

Effect of a Cognitive Function and Social Skills-Based Digital Exercise Therapy Using IoT on Motor Coordination in Children with Intellectual and Developmental Disability


Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
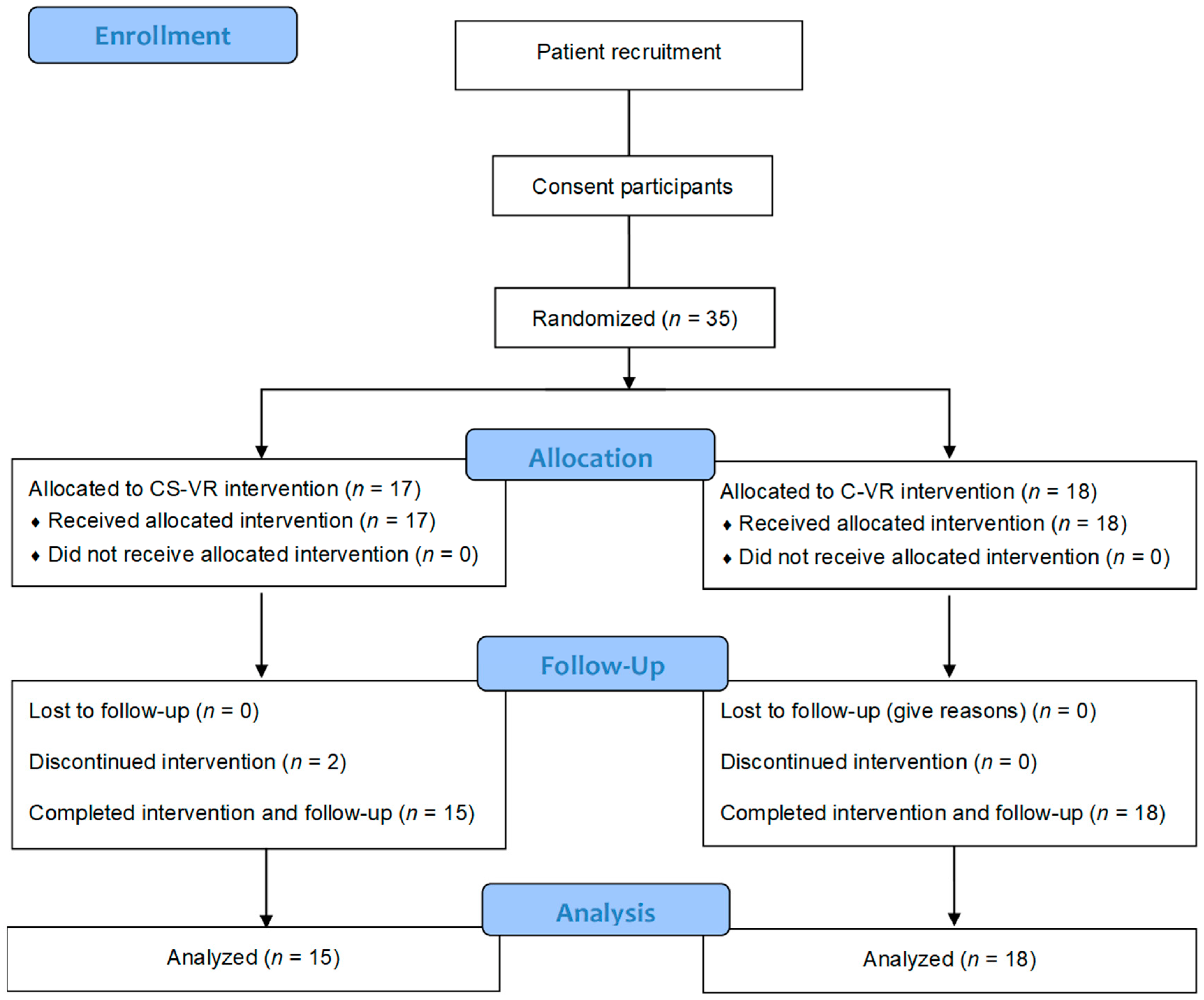
2.2. Study Design
2.3. Motor Coordination and Exercise Performance Test
2.3.1. Extended Horizontal Jump
2.3.2. Hop
2.3.3. Stationary Drills
2.3.4. Overarm Throw
2.3.5. Standing Long Jump
2.3.6. YMCA Step Test
2.4. Cognitive Function Test
2.5. Social Skills Test
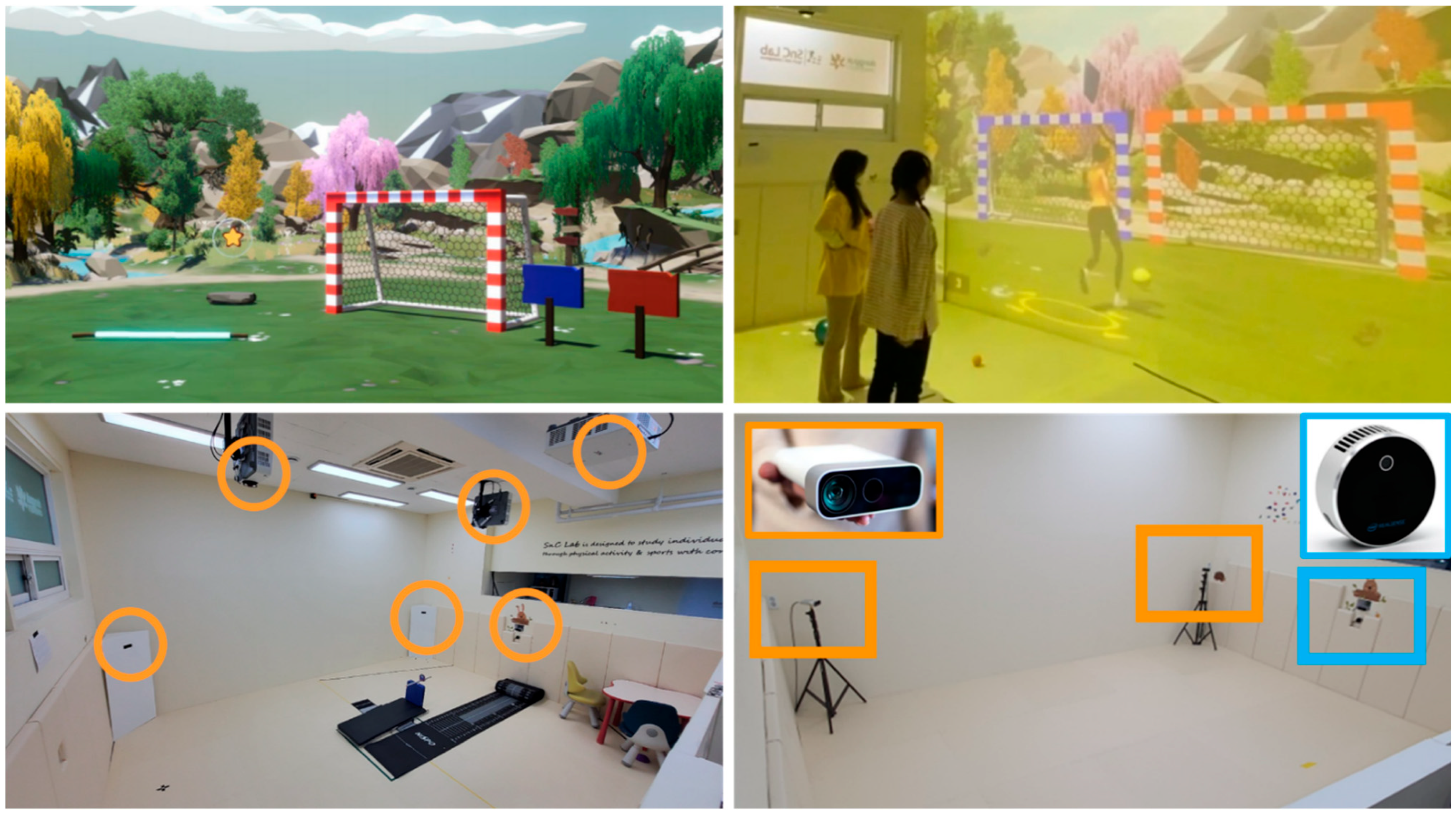
2.6. VR Room Setup
2.7. VR Exercise Program
2.8. Statistical Analysis
3. Results
3.1. Participants’ Demographics
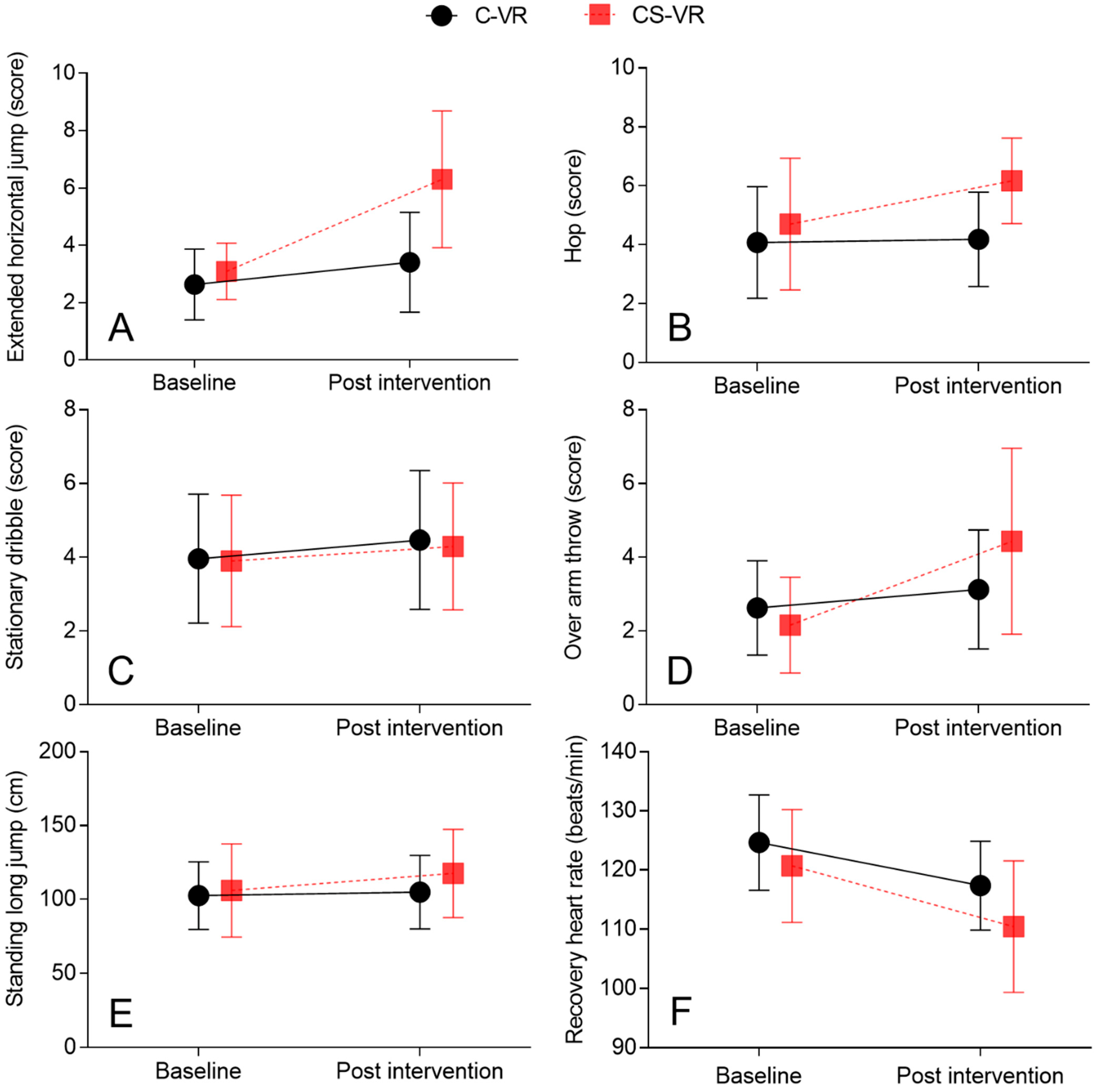
3.2. Extended Horizontal Jump
3.3. Hop
3.4. Stationary Dribble
3.5. Overarm Throw
3.6. Standing Long Jump
3.7. Recovery Heart Rate (RHR)
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zablotsky, B.; Black, L.I.; Maenner, M.J.; Schieve, L.A.; Danielson, M.L.; Bitsko, R.H.; Blumberg, S.J.; Kogan, M.D.; Boyle, C.A. Prevalence and Trends of Developmental Disabilities among Children in the United States: 2009–2017. Pediatrics 2019, 144, e20190811. [Google Scholar] [CrossRef] [PubMed]
- Edition, F. Diagnostic and statistical manual of mental disorders. Am. Psychiatr. Assoc. 2013, 21, 591–643. [Google Scholar]
- Lotan, M.; Yalon-Chamovitz, S.; Weiss, P.L. Improving physical fitness of individuals with intellectual and developmental disability through a Virtual Reality Intervention Program. Res. Dev. Disabil. 2009, 30, 229–239. [Google Scholar] [CrossRef] [PubMed]
- St John, L.; Borschneck, G.; Cairney, J. A Systematic Review and Meta-Analysis Examining the Effect of Exercise on Individuals with Intellectual Disability. Am. J. Intellect. Dev. Disabil. 2020, 125, 274–286. [Google Scholar] [CrossRef]
- Beckung, E.; Steffenburg, U.; Uvebrant, P. Motor and sensory dysfunctions in children with mental retardation and epilepsy. Seizure 1997, 6, 43–50. [Google Scholar] [CrossRef]
- Golubović, Š.; Maksimović, J.; Golubović, B.; Glumbić, N. Effects of exercise on physical fitness in children with intellectual disability. Res. Dev. Disabil. 2012, 33, 608–614. [Google Scholar] [CrossRef]
- Kapsal, N.J.; Dicke, T.; Morin, A.J.S.; Vasconcellos, D.; Maïano, C.; Lee, J.; Lonsdale, C. Effects of Physical Activity on the Physical and Psychosocial Health of Youth With Intellectual Disabilities: A Systematic Review and Meta-Analysis. J. Phys. Act. Health 2019, 16, 1187–1195. [Google Scholar] [CrossRef]
- Hartman, E.; Smith, J.; Westendorp, M.; Visscher, C. Development of physical fitness in children with intellectual disabilities. J. Intellect. Disabil. Res. 2015, 59, 439–449. [Google Scholar] [CrossRef]
- Lotan, M. Quality physical intervention activity for persons with Down syndrome. Sci. World J. 2007, 7, 7–19. [Google Scholar] [CrossRef]
- Kang, T.-C.; Wen, C.-H.; Guo, S.-W.; Chang, W.-Y.; Chang, C.-L. The implementation of an IoT-based exercise improvement system. J. Supercomput. 2020, 76, 6361–6375. [Google Scholar] [CrossRef]
- Lee, I.; Lee, K. The Internet of Things (IoT): Applications, investments, and challenges for enterprises. Bus. Horiz. 2015, 58, 431–440. [Google Scholar] [CrossRef]
- McMahon, D.D.; Barrio, B.; McMahon, A.K.; Tutt, K.; Firestone, J. Virtual Reality Exercise Games for High School Students With Intellectual and Developmental Disabilities. J. Spec. Educ. Technol. 2020, 35, 87–96. [Google Scholar] [CrossRef]
- Standen, P.J.; Brown, D.J. Virtual reality in the rehabilitation of people with intellectual disabilities: Review. Cyberpsychol. Behav. 2005, 8, 272–282. [Google Scholar] [CrossRef]
- Sorensen, C.; Zarrett, N. Benefits of Physical Activity for Adolescents with Autism Spectrum Disorders: A Comprehensive Review. Rev. J. Autism Dev. Disord. 2014, 1, 344–353. [Google Scholar] [CrossRef]
- Memari, A.H.; Mirfazeli, F.S.; Kordi, R.; Shayestehfar, M.; Moshayedi, P.; Mansournia, M.A. Cognitive and social functioning are connected to physical activity behavior in children with autism spectrum disorder. Res. Autism Spectr. Disord. 2017, 33, 21–28. [Google Scholar] [CrossRef]
- Breslin, C.M.; Rudisill, M.E. The effect of visual supports on performance of the TGMD-2 for children with autism spectrum disorder. Adapt. Phys. Act. Q. 2011, 28, 342–353. [Google Scholar] [CrossRef]
- Simons, J.; Daly, D.; Theodorou, F.; Caron, C.; Simons, J.; Andoniadou, E. Validity and reliability of the TGMD-2 in 7-10-year-old Flemish children with intellectual disability. Adapt. Phys. Activ. Q. 2008, 25, 71–82. [Google Scholar] [CrossRef]
- Wilson, R.B.; McCracken, J.T.; Rinehart, N.J.; Jeste, S.S. What’s missing in autism spectrum disorder motor assessments? J. Neurodev. Disord. 2018, 10, 33. [Google Scholar] [CrossRef]
- Wuang, Y.P.; Su, C.Y.; Huang, M.H. Psychometric comparisons of three measures for assessing motor functions in preschoolers with intellectual disabilities. J. Intellect. Disabil. Res. 2012, 56, 567–578. [Google Scholar] [CrossRef] [PubMed]
- Chol, J.-Y.; Kim, J.-S. The Effect of Inline Skate Program on Physical Fitness (PAPS-D) Improvement of Student with Developmental Disability. J. Korean Appl. Sci. Technol. 2019, 36, 541–550. [Google Scholar]
- Rey, E.; Carballo-Fazanes, A.; Varela-Casal, C.; Abelairas-Gómez, C. Reliability of the test of gross motor development: A systematic review. PLoS ONE 2020, 15, e0236070. [Google Scholar] [CrossRef]
- Kim, S.; Kim, M.J.; Valentini, N.C.; Clark, J.E. Validity and reliability of the TGMD-2 for South Korean children. J. Mot. Behav. 2014, 46, 351–356. [Google Scholar] [CrossRef]
- Manual, G. YMCA Fitness Testing and Assessment, 4th ed.; Published for the YMCA of the USA; Human Kinetics: Champaign, IL, USA, 2000; Available online: https://www.worldcat.org/title/ymcafitness-testing-and-assessment-manual/oclc/43798539 (accessed on 9 November 2022).
- Ju, Y.-M.; Chung, J.-W.; Kim, J.-H.; Jung, S.-W.; Cho, S.-Y. Development and Pilot Validation of Tablet-Based Social Assessment for Children With Developmental Disabilities. J. Korean Soc. Occup. Ther. 2021, 29, 127–142. [Google Scholar] [CrossRef]
- Hillman, C.H.; Pontifex, M.B.; Raine, L.B.; Castelli, D.M.; Hall, E.E.; Kramer, A.F. The effect of acute treadmill walking on cognitive control and academic achievement in preadolescent children. Neuroscience 2009, 159, 1044–1054. [Google Scholar] [CrossRef]
- Hiruntrakul, A.; Nanagara, R.; Emasithi, A.; Borer, K.T. Effect of once a week endurance exercise on fitness status in sedentary subjects. J. Med. Assoc. Thail. 2010, 93, 1070–1074. [Google Scholar]
- Richardson, J.T. Eta squared and partial eta squared as measures of effect size in educational research. Educ. Res. Rev. 2011, 6, 135–147. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: London, UK, 2013. [Google Scholar]
- Haff, G.G.; Triplett, N.T. Essentials of Strength Training and Conditioning, 4th ed.; Human kinetics: Champaign, IL, USA, 2015. [Google Scholar]
- Liu, T.; Hamilton, M.; Davis, L.; ElGarhy, S. Gross motor performance by children with autism spectrum disorder and typically developing children on TGMD-2. J. Child Adolesc. Behav. 2014, 2, 123. [Google Scholar] [CrossRef]
- Quinzi, F.; Camomilla, V.; Bratta, C.; Piacentini, M.F.; Sbriccoli, P.; Vannozzi, G. Hopping skill in individuals with Down syndrome: A qualitative and quantitative assessment. Hum. Mov. Sci. 2021, 78, 102821. [Google Scholar] [CrossRef] [PubMed]
- Bishop, J.C.; Pangelinan, M. Motor skills intervention research of children with disabilities. Res. Dev. Disabil. 2018, 74, 14–30. [Google Scholar] [CrossRef] [PubMed]
- Erickson, B.J.; Thorsness, R.J.; Hamamoto, J.T.; Verma, N.N. The Biomechanics of Throwing. Oper. Tech. Sport. Med. 2016, 24, 156–161. [Google Scholar] [CrossRef]
- Ashkenazi, T.; Weiss, P.L.; Orian, D.; Laufer, Y. Low-cost virtual reality intervention program for children with developmental coordination disorder: A pilot feasibility study. Pediatr. Phys. Ther. 2013, 25, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Raygoza-Romero, J.; Gonzalez-Hernandez, A.; Bermudez, K.; Martinez-Garcia, A.I.; Caro, K. Move&Learn: An Adaptive Exergame to Support Visual-Motor Skills of Children with Neurodevelopmental Disorders. Proceedings of Conference on Information Technology for Social Good, Roma, Italy, 9–11 September 2021; pp. 169–174. [Google Scholar]
- Rafiei Milajerdi, H.; Sheikh, M.; Najafabadi, M.G.; Saghaei, B.; Naghdi, N.; Dewey, D. The Effects of Physical Activity and Exergaming on Motor Skills and Executive Functions in Children with Autism Spectrum Disorder. Games Health J. 2021, 10, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Edwards, J.; Jeffrey, S.; May, T.; Rinehart, N.J.; Barnett, L.M. Does playing a sports active video game improve object control skills of children with autism spectrum disorder? J. Sport Health Sci. 2017, 6, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Educating the Student Body: Taking Physical Activity and Physical Education to School; The National Academies Press: Washington, DC, USA, 2013; p. 502. [Google Scholar] [CrossRef]
- Stodden, D.F.; Goodway, J.D.; Langendorfer, S.J.; Roberton, M.A.; Rudisill, M.E.; Garcia, C.; Garcia, L.E. A developmental perspective on the role of motor skill competence in physical activity: An emergent relationship. Quest 2008, 60, 290–306. [Google Scholar] [CrossRef]
- Ku, B. The Effects of Motor Skill Interventions on Motor Skills in Children with Developmental Disabilities: A Literature Review. Asian J. Kinesiol. 2020, 22, 11–22. [Google Scholar] [CrossRef]
- Sit, C.H.-P.; Yu, J.J.; Wong, S.H.-S.; Capio, C.M.; Masters, R. A school-based physical activity intervention for children with developmental coordination disorder: A randomized controlled trial. Res. Dev. Disabil. 2019, 89, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kong, Z.; Sze, T.M.; Yu, J.J.; Loprinzi, P.D.; Xiao, T.; Yeung, A.S.; Li, C.; Zhang, H.; Zou, L. Tai Chi as an Alternative Exercise to Improve Physical Fitness for Children and Adolescents with Intellectual Disability. Int. J. Environ. Res. Public Health 2019, 16, 1152. [Google Scholar] [CrossRef]
- Fragala-Pinkham, M.; Haley, S.M.; O’Neil, M.E. Group aquatic aerobic exercise for children with disabilities. Dev. Med. Child Neurol. 2008, 50, 822–827. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Performance Criteria |
|---|
| 1. An initial pose is formed with arms stretched behind and knees bent. |
| 2. Both arms are thrust upwards with force towards the top of the head. |
| 3. Both feet completed a simultaneous jump before touching the ground together. |
| 4. Both arms are stretched downwards during landing. |
| Performance Criteria |
|---|
| 1. The leg without load swings like a pendulum to create force. |
| 2. The leg without load is positioned on the side of the body. |
| 3. Arms are bent and in a swing to create force. |
| 4. The dominant or preferred leg is used to perform three or more consecutive leaps and landings. |
| 5. The non-dominant or non-preferred leg is used to perform three or more consecutive leaps and landings. |
| Performance Criteria |
|---|
| 1. One hand comes into contact with the ball at the height of the navel. |
| 2. The ball is pushed by the fingers and not the palm. |
| 3. Ball contacts surface in front of or to the outside of foot on the preferred side. |
| 4. The feet are not to be moved during four consecutive dribbles. |
| Performance Criteria |
|---|
| 1. Windup is initiated with downward movement of hand/arm. |
| 2. The ball is pushed by the fingers and not the palm. |
| 3. Weight is transferred by stepping with the foot opposite the throwing hand. |
| Sub-Item | Screenshot | Task Description | |
|---|---|---|---|
| Working Memory | Spatial Working Memory |  | Find the teddy bear in the box after showing and covering it |
| Working Memory Span |  | Find multiple (2–7) teddy bears in order | |
| Visual Working Memory |  | Find the changed fruit in four locations | |
| Global and Local Processing of Visual Perception | Congruent |  | Find the congruent flower and butterfly according to voice instructions |
| Incongruent |  | Find the incongruent flower and butterfly according to voice instructions | |
| Executive Function | Planning |  | Place the figures such as dog, cat, bone etc. in order by size |
| Response Inhibition |  | Press the button when a fish appears, hold the button when a shark appears | |
| Inhibition and Attention |  | Press the glass bottle without candy while not pressing the other bottle with candy | |
| Sub-Item | Screenshot | Task Description | |
|---|---|---|---|
| Activity Participation | Following Instructions |  | Follow the instructions and press the button that the finger pointed to |
| Imitation |  | Imitate the posture or movement of the avatar | |
| Solitary Play | Joint Attention |  | Touch the object where the gaze of the avatar’s eyes is directed |
| Pre-symbolic knowledge |  | Select the correct tool to use for the avatar’s behavior | |
| Symbolic behaviors |  | Imitate the behavior according to the verbal instruction using the avatar’s cue | |
| Cooperative Play | Understanding rules |  | Play the dice game with an examiner by taking turns |
| Emotion Perception |  | Recognize facial and emotional expressions | |
| Perspective taking |  | Select the view of the panda from the avatar’s perspective | |
| Section | Time | Exercise | Frequency |
|---|---|---|---|
| Warm up | 10 min | Dynamic stretching | 1 session/ week |
| Main part (VR exercise) | 40 min | Horizontal jump Running High jump Walking exercise Bar hurdle Step exercise Ball-kick Ball throw Balance exercise Animal-like motion | |
| Cool down | 10 min | Feedback and Dynamic stretching |
| Sub-Item | Details | |
|---|---|---|
| Horizontal Jump | Low-level |
|
| High-level |
| |
| Running | Low-level |
|
| High-level |
| |
| High Jump | Low-Level |
|
| High-Level |
| |
| Walking Exercise | Low-Level |
|
| High-Level |
| |
| Bar Hurdle | Low-Level |
|
| High-Level |
| |
| Step Exercise | Low-Level |
|
| High-Level |
| |
| Ball Kick | Low-Level |
|
| High-Level |
| |
| Ball Throw | Low-Level |
|
| High-Level |
| |
| Balance Exercise | Low-Level |
|
| High-Level |
| |
| Animal-Like Motion | Low-Level |
|
| High-Level |
| |
| P# | CS-VR (n = 15) | Age | Sex | P# | C-VR (n = 18) | Age | Sex |
|---|---|---|---|---|---|---|---|
| P1 | ASD | 10 | M | P1 | ASD | 13 | F |
| P2 | ASD | 13 | M | P2 | ASD | 9 | M |
| P1 | MID | 10 | F | P3 | ASD | 11 | M |
| P4 | ASD | 9 | M | P4 | MID | 9 | M |
| P5 | MID | 12 | M | P5 | ASD | 12 | F |
| P6 | DS | 10 | F | P6 | MID | 8 | M |
| P7 | ASD | 10 | M | P7 | DS | 8 | M |
| P8 | ASD | 11 | M | P8 | ASD | 12 | M |
| P9 | MID | 12 | M | P9 | MID | 12 | M |
| P10 | MID | 11 | F | P10 | ASD | 11 | F |
| P11 | ASD | 8 | M | P11 | MID | 12 | M |
| P12 | ASD | 13 | M | P12 | ASD | 13 | M |
| P13 | ASD | 10 | M | P13 | DS | 11 | F |
| P14 | ASD | 9 | M | P14 | ASD | 12 | M |
| P15 | MID | 9 | M | P15 | ASD | 11 | M |
| P16 | MID | 10 | M | ||||
| P17 | MID | 11 | M | ||||
| P18 | ASD | 10 | M |
| Variable | CS-VR | C-VR | Time × Intervention Interaction | Effect Size (ηp2) | ||||
|---|---|---|---|---|---|---|---|---|
| Pre Mean (SD) | Post Mean (SD) | MD | Pre Mean (SD) | Post Mean (SD) | MD | |||
| Extended horizontal jump (score) | 2.4 ± 1.41 | 5.6 ± 2.38 | 3.2 | 2.33 ± 1.23 | 3.11 ± 1.74 | 0.78 | p = 0.001 | 0.287 |
| Hop (score) | 4 ± 2.23 | 5.46 ± 1.45 | 1.46 | 3.77 ± 1.89 | 3.88 ± 1.6 | 0.11 | p = 0.015 | 0.178 |
| Stationary dribble (score) | 3.2 ± 1.78 | 3.6 ± 1.72 | 0.4 | 3.66 ± 1.74 | 4.16 ± 1.88 | 0.5 | p = 0.773 | 0.003 |
| Over arm throw (score) | 1.46 ± 1.3 | 3.73 ± 2.52 | 2.27 | 2.33 ± 1.28 | 2.83 ± 1.61 | 0.5 | p = 0.009 | 0.198 |
| Standing long jump (cm) | 105.33 ± 31.63 | 116.93 ± 29.91 | 11.6 | 102.27 ± 22.91 | 104.61 ± 24.77 | 2.34 | p = 0.002 | 0.316 |
| Recovery heart rate (beats/min) | 120 ± 9.53 | 109.73 ± 11.06 | −11 | 124.33 ± 8.1 | 117.05 ± 9.08 | −7.28 | p = 0.333 | 0.023 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.-B.; Ju, Y.; Kwon, H.; Youm, H.; Kim, M.J.; Chung, J. Effect of a Cognitive Function and Social Skills-Based Digital Exercise Therapy Using IoT on Motor Coordination in Children with Intellectual and Developmental Disability. Int. J. Environ. Res. Public Health 2022, 19, 16499. https://doi.org/10.3390/ijerph192416499
Park S-B, Ju Y, Kwon H, Youm H, Kim MJ, Chung J. Effect of a Cognitive Function and Social Skills-Based Digital Exercise Therapy Using IoT on Motor Coordination in Children with Intellectual and Developmental Disability. International Journal of Environmental Research and Public Health. 2022; 19(24):16499. https://doi.org/10.3390/ijerph192416499
Chicago/Turabian StylePark, Seung-Bo, Yumi Ju, Hyunjin Kwon, Heeok Youm, Min Joo Kim, and Jinwook Chung. 2022. "Effect of a Cognitive Function and Social Skills-Based Digital Exercise Therapy Using IoT on Motor Coordination in Children with Intellectual and Developmental Disability" International Journal of Environmental Research and Public Health 19, no. 24: 16499. https://doi.org/10.3390/ijerph192416499
APA StylePark, S.-B., Ju, Y., Kwon, H., Youm, H., Kim, M. J., & Chung, J. (2022). Effect of a Cognitive Function and Social Skills-Based Digital Exercise Therapy Using IoT on Motor Coordination in Children with Intellectual and Developmental Disability. International Journal of Environmental Research and Public Health, 19(24), 16499. https://doi.org/10.3390/ijerph192416499