
Mountain Hiking vs. Forest Therapy: A Study Protocol of Novel Types of Nature-Based Intervention


 , ,
, , 
Abstract
:1. Introduction
- (1)
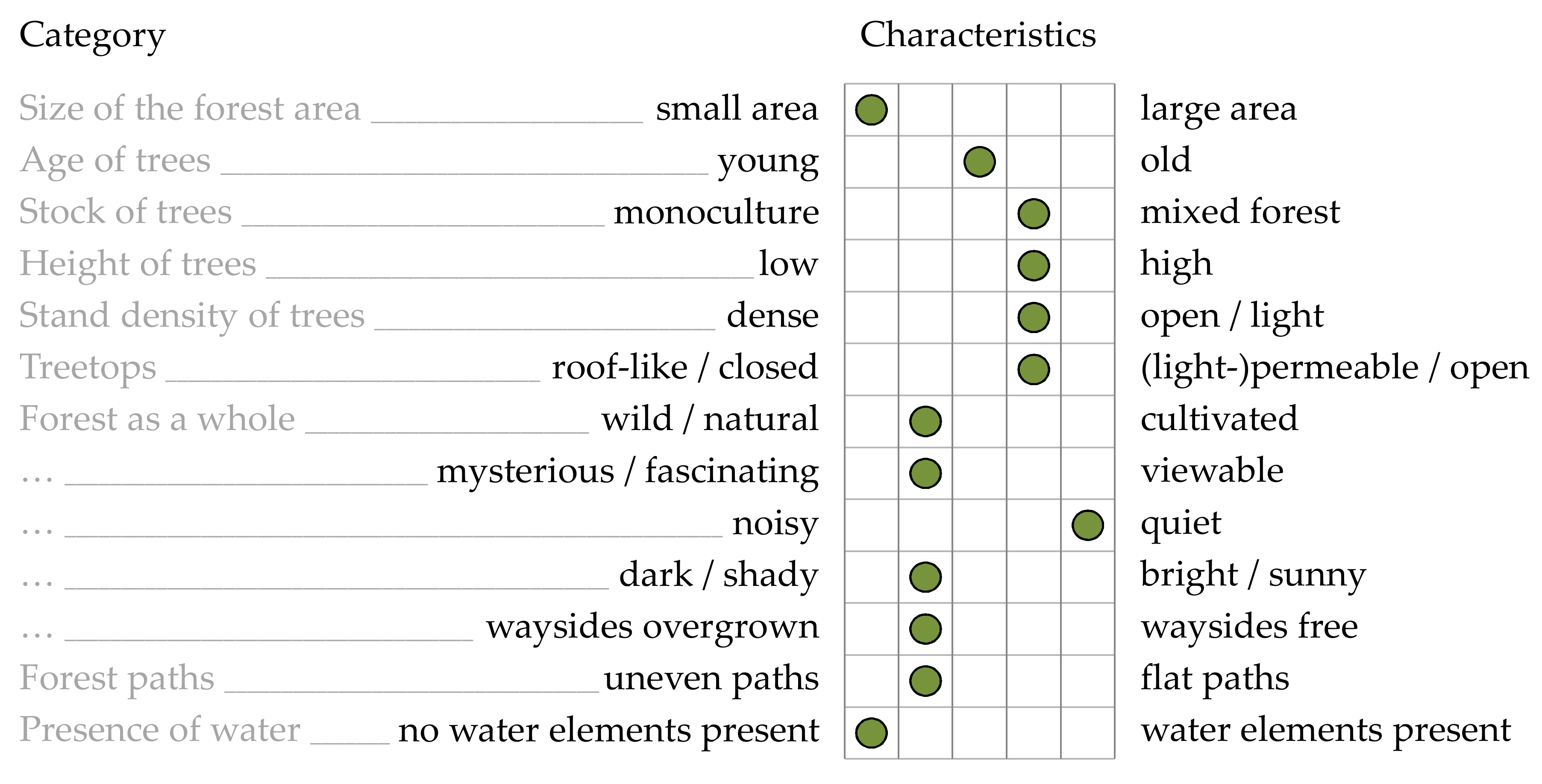
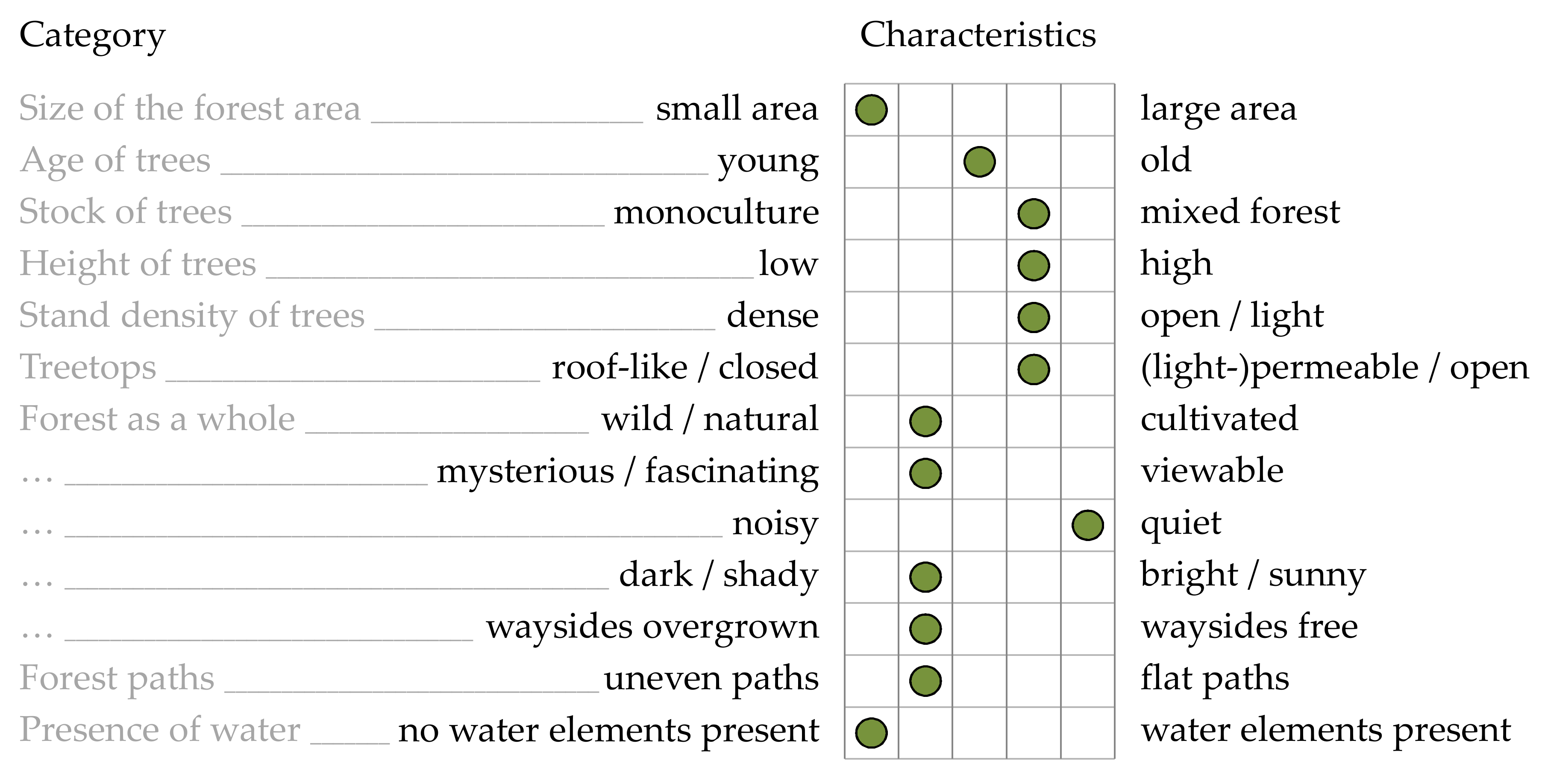
- Size of the forest area: Larger, more coherent forests increase well-being and can also be activity enhancing [28].
- (2)
- Age of trees: Older forests with large and mature trees increase well-being and positively contribute to recreational preferences [29].
- (3)
- Stock of trees: Mixed forests with deciduous and coniferous trees are perceived as more attractive than monocultures and thus increase well-being [30].
- (4)
- Height and structure of the trees: Higher trees increase well-being. In addition, different tree heights (levels of the treetops) are perceived as more attractive [27].
- (5)
- Stand density of the trees: Light forests with a rather low stand density of trees, and thus a higher incidence of light, increase well-being [10].
- (6)
- Characteristics of the treetops: A crown covering of about 75%, combined with sufficient light incidence, increases well-being [27].
- (7)
- Characteristics of the forest as a whole: Well-tended forests in the sense of managed forests (mood-lifting effect) [31] and a low proportion of dead wood, but at the same time, no excessive traces of lumbering [27], are preferred. In addition, the forests should be bright (orientation and safety), free of waste and noise [27].
- (8)
- Other vegetation: A varied, green-to-colorful vegetation (in addition to the trees), which is neither too dense nor too open, is generally preferred [14].
- (1)
- Characteristics of the forest paths: Flat, easily walkable paths, as well as free waysides and thus easy orientation (wide view), increase well-being, as well as the recreational value [32].
- (2)
- Characteristics of the forest floor: An area-wide vegetation, which is not overgrown and essentially walkable, increases well-being [32].
Objectives and Trial Design
2. Materials and Methods
2.1. Participants, Interventions and Outcomes
2.1.1. Study Design
2.1.2. Eligibility Criteria
2.1.3. Interventions
2.1.4. Outcomes
Primary Outcomes
Secondary Outcomes—Questionnaires
Secondary Outcomes—Physiological Parameter
Environmental Monitoring
2.1.5. Sample Size
2.1.6. Recruitment
2.2. Assignment of Interventions
2.3. Data Collection, Management, and Analysis
2.3.1. Data Collection Methods
2.3.2. Data Management
2.3.3. Statistical Methods
2.4. Monitoring
2.5. Ethics and Dissemination
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BFI-10 | 10 Item Big Five Inventory |
| Bf-SR | Mood Scale |
| BIA | Bio Impedance Analysis |
| B-L’ | Complaints List |
| BMI | Body Mass Index |
| CNS | Connectedness to Nature Scale |
| EQ-5D | Euro Quality of Life Questionnaire |
| FAS | Felt Arousal Scale |
| FEGK | Questionnaire for the Collection of Health-Related Control Beliefs |
| FS | Feeling Scale |
| FS-D | German Version of the Flourishing Scale |
| HRQOL | Health-Related Quality of Life |
| IPAQ-SF | International Physical Activity Questionnaire Short Form |
| iQOLC | Intercultural Quality of Life Comic |
| MAAS | Mindful Attention and Awareness Scale |
| nparLD | Nonparametric Longitudinal Data Analysis |
| NRS-6 | Nature Relatedness Scale 6 |
| PAR-Q | Physical Activity Readiness Questionnaire |
| PFB | Partnership Questionnaire |
| PFD | Partner Diagnostics Questionnaire |
| PHQ-9 | Patient Health Questionnaire |
| PL | Problem List |
| SF-12 | Short Form Health Survey |
| SWLS | Satisfaction with Life Scale |
| VAS | Visual Analog Scale |
Appendix A

{kind=link}
| Scheme 1. | Filled by: | |||||
| Date: | Weather: | |||||
| Location/forest: | Route: | |||||
| Duration: | Distance in km: | Altitude in m: | ||||
| Scale explanation | ||||||
 | ||||||
| Guidance* Characteristic X | 1 = is fully true | 2 = rather true | 3 = partially | 4 = rather true | 5 = is fully true | Guidance* Characteristic Y |
| Characteristics forest/trees | ||||||
| <200 hectares | Size of the forest area | >1000 hectares | ||||
| small area | 1 | 2 | 3 | 4 | 5 | large area |
| <10 years | Age of trees | >50 years | ||||
| young | 1 | 2 | 3 | 4 | 5 | old |
| Stock of trees | ||||||
| monoculture | 1 | 2 | 3 | 4 | 5 | Mixed forest |
| <5 meters | High and structure of the trees | >20 meters | ||||
| low | 1 | 2 | 3 | 4 | 5 | high |
| single stage | 1 | 2 | 3 | 4 | 5 | multistage |
| Stand density of the trees | ||||||
| dense | 1 | 2 | 3 | 4 | 5 | open/light |
| Structure of treetops | ||||||
| low-hanging | 1 | 2 | 3 | 4 | 5 | high |
| not sprawling | 1 | 2 | 3 | 4 | 5 | sprawling |
| roof-like/closed | 1 | 2 | 3 | 4 | 5 | (light-)perme-able/open |
| Forest as a whole | ||||||
| wild/natural | 1 | 2 | 3 | 4 | 5 | cultivated |
| mysterious/fascinating | 1 | 2 | 3 | 4 | 5 | viewable |
| relaxing | 1 | 2 | 3 | 4 | 5 | stimulating |
| cool | 1 | 2 | 3 | 4 | 5 | warm |
| dirty (garbage) | 1 | 2 | 3 | 4 | 5 | clean (garbage) |
| loud | 1 | 2 | 3 | 4 | 5 | quiet |
| lonely | 1 | 2 | 3 | 4 | 5 | full/socially connecting |
| unsafe | 1 | 2 | 3 | 4 | 5 | safe |
| dark/shady | 1 | 2 | 3 | 4 | 5 | bright/sunny |
| Other vegetation | ||||||
| monotonous | 1 | 2 | 3 | 4 | 5 | biodiverse |
| colorless | 1 | 2 | 3 | 4 | 5 | colorful |
| Survey form forest (2/2) | ||||||
| Scale explanation | ||||||
| | ||||||
| Characteristic X | 1 = is fully true | 2 = rather true | 3 = partially | 4 = rather true | 5 = is fully true | Characteristic Y |
| Characteristics forest paths/forest floor | ||||||
| Condition/structure forest paths | ||||||
| waysides overgrown | 1 | 2 | 3 | 4 | 5 | waysides free |
| slim | 1 | 2 | 3 | 4 | 5 | wide |
| twisty | 1 | 2 | 3 | 4 | 5 | straight |
| plain | 1 | 2 | 3 | 4 | 5 | steep |
| uneven | 1 | 2 | 3 | 4 | 5 | flat |
| hard | 1 | 2 | 3 | 4 | 5 | soft |
| designed | 1 | 2 | 3 | 4 | 5 | natural |
| Condition/structure forest floor | ||||||
| bare | 1 | 2 | 3 | 4 | 5 | overgrown |
| impassable | 1 | 2 | 3 | 4 | 5 | accessible |
| Other characteristics of the forest | ||||||
| no water elements *1 present | 1 | 2 | 3 | 4 | 5 | Water elements present |
| no views/sceneries present | 1 | 2 | 3 | 4 | 5 | views/sceneries present |
| no natural resting places *2 present | 1 | 2 | 3 | 4 | 5 | natural resting places present |
| not barrier-free | 1 | 2 | 3 | 4 | 5 | barrier-free |
References
- Wild, C.P. Complementing the Genome with an “Exposome”: The Outstanding Challenge of Environmental Exposure Measurement in Molecular Epidemiology. Cancer Epidemiol. Biomark. Prev. 2005, 14, 1847–1850. [Google Scholar]
- Wild, C.P. The Exposome: From Concept to Utility. Int. J. Epidemiol. 2012, 41, 24–32. [Google Scholar] [PubMed]
- Rappaport, S.M.; Smith, M.T. Environment and Disease Risks. Science 2010, 330, 460–461. [Google Scholar]
- Dagnino, S.; Macherone, A. (Eds.) Unraveling the Exposome: A Practical View; Springer Science + Business Media: New York, NY, USA, 2018; ISBN 978-3-319-89320-4. [Google Scholar]
- Rappaport, S.M. Implications of the Exposome for Exposure Science. J. Expo. Sci. Environ. Epidemiol. 2011, 21, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Frumkin, H.; Haines, A. Global Environmental Change and Noncommunicable Disease Risks. Annu. Rev. Public Health 2019, 40, 261–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gladwell, V.F.; Brown, D.K.; Wood, C.; Sandercock, G.R.; Barton, J.L. The Great Outdoors: How a Green Exercise Environment Can Benefit All. Extrem. Physiol. Med. 2013, 2, 3. [Google Scholar] [PubMed] [Green Version]
- Vrijheid, M. The Exposome: A New Paradigm to Study the Impact of Environment on Health. Thorax 2014, 69, 876–878. [Google Scholar]
- Oh, B.; Lee, K.J.; Zaslawski, C.; Yeung, A.; Rosenthal, D.; Larkey, L.; Back, M. Health and Well-Being Benefits of Spending Time in Forests: Systematic Review. Environ. Health Prev. Med. 2017, 22, 71. [Google Scholar]
- Schuh, A.; Immich, G. Waldtherapie—Das Potential des Waldes für Ihre Gesundheit; Springer Nature: Cham, Switzerland, 2019; ISBN 978-3-662-59025-6. [Google Scholar]
- Li, Q. Shinrin-Yoku: The Art and Science of Forest Bathing; Penguin Books: London, UK, 2018; ISBN 978-0-241-34695-2. [Google Scholar]
- Karjalainen, E.; Sarjala, T.; Raitio, H. Promoting Human Health through Forests: Overview and Major Challenges. Environ. Health Prev. Med. 2010, 15, 1. [Google Scholar]
- Shin, W.S.; Yeoun, P.S.; Yoo, R.W.; Shin, C.S. Forest Experience and Psychological Health Benefits: The State of the Art and Future Prospect in Korea. Environ. Health Prev. Med. 2010, 15, 38–47. [Google Scholar]
- Stigsdotter, U.K.; Corazon, S.S.; Sidenius, U.; Refshauge, A.D.; Grahn, P. Forest Design for Mental Health Promotion—Using Perceived Sensory Dimensions to Elicit Restorative Responses. Landsc. Urban Plan. 2017, 160, 1–15. [Google Scholar]
- Mao, G.-X.; Cao, Y.-B.; Lan, X.-G.; He, Z.-H.; Chen, Z.-M.; Wang, Y.-Z.; Hu, X.-L.; Lv, Y.-D.; Wang, G.-F.; Yan, J. Therapeutic Effect of Forest Bathing on Human Hypertension in the Elderly. J. Cardiol. 2012, 60, 495–502. [Google Scholar] [PubMed] [Green Version]
- Ikei, H.; Song, C.; Miyazaki, Y. Physiological Effect of Olfactory Stimulation by Hinoki Cypress (Chamaecyparis obtusa) Leaf Oil. J. Physiol. Anthropol. 2015, 34, 44. [Google Scholar] [PubMed] [Green Version]
- Mao, G.X.; Cao, Y.; Wang, B.; Wang, S.; Chen, Z.; Wang, J.; Xing, W.; Ren, X.; Lv, X.; Dong, J.; et al. The Salutary Influence of Forest Bathing on Elderly Patients with Chronic Heart Failure. Int. J. Environ. Res. Public Health 2017, 14, 368. [Google Scholar]
- Mao, G.X.; Cao, Y.B.; Yang, Y.; Chen, Z.M.; Dong, J.H.; Chen, S.S.; Wu, Q.; Lyu, X.L.; Jia, B.B.; Yan, J.; et al. Additive Benefits of Twice Forest Bathing Trips in Elderly Patients with Chronic Heart Failure. Biomed. Environ. Sci. BES 2018, 31, 159–162. [Google Scholar] [PubMed]
- Jia, B.B.; Yang, Z.X.; Mao, G.X.; Lyu, Y.D.; Wen, X.L.; Xu, W.H.; Lyu, X.L.; Cao, Y.B.; Wang, G.F. Health Effect of Forest Bathing Trip on Elderly Patients with Chronic Obstructive Pulmonary Disease. Biomed. Environ. Sci. BES 2016, 29, 212–218. [Google Scholar] [PubMed]
- Shin, W.S.; Shin, C.S.; Yeoun, P.S. The Influence of Forest Therapy Camp on Depression in Alcoholics. Environ. Health Prev. Med. 2012, 17, 73–76. [Google Scholar]
- Sonntag-Öström, E.; Nordin, M.; Dolling, A.; Lundell, Y.; Nilsson, L.; Slunga Järvholm, L. Can Rehabilitation in Boreal Forests Help Recovery from Exhaustion Disorder? The Randomised Clinical Trial ForRest. Scand. J. For. Res. 2015, 30, 732–748. [Google Scholar]
- Morita, E.; Imai, M.; Okawa, M.; Miyaura, T.; Miyazaki, S. A before and after Comparison of the Effects of Forest Walking on the Sleep of a Community-Based Sample of People with Sleep Complaints. Biopsychosoc. Med. 2011, 5, 13. [Google Scholar]
- Van den Berg, M.; van Poppel, M.; Smith, G.; Triguero-Mas, M.; Andrusaityte, S.; van Kamp, I.; van Mechelen, W.; Gidlow, C.; Gražulevičiene, R.; Nieuwenhuijsen, M.J.; et al. Does Time Spent on Visits to Green Space Mediate the Associations between the Level of Residential Greenness and Mental Health? Urban For. Urban Green. 2017, 25, 94–102. [Google Scholar]
- Stier-Jarmer, M.; Throner, V.; Kirschneck, M.; Immich, G.; Frisch, D.; Schuh, A. The Psychological and Physical Effects of Forests on Human Health: A Systematic Review of Systematic Reviews and Meta-Analyses. Int. J. Environ. Res. Public Health 2021, 18, 1770. [Google Scholar] [CrossRef] [PubMed]
- Hansen, M.M.; Jones, R.; Tocchini, K. Shinrin-Yoku (Forest Bathing) and Nature Therapy: A State-of-the-Art Review. Int. J. Environ. Res. Public Health 2017, 14, 851. [Google Scholar] [CrossRef] [Green Version]
- Wen, Y.; Yan, Q.; Pan, Y.; Gu, X.; Liu, Y. Medical Empirical Research on Forest Bathing (Shinrin-Yoku): A Systematic Review. Environ. Health Prev. Med. 2019, 24, 70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cervinka, R.; Höltge, J.; Pirgie, L.; Schwab, M.; Sudkamp, J.; Haluza, D.; Arnberger, A.; Eder, R.; Ebenberger, M. Zur Gesundheitswirkung von Waldlandschaften: Green Public Health—Benefits of Woodland on Human Health and Well-Being; BFW-Berichte; Bundesforschungszentrum für Wald: Wien, Austria, 2014; ISBN 978-3-7001-6098-4. [Google Scholar]
- Marušáková, Ľ.; Sallmannshofer, M. Human Health and Sustainable Forest Management; Forest Europe: Zvolen, Slovakia, 2019. [Google Scholar]
- Edwards, D.M.; Jay, M.; Jensen, F.S.; Lucas, B.; Marzano, M.; Montagné, C.; Peace, A.; Weiss, G. Public Preferences Across Europe for Different Forest Stand Types as Sites for Recreation. Ecol. Soc. 2012, 17, art27. [Google Scholar]
- Braun, A. Wahrnehmung von Wald und Natur; vs. Verlag für Sozialwissenschaften: Wiesbaden, Germany, 2000; ISBN 978-3-8100-2583-8. [Google Scholar]
- Martens, D.; Gutscher, H.; Bauer, N. Walking in “Wild” and “Tended” Urban Forests: The Impact on Psychological Well-Being. J. Environ. Psychol. 2011, 31, 36–44. [Google Scholar]
- Herzog, T.R.; Kirk, K.M. Pathway Curvature and Border Visibility as Predictors of Preference and Danger in Forest Settings. Environ. Behav. 2005, 37, 620–639. [Google Scholar]
- Kearney, A.R.; Bradley, G.A. The Effects of Viewer Attributes on Preference for Forest Scenes: Contributions of Attitudes, Knowledge, Demographic Factors, and Stakeholder Group Membership. Environ. Behav. 2011, 43, 147–181. [Google Scholar] [CrossRef]
- Nielsen, A.B.; Heyman, E.; Richnau, G. Liked, Disliked and Unseen Forest Attributes: Relation to Modes of Viewing and Cognitive Constructs. J. Environ. Manag. 2012, 113, 456–466. [Google Scholar]
- Appleton, J. The Experience of Landscape; Wiley: Chichester, NY, USA, 1996; ISBN 978-0-471-96233-5. [Google Scholar]
- Morris, J.; O’Brien, E.; Ambrose-Oji, B.; Lawrence, A.; Carter, C.; Peace, A. Access for All? Barriers to Accessing Woodlands and Forests in Britain. Local Environ. 2011, 16, 375–396. [Google Scholar] [CrossRef]
- Chan, A.-W.; Tetzlaff, J.M.; Altman, D.G.; Laupacis, A.; Gøtzsche, P.C.; Krleža-Jerić, K.; Hróbjartsson, A.; Mann, H.; Dickersin, K.; Berlin, J.A.; et al. SPIRIT 2013 Statement: Defining Standard Protocol Items for Clinical Trials. Ann. Intern. Med. 2013, 158, 200–207. [Google Scholar] [CrossRef] [Green Version]
- Berto, R. The Role of Nature in Coping with Psycho-Physiological Stress: A Literature Review on Restorativeness. Behav. Sci. 2014, 4, 394–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schutte, N.S.; Malouff, J.M. Mindfulness and Connectedness to Nature: A Meta-Analytic Investigation. Personal. Individ. Differ. 2018, 127, 10–14. [Google Scholar] [CrossRef]
- APA. Complementary and Integrative Treatments in Psychiatric Practice. Available online: https://www.appi.org/complementary_and_integrative_treatments_in_psychiatric_practice (accessed on 1 December 2020).
- Richardson, M.; Sheffield, D. Reflective Self-Attention: A More Stable Predictor of Connection to Nature Than Mindful Attention. Ecopsychology 2015, 7, 166–175. [Google Scholar]
- Wirtz, M.A.; Morfeld, M.; Glaesmer, H.; Brähler, E. Normierung Des SF-12 Version 2.0 Zur Messung Der Gesundheitsbezogenen Lebensqualität in Einer Deutschen Bevölkerungsrepräsentativen Stichprobe. Diagnostica 2018, 64, 215–226. [Google Scholar] [CrossRef]
- Ludwig, K.; Graf von der Schulenburg, J.-M.; Greiner, W. German Value Set for the EQ-5D-5L. PharmacoEconomics 2018, 36, 663–674. [Google Scholar] [CrossRef] [Green Version]
- Meuwly, N.; Schoebi, D.; Bierhoff, H.-W. TBS-TK Rezension: Fragebogen Zur Partnerschaftsdiagnostik (FPD; 2., Neu Normierte Und Erweiterte Auflage). Psychol. Rundsch. 2018, 69, 391–393. [Google Scholar] [CrossRef]
- Mayer, F.; Frantz, C. The Connectedness to Nature Scale: A Measure of Individuals’ Feeling in Community with Nature. J. Environ. Psychol. 2004, 24, 503–515. [Google Scholar] [CrossRef] [Green Version]
- Nisbet, E.K.; Zelenski, J.M. The NR-6: A New Brief Measure of Nature Relatedness. Front. Psychol. 2013, 4, 813. [Google Scholar] [CrossRef] [Green Version]
- Esch, T.; Jose, G.; Gimpel, C.; Scheidt, C.; Michalsen, A. Die Flourishing Scale (FS) von Diener et al. Liegt Jetzt in Einer Autorisierten Deutschen Fassung (FS-D) Vor: Einsatz Bei Einer Mind-Body-Medizinischen Fragestellung. Forsch. Komplementärmedizin 2006 2013, 20, 267–275. [Google Scholar] [CrossRef]
- Glaesmer, H.; Grande, G.; Braehler, E.; Roth, M. The German Version of the Satisfaction with Life Scale (SWLS): Psychometric Properties, Validity, and Population-Based Norms. Eur. J. Psychol. Assess. 2011, 27, 127–132. [Google Scholar] [CrossRef]
- B-LR—Beschwerden-Liste. Revidierte Fassung—Hogrefe Verlag. Available online: https://www.testzentrale.de/shop/beschwerden-liste-revidierte-fassung.html (accessed on 11 November 2020).
- Michalak, J.; Heidenreich, T.; Ströhle, G.; Nachtigall, C. Die Deutsche Version Der Mindful Attention and Awareness Scale (MAAS) Psychometrische Befunde Zu Einem Achtsamkeitsfragebogen. Z. Für Klin. Psychol. Psychother. 2008, 37, 200–208. [Google Scholar] [CrossRef]
- Hardy, C.J.; Rejeski, W.J. Not What, but How One Feels: The Measurement of Affect during Exercise. J. Sport Exerc. Psychol. 1989, 11, 304–317. [Google Scholar] [CrossRef]
- Svebak, S.; Murgatroyd, S. Metamotivational Dominance: A Multimethod Validation of Reversal Theory Constructs. J. Pers. Soc. Psychol. 1985, 48, 107–116. [Google Scholar] [CrossRef]
- Von Zerssen, D.; Petermann, F. Die Befindlichkeits-Skala: Revidierte Fassung; Manual; Hogrefe Verlag: Göttingen, Germany, 2011. [Google Scholar]
- Rammstedt, B.; Kemper, C.J.; Klein, M.C.; Beierlein, C.; Kovaleva, A. A Short Scale for Assessing the Big Five Dimensions of Personality: 10 Item Big Five Inventory (BFI-10). Methods Data Anal. 2013, 7, 17. [Google Scholar] [CrossRef]
- Ferring, D. Forschungsbericht Zum “Fragebogen Zur Erfassung Gesundheitsbezogener Kontrollüberzeugungen” (FEGK); University of Luxembourg: Luxembourg, 2003. [Google Scholar] [CrossRef]
- Raschner, C.; Lembert, S.; Platzer, H.-P.; Patterson, C.; Hilden, T.; Lutz, M. S3-Check—evaluation and generation of normal values of a test for balance ability and postural stability. Sportverletz. Sportschaden Organ Ges. Orthop. Traumatol. Sportmed. 2008, 22, 100–105. [Google Scholar] [CrossRef]
- Lukaski, H.C.; Bolonchuk, W.W.; Hall, C.B.; Siders, W.A. Validation of Tetrapolar Bioelectrical Impedance Method to Assess Human Body Composition. J. Appl. Physiol. 1986, 60, 1327–1332. [Google Scholar] [CrossRef] [Green Version]
- American Thoracic Society; European Respiratory Society. ATS/ERS Recommendations for Standardized Procedures for the Online and Offline Measurement of Exhaled Lower Respiratory Nitric Oxide and Nasal Nitric Oxide, 2005. Am. J. Respir. Crit. Care Med. 2005, 171, 912–930. [Google Scholar] [CrossRef]
- WHO. WHO STEPS Surveillance Manual: The WHO STEPwise Approach to Chronic Disease Risk Factor Surveillance; World Health Organization: Geneva, Switzerland, 2005; ISBN 978-92-4-159383-0. [Google Scholar]
- Buckley, J.P.; Sim, J.; Eston, R.G.; Hession, R.; Fox, R. Reliability and Validity of Measures Taken during the Chester Step Test to Predict Aerobic Power and to Prescribe Aerobic Exercise. Br. J. Sports Med. 2004, 38, 197–205. [Google Scholar]
- Prossegger, J.; Huber, D.; Grafetstätter, C.; Pichler, C.; Weisböck-Erdheim, R.; Iglseder, B.; Wewerka, G.; Hartl, A. Effects of Moderate Mountain Hiking and Balneotherapy on Community-Dwelling Older People: A Randomized Controlled Trial. Exp. Gerontol. 2019, 122, 74–84. [Google Scholar]
- Kraus, D. Consolidated Data Analysis and Presentation Using an Open-Source Add-in for the Microsoft Excel® Spreadsheet Software. Med. Writ. 2014, 23, 25–28. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 Statement: Updated Guidelines for Reporting Parallel Group Randomised Trials. BMJ 2010, 11, 340. [Google Scholar] [CrossRef]
- Noguchi, K.; Gel, Y.R.; Brunner, E.; Konietschke, F. NparLD: An R Software Package for the Nonparametric Analysis of Longitudinal Data in Factorial Experiments. J. Stat. Softw. 2012, 50, 12. [Google Scholar] [CrossRef] [Green Version]
- Lunneborg, C.E. Bootstrap Applications for the Behavioral Sciences. Educ. Psychol. Meas. 1987, 47, 627–629. [Google Scholar] [CrossRef]
- Lochner, A. Naturzeit Wald Was er uns Schenkt, Wie Wir Ihn Prägen; Kosmos Verlag: Stuttgart, Germany, 2019; ISBN 978-3-440-50189-4. [Google Scholar]
- Li, Q. Effect of forest bathing (shinrin-yoku) on human health: A review of the literature. Sante Publique Vandoeuvre Nancy Fr. 2019, S1, 135–143. [Google Scholar] [CrossRef] [Green Version]
- Fiteni, F.; Westeel, V.; Pivot, X.; Borg, C.; Vernerey, D.; Bonnetain, F. Endpoints in Cancer Clinical Trials. J. Visc. Surg. 2014, 151, 17–22. [Google Scholar]
- Buiting, H.M.; Olthuis, G. Importance of Quality-of-Life Measurement Throughout the Disease Course. JAMA Netw. Open 2020, 3, e200388. [Google Scholar] [CrossRef] [Green Version]
- Mercieca-Bebber, R.; King, M.T.; Calvert, M.J.; Stockler, M.R.; Friedlander, M. The Importance of Patient-Reported Outcomes in Clinical Trials and Strategies for Future Optimization. Patient Relat. Outcome Meas. 2018, 9, 353–367. [Google Scholar] [CrossRef] [Green Version]
- Corazon, S.; Stigsdotter, U.; Claudi Jensen, A.G.; Nilsson, K. Development of the Nature-Based Therapy Concept for Patients with Stress-Related Illness at the Danish Healing Forest Garden Nacadia. J. Hortic 2010, 20, 33–51. [Google Scholar]
- Michalsen, A. Natur als Therapie und Prävention. Z. für Komplementärmedizin 2020, 12, 12–17. [Google Scholar] [CrossRef]
- De Bock, F.; Dietrich, M.; Rehfuess, E. Evidenzbasierte Prävention und Gesundheitsförderung. Memo. Bundeszentrale Gesundh. Aufklärung (BZgA) 2020, 1.0, 8–9. [Google Scholar] [CrossRef]
- Global Forest Resources Assessment 2020; FAO: Rome, Italy, 2020; ISBN 978-92-5-132974-0.
- Eurostat Anteil Der Waldfläche. Available online: https://ec.europa.eu/eurostat/databrowser/view/sdg_15_10/default/table?lang=de (accessed on 22 January 2021).
- Hoffmann, S. (Ed.) Angewandtes Gesundheitsmarketing; Springer Gabler: Wiesbaden, Germany, 2012; ISBN 978-3-8349-4034-6. [Google Scholar]
- Muntschick, V. Der Neue Resonanz-Tourismus: Herzlich Willkommen! Zukunftsinstitut: Frankfurt, Germany, 2019; ISBN 978-3-945647-62-2. [Google Scholar]
| Distance (km) | Altitude (m) | Duration (h) | |
|---|---|---|---|
| Day 1 | 12.6 | 334 | 04:07 |
| Day 2 | 7.5 | 298 | 03:03 |
| Day 3 | 10.0 | 639 | 04:01 |
| Day 5 | 9.8 | 569 | 03:38 |
| Day 6 | 5.9 | 680 | 02:37 |
| Theme | Content | Activities | |
|---|---|---|---|
| Day 1 | Mindfulness and relaxation | Importance of mindfulness and relaxation in personal and work life, explanation of how nature can be used to foster and induce mindfulness and psycho-physiological relaxation [38]; | Nature-based mindfulness practices, e.g., walking meditation |
| Day 2 | Connection to nature | Importance of health benefits of nature connection; “forest bathing” as a formal method to strengthen the bond between oneself and one’s natural environment [39]; | “Forest bathing” activities, e.g., mindfully breathing with a tree |
| Day 3 | Social connections | Importance of social relationships, methods to calm down the nervous system to improve the social engagement system, which allows for connecting with one another better [40]; | Interpersonal mindfulness exercises, e.g., natural artwork |
| Day 5 | Connection to self | Importance of self-awareness, different aspects of oneself as a critical factor for mental well-being [41], how to use nature as a tool to initiate self-reflective processes; | e.g., medicine walk, invitation to communicate with nature |
| Day 6 | Goal setting and next steps | Goal setting, behavioral change, self-regulation, transformation of the practices and exercises learned in this program into lasting habits | Nature-based mindfulness practices |
| STUDY PERIOD | ||||||||
|---|---|---|---|---|---|---|---|---|
| Enrollment | Allocation | Post-Allocation | ||||||
| TIMEPOINT | T-2 | T-1 | T0 Baseline | T1 Day 0 | T1.2 Day 2 | T2 Day 7 | T3 Day 60 | T4 Day 180 |
| ENROLLMENT | ||||||||
Eligibility screen—step 1
| x | |||||||
Eligibility screen—step 2
| x | |||||||
| Informed consent | x | |||||||
| Group allocation | x | |||||||
| INTERVENTIONS | ||||||||
| Mountain hiking |  | |||||||
| Forest Therapy | | |||||||
| ASSESSMENTS | ||||||||
Primary Outcomes
| x | x | x | x | ||||
Secondary Outcomes
| x | x | x | x | ||||
Secondary Outcomes
| x | x | x | |||||
| x | x | ||||||
Short-term effects
| x | |||||||
Control parameter
| | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pichler, C.; Freidl, J.; Bischof, M.; Kiem, M.; Weisböck-Erdheim, R.; Huber, D.; Squarra, G.; Murschetz, P.C.; Hartl, A. Mountain Hiking vs. Forest Therapy: A Study Protocol of Novel Types of Nature-Based Intervention. Int. J. Environ. Res. Public Health 2022, 19, 3888. https://doi.org/10.3390/ijerph19073888
Pichler C, Freidl J, Bischof M, Kiem M, Weisböck-Erdheim R, Huber D, Squarra G, Murschetz PC, Hartl A. Mountain Hiking vs. Forest Therapy: A Study Protocol of Novel Types of Nature-Based Intervention. International Journal of Environmental Research and Public Health. 2022; 19(7):3888. https://doi.org/10.3390/ijerph19073888
Chicago/Turabian StylePichler, Christina, Johanna Freidl, Michael Bischof, Martin Kiem, Renate Weisböck-Erdheim, Daniela Huber, Gabriella Squarra, Paul Clemens Murschetz, and Arnulf Hartl. 2022. "Mountain Hiking vs. Forest Therapy: A Study Protocol of Novel Types of Nature-Based Intervention" International Journal of Environmental Research and Public Health 19, no. 7: 3888. https://doi.org/10.3390/ijerph19073888
APA StylePichler, C., Freidl, J., Bischof, M., Kiem, M., Weisböck-Erdheim, R., Huber, D., Squarra, G., Murschetz, P. C., & Hartl, A. (2022). Mountain Hiking vs. Forest Therapy: A Study Protocol of Novel Types of Nature-Based Intervention. International Journal of Environmental Research and Public Health, 19(7), 3888. https://doi.org/10.3390/ijerph19073888