
The Role of Social and Cultural Values in Pandemic Control in a Chinese Community: An Ethnographic Study on the Construction and Stigmatization of “Others” in Severe Acute Respiratory Syndrome (SARS) and COVID-19 in Hong Kong


{kind=link}
Abstract
1. Introduction
Significance
2. Methods
2.1. Design and Study Area
2.2. My Reflexivity in This Research
2.3. Data Collection
2.4. Ethics
2.5. Data Analysis
3. Results
3.1. Social Construction and Stigmatization of “Others”
3.1.1. Social Construction of “Diseased Others”
Infected Individuals
SARS and pneumonia [COVID-19] are highly infectious and deadly, so I avoid those who are infected. These two diseases are worse than AIDS because AIDS is not that contagious. Yuen Kwok-yung [Professor in microbiology at the Medical School of the University of Hong Kong] said that pneumonia can be transmitted by air, and even the WHO does not deny this. Some news reports have also reported that you can be infected by simply walking past virus carriers for a few seconds only. Therefore, if I know someone is infected, I would definitely avoid them.(P2)
One of my neighbors contracted SARS during [the] SARS [outbreak]. I remember when I learned that my neighbor had [contracted] SARS. My immediate response was to feel horrified and afraid, and I was concerned about whether I had already caught the virus from them. My other neighbors and I scolded the infected neighbor loudly outside their flat, blaming them for bringing this disease so close to our homes. I believe that, if you can maintain good hygiene, you will not be infected [with SARS]. Those who were infected with SARS are likely dirty and have low quality… Now, with regard to pneumonia [COVID-19], I feel even more nervous because if any of the neighbors are infected, we would all be sent to quarantine camps. Therefore, I have been maintaining an eye out for neighbors who appear to have a higher possibility of being infected and then avoid them. Those who are poor, are dirty, and have low quality are likely to be at a higher risk of being infected.(P26)
Three neighbors in my block were infected with pneumonia [COVID-19] in December [2020]. You know, if individuals from two flats in the same block are infected, then all the people living in the block would be forced to undergo compulsory testing. Because of these three neighbors, all of us were forced to undergo testing. I did not mind undergoing testing, but that affected my job because my boss immediately asked me not to come back to the office. I have no money if I cannot work because my salary is calculated on the basis of working days. These three neighbors have caused me to lose my salary. They are really ‘bad luck gods’ [a Cantonese slang that denotes someone who brings bad fortune to others].(P19)
It is very important to prevent myself from being infected. If [I] get infected, not only will my family members be sent to an isolation camp (quarantine camp), but my neighbors will also be required to undergo compulsory testing. If the neighbors know that I am infected, then I will be blamed. Similarly, if I know that a neighbor is infected, I will blame them as well because I will be forced to undergo compulsory testing. To avoid being blamed, I must be more cautious for evading infection.(P4)
I am not quite afraid of being infected, but I am considerably afraid of infecting others, especially because I can never know if I am a hidden virus carrier. If I infect others, I will make them and those who had contact with them suffer isolation [quarantine]. If it is just me becoming sick, that’s fine because it is my own business. However, being infected is a collective matter and has a chain effect; involving others is what I am most afraid of. Therefore, I am very cautious to avoid being infected, not just for my own health but, more importantly, for not involving others.(P58)
The building where I live had three [COVID-19] cases. When my colleagues learned about this from the Internet, they immediately reported it to my boss, and I was then asked to work from home immediately. Even my friends avoided me. I understood that everyone would be afraid of me, but I still felt bad. If I was the one to be infected, I would find it easier to understand [the situation]; however, it was my neighbors who were infected, not me. I believe that I did not deserve to be shunned.(P13)
- Neighbor A:
- “See? Block 45 has a new infection again! The residents living in that block must have low quality.”
- Neighbor B:
- “I don’t feel surprised though. The flat size in that block is small, so the people living there are likely to be not as rich as us. If they are not rich, then their jobs may not be good, and they may not be of good quality; otherwise, they would be able to get a good job and high salary and be able to afford to live in bigger units like us. If they were of high quality, then they would be cleaner. Do you recognize that all infections are happening in blocks with a small flat size?” [SARS_G2]
Those Who Had Respiratory Symptoms
It is a bad idea to get sick during COVID [COVID-19], because no doctor will want to see you. I had a fever and diarrhea two months ago, and it was a nightmare for me because no doctors were willing to see me. Some would ask you to have a proof of a virus-negative result from a deep throat saliva test before they see you, but taking a deep throat test requires [several] days to get the result, and I would have died before I could get that. Others would just ask you to go to the emergency room. Indeed, many diseases can give you a fever and diarrhea, but in COVID times, all people, including doctors, would just think that you are getting COVID. It is a sad thing, because you can never imagine that you are being treated in such a way by doctors, who are expected to help those who are sick. The whole experience in COVID is much different from SARS. It is especially important to stay healthy in these COVID times.(P69)
Chronically Ill Patients
News reports have stated that chronically ill patients can carry a high viral load, become “super-spreaders,” and infect many people because they are weakened [more than others are] when infected [with COVID-19]. I have avoided those whom I know to have chronic conditions since the [COVID-19] outbreak. Indeed, I learned about this during [the] SARS [outbreak]. I remember that a chronically ill patient was a super-spreader at that time, and he had spread the virus through his excreta when he was living in Amoy Gardens [a private housing area]. He caused many people living there to become infected.(P10)
I believe that chronically ill patients are dangerous because they are super-spreaders. They can carry a high viral load and can infect many people. Because pneumonia [COVID-19] is very similar to SARS, I believe that chronically ill patients might become super-spreaders again. It is better for me to stay away from them. Although they may not be super-spreaders at this time, they still have to go to hospitals and clinics often. You know, hospitals and clinics have numerous bacteria and viruses, so it is safer for me to stay away from them these days.(P17)
3.1.2. Social Construction of “Deviant Others”
Not Wearing a Face Mask
If I see anyone not wearing a face mask, I walk away from them and give them a dirty look. I understand that no one likes wearing a face mask, but everyone should make efforts to fight against pneumonia [COVID-19] by wearing a face mask. Wearing a face mask is not only for your own health, but also for others’ health. All of us should have learned about this from [the] SARS [outbreak] already. At that time, no one would force you to use a face mask, but everyone would use a face mask in public areas, even though there was no face mask law at that time, because everyone understood that wearing a face mask was socially responsible. If someone does not wear a face mask, that means that they do not have [a sense of] civic responsibility and consideration for others. I would let these people know explicitly that they are so disgusting.(P24)
I walk away from those who are smoking on the streets because they have to take off their face masks when they smoke. They blow out air and saliva, so it is very dangerous to walk close to them. […] Smoking indeed is very annoying. Those who smoke are not good people, and they may be members of gangs, so it is impossible to ask them not to smoke unless you want to be beaten. The best way is to walk away from them.(P11)
- Bus driver:
- “You have to wear a face mask to get on this bus.”
- Old lady:
- “I am sorry but I have no face mask now…”
- Bus driver:
- “You cannot get on [the bus] without a face mask. If you have no face mask, you should stay at home. I cannot help.”
Not Following the Stay-at-Home Policy
Now, everyone is talking about staying at home on Facebook. The slogan of ‘I (health-care provider) stay at work for you (the public), you stay at home for us’ is really a form of social pressure. It sounds like, if you do not stay at home, you are bad. I dare not tell others that I still go out because I am working in a restaurant, and my job does not allow me to work from home. However, no one would care about the fact that many people cannot stay at home and work from home, but others would just think that you are harming society because you still go out.(P63)
To help our society and to reduce the burden on doctors and nurses, I think we should stay at home as much as we can these days. Many doctors and nurses have been posting the slogan of ‘I stay at work for you, you stay at home for us’ on Facebook now. They have been asking for our help, so I think every responsible citizen should stay at home as much as possible. Those who are still going out and eating out are so irresponsible toward society! I don’t care if they are exposing themselves to harm and infection, but I care that they are harming others and increasing the workload of health-care providers by exposing themselves to infection.(P3)
This is really a motivating slogan because this slogan not only praises doctors and nurses but also emphasizes to the public that everyone can contribute to the fight against the pandemic [COVID-19]. Every time I see this slogan, I feel that I am playing a very important role [in the fight] against pneumonia [COVID-19]. If I do not follow this slogan, then it would appear that I am not playing a role in this pandemic and not supporting doctors and nurses.(P42)
I also want to stay at home. After all, who is not afraid of being infected? However, not all people can really stay at home. I still have to go out for work because I am living in a subdivided flat [a flat in which multiple families reside], so how can I afford to use a computer and the Internet to work from home? Also, not all jobs allow working from home. For example, many street cleaners, transportation workers, and service and catering workers have to go out to work. Not all people have the privilege [of being able to] work from home. However, working from home and staying at home have become new social values that you have to follow now because no one would think that you cannot stay at home.(P35)
Not Following the Takeout Policy
Medical professors always encourage eating takeout [instead of dining-in]. Yuen Kwok-yung [Professor of microbiology at the Medical School of the University of Hong Kong] has said that dining in can be very dangerous because everyone takes off their face mask when eating. Now, so many people are buying takeout, and it [the encouragement for buying takeout] is just like a type of peer pressure; if you dine-in, you would appear strange. If someone dines in, I would think that they are very brave, but simultaneously, I would also think that they are not very responsible toward society.(P16)
It is very difficult for me to eat takeout because I work outdoors and do not have a stable workplace. Dining in is very important to me because this is the only moment that I can have some rest and can enjoy air conditioning. If I am forced to eat takeout, I can just go to parks to eat, but parks are very hot now. However, not wearing a face mask outdoors is against the law, so can I really eat in parks? Eating takeout looks very simple to many people, but it is very difficult for those who have to work outdoors, like me. It is a privilege if your job allows you to eat takeout.(P9)
People of Low Socioeconomic Status
I believe that those who do not wear face masks belong to a low social class. They cannot afford to buy face masks, and they are not sufficiently educated to understand the importance of wearing face masks. Therefore, I believe that people from low social classes are a high-risk group. If you look at recent community outbreaks, most of them occurred in public housing estates [subsidized housing provided by the government for the low-income class] and in old buildings in poor districts. Have you ever seen the Mid-Levels and Kowloon Tong [residential areas for the high-income class] experience an outbreak? No, because the people living [there] are rich and highly educated, so they wear face masks and are more hygienic. Not only in the case of pneumonia [COVID-19], but also during the SARS outbreak, these infections never hit the rich areas.(P7)
- Neighbor A:
- “That fat man’s family is really dirty. I cannot understand why they do not wear face masks. They just used tissues to cover their noses and mouths.”
- Neighbor B:
- “I have heard that they are receiving CSSA (Comprehensive Social Security Assistance) and are waiting for public housing estates, so they may not be able to afford [buying] face masks.”
- Neighbor C:
- “From their appearance and dressing, you can understand that they are poor. If they are not ‘eating government welfare’ [a Cantonese slang meaning receiving social welfare assistance from the government], how can they afford to live here? You know, the government pays the rent for them while they are waiting for public housing.”
- Neighbor B:
- “We taxpayers keep subsidizing these lazy people, but they never make any contribution [to society]. They just keep taking resources from society, and now, they are harming society by not wearing face masks. If they become infected, all of us will be affected, and we will all be sent to an isolation camp [quarantine camp].” (COVID_G5)
Older People
I believe that older people are the most uncooperative group. I can always see older people pull their face masks down to the chin. Indeed, those who spit on the streets are mostly older people. During [the] SARS [outbreak], older people were a high-risk group, and they were very “toxic” because they were hidden virus spreaders. I believe that this logic [also] applies to the pneumonia [COVID-19] outbreak because many cluster outbreaks are occurring among older people in nursing homes. I would walk away from them [older people], as you can never know if any of them is a hidden virus spreader.(P18)
I also want [to wear] face masks, but they are very expensive now. I have retired and have no income, and I just rely on “fruit money” [Old Age Allowance] and my savings to maintain my livelihood. How can I have spare money to buy face masks? If I have money, I would rather buy food first. If you have no face mask, you will not die, but if you have no food, you will die in 2 or 3 days. I am not afraid of pneumonia [COVID-19], but I am afraid of having no money and no food. I know that I have to wear a face mask when I am not at home, so I usually reuse a face mask if I need to go out.(P20)
Not Receiving COVID-19 Vaccines
The government and doctors have been saying that you should receive vaccines because you are protecting not only yourselves but also others. They have been saying that receiving vaccines is a social responsibility, and this is like a form of social pressure. If you do it, then you are a good person; otherwise, you will be labeled as having no civic responsibility.(P22)
I would not intentionally avoid those who have not been vaccinated, but I would consider those who have been vaccinated as safer and so would be more willing to gather or eat with them. I would feel more hesitant to gather with those who have not been vaccinated because they are at a higher risk [of infection with COVID-19]. If they were to be infected, I would be quarantined even though I have been vaccinated.(P64)
I have some friends who eat with only those who have been vaccinated—they really ask if you have been vaccinated before eating with you. A friend of mine who has been vaccinated really asked me whether I have been vaccinated before eating with me. Because I had not yet been vaccinated, she suggested eating later… Vaccination is no longer a choice for me, but it has become a pressure for me if I still want to eat with my friends.(P41)
I have been vaccinated, and now, I can eat with more of my friends at a table according to the vaccine bubble. If we are all vaccinated, then there will be less restriction in eating because we can sit together at the same table… When we organize meal gatherings, we usually only ask those who have been vaccinated to join us. It would be very difficult to eat with those who have not yet been vaccinated because doing so would mean that we are unable to sit together and have to sit at separate tables.(P49)
I can only eat with those who have already finished the vaccine course according to the Vaccine Pass. I have some very good friends and I want to see them, but unfortunately they are not yet vaccinated, so they cannot eat in any restaurants. You know, it is very important to eat together so we can have chit-chat. But because they are not yet vaccinated, they cannot eat in any restaurants, so I haven’t met them for a long time already.(P68)
3.1.3. Social Construction of “Geographical Others”
I believe that Tsz Wan Shan and Tuen Mun are very dangerous because there have been serious cluster outbreaks in these two areas. In Tsz Wan Shan, many people have been infected at restaurants in shopping malls. If I know that someone is living in Tsz Wan Shan or Tuen Mun, I will avoid them. […] I remember that there were certain dangerous areas that I would avoid during [the] SARS [outbreak] as well, such as Shatin and Amoy Gardens, because there were severe outbreaks there.(P14)
Rich districts would be safer [than would poor districts] because the people [residing] there would have higher quality and be cleaner. I would avoid going to poor districts. The most dangerous areas are those with many poor people because they would be dirty. The education level [of the people residing in poor areas] would be low, so they do not have much knowledge regarding hygiene. Also, they [poor people] can only work in low-status jobs, such as cleaning and catering, which are associated with high risks of [SARS and COVID-19] infection. Many outbreaks have occurred in public housing estates and old districts because poor people reside there.(P1)
All my relatives and friends are scared of me because I live in a building that was enclosed by the government. They knew about this from the news, so I could not hide this [information]. My boss even asked me not to go back to the office for two weeks. Although I tested negative [for COVID-19 during the compulsory testing] and I can go back to work now, my colleagues still avoid me. My relatives avoid me as well, so I could not celebrate Chinese New Year with them this year… I feel that the situation is a bit unfair because enclosure orders are rarely implemented in rich districts, even though infections are found in the rich districts as well. I feel that we are targeted because we are poor. Do you think that the government would dare to enclose the Mid-Levels? I do not think so because the government is afraid of the rich.(P32)
3.1.4. Social Construction of “Occupational Others”
It sounds like many cluster outbreaks are related to restaurants. Catering workers have to come into contact with many customers every day, and they have to touch things that have been used by different customers. Their hands can easily carry the [COVID-19] virus [and spread it to them]. Also, most of the catering workers belong to a low social class, so they may not be very hygienic and can be potential virus spreaders. Therefore, I do not go out to eat now.(P15)
Street cleaners are at a very high risk because they have to touch a lot of dirty things. Although I know that they have contributed a lot to our society, I would still avoid them. Because of their job and because they belong to a low social class, they would find it very difficult to prevent themselves from being infected.(P28)
Because I am working in a hospital, I had moved to a hotel to avoid bringing the virus home. However, finding a hotel was a very frustrating process. Many hotels would ask you to fill in a health declaration form, asking if you have any symptoms and if you have contacted any infected patients. Because of my job, I would encounter infected patients every day. But if I were honest with them [hotel staff], I would not be able to get a room. It is frustrating. Although many people would say that they support you, in reality, we were not accepted by society during COVID [the COVID-19 pandemic] and SARS. When epidemics come, we [health-care providers] will be isolated.(P30)
Health-care workers are dangerous because they are working in hospitals. I am living close to the Prince of Wales Hospital, and you know, this hospital had a severe outbreak of SARS before. This pneumonia [COVID-19] really makes me think about those horrible days of [the] SARS [outbreak]. However, I welcome them [health-care workers] to live here because they are professionals and so can increase the status and quality of this housing area. I trust that they would be very clean and would not spread viruses and bacteria among us [the residents]. After all, they are highly educated and are of high quality, so they should not be too dangerous.(P56)
3.1.5. Social Construction of “Ethnic Others”
I believe that Filipino and Indonesian maids are at a very high risk because their home countries are not developed, so their hygiene standards are not high. It is not news at all that the food prepared by these maids can be contaminated. Also, they often get together on Sundays, without any face masks and social distancing. They often leave places in a mess after their gathering, too. The pneumonia [COVID-19] outbreaks in the hostels of these maids further prove that they are at high risk. I have been aware of their risk since [the] SARS [outbreak], so I do not hire any maids since then.(P33)
It is the third case of mutated virus infections among Filipino maids already. They are dangerous, but it is not a surprise. The Philippines is not a well-developed country, so [Filipino] people’s hygiene standards are not high. The [COVID-19] outbreak there was also very serious. Therefore, you can expect that there would be many virus carriers in this group. You know, they often hang out with other Filipino maids on Sundays, sitting very close to each other without any face masks or social distancing. Whenever I see them these days, I walk away from them. They really have very low awareness, and they still complain about the compulsory virus testing order on them. Because they have low awareness, they do not remain alert regarding infection—this is the most dangerous thing.(P52)
India and Pakistan have many cases [of COVID-19]. It is not surprising because India and Pakistan are under-developed. The hygiene standards of these countries and their people are low as well. I dare not go to those places where there are many Indians and Pakistanis, such as Chungking Mansions. Actually, Chungking Mansions have been infamous and dangerous for a long time. This outbreak period is even more dangerous because of these people. They are the poor in Hong Kong and can only work in low-status jobs, which makes them more risk-prone [to COVID-19 infection].(P21)
Foreigners are dangerous because pneumonia [COVID-19] is so serious in many Western countries. What I worry the most about are those who are studying overseas and now coming back to Hong Kong for summer vacation. Although they should stay in hotels for quarantine, the news reported that many of them had escaped from quarantine. Therefore, I would pay high attention to see if anyone around me is wearing an electronic wristband. If yes, I would immediately walk away from them. Even many shops refuse to allow people with electronic wristbands to go in. […] Also, many foreigners do not wear face masks properly. They only wear a cloth face mask, or they do not cover their noses, and this causes them to spread the virus. Whenever I see any foreigners who are not wearing a surgical face mask properly, I walk away from them immediately.(P34)
I believe that Westerners and students studying abroad are not as dangerous as Indians, Pakistanis, and Filipino and Indonesian maids. They [Westerners and students studying abroad] come from more advanced places [than India, Pakistan, the Philippines, and Indonesia], which are richer and more highly educated, so they should be cleaner. It is just that Westerners do not wear a face mask; otherwise, they are not that dangerous. They are unlike those who are coming from under-developed places.(P34)
3.2. Traditional Cultural Values
3.2.1. Glorification and Moral Condemnation of Healthcare Providers
The doctors and nurses in Hong Kong have a very high quality. We are so fortunate to have these very good doctors and nurses who have sacrificed themselves during the two outbreaks. They are unlike those in Taiwan, where many doctors and nurses were so unprofessional that they escaped from hospitals during [the] SARS [outbreak]. “Doctors have a parental heart,” and leaving patients behind because of the fear of being infected is so unprofessional, selfish, and irresponsible. If you are really afraid of being infected, then you should not work in health care.(P12)
Without a doubt, I appreciate the work of doctors and nurses in this time of pneumonia [COVID-19]. However, frankly, it is their responsibility, and they are obligated. They are well paid for this, and no one takes advantage of them. It is because of this potential risk that they are well paid as a reward, and this is the core value of a commercial society. They should have understood this risk well when they chose to work in health care. If they are afraid, they can always quit, and no one will force them to continue. If they choose to stay, then they should not complain at all. I agree that they should be respected, but I do not think that we need to overemphasize their devotion.(P5)
It is totally unacceptable for these private hospitals and private doctors to refuse pneumonia [COVID-19] patients. They are well paid, and they should have already thought about this risk when they first chose to work in health care. Refusing a patient is immoral, and private hospitals and private doctors should help the public hospitals by treating pneumonia patients as well in this difficult time. “A healing person should have a parental heart”. I am so frustrated that our doctors and nurses nowadays have become so different from those in the SARS outbreak.(P55)
I appreciate the doctors and nurses who worked during [the] SARS [outbreak] much more than those who worked in this pneumonia [COVID-19] outbreak. During [the] SARS [outbreak], none of the doctors and nurses ever complained; they just kept working very hard. However, during the current pneumonia outbreak, some doctors and nurses have not been devoted. They have many complaints and even went on strike. I believe that, if the public had not condemned their strike, it [their strike] would have still be on now. As doctors and nurses, they should consider patients their top priority because “a healing person should have a parental heart.” If they are dissatisfied, they can just quit, but they should never make use of patients to achieve their goals.(P66)
3.2.2. Patriarchal Values against Homemakers
I feel that the [periods of the] SARS and pneumonia [COVID-19] outbreaks were the toughest time for me. As a housewife, I have no excuse, and I have to work harder to keep the home clean. No one thinks about how terrible the life of a housewife can be during pandemics. I have to do more cleaning and disinfection at home. If any of my family members were to get infected, I would be responsible, and others may think that I did not do my job well. The situation is worse under the pneumonia outbreak because the pressure is much heavier than that under [the] SARS [outbreak]. During the SARS [outbreak], I only had to do more home cleaning. However, during [the] pneumonia [outbreak], I have had to not only do more home cleaning but also take care of my husband and children, all of whom are working or studying from home. The situation is similar to “closed-cage beast fighting” [a Cantonese slang term meaning that several people are struggling together within a small area]. I did not ask for my husband’s help because he would expect it [household work] to be my duty. I believe that all people think it is normal for a housewife to do all these [tasks]. After all, as a housewife, this is what I am expected to do.(P25)
I have been much busier during [the] pneumonia [COVID-19] [pandemic] than [I was] during [the] SARS [outbreak]. During [the] SARS [outbreak], I only had to do more cleaning at home, and I could still go out to work to have some hours off from family duties. However, during [the] pneumonia [pandemic], there has been far more for me to do because I have to work from home. In addition to office work, I have to do cleaning and disinfection at home and take care of my husband and two children simultaneously, so I have to perform at least three tasks simultaneously. I am the only one to keep my children busy until they have gone to sleep at night, but then I have to do my office work and housework. I am so tired because I have been working for almost 24 h a day throughout the pneumonia [pandemic]. No one helps me, not even my husband, because he believes that those [household tasks] are my duties.(P23)
4. Discussion
5. Limitations
6. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. The Demographics of the Participants
| Informant ID | Gender | Age | Education Level | Occupation | Ethnicity |
| P1 | F | 44 | University | Executive officer | Chinese |
| P2 | F | 39 | University | Secretary | Chinese |
| P3 | F | 42 | Masters | Executive officer | Chinese |
| P4 | M | 50 | Masters | Information and technology officer | Chinese |
| P5 | M | 36 | Masters | Research officer | Chinese |
| P6 | F | 36 | University | Clerk | Chinese |
| P7 | F | 38 | University | Clerical officer | Chinese |
| P8 | F | 39 | Masters | Accounting officer | Chinese |
| P9 | M | 44 | Secondary | Construction worker | Chinese |
| P10 | F | 52 | Secondary | Clerk | Chinese |
| P11 | F | 58 | Secondary | Clerk | Chinese |
| P12 | F | 56 | Secondary | Clerk | Chinese |
| P13 | F | 49 | University | Project officer | Chinese |
| P14 | F | 54 | Secondary | Secretary | Chinese |
| P15 | F | 38 | University | Research associate | Chinese |
| P16 | M | 36 | Masters | Research associate | Chinese |
| P17 | F | 48 | Junior-secondary | Cleaning lady | Chinese |
| P18 | F | 56 | Secondary | Clerk | Chinese |
| P19 | F | 62 | Junior secondary | Cleaning lady | Chinese |
| P20 | F | 77 | Primary | Retired | Chinese |
| P21 | F | 52 | Secondary | Food and catering | Chinese |
| P22 | M | 50 | University | Civil servant | Chinese |
| P23 | F | 42 | University | Financial planner | Chinese |
| P24 | M | 56 | University | Civil servant | Chinese |
| P25 | F | 38 | University | Housewife | Chinese |
| P26 | F | 64 | University | Housewife | Chinese |
| P27 | M | 40 | University | Customer service | Chinese |
| P28 | F | 54 | Secondary | Housewife | Chinese |
| P29 | M | 60 | Secondary | Food and catering | Chinese |
| P30 | M | 39 | University | Doctor | Chinese |
| P31 | M | 45 | University | Information and technology programmer | Chinese |
| P32 | M | 56 | Secondary | Food and catering | Chinese |
| P33 | M | 41 | University | Transportation | Chinese |
| P34 | F | 50 | University | Accounting | Chinese |
| P35 | M | 61 | Secondary | Food and catering | Chinese |
| P36 | M | 75 | Secondary | Retired | Chinese |
| P37 | M | 78 | Secondary | Retired | Chinese |
| P38 | F | 66 | Secondary | Part-time cleaner | Chinese |
| P39 | M | 71 | Secondary | Retired | Chinese |
| P40 | M | 62 | University | Hotel management | Chinese |
| P41 | F | 52 | Secondary | Food and catering | Chinese |
| P42 | M | 58 | Secondary | Property management | Chinese |
| P43 | M | 61 | University | Property management | Chinese |
| P44 | F | 60 | Secondary | Clerk | Chinese |
| P45 | F | 64 | Secondary | Clerk | Chinese |
| P46 | F | 46 | Secondary | Clerk | Chinese |
| P47 | M | 51 | University | Finance | Chinese |
| P48 | F | 49 | University | Finance | Chinese |
| P49 | F | 52 | University | Finance | Chinese |
| P50 | M | 61 | University | Sales and retailing | Chinese |
| P51 | F | 44 | Secondary | Clerk | Chinese |
| P52 | F | 46 | University | Finance | Chinese |
| P53 | F | 36 | University | Teacher | Chinese |
| P54 | F | 40 | University | Clerk | Chinese |
| P55 | M | 56 | University | Banking | Chinese |
| P56 | F | 68 | Secondary | Part-time clerk | Chinese |
| P57 | M | 61 | University | Banking | Chinese |
| P58 | F | 64 | Secondary | Sales and retailing | Chinese |
| P59 | M | 58 | University | Sales and retailing | Chinese |
| P60 | M | 75 | Secondary | Retired | Chinese |
| P61 | F | 70 | Secondary | Housewife | Chinese |
| P62 | M | 51 | Secondary | Sales and retailing | Chinese |
| P63 | F | 40 | Secondary | Food and catering | Chinese |
| P64 | F | 58 | Secondary | Clerk | Chinese |
| P65 | M | 41 | Masters | Tourism | Chinese |
| P66 | F | 45 | Masters | Logistics and shipping | Chinese |
| P67 | M | 40 | University | Tourism | Chinese |
| P68 | F | 38 | University | Clerk | Chinese |
| P69 | F | 37 | University | Sales and retailing | Chinese |
| P70 | M | 40 | Secondary | Clerk | Chinese |
Appendix B. Interview Question Guide
- What are the impressions of SARS to you?
- How was your life during the time of the SARS outbreak? How did your life was affected by SARS?
- What are the most unforgettable experiences to you in the SARS outbreak (good and/or bad)? Can you share them with me?
- What are the difficulties that you encountered in the SARS outbreak?
- To you, who are the people that you believe more vulnerable to SARS? Why?
- Are there any particular groups of people that you would avoid during the SARS outbreak? Why?
- What are the impressions of COVID-19 to you?
- How was your life during the COVID-19 pandemic? How did your life was affected by COVID-19?
- What are the most unforgettable experiences to you in the COVID-19 pandemic (good and/or bad)? Can you share them with me?
- What are the difficulties that you have encountered in the COVID-19 pandemic?
- To you, who are the people that you believe more vulnerable to COVID-19? Why?
- Are there any particular groups of people that you would avoid during the COVID-19 pandemic? Why?
- Do you think the experiences that you have gone through in the SARS outbreak can affect you when facing the COVID-19 pandemic now? How?
- Are there any experiences that you found similar during the SARS outbreak and COVID-19 outbreak? If yes, what are these experiences?
- Are there any experiences that you found contrasting between the SARS outbreak and COVID-19 outbreak? If yes, what are these experiences?
- You have experienced both the SARS outbreak and COVID-19 pandemic. How will you compare your life and experiences (or anything that you want to compare) in these two outbreaks?
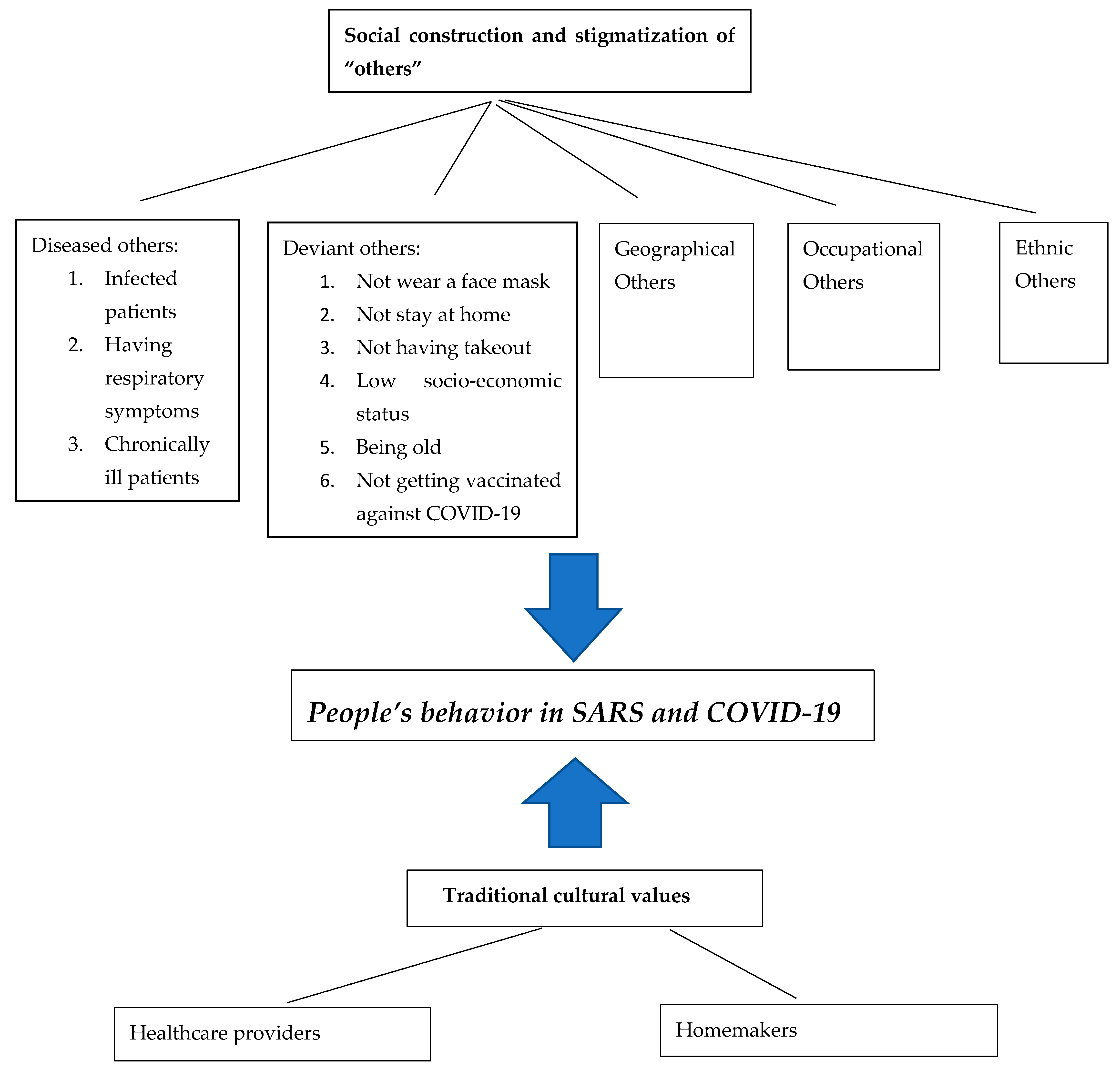
Appendix C. Concept Map on Social and Cultural Values in Infection Control of SARS and COVID-19 in Hong Kong

References
- Hall, M.A.; Orentlicher, D.; Bobinski, M.A.; Bagley, N.; Cohen, I.G. “8. Public Health Law”. Health Care Law and Ethics, 9th ed.; Wolters Kluwer: New York, NY, USA, 2018; p. 908. [Google Scholar]
- Posid, J.M.; Bruce, S.; Guarnizo, J.T.; Taylor, M.L.; Garza, B.W. SARS: Mobilizing and Maintaining a Public Health Emergency Response. J. Public Health Manag. Pract. 2005, 11, 208–215. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. “Statement on the Second Meeting of the International Health Regulations (2005) Emergency Committee Regarding the Outbreak of Novel Coronavirus (2019-nCoV)” 2020. Available online: https://www.who.int/news/item/30-01-2020-statement-on-the-second-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavirus-(2019-ncov) (accessed on 10 June 2022).
- World Health Organization. Statement on the Seventh Meeting of the International Health Regulations (2005) Emergency Committee Regarding the Coronavirus Disease (COVID-19) Pandemic. 2021. Available online: https://www.who.int/news/item/19-04-2021-statement-on-the-seventh-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-coronavirus-disease-(COVID-19)-pandemic (accessed on 10 June 2022).
- Centers for Disease Control and Prevention. SARS Basics Fact Sheet. 2017. Available online: https://www.cdc.gov/sars/about/fs-sars.html. (accessed on 1 June 2022).
- Centers for Disease Control and Prevention. SARS-CoV-2 Variant Classifications and Definitions. 2017. Available online: https://www.cdc.gov/coronavirus/2019-ncov/variants/variant-classifications.html. (accessed on 1 June 2022).
- Legislative Council. Chronology of Major Events of the SARS Incident in Hong Kong. 2004. Available online: https://www.legco.gov.hk/yr03-04/chinese/sc/sc_sars/reports/tbl/e3b-13.pdf (accessed on 8 May 2022).
- Department of Health. Latest Figures on 2003 Severe Acute Respiratory Syndrome Outbreak (as at 19 January 2004). 2004. Available online: https://www.info.gov.hk/info/sars/en/infected.htm. (accessed on 2 May 2022).
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. 2019. Available online: https://covid19.who.int/ (accessed on 7 July 2022).
- Centre for Health Protection. Latest Situation of Coronavirus Disease (COVID-19) in Hong Kong. 2022. Available online: https://chp-dashboard.geodata.gov.hk/covid-19/en.html. (accessed on 7 July 2022).
- Yen, I.H.; Syme, S.L. The Social Environment and Health: A Discussion of the Epidemiologic Literature. Annu. Rev. Public Health 1999, 20, 287–308. [Google Scholar] [CrossRef] [PubMed]
- Chingwaru, W.; Vidmar, J. Culture, myths and panic: Three decades and beyond with an HIV/AIDS epidemic in Zimbabwe. Glob. Public Health 2018, 13, 249–264. [Google Scholar] [CrossRef] [PubMed]
- Farmer, P. Infections and Inequalities: The Modern Plagues; University of California Press: Berkeley, CA, USA, 1999. [Google Scholar]
- Hays, J.N. The Burdens of Disease: Epidemics and Human Response in Western History; Rutgers University Press: New Brunswick, NJ, USA, 2003. [Google Scholar]
- Farmer, P. AIDS and Accusation: Haiti and the Geography of Blame; University of California Press: Berkeley, CA, USA, 2006. [Google Scholar]
- Goffman, E. Stigma: Notes on the Management of Spoiled Identity; Penguin: London, UK, 1968. [Google Scholar]
- Ayede, A.; Osinusi, K.; Falade, A.G. Responses to spread of Ebola virus disease epidemic in West Africa: A review. Afr. J. Med. Med. Sci. 2016, 45, 119–134. [Google Scholar]
- Beine, D.K. Ensnared by AIDS: Cultural Contexts of HIV/AIDS in Nepal; Mandala Book Point: Kathmandu, Nepal, 2003. [Google Scholar]
- Siu, Y.M. From An Epidemic to Mass “Panic”: The Cultural Construction of the SARS Epidemic in Hong Kong. Ph.D. Thesis, School of Population Health, The University of Queensland, Brisbane, Australia, 2007. [Google Scholar]
- Bernard, H.R. Research Methods in Anthropology: Qualitative and Quantitative Approaches; AltaMira Press: Walnut Creek, CA, USA, 2002. [Google Scholar]
- Chung, G.K.K.; Chan, S.M.; Chan, Y.H.; Woo, J.; Wong, H.; Wong, S.Y.; Yeoh, E.K.; Marmot, M.; Chung, R.Y.N. Socioeconomic patterns of COVID-19 clusters in low-incidence city, Hong Kong. Emerg. Infect. Dis. 2021, 27, 2874–2877. [Google Scholar] [CrossRef]
- Chung, G.K.K.; Chan, S.M.; Chan, Y.H.; Yip, T.C.F.; Ma, H.M.; Wong, G.L.H.; Chung, R.Y.N.; Wong, H.; Wong, S.Y.S.; Yeoh, E.K.; et al. Differential Impacts of Multimorbidity on COVID-19 Severity across the Socioeconomic Ladder in Hong Kong: A Syndemic Perspective. Int. J. Environ. Res. Public Health 2021, 18, 8168. [Google Scholar] [CrossRef]
- Wu, Y.; Yan, X.; Zhao, S.; Wang, J.X.; Ran, J.J.; Dong, D.; Wang, M.; Fung, H.; Yeoh, E.K.; Chung, R.Y.N. Association of time to diagnosis with socioeconomic position and geographical accessibility to healthcare among symptomatic COVID-19 patients: A retrospective study in Hong Kong. Health Place 2020, 66, 102465. [Google Scholar] [CrossRef]
- Hong Kong Federation of Trade Unions. Introduction. Available online: http://www.ftu.org.hk/en/about_us/introduction/. (accessed on 6 January 2020).
- Green, J.; Thorogood, N. Qualitative Methods for Health Research; SAGE Publications: London, UK, 2004. [Google Scholar]
- Thomas, D.R. A general inductive approach for analyzing qualitative evaluation data. Am. J. Eval. 2006, 27, 237–246. [Google Scholar] [CrossRef]
- Liamputtong, P.; Ezzy, D. Qualitative Research Methods. South Melbourne; Oxford University Press: Victoria, UK, 2005. [Google Scholar]
- RTHK. Private Hospitals Should Treat COVID: Han Zheng. 2022. Available online: https://news.rthk.hk/rthk/en/component/k2/1637576-20220307.htm (accessed on 7 March 2022).
- SCMP. Why Haven’t Hong Kong’s Private Hospitals Stepped Up in Covid Fight? Lack of Facilities, Manpower to Blame, Sector Chief Says as Pressure Mounts. 2022. Available online: https://www.scmp.com/news/hong-kong/health-environment/article/3169610/hong-kong-private-hospitals-lack-isolation (accessed on 3 March 2022).
- SCMP. Coronavirus: Chinese State Leader Slams Hong Kong Private Hospitals over Reluctance to Admit COVID-19 Patients. 2022. Available online: https://www.scmp.com/news/hong-kong/health-environment/article/3169465/coronavirus-chinese-state-leader-slams-hong-kong?module=perpetual_scroll_0&pgtype=article&campaign=3169465 (accessed on 6 March 2022).
- Lau, J.T.F.; Yang, X.; Tsui, H.Y.; Kim, J.H. Monitoring Community Responses to the SARS Epidemic in Hong Kong: From Day 10 to Day 62. J. Epidemiol. Community Health 2003, 57, 864–870. [Google Scholar] [CrossRef]
- Leung, G.M.; Lam, T.H.; Ho, L.M.; Ho, S.Y.; Chan, B.H.; Wong, I.O.; Hedley, A.J. The Impact of Community Psychological Responses on Outbreak Control for Severe Acute Respiratory Syndrome in Hong Kong. J. Epidemiol. Community Health 2003, 57, 857–863. [Google Scholar] [CrossRef]
- Tang, C.S.K.; Wong, C.Y. Factors Influencing the Wearing of Facemasks to Prevent the Severe Acute Respiratory Syndrome among Adult Chinese in Hong Kong. Prev. Med. 2004, 39, 1187–1193. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.Y.; Tang, C.S.K. Practice of Habitual and Volitional Health Behaviours to Prevent Severe Acute Respiratory Syndrome among Chinese Adolescents in Hong Kong. J. Adolesc. Health 2005, 36, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Lui, T.L. Rearguard Politics: Hong Kong’s Middle Class. Dev. Econ. 2003, XL1-2, 161–183. [Google Scholar] [CrossRef][Green Version]
- Baer, H.A.; Singer, M.; Susser, I. Medical Anthropology and the World System: Critical Perspectives; Bergin & Garvey: Westport, CT, USA, 1997. [Google Scholar]
- Douglas, M. Purity and Danger: An Analysis of the Concepts of Pollution and Taboo; Ark: London, UK, 1984. [Google Scholar]
- Jiang, T.; Zhou, X.; Lin, L.; Pan, Y.; Zhong, Y.; Wang, X.; Zhu, H. COVID-19-related stigma and its influencing factors: A nationwide cross-sectional study during the early stage of pandemic in China. BMJ Open 2021, 11, e048983. [Google Scholar] [CrossRef]
- Singh, R.; Subedi, M. COVID-19 and stigma: Social discrimination towards frontline healthcare providers and COVID-19 recovered patients in Nepal. Asian J. Psychiatry 2020, 53, 102222. [Google Scholar] [CrossRef]
- Siu, J.Y.M. The SARS-associated stigma of SARS victims in the post-SARS era of Hong Kong. Qual. Health Res. 2008, 18, 729–738. [Google Scholar] [CrossRef]
- Siu, J.Y.M. Health inequality experienced by the socially disadvantaged populations in the outbreak of COVID-19 in Hong Kong: An interaction with social inequality. Health Soc. Care Community 2020, 29, 1522–1529. [Google Scholar] [CrossRef]
- Bhanot, D.; Singh, T.; Verma, S.K.; Shared, S. Stigma and Discrimination During COVID-19 Pandemic. Front. Public Health 2021, 8, 577018. [Google Scholar] [CrossRef]
- Xu, J.; Sun, G.; Cao, W.; Fan, W.; Pan, Z.; Yao, Z.; Li, H. Stigma, Discrimination, and Hate Crimes in Chinese-Speaking World amid COVID-19 Pandemic. Asian J. Criminol. 2021, 16, 51–74. [Google Scholar] [CrossRef]
- Dye, T.D.; Alcantara, L.; Siddiqi, S.; Barbosu, M.; Sharma, S.; Panko, T.; Pressman, E. Risk of COVID-19-related bullying, harassment and stigma among healthcare workers: An analytical cross-sectional global study. BMJ Open 2020, 10, e046620. [Google Scholar] [CrossRef]
- Kisely, S.; Warren, N.; McMahon, L.; Dalais, C.; Henry, I.; Siskind, D. Occurrence, prevention, and management of the psychological effects of emerging virus outbreaks on healthcare workers: Rapid review and meta-analysis. BMJ 2020, 369, m1642. [Google Scholar] [CrossRef] [PubMed]
- Mostafa, A.; Sabry, W.; Mostafa, N.S. COVID-19-related stigmatization among a sample of Egyptian healthcare workers. PLoS ONE 2020, 15, e0244172. [Google Scholar] [CrossRef] [PubMed]
- Shiu, C.; Chen, W.T.; Hung, C.C.; Huang, E.P.; Lee, T.S. COVID-19 stigma associates with burnout among healthcare providers: Evidence from Taiwanese physicians and nurses. J. Formos. Med. Assoc. 2021, 121, 1384–1391. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siu, J.Y.-m. The Role of Social and Cultural Values in Pandemic Control in a Chinese Community: An Ethnographic Study on the Construction and Stigmatization of “Others” in Severe Acute Respiratory Syndrome (SARS) and COVID-19 in Hong Kong. Int. J. Environ. Res. Public Health 2022, 19, 13517. https://doi.org/10.3390/ijerph192013517
Siu JY-m. The Role of Social and Cultural Values in Pandemic Control in a Chinese Community: An Ethnographic Study on the Construction and Stigmatization of “Others” in Severe Acute Respiratory Syndrome (SARS) and COVID-19 in Hong Kong. International Journal of Environmental Research and Public Health. 2022; 19(20):13517. https://doi.org/10.3390/ijerph192013517
Chicago/Turabian StyleSiu, Judy Yuen-man. 2022. "The Role of Social and Cultural Values in Pandemic Control in a Chinese Community: An Ethnographic Study on the Construction and Stigmatization of “Others” in Severe Acute Respiratory Syndrome (SARS) and COVID-19 in Hong Kong" International Journal of Environmental Research and Public Health 19, no. 20: 13517. https://doi.org/10.3390/ijerph192013517
APA StyleSiu, J. Y.-m. (2022). The Role of Social and Cultural Values in Pandemic Control in a Chinese Community: An Ethnographic Study on the Construction and Stigmatization of “Others” in Severe Acute Respiratory Syndrome (SARS) and COVID-19 in Hong Kong. International Journal of Environmental Research and Public Health, 19(20), 13517. https://doi.org/10.3390/ijerph192013517