
Adolescent COVID-19 Vaccine Decision-Making among Parents in Southern California


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design, Participants, and Setting
2.2. Data Collection
2.3. Recruitment
2.4. Parent Survey and Focus Group Discussion Guide
2.5. Data Analysis
3. Results
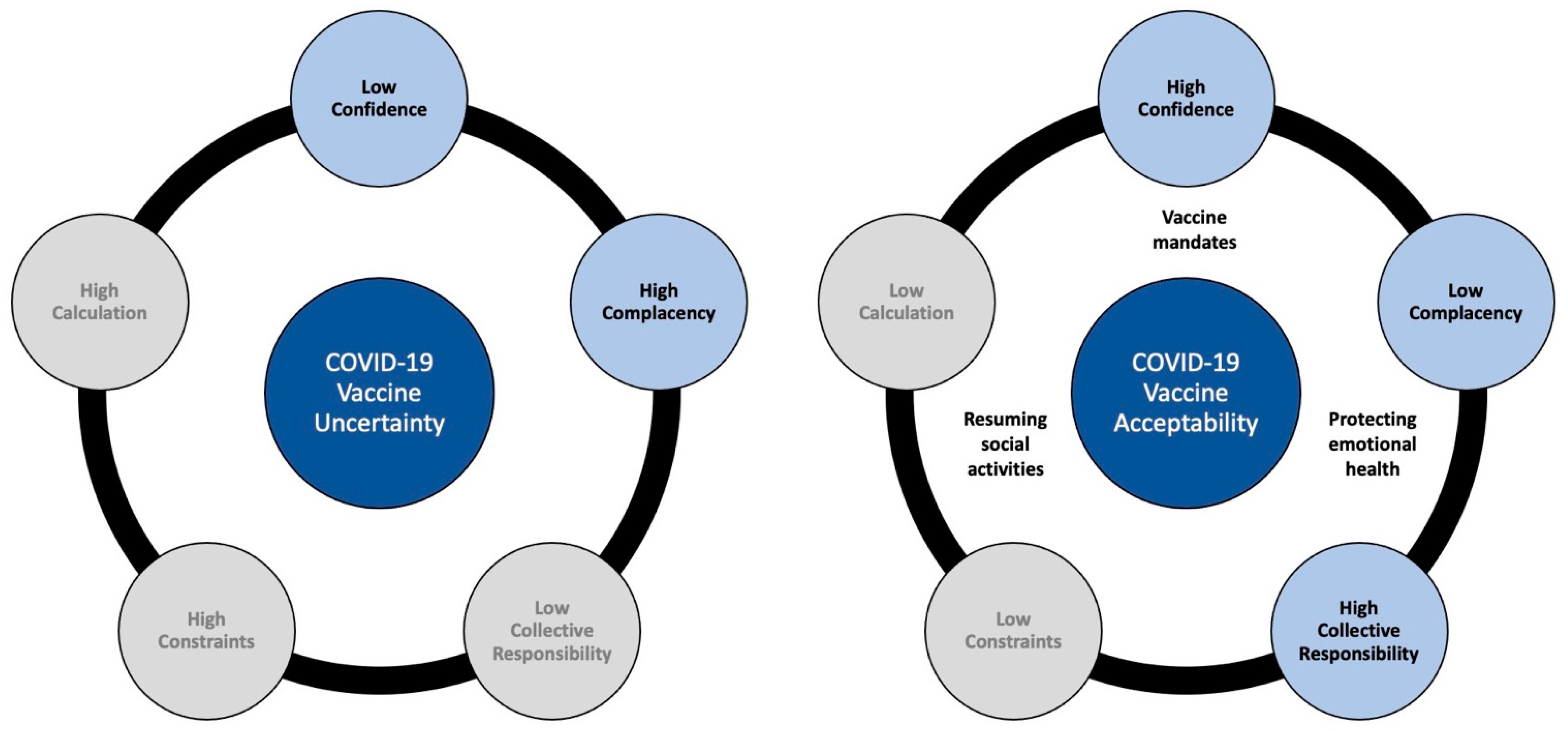
3.1. COVID-19 Vaccine Uncertainty
3.1.1. Low Confidence in the COVID-19 Vaccine
3.1.2. High Complacency regarding COVID-19 Disease Risk
3.2. COVID-19 Vaccine Acceptability
3.2.1. High Confidence in the COVID-19 Vaccine
3.2.2. Low Complacency regarding COVID-19 Disease Risk
3.2.3. High Collective Responsibility to Vaccinate
3.2.4. Vaccinating for Emotional Health
3.2.5. Vaccinating to Resume Social Activities
3.2.6. Vaccinating Due to Mandates
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Correction Statement
References
- US Census Quick Facts Percent Children under the Age of 18. 2020. Available online: https://www.census.gov/quickfacts/fact/table/US# (accessed on 3 February 2022).
- American Academy of Pediatrics (AAP). Children and COVID-19 Vaccination Trends: AAP Analysis of Data Posted by the Centers for Disease Control and Prevention (CDC) on All States Except Idaho as of December 29, 2021; AAP: Itasca, IL, USA, 2021. [Google Scholar]
- Aschwanden, C. Five reasons why COVID-19 herd immunity is probably impossible. Nature 2021, 591, 520–522. [Google Scholar] [CrossRef] [PubMed]
- Chu, V.; Yousaf, A.R.; Chang, K.; Schwartz, N.G.; McDaniel, C.J.; Lee, S.H.; Szablewski, C.M.; Brown, M.; Drenzek, C.L.; Dirlikov, E.; et al. Household transmission of SARS-CoV-2 from children and adolescents. N. Engl. J. Med. 2021, 385, 954–956. [Google Scholar] [CrossRef]
- Yonker, L.; Boucau, J.; Regan, J.; Choudhary, M.C.; Burns, M.D.; Young, N.; Farkas, E.J.; Davis, J.P.; Moschovis, P.P.; Kinane, T.B.; et al. Virologic features of SARS-CoV-2 infection in children. J. Infect. Dis. 2021, 224, 1821–1829. [Google Scholar] [CrossRef]
- Blanchard-Rohner, G.; Didierlaurent, A.; Tilmanne, A.; Smeesters, P.; Marchant, A. Pediatric COVID-19: Immunopathogenesis, transmission and prevention. Vaccines 2021, 9, 1002. [Google Scholar] [CrossRef] [PubMed]
- Cooper, D.M.; Afghani, B.; Byington, C.L.; Cunningham, C.K.; Golub, S.; Lu, K.D.; Radom-Aizik, S.; Ross, L.F.; Singh, J.; Smoyer, W.E.; et al. SARS-CoV-2 vaccine testing and trials in the pediatric population: Biologic, ethical, research, and implementation challenges. Pediatric Res. 2021, 90, 966–970. [Google Scholar] [CrossRef] [PubMed]
- Ladhani, S. Crossing the rubicon: A fine line between waiting and vaccinating adolescents against COVID-19. J. Infect. 2021, 83, 294–297. [Google Scholar] [CrossRef] [PubMed]
- Shiri, T.; Evans, M.; Talarico, C.A.; Morgan, A.R.; Mussad, M.; Buck, P.O.; McEwan, P.; Strain, W.D. Vaccinating adolescents and children significantly reduces COVID-19 morbidity and mortality across all ages: A population-based modeling study using the UK as an example. Vaccines 2021, 9, 1180. [Google Scholar] [CrossRef] [PubMed]
- AAP. Children and COVID-19: State Data Report; AAP and Children’s Hospital Association: Itasca, IL, USA, 2021. [Google Scholar]
- Delahoy, M.; Ujamaa, D.; Whitaker, M.; O’Halloran, A.; Anglin, O.; Burns, E.; Cummings, C.; Holstein, R.; Kambhampati, A.K.; Milucky, J.; et al. Hospitalizations associated with COVID-19 among children and adolescents—COVID-NET, 14 states, March 1, 2020–August 14, 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 1255–1260. [Google Scholar] [CrossRef]
- Tsabouri, S.; Makis, A.; Kosmeri, C.; Siomou, E. Risk factors for severity in children with Coronavirus disease 2019: A comprehensive literature review. Pedatric Clin. N. Am. 2021, 68, 321–338. [Google Scholar] [CrossRef]
- AAP. Children and COVID-19 State Data Report; American Academy of Pediatrics: Itasca, IL, USA, 2021. [Google Scholar]
- McCormick, D.; Richardson, L.C.; Young, P.R.; Viens, L.J.; Gould, C.V.; Kimball, A.; Pindyck, T.; Rosenblum, H.G.; Siegel, D.A.; Vu, Q.M.; et al. Deaths in children and adolescents associated with COVID-19 and MIS-C in the United States. Pediatrics 2021, 148, e2021052273. [Google Scholar] [CrossRef] [PubMed]
- Payne, A.; Gilani, Z.; Godfred-Cato, S.; Belay, E.D.; Feldstein, L.R.; Patel, M.M.; Randolph, A.G.; Newhams, M.; Thomas, D.; Magleby, R.; et al. Incidence of Multisystem Inflammatory Syndrome in Children among US Persons infected with SARS-CoV-2. JAMA Netw. Open 2021, 4, e2116420. [Google Scholar] [CrossRef] [PubMed]
- Hause, A.M.; Gee, J.; Baggs, J.; Abara, W.E.; Marquez, P.; Thompson, D.; Su, J.R.; Licata, C.; Rosenblum, H.G.; Myers, T.R.; et al. COVID-19 vaccine safety in adolescents aged 12–17 years—United States, December 14, 2020–July 16, 2021. In Morbidity and Mortality Weekly Report; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2021; pp. 1053–1058. [Google Scholar]
- Parker, D.M.; Bruckner, T.; Vieira, V.M.; Medina, C.; Minin, V.N.; Felgner, P.L.; Dratch, A.; Zahn, M.; Bartell, S.M.; Boden-Albala, B. Predictors of test positivity, mortality, and seropositivity during the early Coronavirus disease epidemic, Orange County, CA, USA. Emerg. Infect. Dis. 2021, 27, 2604–2618. [Google Scholar] [CrossRef] [PubMed]
- Together, O.H. Population by Language Spoken at Home; OC Healthier Together Dashboard: Orange County, CA, USA, 2022. [Google Scholar]
- William, D. Recall, Special Elections: Looking Back on the Year in Orange County Politics. 2022. Available online: https://spectrumnews1.com/ca/orange-county/politics/2022/01/04/orange-county-politics--2021-in-review (accessed on 6 February 2022).
- Pfizer. Pfizer-Biontech Announces Positive Toplinei Results of Pivotal COVID-19 Vaccine Study in Adolescents; Pfizer: Mainz, Germany, 2021. [Google Scholar]
- Scherer, A.; Gedlinske, A.M.; Parker, A.M.; Gidengil, C.A.; Askelson, N.M.; Petersen, C.A.; Woodworth, K.R.; Lindley, M.C. Acceptability of Adolescent COVID-19 Vaccination among Adolescents and Parents of Adolescents—United States, April 15–23, 2021. In Morbidity and Morality Weekly Report; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2021; pp. 997–1003. [Google Scholar]
- FDA. Coronavirus (COVID-19) Update: FDA Authorizes Pfizer-BioNTech COVID-19 Vaccine for Emergency Use in Adolescents in Another Important Action in Fight against Pandemic; US Food & Drug Administration: Silver Spring, MD, USA, 2021.
- Montalti, M.; Rallo, F.; Guaraldi, F.; Bartoli, L.; Po, G.; Stillo, M.; Perrone, P.; Squillace, L.; Dallolio, L.; Pandolfi, P.; et al. Would parents get their children vaccinated against SARS-CoV-2? Rate and predictors of vaccine hesitancy according to a survey over 5000 families from Bologna, Italy. Vaccines 2021, 9, 366. [Google Scholar] [CrossRef] [PubMed]
- Yigit, M.; Ozkaya-Parlakay, A.; Senel, E. Evaluation of COVID-19 vaccine refusal in parents. Pediatric Infect. Dis. J. 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.; Steele, J.M.; Fonseca, B.; Huang, S.; Shah, S.; Maskatia, S.A.; Buddhe, S.; Misra, N.; Ramachandran, P.; Gaur, L.; et al. COVID-19 vaccination—Associated myocarditis in adolescents. Pediatrics 2021, 148, e2021053427. [Google Scholar] [CrossRef] [PubMed]
- CDC. Clinical Considerations: Myocarditis and Pericarditis after Receipt of mRNA COVID-19 Vaccines among Adolescents and Young Adults; Department of Immunization and Vaccines, CDC: Atlanta, Georgia, 2021. [Google Scholar]
- Betsch, C.; Schmid, P.; Heinemeier, D.; Korn, L.; Holtmann, C.; Böhm, R. Beyond confidence: Development of a measure assessing the 5C psychological antecedents of vaccination. PLoS ONE 2018, 13, e0208601. [Google Scholar] [CrossRef] [PubMed]
- Tracy, S.J. Data analysis basics: A phronetic iterative approach. In Qualitative Research Methods: Collecting Evidence, Crafting Analysis, Communicating Impact; Tracy, S.J., Ed.; John Wiley and Sons: Hoboken, NJ, USA, 2019; pp. 208–235. [Google Scholar]
- Tracy, S.J. A phronetic iterative approach to data analysis in qualitative research. J. Qual. Res. 2018, 19, 61–76. [Google Scholar]
- Tracy, S.J. Advanced data analysis: The art and magic of interpretation. In Qualitative Research Methods: Collecting Evidence, Crafting Analysis, Communicating Impact; Tracy, S.J., Ed.; John Wiley and Sons: Hoboken, NJ, USA, 2019; pp. 236–264. [Google Scholar]
- Hennink, M.M.; Kaiser, B.N.; Weber, M.B. What influences saturation? Estimating sample sizes in focus group research. Qual. Health Res. 2019, 29, 1483–1496. [Google Scholar] [CrossRef]
- Murthy, B.; Zell, E.; Saelee, R.; Murthy, N.; Meng, L.; Meador, S.; Reed, K.; Shaw, L.; Gibbs-Scharf, L.; Gibbs-Scharf, L.; et al. COVID-19 Vaccination Coverage among Adolescents Aged 12–17 Years—United States, December 14, 2020–July 31, 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 1206–1213. [Google Scholar] [CrossRef]
- OC Health Care Agency. COVID-19 Vaccination Status of Youths. COVID-19 Vaccination Status of Youths Age 12–17. 2022. Available online: https://ochca.maps.arcgis.com/apps/dashboards/8202b85d0e944b88af5a1140c9206031 (accessed on 30 January 2022).
- Plotkin, S.A.; Levy, O. Considering mandatory vaccination of children for COVID-19. Pediatrics 2021, 147, e2021050531. [Google Scholar] [CrossRef] [PubMed]
- CDC. Delta Variant: What We Know about the Science; Division of Viral Diseases, Centers for Disease Control and Prevention: Atlanta, GA, USA, 2021. Available online: https://stacks.cdc.gov/view/cdc/108671 (accessed on 3 February 2022).
- Latkin, C.; Dayton, L.; Yi, G.; Konstantopoulos, A.; Boodram, B. Trust in a COVID-19 vaccine in the U.S.: A social-ecological perspective. Soc. Sci. Med. 2021, 270, 113684. [Google Scholar] [CrossRef]
- Hopfer, S.; Fields, E.J.; Lu, Y.; Ramakrishnan, G.; Grover, T.; Bai, Q.; Huang, Y.; Li, C.; Mark, G. The social amplification and attenuation of COVID-19 risk perception shaping mask wearing behavior: A longitudinal Twitter analysis. PLoS ONE 2021, 16, e0257428. [Google Scholar] [CrossRef] [PubMed]
- Brandt, E.J.; Rosenberg, J.; Waselewski, M.E.; Amaro, X.; Wasag, J.; Chang, T. National study of youth opinions on vaccination for COVID-19 in the U.S. J. Adolesc. Health 2021, 68, 869–872. [Google Scholar] [CrossRef]
- Brewer, N.T.; Hall, M.E.; Malo, T.L.; Gilkey, M.B.; Quinn, B.; Lathren, C. Announcements versus conversations to improve HPV vaccination coverage: A randomized trial. Pediatrics 2017, 139, e20161764. [Google Scholar] [CrossRef] [PubMed]
- Hopfer, S.; Wright, M.; Pellman, H.; Wasserman, R.; Fiks, A.G. HPV vaccine recommendation profiles among a national network of pediatric practitioners: Understanding contributors to parental vaccine hesitancy and acceptance. Hum. Vaccine Immunother. 2019, 15, 1776–1783. [Google Scholar] [CrossRef] [PubMed]
- NCI-Designated Cancer Centers Call for Urgenet Action to Get HPV Vaccination Back on Track. 2021. Available online: https://www.asco.org/sites/new-www.asco.org/files/NCI-CC-Statement-HPV-2021.pdf (accessed on 2 November 2021).
- Malo, T.L.; Hall, M.E.; Brewer, N.T.; Lathren, C.R.; Gilkey, M.B. Why is announcement training more effective than conversation training for introducing HPV vaccination? A theory-based investigation. Implement. Sci. 2018, 13, 57–68. [Google Scholar] [CrossRef]
- Dempsey, A.; O’Leary, S. Human Papillomavirus Vaccination: Narrative review of studies on how providers’ vaccine communication affects attitudes and uptake. Acad. Pediatrics 2018, 18, S23–S27. [Google Scholar] [CrossRef]
- Wilkinson, D.; Finlay, I.; Pollard, A.J.; Forsberg, L.; Skelton, A. Should we delay COVID-19 vaccination in children? Br. Med. J. 2021, 374, n1687. [Google Scholar] [CrossRef] [PubMed]
- Carson, S.; Casillas, A.; Castellon-Lopez, Y.; Mansfield, L.N.; Morris, D.; Barron, J.; Ntekume, E.; Landovitz, R.; Vassar, S.D.; Norris, K.C.; et al. COVID-19 vaccine decision-making factors in racial and ethnic minority communities in Los Angeles, California. J. Am. Med. Assoc. Netw. Open 2021, 4, e2127582. [Google Scholar] [CrossRef] [PubMed]
- Hamel, L.; Lopes, L.; Sparks, G.; Kirzinger, A.; Kearney, A.; Stokes, M.; Brodie, M. KFF COVID-19 Vaccine Monitor: October 2021; Kaiser Foundation: Oakland, CA, USA, 2021. [Google Scholar]
- Zimet, G.; Silverman, R.; Fortenberry, J.D. Coronavirus disease in 2019 and vaccination of children and adolescents: Prospects and challenges. J. Pediatrics 2021, 231, 254–258. [Google Scholar] [CrossRef]
- AuYoung, M.; Espinosa, P.R.; Chen, W.-T.; Juturu, P.; Young, M.-E.D.T.; Casillas, A.; Adkins-Jackson, P.; Hopfer, S.; Kissam, E.; Alo, A.K.; et al. Addressing racial/ethnic inequities in vaccine hesitancy and uptake: Lessons learned from the California Alliance against COVID-19. J. Behav. Med. 2022. [Google Scholar] [CrossRef] [PubMed]
- Saxena, S.; Skirrow, H.; Bedford, H.; Wighton, K. COVID-19 vaccines for teenagers: Conversations and consent. Br. Med. J. 2021, 374, n2312. [Google Scholar] [CrossRef] [PubMed]
- Hause, A.M.; Gee, J.; Johnson, T.; Jazwa, A.; Marquez, P.; Miller, E.; Su, J.; Shimabukuro, T.T.; Shay, D.K. Anxiety-related adverse event clusters after Janssen COVID-19 vaccination—Five US mass vaccination sites, April 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 685–688. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Topic | Example |
|---|---|
| Parent–Child Communication | I have asked my adolescent child about their thoughts and opinions regarding the COVID-19 vaccine. (5-point Likert scale) |
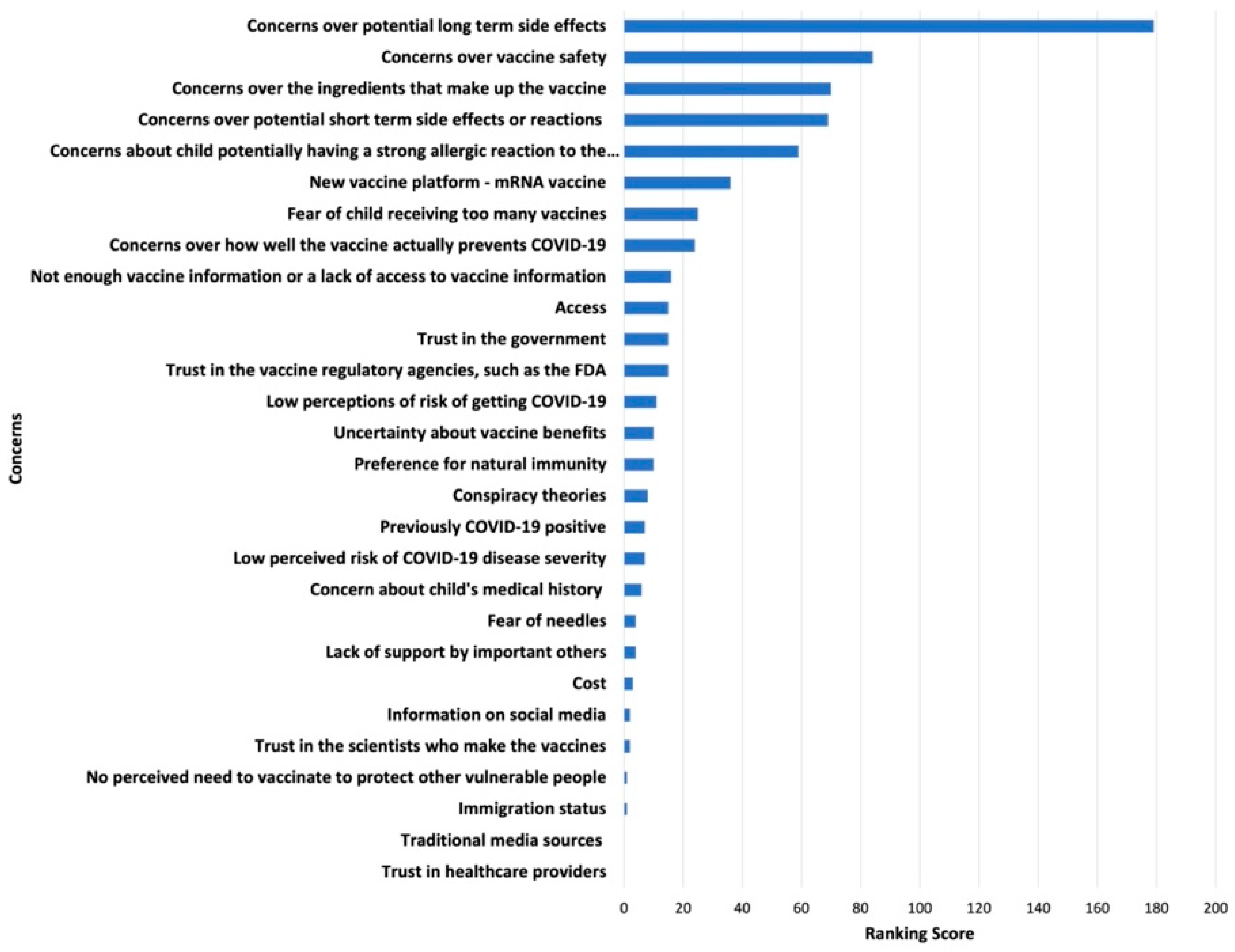
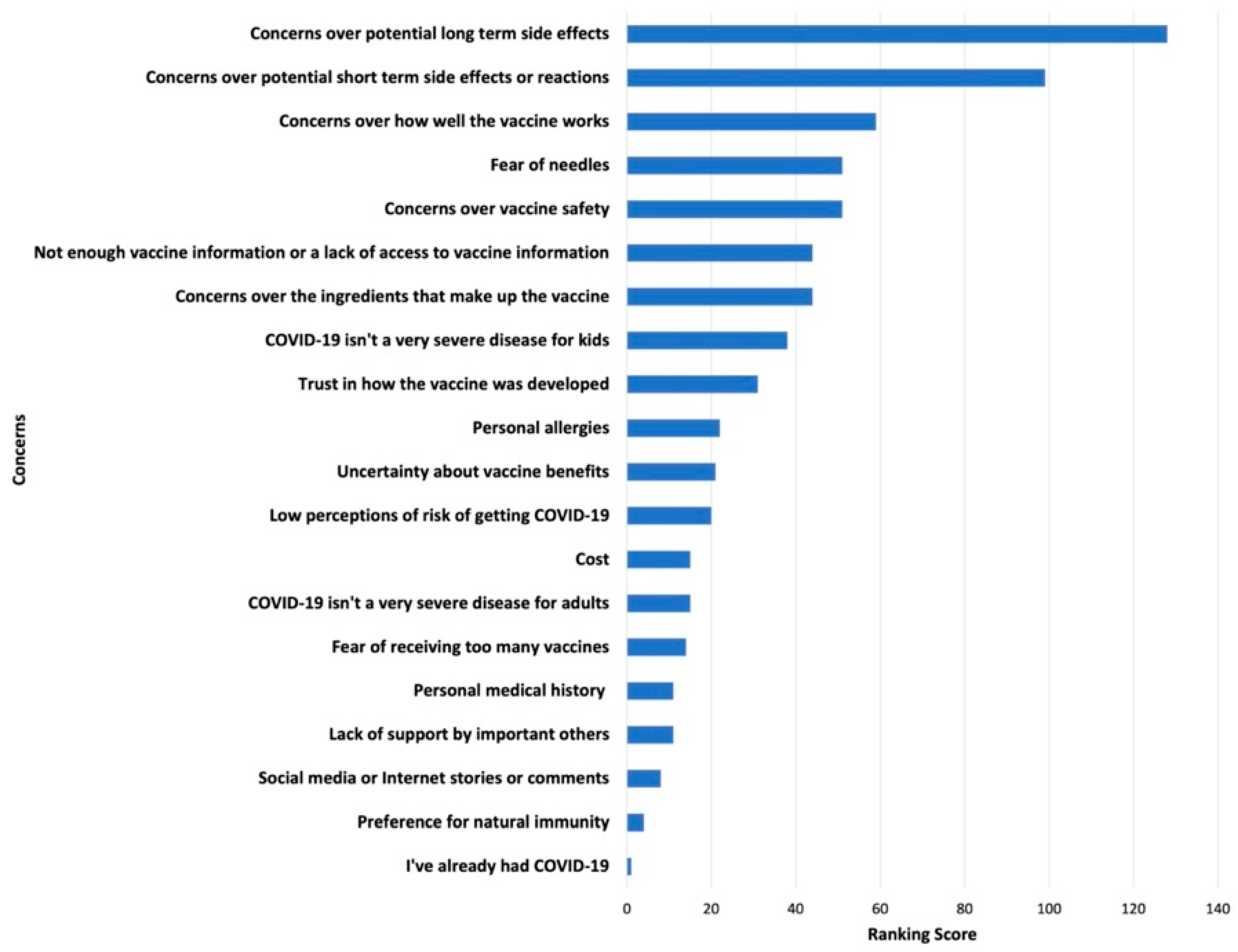
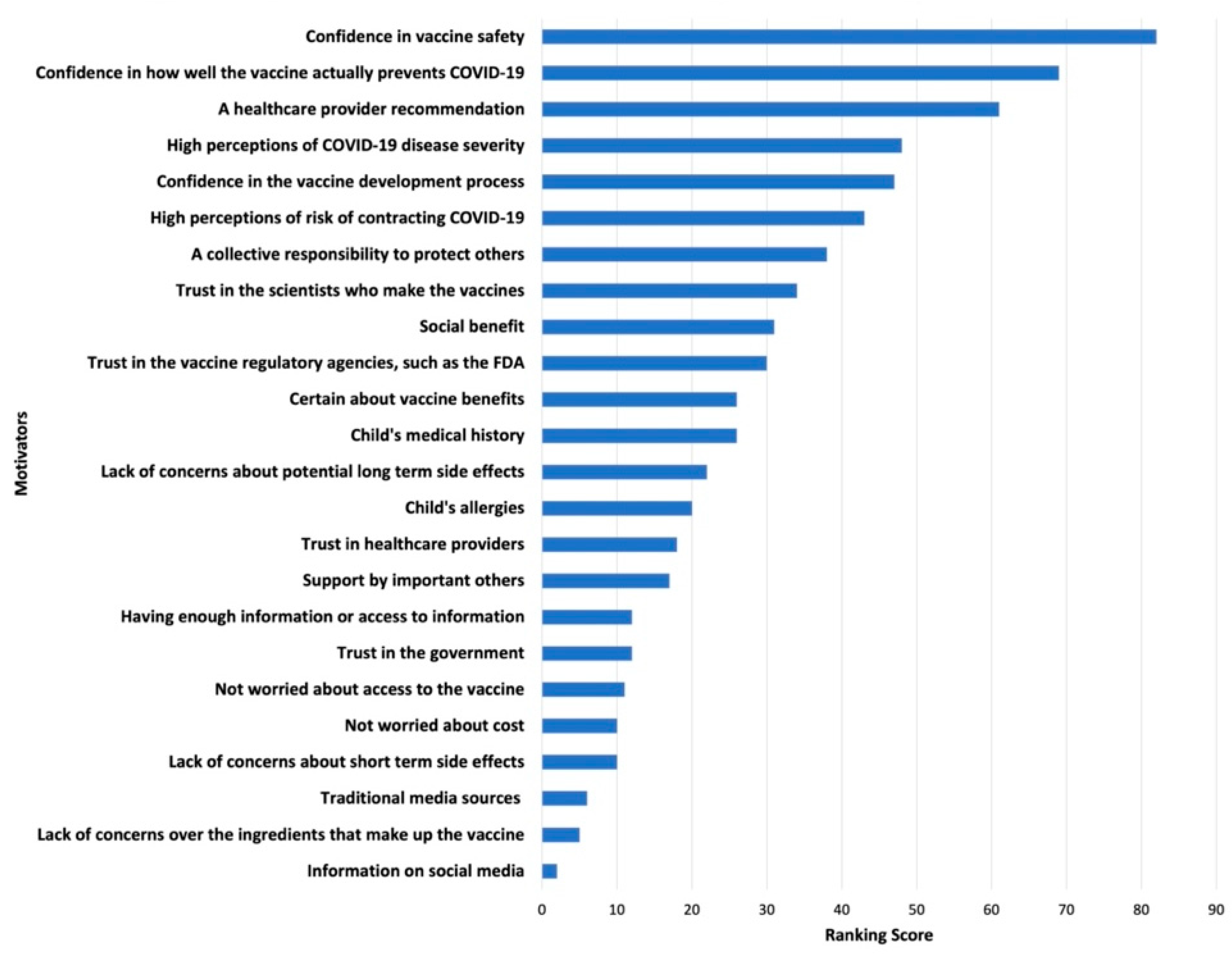
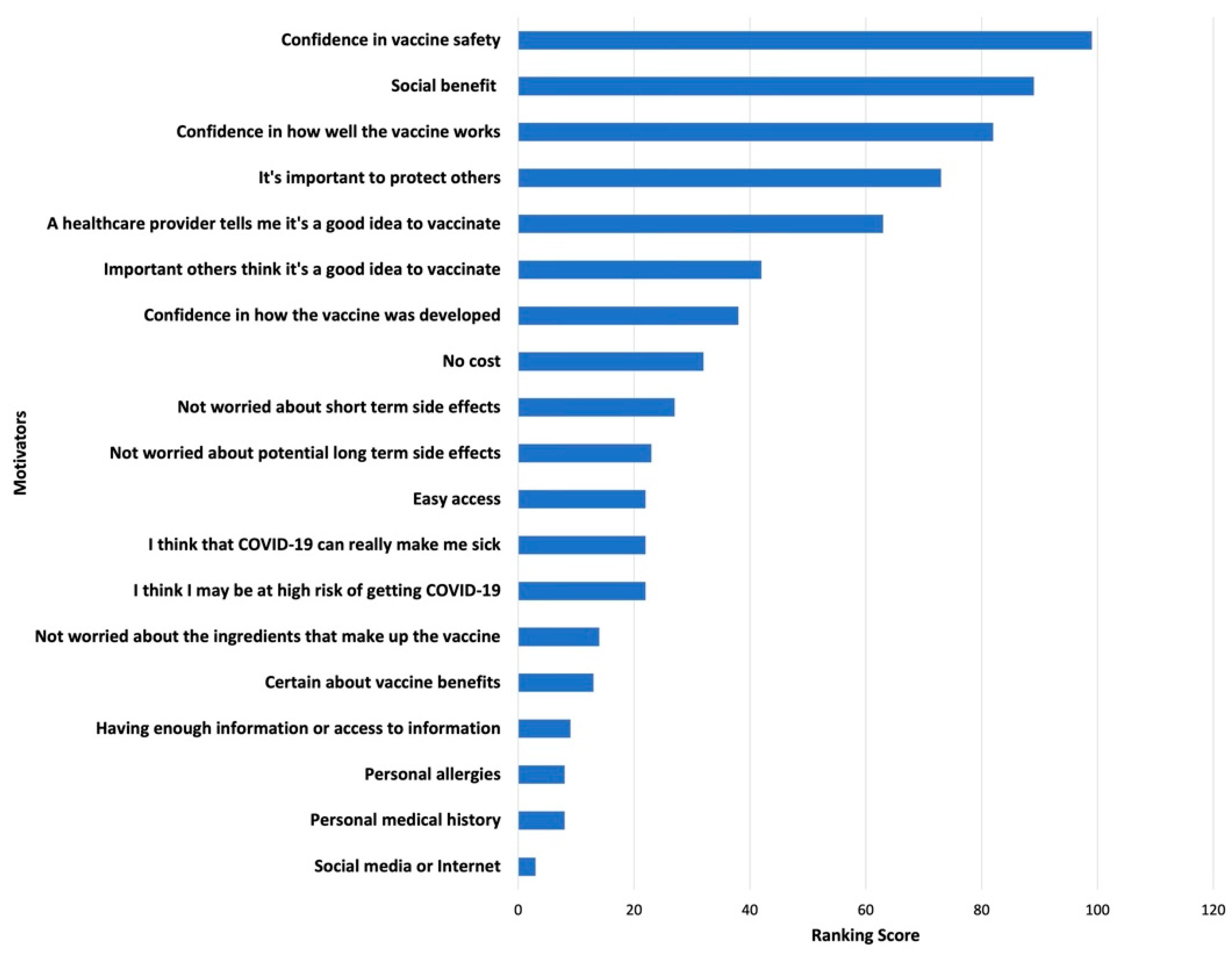
| Ranking Vaccine Concerns and Motivators (5C Vaccine Hesitancy Model) | When thinking about vaccinating your adolescent, please rank your top five COVID-19 vaccine concerns… |
| Confidence | Concerns over potential long-term side effects. Trust in health care providers. |
| Complacency | Low perceived risk of getting COVID-19. Low perceived risk of COVID-19 disease severity. |
| Constraints | Cost, access. |
| Collective Responsibility | No perceived need to vaccinate to protect vulnerable people. |
| Calculation | Uncertainty about vaccine benefits. |
| Parenting Style | In general, how are the most important health decisions made between you and your adolescent child? |
| Positive Expectancies | I think the COVID-19 vaccine will protect my adolescent child from the COVID-19 virus. (5-point Likert scale) |
| Vaccinating Under Conditions of Uncertainty | From information that I have been able to find, I think the COVID-19 vaccine is safe for my adolescent child. (5-point Likert scale) |
| Information Sources | Indicate how much you trust vaccine information from medical professionals. For example, doctors. (5-point Likert scale) |
| Topic | Example |
|---|---|
| General Vaccine Attitudes and Warm Up | Tell me about how you made the decision about whether or not to vaccinate your adolescent the last time you were asked to do so? |
| Parent COVID-19 Vaccine Decision Making | 5C Vaccine Hesitancy Model. |
| Confidence | Describe to me what you know about COVID-19 vaccine safety and effectiveness in adults and children. |
| Complacency | Describe your perspective on whether your adolescent needs the COVID-19 vaccine and whether you think your child is at risk for getting COVID-19. |
| Constraints | Tell me how confident you feel that you will be able to get your children vaccinated once it becomes available? |
| Tell me about any potential barriers that might impact you (e.g., insurance, cost, finding out where and when you can vaccinate your child, availability). | |
| Collective Responsibility | Tell me how helpful the vaccine will be for you, your child, your household or your community (e.g., herd immunity). |
| Calculation | Explain to me what you plan to do about vaccinating your adolescent once the vaccine becomes available and recommended? |
| Tell me about the things that you consider in your decision (e.g., the health of your child, the opinions of others, preference for natural immunity, etc.). | |
| Vaccine Acceptability After Emergency Use Authorization | What information or actions, if any, would make getting the vaccine more acceptable? |
| COVID-19 Vaccine Information Sources | Where or who do you turn to for information about the COVID-19 vaccine? |
| Vaccinating Children Younger than 12 Years (if applicable) | For those of you who have children under the age of 12 in the home, how are your decisions about whether or not to have them take the vaccine the same or different? |
| Demographics | n | % or M (SD) 1 |
|---|---|---|
| Parent age (in years) | - | 44.5 (6.1) |
| Adolescent age (in years) | - | 14.1 (1.7) |
| Parent gender | ||
| Female | 45 | 98 |
| Male | 1 | 2 |
| Adolescent gender | ||
| Female | 19 | 41 |
| Male | 26 | 57 |
| Transgender, male | 1 | 2 |
| Parent race and ethnicity | ||
| Latino | 22 | 48 |
| Caucasian | 13 | 28 |
| Asian | 9 | 20 |
| American Indian | 1 | 2 |
| Pacific Islander | 1 | 2 |
| Parent nativity status | ||
| U.S. born | 19 | 41 |
| Foreign born | 27 | 59 |
| Parent education | ||
| Less than high school | 1 | 2 |
| High school | 3 | 7 |
| Vocational or technical school | 1 | 2 |
| Some college | 3 | 7 |
| Associate degree | 4 | 9 |
| Bachelor’s degree | 11 | 24 |
| Graduate school | 23 | 50 |
| Parent occupation | ||
| Business | 13 | 28 |
| Education | 11 | 24 |
| Health care | 4 | 9 |
| Social services | 3 | 7 |
| Other | 15 | 33 |
| Multigenerational household | 13 | 28 |
| Adolescent school type | ||
| Public | 36 | 78 |
| Charter | 6 | 13 |
| Private | 4 | 9 |
| Adolescent schooling delivery mode | ||
| Online distance learning | 30 | 65 |
| In-person or hybrid | 16 | 35 |
| Adolescent chronic conditions | 10 | 22 |
| Asthma | 4 | 9 |
| Asperger’s | 1 | 2 |
| Mental illness | 2 | 4 |
| Epilepsy | 1 | 2 |
| Obesity | 1 | 2 |
| Seasonal allergies | 1 | 2 |
| Adolescent influenza vaccination status | ||
| Vaccinated in the past year | 31 | 67 |
| Not vaccinated in the past year | 15 | 33 |
| 5C Model Construct | Construct Details | Participant Quotes |
|---|---|---|
| Low confidence in the COVID-19 vaccine | Vaccine safety concerns: long-term side effects, exacerbating existing chronic conditions, vaccine ingredients, and more studies needed | “My concerns are just what the long-term side effects are and how each individual would react to it”—Parent 11 |
| “My daughter, like I said, the youngest one does have underlying issues and she already has things going on with her, so I don’t want to cause any more on her”—Parent 32 | ||
| “Because like I said, the ingredient, we don’t know what’s in it, so we don’t know how it’s gonna affect our children”—Parent 17 | ||
| “Well, for me personally it’s just a matter of time, and I want to see more testing—basically more people, just more studies being done, and of course, have more research articles coming out on the vaccine overall”—Parent 3 | ||
| Vaccine efficacy concerns | “The other thing that I wanted to mention was with all the variants coming through, you know, and so that was the other concern. Is this going to be effective, still be as effective with new variants?”—Parent 20 | |
| Trust concerns: mistrust in pharmaceutical companies, regulatory agencies, public health authorities, and health care providers | “This vaccine was developed super-fast. So, you know, I don’t have a lot of trust about that”—Parent 25 | |
| “If you’re on the J&J [Johnson & Johnson] panel, everyone’s expecting it [the vaccine] to be rolled out and in arms like next week. Who’s gonna be the one that’s like, ‘Well, I think that there might be a concern,’ so that does concern me a little bit because whistleblowing is hard enough”—Parent 15 | ||
| “There is a lot of business and tremendous politics involved in it, and that makes a common person worrisome—like OK, is the government or are the authorities really concerned about the common person’s health or is there big business involved in it and that’s why there is a lot of promotion to get the vaccine all of a sudden?”—Parent 19 | ||
| “It’s not just about public health at all or the good of the people. There’s just so many other factors involved, which, you know, unfortunately, in the area of public health, it shouldn’t be, but it is”—Parent 21 | ||
| “They [CDC] did not give us the accurate information to begin with. They said mask is not needed, but it was needed from the first day. So, I’m thinking about vaccine. They may say, no, the vaccine is not needed for younger children and when everybody goes back to normal, we may have a peak for people that are not vaccinated yet. That’s my concern”—Parent 13 | ||
| “Pfizer and Moderna had been kind of secretive; what’s in that vaccine is not really public knowledge, so that makes me suspicious. Why is it not common knowledge?”—Parent 3 | ||
| High complacency regarding COVID-19 disease risk | Low perceived risk of contracting SARS-CoV-2 | “My kids are still in distance learning … and so, I don’t think they’re at risk at this time”—Parent 36 |
| “She’ll have a higher than usual chance of getting it at college versus high school, middle school where they’re coming home, and you have some control of what they’re doing socially, so like right now, I don’t think she’s getting COVID any time before she leaves home”—Parent 15 | ||
| “As a family, we do everything wrong. We host parties. My son has a huge party. We had a huge party. We went to gather with family for the holiday. We travel. I purposely tried to get COVID, and I’m not getting it! Then I have people like my neighbor who are always home, and they have COVID. So, I just find it mind blowing, like, we are trying to get COVID! No masks, everywhere touching everything, especially my youngest with everything in his mouth, and we can’t get it, you know? [laughs] So, it’s like why the heck do we even need a vaccine?”—Parent 3 | ||
| “I don’t know if they need it. We were sick and they tested negative, all of the kids. I feel like for kids it’s a little bit … like their immune system. I don’t know if it’s—but all adults here got it and none of the kids did”—Parent 40 | ||
| COVID-19 perceived as a mild disease | “They are fine with COVID because my son, he doesn’t have, like, any chronic disease or no allergies, so I think he’s fine if he has it”—Parent 16 | |
| “Like I said, we don’t get sick very often, so I think their immune systems are pretty strong and that if they were to get it, they would have a good outcome”—Parent 37 | ||
| “We’ve seen it, I guess, with a lot of adolescents and they’re all fine—fine meaning it seems like it’s not even as bad as the flu”—Parent 15 | ||
| “Like, it is more of an inconvenience to be really honest with you, right, you know, it’s more of a like scarlet letter on your chest, right, you know what I mean, and an inconvenience in your life”—Parent 20 | ||
| “The COVID actually [is] not very harmful for the kid under 16, so for the COVID vaccine, I think like I said, I will wait maybe for one or more years”—Parent 17 | ||
| “You know, she is very young. Is it better just to get COVID, get it over with? And who knows if those antibodies last either, but they don’t, similarly, they don’t know what the vaccination is going to do. I don’t know, so we’re on the fence”—Parent 15 |
| Relevant 5C Model Construct | Construct Details | Participant Quotes |
|---|---|---|
| High confidence in the COVID-19 vaccine | Trust in health care providers; increasing confidence because an increasing number of others have vaccinated without complications; family norms to vaccinate | “I go with the recommendation, you know? As soon as it’s ready and available for our children, we’d certainly do it. My husband and I already agreed we’d all go do it”—Parent 14 |
| “I rely on the, you know, the expert advice of two people that I trust and personally, that’s my doctor and my children’s doctor”—Parent 2 | ||
| “Since I can remember, my parents have always taught me that vaccines are good. I’m educated as far as health. Regardless of what is said, whether they’re good or bad, the things I have learned since childhood is that vaccines are good”—Parent 23 | ||
| Low complacency regarding COVID-19 disease risk | Protecting the child’s health | “I’m more concerned actually about the virus”—Parent 4 |
| “Once my 14-year-old can get the vaccine, I’m going to feel even more relief, because he does have, you know, a lung issue, and I worry for him a lot because I’ve watched him over the years as we’ve had nebulizer treatments and, you know, there’s that cough that he gets, that’s so scary for us”—Parent 35 | ||
| “I want my children alive. I want them to have a future, and I want to be alive”—Parent 41 | ||
| “[Vaccinating] is healthy because they get sick less. Back then when they were going to school, you know that they’re sick it’s so uncomfortable even for you as an adult, to be at work or on the street, sneezing, blowing your nose. So, it prevents you from getting sick. That’s why we all decided to get immunized”—Parent 23 | ||
| High collective responsibility to vaccinate | Vaccinating for one’s social circle | “I would like them to have the vaccine, because we have to care about teachers, you know, school staff and others, too. It’s not only family members, it’s neighbors, you know, everyone, grocery staff everywhere”—Parent 12 |
| “I want my children to be protected and also, in a sense, you know, they’re protected and then they’re also protecting the people around them. So, I feel like it’s so critical, and I would like them to get vaccinated”—Parent 26 | ||
| “I would say he needs to be vaccinated. We also have, you know, an older parent living with us. … Some people get really sick, and it never seems to be something that is really predictable”—Parent 33 | ||
| “Yeah, that’s my feeling about my 14-year-old is that just how he could potentially spread it in the community, you know—if like over the summer he’s involved in sports and he’s with a group of kids, he gets it, and then, you know, he’s not wearing his mask and, you know, inadvertently spreads it to, you know, somebody who’s not able to fight it off or whatever or wasn’t able to get the vaccine for whatever reason, and you know, and if something ever happened to somebody else as a result of my son, that would be really difficult”—Parent 35 |
| Theme | Participant Quotes |
|---|---|
| Protecting child’s and adult’s emotional health | “My son plays sports and so far, we do take him for his games, but there’s always a constant fear. What if he contracts it, right? He may not get impacted, but if he’s a carrier and we get it, then what happens, right? So yeah, that might be one benefit of getting your child vaccinated—that you don’t have to live in a constant fear”—Parent 16 |
| “At this point, mental health, not so much for the adults, but for children and teens in particular. Yeah, it’s been a challenge”—Parent 44 | |
| “I think mentally, too, it gives a sense of security, right, that we’re all protected to some extent”—Parent 46 | |
| “I think it [vaccinating] would be very helpful, has been like a sense of relief. At least just a little bit, you know, lowering that risk of exposure to my children and into the community because we, you know, like a lot of us, we don’t go out, but we go to church or we go to the supermarket and just want to do what I can at least on my part to … be safe”—Parent 32 | |
| Resuming social activities | “I feel bad for my senior. He lost half of 11th grade and now he’s a senior and applying for colleges and I feel like he’s going to still be a senior going into college. … I just feel so bad, you know. And my daughter, who graduated eighth grade, didn’t finish eighth grade, didn’t have her ceremony, and then now she’s a freshman and has not stepped foot on high school campus—has no idea. So, it’s almost like all of our kids are one grade behind mentally. … It’s like they lost an age”—Parent 26 |
| “It’s just the fact that once the child gets vaccinated, they can engage in more activities”—Parent 16 | |
| “My husband’s family, there are kind of a lot of seniors in the family, and they all got vaccinated. … They said if you don’t get the vaccine, you’re not welcome to the party”—Parent 12 | |
| “I don’t think I’m going to be the first one to line up for it, but I also want to be able to see people right, you know what I mean, and do certain things, so if that helps me or helps people be able to feel more comfortable, then I would consider it more”—Parent 20 | |
| Vaccine mandates | “I guess if it was mandated, for instance, to attend whether it’s high school or college or to fly, then obviously, you know, we’re going to get it”—Parent 15 |
| “It might be more related to things we value, rather than information. So, work opportunities or doing things that are important to us like being able to travel. We have family who are spread out both internationally and across the country, so if it was required for travel, we would because that that would supersede our perceived risk or hesitation to take it”—Parent 37 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hopfer, S.; Fields, E.J.; Ramirez, M.; Long, S.N.; Huszti, H.C.; Gombosev, A.; Boden-Albala, B.; Sorkin, D.H.; Cooper, D.M. Adolescent COVID-19 Vaccine Decision-Making among Parents in Southern California. Int. J. Environ. Res. Public Health 2022, 19, 4212. https://doi.org/10.3390/ijerph19074212
Hopfer S, Fields EJ, Ramirez M, Long SN, Huszti HC, Gombosev A, Boden-Albala B, Sorkin DH, Cooper DM. Adolescent COVID-19 Vaccine Decision-Making among Parents in Southern California. International Journal of Environmental Research and Public Health. 2022; 19(7):4212. https://doi.org/10.3390/ijerph19074212
Chicago/Turabian StyleHopfer, Suellen, Emilia J. Fields, Magdalen Ramirez, Sorina Neang Long, Heather C. Huszti, Adrijana Gombosev, Bernadette Boden-Albala, Dara H. Sorkin, and Dan M. Cooper. 2022. "Adolescent COVID-19 Vaccine Decision-Making among Parents in Southern California" International Journal of Environmental Research and Public Health 19, no. 7: 4212. https://doi.org/10.3390/ijerph19074212
APA StyleHopfer, S., Fields, E. J., Ramirez, M., Long, S. N., Huszti, H. C., Gombosev, A., Boden-Albala, B., Sorkin, D. H., & Cooper, D. M. (2022). Adolescent COVID-19 Vaccine Decision-Making among Parents in Southern California. International Journal of Environmental Research and Public Health, 19(7), 4212. https://doi.org/10.3390/ijerph19074212