satogami, K.; et al. Telecardiology in Rural Practice: Global Trends. Int. J. Environ. Res. Public Health 2022, 19, 4335. https://doi.org/10.3390/ijerph19074335
Yamano T, Kotani K, Kitano N, Morimoto J, Emori H, Takahata M, Fujita S, Wada T, Ota S, Satogami K, et al. Telecardiology in Rural Practice: Global Trends. International Journal of Environmental Research and Public Health. 2022; 19(7):4335. https://doi.org/10.3390/ijerph19074335
Chicago/Turabian StyleYamano, Takashi, Kazuhiko Kotani, Naomi Kitano, Junko Morimoto, Hiroki Emori, Masahiro Takahata, Suwako Fujita, Teruaki Wada, Shingo Ota, Keisuke Satogami, and et al. 2022. "Telecardiology in Rural Practice: Global Trends" International Journal of Environmental Research and Public Health 19, no. 7: 4335. https://doi.org/10.3390/ijerph19074335
APA StyleYamano, T., Kotani, K., Kitano, N., Morimoto, J., Emori, H., Takahata, M., Fujita, S., Wada, T., Ota, S., Satogami, K., Kashiwagi, M., Shiono, Y., Kuroi, A., Tanimoto, T., & Tanaka, A. (2022). Telecardiology in Rural Practice: Global Trends. International Journal of Environmental Research and Public Health, 19(7), 4335. https://doi.org/10.3390/ijerph19074335