
The Understanding and Experiences of Living with Dementia in Chinese New Zealanders

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
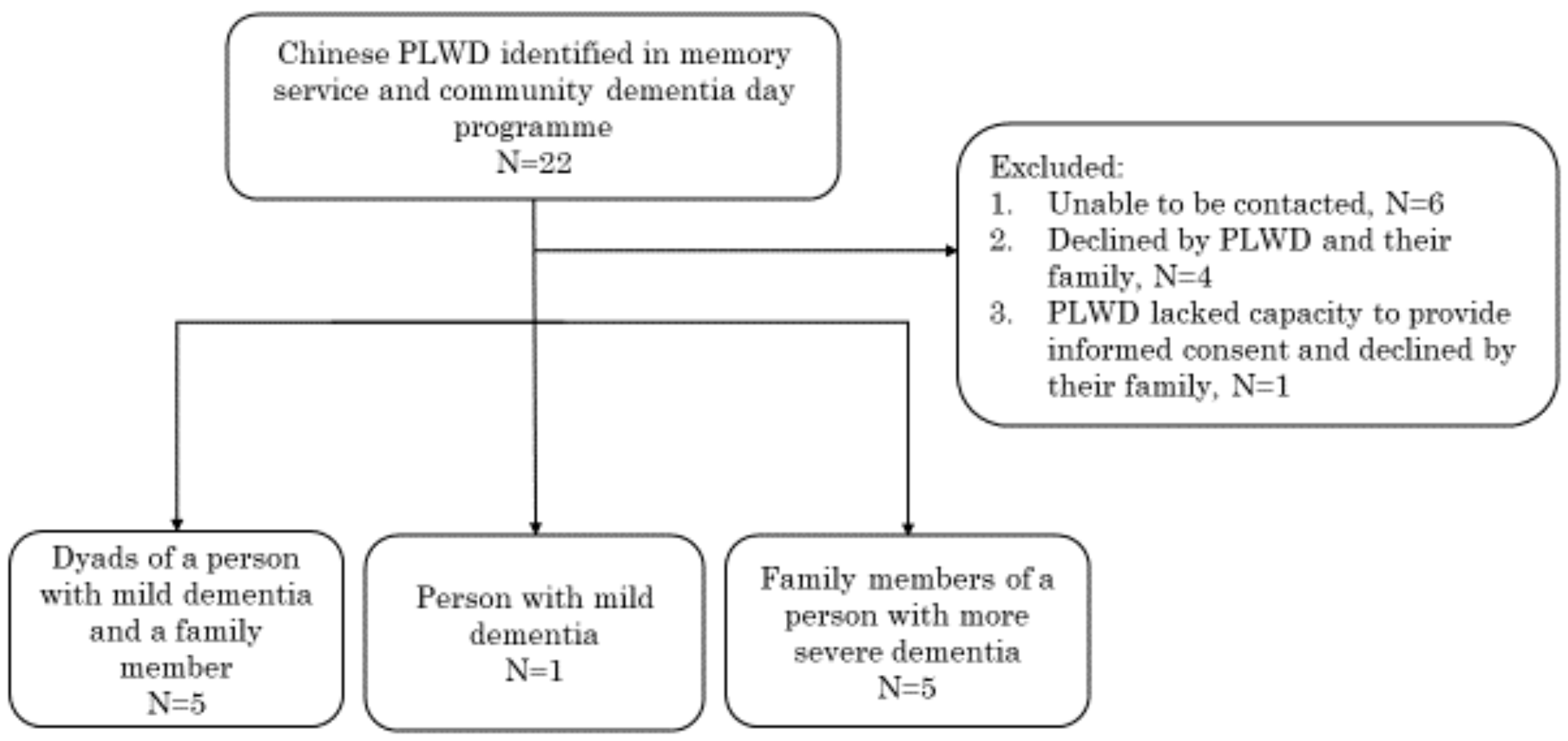
2.1. Participants and Setting
2.2. Semi-Structured Interviews
2.3. Data Analysis
Data Reporting
3. Results
3.1. Theme 1: Understandings of Dementia
3.1.1. Subtheme 1: Lack of Understanding of Dementia Prior to Diagnosis
Interviewer: Sorry John. So before your mother was diagnosed with Alzheimer’s dementia, did you have any like knowledge about dementia. What did you know about dementia?John: Nothing, I was very ignorant until later on.
3.1.2. Subtheme 2: The Concept of “Brain Shrinkage”
3.1.3. Subtheme 3: Dementia Is Part of Getting Older
3.2. Theme 2: Impact on the PLWD
3.2.1. Subtheme 1: Memory-Related Problems Are Common
3.2.2. Subtheme 2: Anhedonia, Apathy, Other Neuropsychiatric Symptoms and Functional Impairment
3.2.3. Subtheme 3: Different Ways of Coping
3.3. Theme 3: Impact on Family Carers
3.3.1. Subtheme 1: Cultural Obligation
3.3.2. Subtheme 2: Carer Stress and Coping
3.3.3. Subtheme 3: Importance of Hope
3.4. Theme 4: Stigma
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Semi-Structured Interview Topic Guide
| ”What do we mean by dementia?“ Different communities have different understandings of dementia, some see dementia as a disease, others see it as a natural part of normal ageing” Tell me what you know about dementia and memory changes as people get older? What are the Tongan/Chinese/Indian terms use to talk about dementia? What is your understanding of dementia? What do those words mean? Why do you think older people get dementia? How are dementia and normal ageing related? What are the signs that someone has dementia? What do you think causes dementia? “Could you tell me more about that?” | Getting the diagnosis Could you tell us how it has been for you? What did you first notice? Could you describe the changes What was your explanation Who diagnosed you? (GP/hospital doc/other?) Can you remember what happened Did they tell you the results of your blood tests/memory tests/scan? How did you feel when they told you the diagnosis? How were the staff towards you (sympathetic? value your opinion? respectful?) What kind of information did they offer on what to do next (or about services)? What were the most significant moments in the process (what do you remember most clearly)? “Could you tell me more about that?” |
| After the diagnosis How are things now? What changes have you made to cope? What help do you need? How do your family/community help you? * Has it changed your role in the family/community? * What are the positive things that have happened? How do other people outside the family act towards you? Do you tell other people about the diagnosis? (if not, why not?) “Could you tell me more about that?” * think about risks eg cooking, driving, being home alone; but also positive changes e.g.) more family time, increased understanding of their experience, less arguments with family as they understand the disorder | Services What kind of help do you get? e.g., GP, nurse, home/day care? What kind of things help/don’t help? What do you need but don’t get? Do you use “day centres”? (which one) How often do you go? What do you think about those services? What do you like/didn’t like? Is it specifically for people from …… (Tonga, Samoa, India, China) How do you think things might change in the future? What do you think you might need in the future? “Could you tell me more about that?” If you weren’t living in New Zealand how do you think your life would be different? (if you were still living in …..) |
| Questions for people with dementia Is there anything you want to add? What are your main concerns now? What is most difficult for you? What is most positive? In our culture we are often expected to look after our elders—how is that for you Have you planned for the future? “Could you tell me more about that?” Is there anything that we have missed? “Could you tell me more about that?” | Questions for carers Is there anything you want to add? How many hours on average are you a care partner for [Name] at your home? Describe what caring you provide. How does your caring routine impact your daily life? Do you talk with others about your role as a care partner? How do you do this? Does anyone else provide care for [Name]? What is your reason for taking on the role of care partner? What are your main concerns around caring for your relative with dementia? What is most difficult for you? What is most positive? In our culture we are often expected to look after our elders—how is that for you Have you planned for the future? “Could you tell me more about that?” Is there anything that we have missed? “ Could you tell me more about that?” |
References
- Wortmann, M. Dementia: A global health priority—Highlights from an ADI and World Health Organization report. Alzheimers Res. Ther. 2012, 4, 1–3. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Dementia. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 17 December 2021).
- Statistics New Zealand. 2018 Census Population and Dwelling Counts. Available online: https://www.stats.govt.nz/information-releases/2018-census-population-and-dwelling-counts (accessed on 17 November 2021).
- Ministry of Social Development. Our Ageing Population; Ministry of Social Development: Wellington, New Zealand, 2016. [Google Scholar]
- Deloitte Access Economics. Updated Dementia Economic Impact Report 2016. Available online: https://alzheimers.org.nz/explore/research/ (accessed on 17 November 2021).
- Smith, E.; Lamb-Yorski, R.; Thompson, A.; Grootveld, C. This Is Our Story: A Qualitative Research Report on Living with Dementia; Litmus: Wellington, New Zealand, 2019. [Google Scholar]
- Dudley, M.; Menzies, O.; Elder, H.; Nathan, L.; Garrett, N.; Wilson, D. Mate wareware: Understanding ‘dementia’ from a Māori perspective. N. Z. Med. J. 2019, 132, 66–74. [Google Scholar]
- Fakahau, T.; Faeamani, G.; Maka, M. Pacific People and Dementia; Tongan Advisory Council: Auckland, New Zealand, 2019. [Google Scholar]
- Cheung, G.; Appleton, K.; Boyd, M.; Cullum, S. Perspectives of dementia from Asian communities living in New Zealand: A focus group of Asian health care professionals. Int. J. Geriatr. Psychiatry 2019, 34, 1758–1764. [Google Scholar] [CrossRef]
- Fairburn, M. What best explains the discrimination against the Chinese in New Zealand, 1860s–1950s? J. N. Z. Stud. 2004, 2/3, 65–85. [Google Scholar] [CrossRef]
- QSR International Pty Ltd. NVivo Version 12; QSR International (Americas) Inc.: Burlington, MA, USA, 2018. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Mok, E.; Lai, C.K.; Wong, F.L.; Wan, P. Living with early-stage dementia: The perspective of older Chinese people. J. Adv. Nurs. 2007, 59, 591–600. [Google Scholar] [CrossRef]
- Chiu, H.F.; Sato, M.; Kua, E.H.; Lee, M.S.; Yu, X.; Ouyang, W.C.; Yang, Y.K.; Sartorius, N. Renaming dementia—An East Asian perspective. Int. Psychogeriatr. 2014, 26, 885–887. [Google Scholar] [CrossRef] [Green Version]
- Liu, D.; Cheng, G.; An, L.; Gan, X.; Wu, Y.; Zhang, B.; Hu, S.; Zeng, Y.; Wu, L. Public knowledge about dementia in China: A national WeChat-Based survey. Int. J. Environ. Res. Public Health 2019, 16, 4231. [Google Scholar] [CrossRef] [Green Version]
- Calia, C.; Johnson, H.; Cristea, M. Cross-cultural representations of dementia: An exploratory study. J. Glob. Health 2019, 9, 011001. [Google Scholar] [CrossRef]
- Livingston, G.; Sommerlad, A.; Orgeta, V.; Costafreda, S.G.; Huntley, J.; Ames, D.; Ballard, C.; Banerjee, S.; Burns, A.; Cohen-Mansfield, J.; et al. Dementia prevention, intervention, and care. Lancet 2017, 390, 2673–2734. [Google Scholar] [CrossRef] [Green Version]
- Woods, B.; Aguirre, E.; Spector, A.E.; Orrell, M. Cognitive stimulation to improve cognitive functioning in people with dementia. Cochrane Database Syst. Rev. 2012, 2, CD005562. [Google Scholar] [CrossRef]
- Wong, G.H.Y.; Yek, O.P.L.; Zhang, A.Y.; Lum, T.Y.S.; Spector, A. Cultural adaptation of cognitive stimulation therapy (CST) for Chinese people with dementia: Multicentre pilot study. Int. J. Geriatr. Psychiatry 2018, 33, 841–848. [Google Scholar] [CrossRef]
- Spector, A.; Thorgrimsen, L.; Woods, B.; Orrell, M. Making a Difference: An Evidence-Based Group Programme to Offer Cognitive Stimulation Therapy (CST) to People with Dementia; Hawker Publications: London, UK, 2006. [Google Scholar]
- Boughtwood, D.L.; Adams, J.; Shanley, C.; Santalucia, Y.; Kyriazopoulos, H. Experiences and perceptions of culturally and linguistically diverse family carers of people with dementia. Am. J. Alzheimers Dis. 2011, 26, 290–297. [Google Scholar] [CrossRef]
- Chang, Y.-P.; Schneider, J.K.; Sessanna, L. Decisional conflict among Chinese family caregivers regarding nursing home placement of older adults with dementia. J. Aging Stud. 2011, 25, 436–444. [Google Scholar] [CrossRef]
- Chiu, T.; Marziali, E.; Colantonio, A.; Carswell, A.; Gruneir, M.; Tang, M.; Eysenbach, G. Internet-based caregiver support for Chinese Canadians taking care of a family member with Alzheimer disease and related dementia. Can. J. Aging 2009, 28, 323–336. [Google Scholar] [CrossRef] [Green Version]
- Ho, B.; Friedland, J.; Rappolt, S.; Noh, S. Caregiving for relatives with Alzheimer’s disease: Feelings of Chinese-Canadian women. J. Aging Stud. 2003, 17, 301–321. [Google Scholar] [CrossRef]
- Koo, M.Y.; Pusey, H.; Keady, J. ‘I try my best … I try to relieve the burden of my mum’: A narrative analysis of the everyday care-giving experiences for five intergenerational Singapore-Chinese families where one member has dementia. Ageing Soc. 2020, 41, 1897–1919. [Google Scholar] [CrossRef] [Green Version]
- Low, L.F.; Anstey, K.J.; Lackersteen, S.M.; Camit, M. Help-seeking and service use for dementia in Italian, Greek and Chinese Australians. Aging Ment. Health 2011, 15, 397–404. [Google Scholar] [CrossRef]
- Hinton, L.; Guo, Z.; Hillygus, J.; Levkoff, S. Working with culture: A qualitative analysis of barriers to the recruitment of Chinese-American family caregivers for dementia research. J. Cross. Cult. Gerontol 2000, 15, 119–137. [Google Scholar] [CrossRef]
- Liu, D.; Hinton, L.; Tran, C.; Hinton, D.; Barker, J.C. Reexamining the relationships among dementia, stigma, and aging in immigrant Chinese and Vietnamese family caregivers. J. Cross. Cult. Gerontol. 2008, 23, 283–299. [Google Scholar] [CrossRef] [Green Version]
- Au, A.; Li, S.; Lee, K.; Leung, P.; Pan, P.C.; Thompson, L.; Gallagher-Thompson, D. The Coping with Caregiving Group Program for Chinese caregivers of patients with Alzheimer’s disease in Hong Kong. Patient Educ. Couns. 2010, 78, 256–260. [Google Scholar] [CrossRef]
- Kwok, T.; Wong, B.; Ip, I.; Chui, K.; Young, D.; Ho, F. Telephone-delivered psychoeducational intervention for Hong Kong Chinese dementia caregivers: A single-blinded randomized controlled trial. Clin. Interv. Aging 2013, 8, 1191–1197. [Google Scholar] [CrossRef] [Green Version]
- Braun, K.L.; Browne, C.V. Perceptions of dementia, caregiving, and help seeking among Asian and Pacific Islander Americans. Health Soc. Work 1998, 23, 262–274. [Google Scholar] [CrossRef]
- Jones, R.S.; Chow, T.W.; Gatz, M. Asian Americans and Alzheimer’s disease: Assimilation, culture, and beliefs. J. Aging Stud. 2006, 20, 11–25. [Google Scholar] [CrossRef]
- Yeo, G.; Gerdner, L.A.; Gallagher-Thompson, D. Ethnicity and the Dementias, 3rd ed.; Routledge: New York, NY, USA, 2019. [Google Scholar]
- Tan, L.L.; Wong, H.B.; Allen, H. The impact of neuropsychiatric symptoms of dementia on distress in family and professional caregivers in Singapore. Int. Psychogeriatr. 2005, 17, 253–263. [Google Scholar] [CrossRef]


{kind=link}
| Pseudonym of Person with Dementia | Pseudonym of Family Carer (Relationship) | Age | Gender | Marital Status | Birthplace | Years Living in New Zealand | Language | |
|---|---|---|---|---|---|---|---|---|
| Person with dementia | Wei | -- | 61 | M | Married | Hong Kong | 41 | Cantonese |
| Dyad 1 | Ming | -- | 87 | M | Married | China | 25 | Mandarin |
| -- | Fang (wife) | 83 | F | Married | China | 25 | Mandarin | |
| Dyad 2 | Li | -- | 84 | F | Married | China | 20 | Mandarin |
| Jing (husband) | 89 | M | Married | China | 20 | Mandarin | ||
| Dyad 3 | Yong | -- | 79 | M | Married | China | 19 | Mandarin |
| -- | Yan (wife) | 78 | F | Married | China | 19 | Mandarin | |
| Dyad 4 | Na | -- | 75 | F | Married | China | 17 | Mandarin |
| -- | Sam (son) | 53 | M | Married | China | 22 | Mandarin | |
| Dyad 5 | Fen | -- | 88 | F | Widowed | China | 81 | English |
| -- | Joe (son) | 60 | M | Married | New Zealand | 60 | English | |
| Carer 1 | -- | Ying (wife) | 67 | F | married | China | 11 | Mandarin |
| Carer 2 | -- | Lan (wife) | 64 | F | Married | Cambodia | 20 | Cantonese |
| Carer 3 | -- | John (son) | 48 | M | Married | Hong Kong | 28 | Cantonese |
| Carer 4 | -- | Jo (daughter) | 49 | F | Married | China | 20 | Mandarin |
| Carer 5 | -- | Sandy (daughter) | 55 | F | De facto | China | 25 | Mandarin |
| Main Themes | Subthemes | Potential Interventions |
|---|---|---|
| 1. Understandings of dementia | (i) Lack of understanding of dementia prior to diagnosis (ii) The concept of “brain shrinkage” (iii) Dementia is part of getting older | Public awareness and psychoeducation on dementia and healthy ageing in Chinese community |
| 2. Impact on the person living with dementia | (i) Memory-related problems are common (ii) Anhedonia, apathy, other neuropsychiatric symptoms and functional impairment (iii) Different ways of coping | Living well with dementia and person-centred evidence-based interventions e.g., Cognitive Stimulation Therapy |
| 3. Impact on family carers | (i) Cultural obligation (ii) Carer stress and coping (iii) Importance of hope | Chinese carer psychoeducation and support groups |
| 4. Stigma | - | Public awareness and stigmatisation campaign psychoeducation in the Chinese community |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheung, G.; Su, A.Y.; Wu, K.; Yue, B.; Yates, S.; Martinez Ruiz, A.; Krishnamurthi, R.; Cullum, S. The Understanding and Experiences of Living with Dementia in Chinese New Zealanders. Int. J. Environ. Res. Public Health 2022, 19, 1280. https://doi.org/10.3390/ijerph19031280
Cheung G, Su AY, Wu K, Yue B, Yates S, Martinez Ruiz A, Krishnamurthi R, Cullum S. The Understanding and Experiences of Living with Dementia in Chinese New Zealanders. International Journal of Environmental Research and Public Health. 2022; 19(3):1280. https://doi.org/10.3390/ijerph19031280
Chicago/Turabian StyleCheung, Gary, April Yuehan Su, Karen Wu, Blake Yue, Susan Yates, Adrian Martinez Ruiz, Rita Krishnamurthi, and Sarah Cullum. 2022. "The Understanding and Experiences of Living with Dementia in Chinese New Zealanders" International Journal of Environmental Research and Public Health 19, no. 3: 1280. https://doi.org/10.3390/ijerph19031280
APA StyleCheung, G., Su, A. Y., Wu, K., Yue, B., Yates, S., Martinez Ruiz, A., Krishnamurthi, R., & Cullum, S. (2022). The Understanding and Experiences of Living with Dementia in Chinese New Zealanders. International Journal of Environmental Research and Public Health, 19(3), 1280. https://doi.org/10.3390/ijerph19031280